
Lymphangitic Carcinomatosis: Lymphangitic Carcinomatosis: Some HRCT FindingsSome HRCT Findings
AkochiAkochi AgunwambaAgunwamba, Harvard Medical School Year III , Harvard Medical School Year III and Gillian Lieberman, MDand Gillian Lieberman, MD

Lymphangitic Carcinomatosis: Lymphangitic Carcinomatosis: OverviewOverview
Also known as “Also known as “lymphangiaticlymphangiatic spread of tumors”, “spread of tumors”, “lymphangitislymphangitiscarcinomatosacarcinomatosa”, or “”, or “lymphangiosislymphangiosis carcinomatosacarcinomatosa””
LC refers to the infiltration of pulmonary LC refers to the infiltration of pulmonary parenchymalparenchymal lymphatic lymphatic channels by tumor cellschannels by tumor cells
Usually spread to lungs is Usually spread to lungs is hematogenoushematogenous, while spread within , while spread within lungs is lymphangiticlungs is lymphangitic
Unilateral (primary lung cancer and breast carcinoma) Unilateral (primary lung cancer and breast carcinoma) involvement is less common than bilateral (Stomach, Pancreas, involvement is less common than bilateral (Stomach, Pancreas, Prostate, Cervical, Thyroid, Colon, or Adenocarcinoma from an Prostate, Cervical, Thyroid, Colon, or Adenocarcinoma from an unknown site)unknown site)
~80% of the ~80% of the mettastasesmettastases are are adenocarcinomasadenocarcinomas
Herold CJ, et al. “Lung metastases”. Eur. Radiol. 6, 596-606 (1996)

Menu of Radiological TestsMenu of Radiological Tests
Chest XChest X--ray (CXR)ray (CXR)–– ~50% of lymphangitic carcinomatosis patients appear normal on ~50% of lymphangitic carcinomatosis patients appear normal on
CXR CXR
High Resolution Computed Tomography (HRCT)High Resolution Computed Tomography (HRCT)–– Currently appears to offer the best combination of cost and Currently appears to offer the best combination of cost and
sensitivity. 8sensitivity. 8--74% better than CXR for lymphangitic carcinomatosis74% better than CXR for lymphangitic carcinomatosis
Positron emission tomography with radioPositron emission tomography with radio--labeled [18F]labeled [18F]--22--fluorofluoro--deoxydeoxy--DD--glucose (PETglucose (PET--FDG)FDG)–– Very expensive. Sensitivity appears to be identical to HRCT thouVery expensive. Sensitivity appears to be identical to HRCT though gh
experience with PETexperience with PET--FDG in diagnosing lymphangitic carcinomatosis FDG in diagnosing lymphangitic carcinomatosis is limitedis limited
Khan AN, et al. “Lymphangitic Carcinomatosis”. eMedicine - http://www.emedicine.com/Radio/topic416.htm. Accessed 7/19/2008
HRCT findings in Lymphangitic CarcinomatosisHRCT findings in Lymphangitic Carcinomatosis
Herold CJ, et al. “Lung metastases”. Eur. Radiol. 6, 596-606 (1996); Webb, RW et al. Thoracic Imaging: Pulmonary and Cardiovascular Radiology (2005)
Irregular, smooth or nodular thickening of interlobular septaIrregular, smooth or nodular thickening of interlobular septa
Irregular and nodular thickening of Irregular and nodular thickening of peribronchovascularperibronchovascular sheetssheets
Thickening of Thickening of centrilobularcentrilobular structures structures
Peripherally located wedge shaped densities representing edema Peripherally located wedge shaped densities representing edema from lymphatic destructionfrom lymphatic destruction
Pleural diseasePleural disease
Correct first diagnosis 40% of the timeCorrect first diagnosis 40% of the time

Lymphangitic Carcinomatosis : Clinical Lymphangitic Carcinomatosis : Clinical SymptomsSymptoms
The clinical symptoms often precede radiographic The clinical symptoms often precede radiographic abnormalities and include:abnormalities and include:–– BreathlessnessBreathlessness–– Dry coughDry cough–– Hemoptysis (unusual unless there is primary lung cancer)Hemoptysis (unusual unless there is primary lung cancer)
Screening for lymphangitic carcinomatosis occurs Screening for lymphangitic carcinomatosis occurs in the context of prior malignancyin the context of prior malignancy
British Thoracic Society and Standards of Care Committee, Thorax 1999;54;S1-S28
Copyright ©Radiological Society of North America, 2006
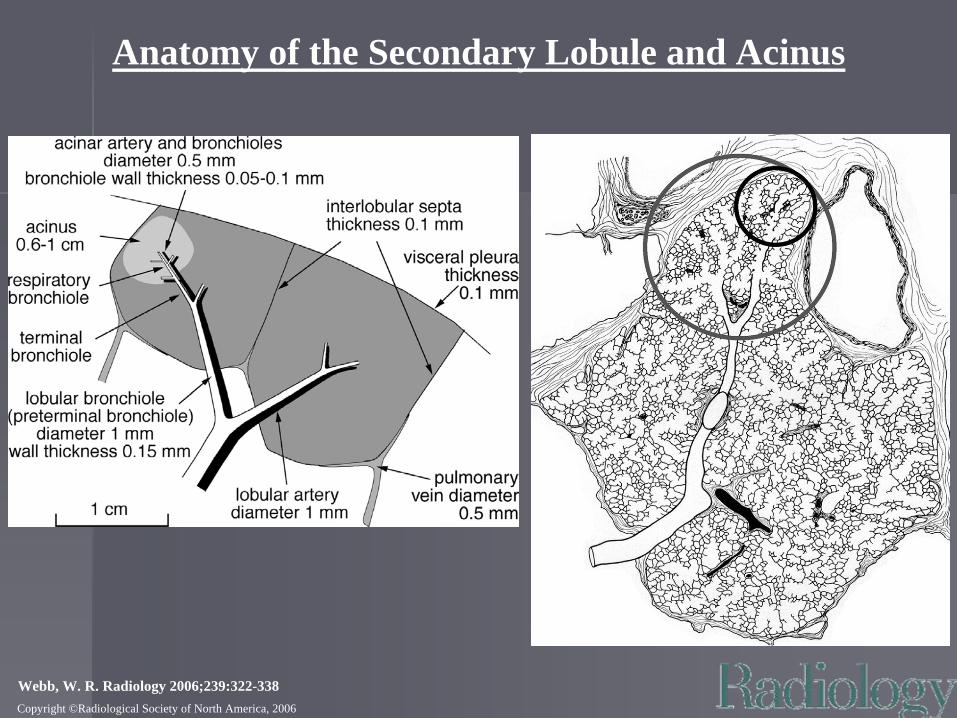
Webb, W. R. Radiology 2006;239:322-338
Anatomy of the Secondary Lobule and Acinus
Copyright ©Radiological Society of North America, 2006
Webb, W. R. Radiology 2006;239:322-338
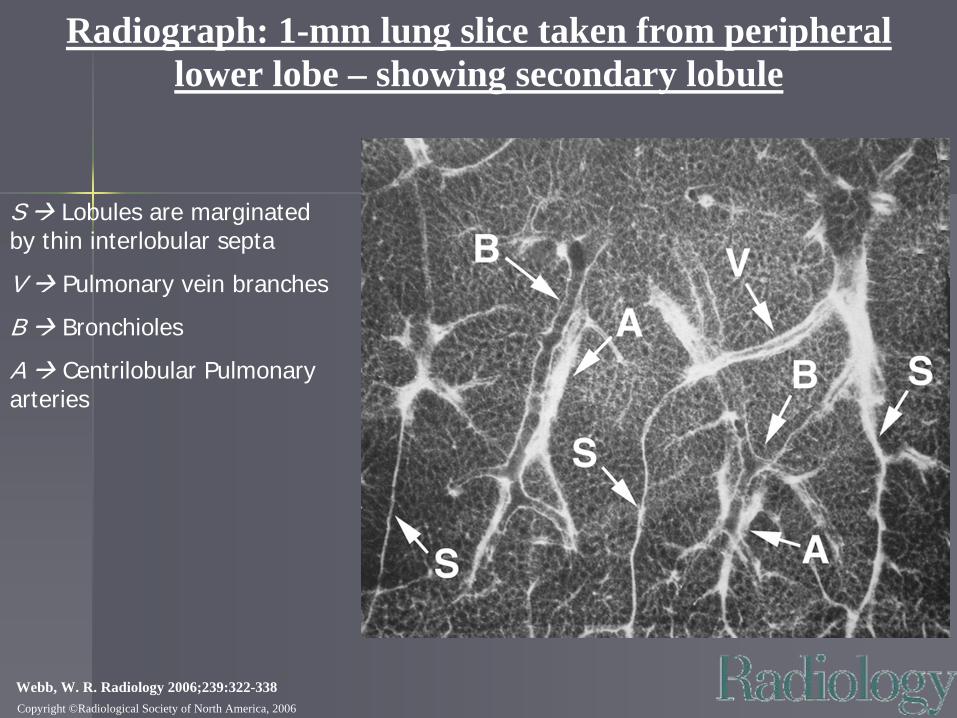
Radiograph: 1-mm lung slice taken from peripheral lower lobe – showing secondary lobule
S Lobules are marginated by thin interlobular septa
V Pulmonary vein branches
B Bronchioles
A Centrilobular Pulmonary arteries

Copyright ©Radiological Society of North America, 2006 Webb, W. R. Radiology 2006;239:322-338
Pathology: Interlobular septal and peribronchovascular thickening in lymphangitic carcinomatosis
On cut lung surface, small white arrows point to thickened interlobular septa and large arrow points to thickened peribronchovascular interstitium
H&E specimen (10x). Black arrows point to nodules of tumor in interlobular septa & centrilobular peribronchovascular region.
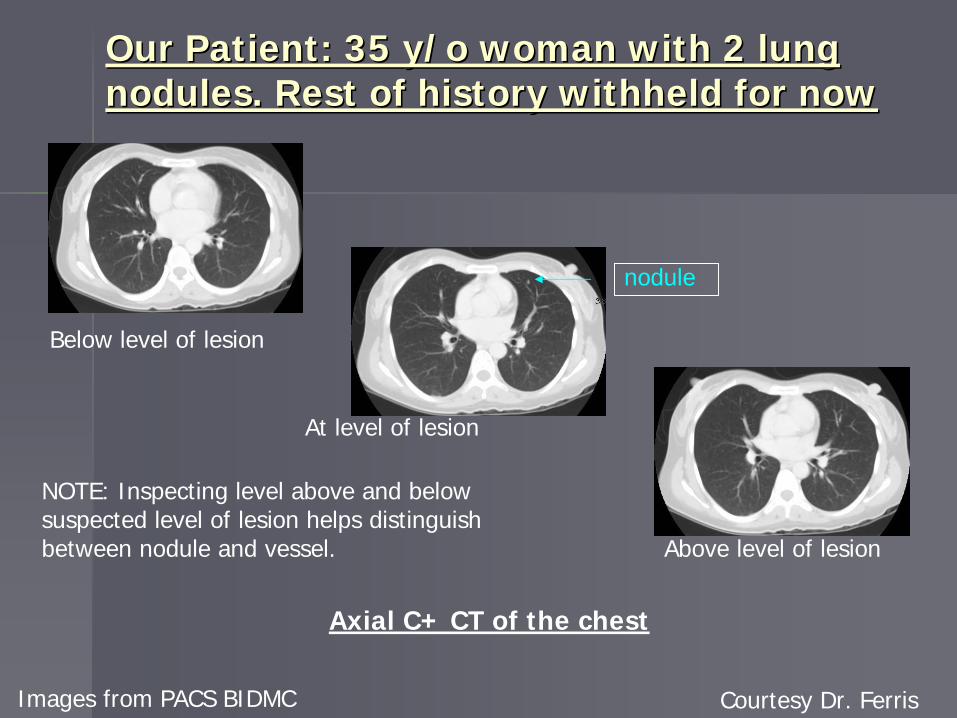
Our Patient: 35 Our Patient: 35 y/oy/o woman with 2 lung woman with 2 lung nodules. Rest of history withheld for nownodules. Rest of history withheld for now
Below level of lesion
At level of lesion
Above level of lesion
NOTE: Inspecting level above and below suspected level of lesion helps distinguish between nodule and vessel.
Images from PACS BIDMC Courtesy Dr. Ferris
nodule
Axial C+ CT of the chest

Differential for solitary nodule Differential for solitary nodule
Malignancy (adenocarcinoma Malignancy (adenocarcinoma -- 40%, 40%, squamoussquamous cell carcinoma cell carcinoma -- 20%, large cell 20%, large cell carcinoma carcinoma -- 15%, 15%, bronchoalveolarbronchoalveolar carcinoma carcinoma -- 10%, solitary metastases)10%, solitary metastases)
Benign Benign neoplasmsneoplasms ((hamartomashamartomas, , lipomaslipomas, and , and fibromasfibromas))
Vascular lesions Vascular lesions -- ArteriovenousArteriovenous malformationmalformation
Infectious Infectious granulomasgranulomas -- Tuberculosis, atypical Tuberculosis, atypical mycobacterialmycobacterial infection, infection, histoplasmosishistoplasmosis, , coccidioidomycosiscoccidioidomycosis, and , and blastomycosisblastomycosis
Other infections Other infections -- AspergillomaAspergilloma, , ascarisascaris, , dirofilariasisdirofilariasis, , echinococcalechinococcal cyst, and cyst, and bacterial abscess bacterial abscess
Noninfectious Noninfectious granulomasgranulomas -- Rheumatoid arthritis, Wegener granulomatosis, and Rheumatoid arthritis, Wegener granulomatosis, and sarcoidosissarcoidosis
Developmental lesions Developmental lesions -- BronchogenicBronchogenic cyst cyst
Other conditions Other conditions -- Hematoma, Hematoma, bronchiolitisbronchiolitis obliteransobliterans--organizing pneumonia, organizing pneumonia, pseudotumorpseudotumor, pulmonary infarction, , pulmonary infarction, amyloidomaamyloidoma, rounded , rounded atelectasisatelectasis, and , and mucoidmucoidimpaction impaction
1. Manocha S, “Solitary Pulmonary Nodule.” eMedicine – accessed 7/21/2008

Our Patient: At 8 Our Patient: At 8 mthmth follow up, presents follow up, presents with tachycardia and with tachycardia and dyspneadyspnea
Images from PACS BIDMC Courtesy Dr. Ferris
Enlarged hilum
Filling defects
Peripheral opacities (probably cellular or fluid infiltrates)
Reformatted HR CTA Axial View of the chest
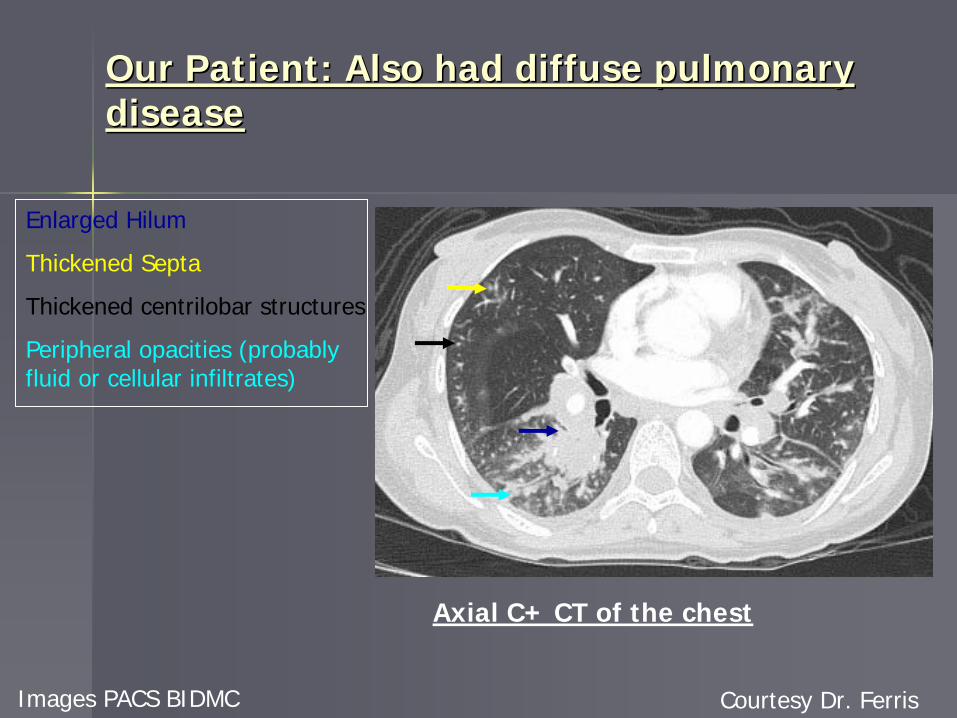
Our Patient: Also had diffuse pulmonary Our Patient: Also had diffuse pulmonary diseasedisease
Images PACS BIDMC Courtesy Dr. Ferris
Enlarged Hilum
Thickened Septa
Thickened centrilobar structures
Peripheral opacities (probably fluid or cellular infiltrates)
Axial C+ CT of the chest

Our Patient: Diffuse interstitial disease on Our Patient: Diffuse interstitial disease on reconstructed reconstructed SagittalSagittal C+ HRCT of the ChestC+ HRCT of the Chest
PACS BIDMC Courtesy Dr. Ferris
Diffuse nodular and septal infiltrates
Major fissure
Serial Slices from Reconstructed Sagittal C+ HRCT of the chest

Our Patient: Interstitial infiltrates on CXR Our Patient: Interstitial infiltrates on CXR and HRCT and HRCT
Images from PACS BIDMC Courtesy Dr. Ferris
Scapula
SVC Porta catheter
Mediastinal enlargement
Increased interstitial markings
Axial C- HRCT
Left Lateral CXRAP Frontal CXR

Differential for septal and centrilobar Differential for septal and centrilobar thickeningthickening
Smooth interlobar septal thickening: Smooth interlobar septal thickening: –– pulmonary edema, hemorrhage, or pulmonary edema, hemorrhage, or venoveno--occlusive disease; occlusive disease;
Lymphangitic carcinomatosis; Lymphangitic carcinomatosis; lymphangiomatosislymphangiomatosis; ; amyloidosisamyloidosis, pneumonia, alveolar , pneumonia, alveolar proteinosisproteinosis
Nodular interlobar septal thickening: Nodular interlobar septal thickening: –– Lymphangitic carcinomatosis; Lymphangitic carcinomatosis; lymphoproliferativelymphoproliferative disease disease
(e.g. lymphocytic interstitial pneumonia); (e.g. lymphocytic interstitial pneumonia); sarcoidosissarcoidosis; silicosis ; silicosis and coal workers pneumoconiosis; and coal workers pneumoconiosis; amyloidosisamyloidosis
Centrilobular nodules due to Centrilobular nodules due to perilymphaticperilymphatic disease: disease: –– Lymphangitic carcinomatosis; Lymphangitic carcinomatosis; sarcoidosissarcoidosis; silicosis, coal ; silicosis, coal
workers pneumoconiosis; lymphocytic interstitial pneumoniaworkers pneumoconiosis; lymphocytic interstitial pneumonia
Ikezoe J, et al. AJR 1995;165:49-52. Webb, W. R. Radiology 2006;239:322-338

Our Patient: Complete HistoryOur Patient: Complete History
The patient is The patient is s/ps/p right right colectomycolectomy for poorly for poorly differentiated signet cell differentiated signet cell mucinousmucinous carcinoma of the carcinoma of the terminal ileum; b/l terminal ileum; b/l salpingosalpingo--oopherectomiesoopherectomies for for metsmets. Mets to . Mets to hemidiaphragmhemidiaphragm, bladder, small , bladder, small bowel, and pelvic side wall also observed. She is bowel, and pelvic side wall also observed. She is currently undergoing chemo.currently undergoing chemo.
This combined with the CT findings makes the This combined with the CT findings makes the suspicion for metastasis to the lung and for suspicion for metastasis to the lung and for lymphangitic carcinomatosis very highlymphangitic carcinomatosis very high
Prognosis for Lymphangitic carcinomatosisPrognosis for Lymphangitic carcinomatosis
Usually very poor Usually very poor –– survival in monthssurvival in monthsIn a small 8yr study of 10 pts treated with In a small 8yr study of 10 pts treated with surgical resection of primary, chemo, and/or surgical resection of primary, chemo, and/or radiation radiation txtx, initially:, initially:–– Pulmonary Pulmonary SxsSxs regressed in 6regressed in 6–– Progressed in 2Progressed in 2–– Unchanged in 2Unchanged in 2–– Median survival post diagnosis was 13 Median survival post diagnosis was 13 mthsmths (range: 11(range: 11--
30mths)30mths)
Ikezoe J, et al. “Pulmonary Lymphangitic Carcinomatosis: Chronicity of Radiographic Findings in Long-Term Survivors”. AJR 1995; 165:49-52.

ConclusionsConclusions
Lymphangitic carcinomatosis spreads Lymphangitic carcinomatosis spreads hematogenouslyhematogenously to the lungs to the lungs and then invades the lymphatic vesselsand then invades the lymphatic vessels
The accumulation of tumor cells causes thickening of the The accumulation of tumor cells causes thickening of the secondary lobule interstitiumsecondary lobule interstitium
HRCT is currently the modality of choice for screening lymphangiHRCT is currently the modality of choice for screening lymphangitic tic carcinomatosis patientscarcinomatosis patients
The diagnosis of lymphangitic carcinomatosis requires a clinicalThe diagnosis of lymphangitic carcinomatosis requires a clinicalcontext that includes malignancy.context that includes malignancy.
The prognosis for lymphangitic carcinomatosis is poorThe prognosis for lymphangitic carcinomatosis is poor
ReferencesReferences
1.1. Bois, R M D. BMJ 16 July 1994;309(6948):175 Bois, R M D. BMJ 16 July 1994;309(6948):175 http://www.bmj.com/cgi/content/full/309/6948/175http://www.bmj.com/cgi/content/full/309/6948/175
2.2. British Thoracic Society and Standards of Care Committee, British Thoracic Society and Standards of Care Committee, Thorax Thorax 1999;54;S11999;54;S1--S28 S28 -- http://thorax.bmj.com/cgi/content/full/54/suppl_1/S1http://thorax.bmj.com/cgi/content/full/54/suppl_1/S1
3.3. Davis S.D. “CT evaluation for pulmonary metastases in patients wDavis S.D. “CT evaluation for pulmonary metastases in patients with ith extrathoracicextrathoracic malignancy” Radiology. 1991 Jul;180(1):1malignancy” Radiology. 1991 Jul;180(1):1--12.12.
4.4. Sakamoto TSakamoto T et al. Pulmonary resection for metastases from colorectal canceet al. Pulmonary resection for metastases from colorectal cancer. Chest. r. Chest. 2001 Apr;119(4):10692001 Apr;119(4):1069--72.72.
5.5. Barclay L, “New Guidelines Issued on Lung Cancer Diagnosis and MBarclay L, “New Guidelines Issued on Lung Cancer Diagnosis and Managementanagement CME.” CME.” -- http://www.medscape.com/viewarticle/562778http://www.medscape.com/viewarticle/562778. Accessed on 7/18/2008. Accessed on 7/18/2008
6.6. Khan AN, et al. “Lymphangitic Carcinomatosis”. Khan AN, et al. “Lymphangitic Carcinomatosis”. eMedicineeMedicine -- http://www.emedicine.com/Radio/topic416.htm. Accessed 7/19/2008http://www.emedicine.com/Radio/topic416.htm. Accessed 7/19/2008
7.7. Stein MG et al. “Pulmonary lymphangitic spread of carcinoma: appStein MG et al. “Pulmonary lymphangitic spread of carcinoma: appearance on CT scans.” earance on CT scans.” Radiology 1987 Feb;162(2):371Radiology 1987 Feb;162(2):371--5. 5.
8.8. HeroldHerold CJ et al. “Lung metastases”. Eur. CJ et al. “Lung metastases”. Eur. RadiolRadiol. 6, 596. 6, 596--606 (1996)606 (1996)9.9. Green N, et al. “Lymphangitic Carcinomatosis: Lung Scan AbnormalGreen N, et al. “Lymphangitic Carcinomatosis: Lung Scan Abnormalities”, J. Nuclear Med. ities”, J. Nuclear Med.
(1975)(1975)10.10. IkezoeIkezoe J, et al. “Pulmonary Lymphangitic Carcinomatosis: J, et al. “Pulmonary Lymphangitic Carcinomatosis: ChronicityChronicity of Radiographic of Radiographic
Findings in LongFindings in Long--Term Survivors”. AJR 1995; 165:49Term Survivors”. AJR 1995; 165:49--52.52.11.11. Webb, WR “Webb, WR “ThinThin--Section CT of the Secondary Pulmonary Lobule: Anatomy and the Section CT of the Secondary Pulmonary Lobule: Anatomy and the
ImageImage——The 2004 The 2004 FleischnerFleischner Lecture”. Lecture”. Radiology 2006;239:322Radiology 2006;239:322--33833812.12. ManochaManocha S, “Solitary Pulmonary Nodule.” S, “Solitary Pulmonary Nodule.” eMedicineeMedicine --
http://www.emedicine.com/RADIO/topic782.htmhttp://www.emedicine.com/RADIO/topic782.htm

AcknowledgementsAcknowledgements
Dr. Clare Dr. Clare HorkenHorkenDr. Dr. GethinGethin WilliamsWilliamsDr. Diana Dr. Diana LitmanovichLitmanovichDr. Diana FerrisDr. Diana FerrisDr. Gillian LiebermanDr. Gillian LiebermanMs. Maria Ms. Maria LevantakisLevantakis







