

Lung Inflammation, Infection
and Collapse

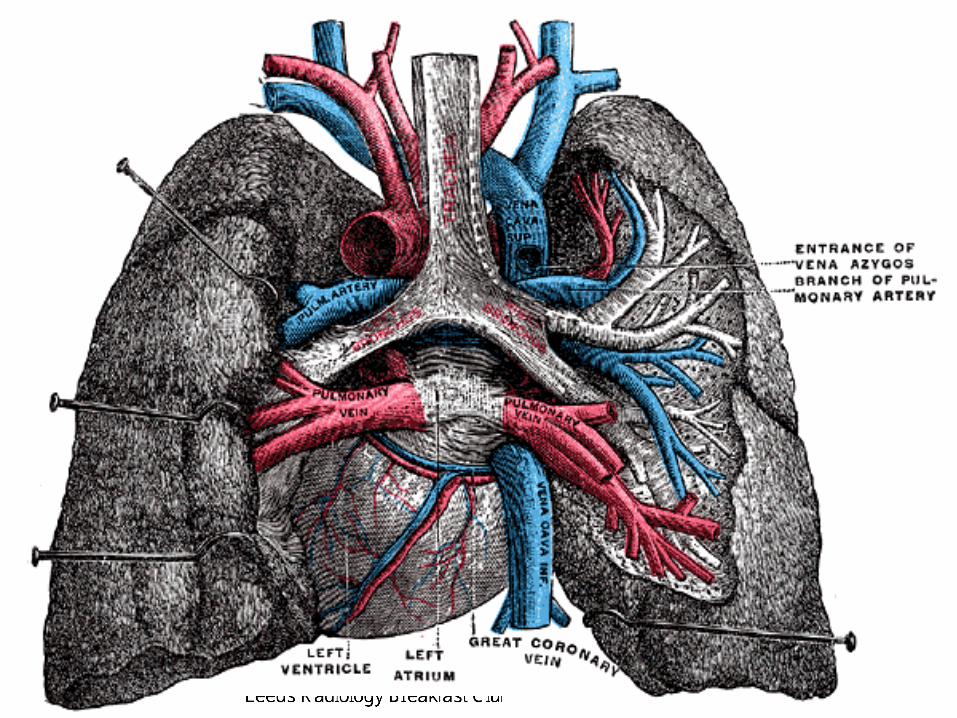
Silhouette Sign

X Ray Densities
AIR FAT SOFT
TISSUE CALCIUM


Airspace Shadowing
• Pathological Definition
– Disease process replacing air from the alveoli
with material of soft tissue attenuation
• Radiological Definition
– Consolidation
– Ground glass


Consolidated lung

Air Space Shadowing
• Ground Glass
– Lungs of increased
attenuation (too white)
but lung markings all
still visible
– Best seen on CT
• Consolidation
– Homogenous opacity
– Loss of vascular
markings
– Ill defined unless
abutting a fissure
– Air bronchograms if
airways remain patent
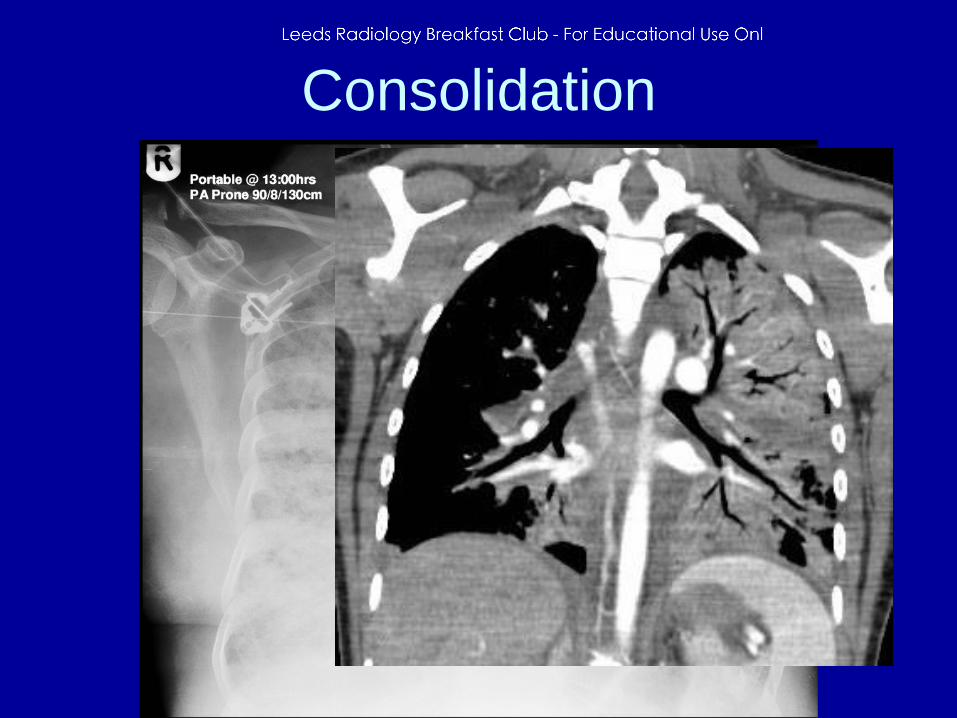
Consolidation


What can fill the alveoli?
• Infection (pus)
• Fluid
• Blood
• Cells
– Inflammatory
– Malignant
• Protein

Infection
• Strep Pneumoniae
– 2/3 bacterial CAP
– 40 - 80% show radiographic resolution by 4
weeks
– 70 -100% by 8 weeks
– Most suggest follow up films at 6 weeks


Round Pneumonia

Infection
• Mycoplasma
– Normally mild disease
– Radiographic resolution rapid
– Most cases resolve completely by 2-4 weeks

Infection
• Legionnaire’s Disease
– Up to 8% CAP
– Higher rates in intensive care
– Up to 40% develop resp failure
– Radiological improvement lags behind clinical
– 50% persistent CXR abnormalities at 12
weeks
– Resolution may take up to 4 months

Legionnaire’s

Infection
• TB/ non tuberculous mycobacteria
– Radiology depends on prior exposure and
immune status
– Primary TB –
• lobar/segmental consolidation
• effusion
– Secondary TB –
• apical upper/lower lobe opacities
• cavitation

Primary TB

Secondary TB

Miliary TB

Infection
• Fungal Pneumonias
– Presentation depends on immune status
– Travel history may be important
• Eg Histoplasmosis/bastomycosis more common in
Mississippi and Ohio river areas
– Chronic necrotising aspergillosis
• associated with underlying lung disease
• Steroid use
• Upper lobe cavitation resembling TB

Aspergillus pneumonia

Causes cavitating pneumonia
• Staphylococcus
• TB
– Classically upper/apical segment lower lobe
• Septic Emboli
– IVDU
• Klebsiella
– Aspiration
• Fungi
– COPD patients, looks very like TB

Fluid
• BIBA
• Central Chest Pain
• Sudden SOB
• Clammy, tachycardic,
• Pulmonary Oedema
due to MI

Fluid
• Recent Surgery
• On ITU
• Sudden Deterioration
• Acute Pulmonary
Oedema due to
leaking aortic valve

Blood
• Police Motorcyclist
• High Speed RTA
• Shocked
• Blood ++ from chest
drains
• Severe Pulmonary
Laceration


Blood
• 60 yo woman
• Acute renal failure
• Anemic
• Haemoptysis
• Acute vasculitis

Cells
• Vague Symptoms
• Cough
• Pyrexia
• Rapid improvement
with steroids
• Cryptogenic
Organising
Pneumonia

2006
2008
COP

Cells
• Persistent cough
• White Sputum ?
• CXR worsening
despite antibiotics
and steroids
• Bronchoalveolar cell
carcinoma

Protein
• Young man
• Productive cough ++
• Repeated admissions
• Regular on ITU
• Alveolar Proteinosis

“Non Resolving” Consolidation
• Definition – Failure to improve by 50% in 2 weeks
– Failure to resolve completely by 4 weeks
– Persisting more than 30 days
• In practice should see significant
improvement on follow up CXR in 6 weeks

Patient behaving like infection but
not getting better?
• Assess for other co morbid factors
• Exclude structural problem in lung
• Isolate organism
• Get sensitivities

Air space shadowing on CXR
but no clinical signs of infection
• Consider other causes
– Heart Failure
– Vasculitis
– ILD
– Drug reaction
– Cancer/Lymphoma
– ARDS

Signs of Lobar Collapse
• Increased density (from collapsed lobe)
• Loss of vessels (into collapsed lobe)
• Shift of hilum (moves with the collapse)
• Volume loss
– Mediastinum
– Diaphragm
• Silhouette
• Overexpansion (of normal lobes)



















