

Chapter 7:Local Anesthetics
JC Gerancher MD
Associate Professor/ RAAPM Section Head

Chapter Review
• Structure• Mechanism of Action• Nerve Sensitivity• Pharmacokinetics• Side Effects:
– CNS toxicity– CV toxicity
– Allergy

Structure of Local Anesthetics
• Lipophilic benzene ring• Hydrophilic tertiary amide
(proton accepting weak base)
• Linkage by an ester or amide bond
• Mepivacaine, bupivacaine, and ropivacaine have chiral centers

Mechanism of Action
• Bind sodium channels in inactivated-closed state
• Slowing rate of depolarization
• Produce block of conduction (propogation of action potential)

LAs bind and inhibit many differing receptors and channels
• Channels– Na– Ca (multiple types)– K
• Enzymes– Adenylyl cyclase– Guanylyl cyclase– Lipases
• Receptors– Nicotinic
acetylcholine– NMDA
– β2-adrenergic
Anesthesiology 1990; 72:711-34

Factors responsible for nerve Sensitivity
• Anatomy, anatomy, anatomy • Myelination increase conduction velocity and
makes nerves more susceptable to local anesthetics
• Small unmylenated fibers are not especially susceptable just because they are small.
• Use dependant blockade (muscle activity, tachycardia)

PNB effect is predictable
• Onset:– Superficial fibers =
proximal and motor– Deep fibers = distal
and sensory
• Recovery:– Deep vessels clear
deep fibers first– Hard to obtain
‘differential’ blockade-Winnie 1977

Local Anesthesia for PNB: Pharmacokinectics
Manufacturer’s Recommended Maximum Dose
(mg)
Mean Latency to Surgical Anesthesia (minutes)
Mean Durationof SurgicalAnesthesia
(hours)
Mean Duration of Postoperative
Analgesia (hours)
2-chloroprocaine(Nesacaine)
980 5-15 1-2 2-3
Lidocaine(Xylocaine)
490 7-15 2-3 3-5
Mepivacaine(Polocaine,Carbocaine)
400 10-15 3-4 4-6
Bupivacaine (Marcaine)
225 15-40 6-10 12-17
Ropivacaine(Naropin)
250 15-40 5-9 8-14

Local Anesthesia for PNB: No Free Lunch
Manufacturer’s Recommended Maximum Dose
(mg)
Mean Latency to Surgical Anesthesia (minutes)
Mean Durationof SurgicalAnesthesia
(hours)
Mean Duration of Postoperative
Analgesia (hours)
2-chloroprocaine(Nesacaine)
980 5-15 1-2 2-3
Lidocaine(Xylocaine)
490 7-15 2-3 3-5
Mepivacaine(Polocaine,Carbocaine)
400 10-15 3-4 4-6
Bupivacaine (Marcaine)
225 15-40 6-10 12-17
Ropivacaine(Naropin)
250 15-40 5-9 8-14

Quotes from the PDR
• “maximal recommended dose” of 4.5 to 7 mg/kg• “maximum single recommended dose” of 11mg to
14mg/kg• “175 to 225 mg” and “more or less drug may be used
depending on individualization of each case” • “expected average dose of 175 to 250 mg” and “a
cumulative dose of 770 mg over 24 hours.”• “400 mg” with higher doses “not recommended”

Dose and Arterial Plasma Levels
-Brown 1996

Local Anesthetic Levels: site
- McClean 1988
35ml 1.5% Plain Prilocaine

Positive effects– Prolongs duration
– Increases intensity
– Reduces toxicity
– Test dose
Epinephrine

Local Anesthetic Levels: Epi
- Pihlajamaki 1987
40ml 1% Bupivacaine +/- Epi
•Epi→↓circulating levels with lido, mepi, Bupiv, Prilo, and Etidocaine
(vs epidural)
•5 mcg/ml may be max
•May delay peak level

33ml 0.5% Ropivacaine +/- Epi
- Hickey 1990
•Epi→no change in levels achieved with ropivacaine
•ropivacaine itself a vasoconstrictor
Local Anesthetic Levels: Epi

Epinephrine• Decreased nerve
blood flow• At risk:
– Diabetes
– Atherosclerosis
– Intraneural injection
-Myers 1989
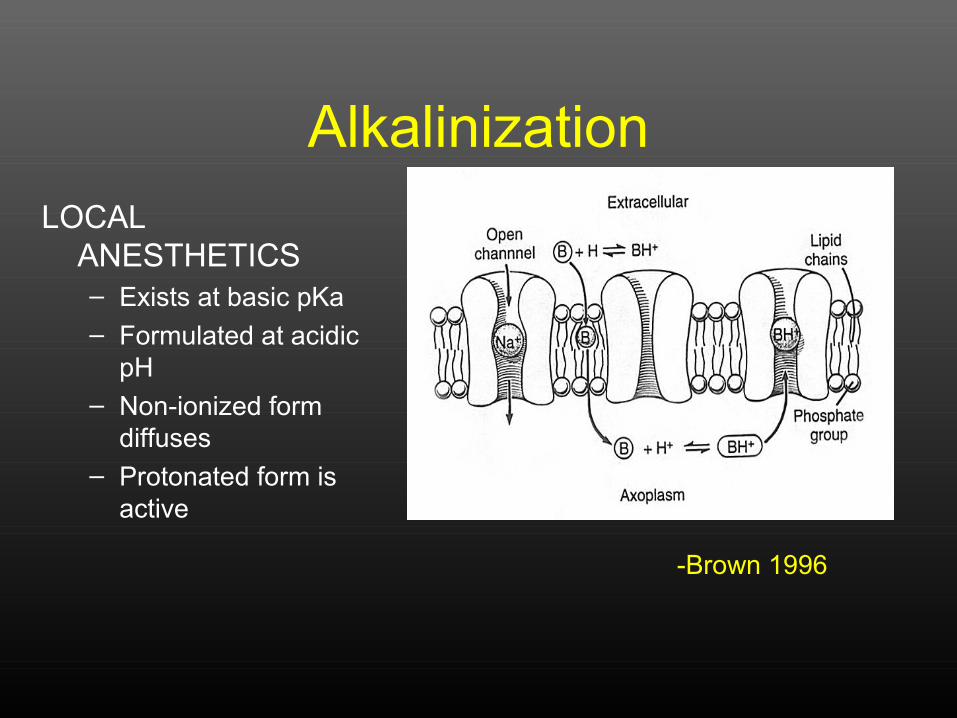
AlkalinizationLOCAL
ANESTHETICS– Exists at basic pKa– Formulated at acidic
pH– Non-ionized form
diffuses– Protonated form is
active
-Brown 1996

Patterns of LA toxicity
• CNS
• CV system
• Allergy
• Treatment

CNS toxicity from LAs• Progression of signs &
symptoms with ↑LA– Vertigo– Tinnitus
– Ominous feelings
– Circumoral numbness– Garrulousness– Tremors– Myoclonic jerks
– Convulsions
– CNS depression
• Convulsive LA dose inversely related to LA potency
• Acidosis, hypercarbia ↓ convulsive dose
• Pregnancy lowers dose but not concentration producing convulsions
• CV toxicity requires greater LA doses and concentrations than CNS toxicity

CNS toxicity from LAs• Progression of signs &
symptoms with ↑LA– Vertigo– Tinnitus
– Ominous feelings
– Circumoral numbness– Garrulousness– Tremors– Myoclonic jerks
– Convulsions
– CNS depression
• Convulsive LA dose inversely related to LA potency
• Acidosis, hypercarbia ↓ convulsive dose
• Pregnancy lowers dose but not concentration producing convulsions
• CV toxicity requires greater LA doses and concentrations than CNS toxicity

LA doses and blood concentrations producing convulsions in sheep: similar rank order as for potency
0
20
40
60
80
100
120
LID ROP BUP
Dose (mg)Conc (mg/L)
Rutten. Anesth Analg 1989;69:291-9

Multiple LA actions on the cardiovascular system
• Electrophysiologic– Bupivacaine vs. lidocaine: faster binding, delayed
unbinding from cardiac Na channels – Antiarrhythmic and proarrhythmic effects– Inhibit conduction system
• Negative inotropic • Vascular
– Vasoconstrict (low concentrations)– Vasodilate (high concentrations)
• LA in CNS can have CV results• Interfere with resuscitation

LAs bind and inhibit many differing receptors and channels
• Channels– Na– Ca (multiple types)– K
• Enzymes– Adenylyl cyclase– Guanylyl cyclase– Lipases
• Receptors– Nicotinic
acetylcholine– NMDA
– β2-adrenergic
Anesthesiology 1990; 72:711-34

LAs bind and inhibit many differing receptors and channels
Do not assume LA toxic side effects arise from Na channel inhibition!
Anesthesiology 1990; 72:711-34

LA blood concentrations producing cardiac arrest in dogs: similar rank
order as for potency
0
20
40
60
80
100
120
Bup Levo Rop Lid
FreeTotal
Groban et al Anesth Analg 2000;91:1103-11
μg
/mL

Allergy to LAs• Common misdiagnosis after
accidental IV injections
• True allergy more common with esters (particularly those related to PABA) than amides
• Avoid PABA in sunscreens• Possible cross reaction
between PABA and methylparaben (preservative in some amide LAs)

None of 90 patients referred for LA reactions have allergy!
• 0 of 90 reacted to 1:100 LA dilutions!
• Few respond to undiluted LA even among 14 referred after anaphylactoid reactions
• Thus, almost no patients had “real” LA allergy
0
20
40
60
80
100
+ - + -
Anaph(N=14)Others(N=76)
1:100 Undiluted
deShazo. J All Clin Immunol 1979;63:387-94
%

Treatment of local anesthetic toxicity
Apparent allergy• Steroids• Histamine (H1) blockers• With severe reactions
– Intravenous fluid– Epinephrine
CNS toxicity• Don’t treat minor
reactions• Seizures: maintain
airway, provide O2
– Terminate seizure with thiopental, midazolam, or propofol
– Intubate patients with full stomachs

Treatment of local anesthetic toxicity
Apparent allergy• Steroids• Histamine (H1) blockers• With severe reactions
– Intravenous fluid– Epinephrine
CNS toxicity• Don’t treat minor
reactions• Seizures: maintain
airway, provide O2
– Terminate seizure with thiopental, midazolam, or propofol
– Intubate patients with full stomachs

Treatment of LA CV toxicity• Follow ACLS guidelines
– Substitute amiodarone for lidocaine– Substitute vasopressin for
epinephrine
• Consider cardiopulmonary bypass or lipid infusion if standard drugs fail

Polarized Light Images: Lidocaine or St Pauli Girl Beer







