
MANAGEMENT OF ACUTE POISONING
Kent R. Olson, MDMedical Director
California Poison Control System
San Francisco Division

Lessons from history
A young princess ate part of an apple given to her by a wicked witch
She was found comatose and unresponsive, as if in a deep sleep
Airway positioning and mouth to mouth ventilation were performed, and she recovered fully

Lesson:
Best antidote is good supportive care
(Love’s first kiss)

Case 1:
Young woman found unconscious, several empty pill bottles nearby
Unresponsive to painful stimuli Shallow breathing

Initial management: ABCDs
Airway Breathing Circulation Dextrose, drugs, decontamination

Airway issues
Risks:• Floppy tongue can obstruct airway• Loss of protective reflexes may permit
pulmonary aspiration of gastric contents
Major cause of morbidity in poisoned patients

Assessing the airway
“Gag” reflex• Indirect measure• May be misleading• Can stimulate vomiting
Alternatives
Breathing
Assess visually pCO2 reflects ventilation - ABG useful pulse oximetry provides convenient,
noninvasive evaluation of O2 saturation

Pitfalls
pO2 measures dissolved oxygen• can be normal despite abnormal
hemoglobin states, eg COHgb, MetHgb
Pulse oximetry also fails to detect CO poisoning

Interventions
Endotracheal intubation• Protects airway• Allows for mechanical ventilation
Reverse coma?• Naloxone: note T½ = 60 min• Flumazenil?
Don’t forget GLUCOSE
“A stroke is never a stroke until it’s had 50 of D50” – Dr. Larry Tierney, 1976
• “Well, you could just do an Accuchek”- ibid, 2002
Give Thiamine 100 mg IM or in IV

Case, continued…
The patient has no gag reflex, and does not resist intubation.
She remains unconscious and on a ventilator overnight
Awakens and extubated the next day Dx: mixed sedative drug overdose
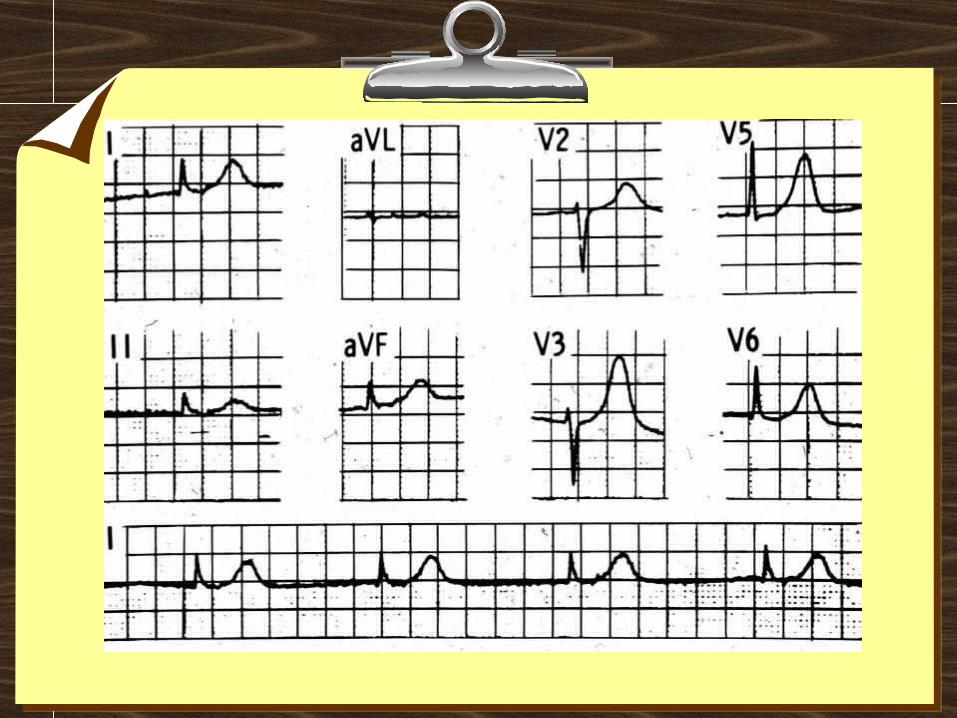
Case 2
47 year old man calls 911, suicidal BP 70/50, HR 50/min Junctional rhythm Hx: uses an antihypertensive

Circulation = plumbing
Pump working? Enough volume (is it primed)? Adequate resistance (no leaks)?
Management of Hypotension
Hypovolemia?• IV fluid challenge
Pump?• Dopamine
Inadequate vascular resistance?• Norepinephrine, phenylephrine

Antihypertensives
Diuretics Beta blockers Calcium channel blockers ACE Inhibitors Centrally acting agents Vasodilators
Calcium channel blockers
Bad ODs!! Low Toxic:Therapeutic ratio High mortality
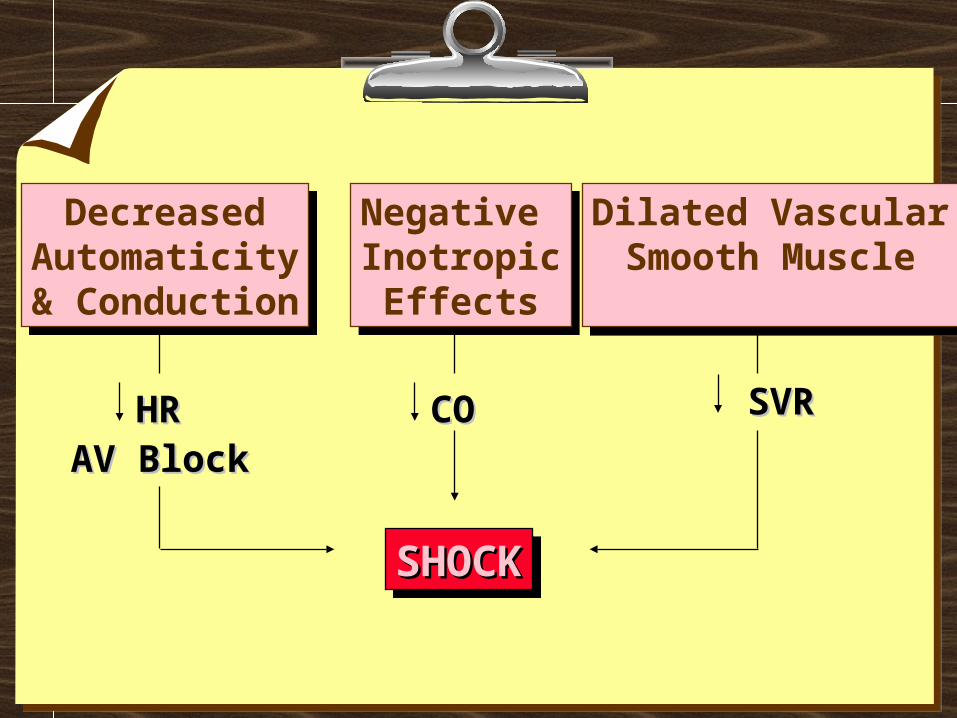
Negative InotropicEffects
Negative InotropicEffects
DecreasedAutomaticity& Conduction
DecreasedAutomaticity& Conduction
Dilated VascularSmooth Muscle
Dilated VascularSmooth Muscle
SVRSVRCOCOHRHRAV BlockAV Block
SHOCKSHOCKSHOCKSHOCK

Calcium antagonists - treatment
Calcium: most effective• High doses may be needed
Glucagon – variable results Insulin plus glucose? (experimental)

Case 3:
An 18 month old takes some of his grandmother’s “sleeping pills”
Brought to the ER after a seizure HR 150/min Pupils dilated, skin flushed, mucous
membranes dry
Common causes of seizures
Amphetamines/cocaine Tricyclic and other antidepressants Isoniazid (INH) Diphenhydramine Alcohol withdrawal Many others . . .

30 minutes later, the ECG shows:

Tricyclic antidepressants
Anticholinergic syndrome Seizures Cardiotoxicity

TCA overdose treatment(similar tox possible w/ massive diphenhydramine)
Stop the seizures• Benzodiazepines, phenobarbital
Treat cardiotoxicity• Sodium bicarbonate 1 mEq/kg IV• IV fluids• Dopamine and/or NE

Case 4: metabolic acidosis
Young man had a seizure at home In ED: obtunded, another seizure pH 6.94, pCO2 32 Recent immigrant, lives with extended
family Uncle being treated for TB

Metabolic Acidosis: MUDPILES
Methanol Uremia DKA Phenformin (whaa?) Isoniazid, Iron Lactic acidosis Ethylene Glycol Salicylate
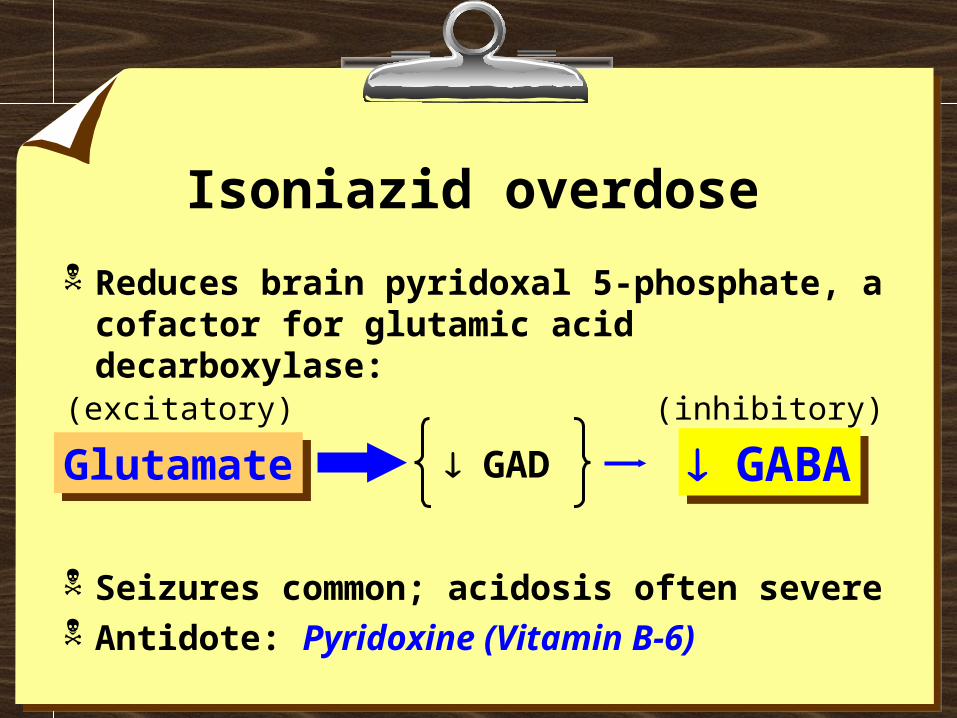
Isoniazid overdose
Reduces brain pyridoxal 5-phosphate, a cofactor for glutamic acid decarboxylase:
Seizures common; acidosis often severe Antidote: Pyridoxine (Vitamin B-6)
GlutamateGlutamate GABA GABA GAD
(excitatory) (inhibitory)

Case 5: another acidosis
44 year old man, obtunded BP 110/80 HR 110 RR 24 pH 7.47 pCO2 22 pO2 92 Na 140 K 3.8 Cl 104 HCO3 18 EtOH 0.18 gm/dL (180 mg/dL)
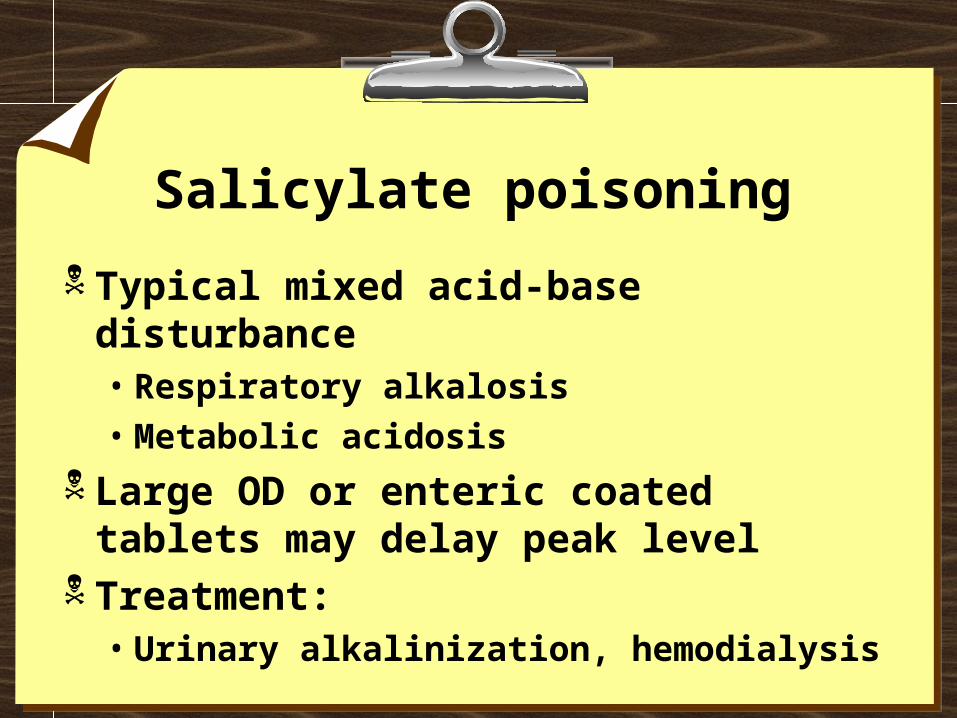
Salicylate poisoning
Typical mixed acid-base disturbance• Respiratory alkalosis• Metabolic acidosis
Large OD or enteric coated tablets may delay peak level
Treatment: • Urinary alkalinization, hemodialysis

Case 6: more acidosis
30 yo woman found comatose T 92 F, pH 6.9 Na 147, K 4.9, Cl 105, Bicarb 5 (AG 37) Glucose 166, BUN 16, Cr 1.5 Measured Osm 331 (calculated 308) EtOH: none detected

The Osmolar Gap
Common causes of Osm Gap:• Ethanol• Methanol & Ethylene Glycol• Other alcohols, also aldehydes, ketones
Osm = 2 (Na) + BUN/2.8 + Glucose/18
Gap = Measured - Calculated Osm = 0 + 5

METHANOLMETHANOL
FORMALDEHYDEFORMALDEHYDE
FORMIC ACIDFORMIC ACIDANION GAPACIDOSIS
ANION GAPACIDOSIS
ELEVATEDOSMOLAR GAP
ELEVATEDOSMOLAR GAP

Methanol or Ethylene Glycol:
Elevated Osm Gap Anion gap
• Low lactate, does not account for gap• Anion gap may be absent early after OD
Other clues (may be unreliable):• Methanol: blindness, visual disturbance• EG: urine crystals, fluorescence

Methanol or Ethylene Glycol:
Main DDx: alcoholic ketoacidosis• Anion and Osm gaps• Low lactate
Clues to AKA:• Gets better quickly w/ IV fluids, dextrose• [Ketones] +/- (mainly -hydroxybutyrate)

Case 7: now we’re cookin’
24 year old man with Hx depression Agitated, confused BP 110/70 HR 120 RR 20 T 40.4 C Muscle tone increased, LE clonus Tox screen negative for cocaine,
amphetamines

Drug-induced Hyperthermia
Heat Stroke Malignant Hyperthermia Neuroleptic Malignant Syndrome Serotonin Syndrome

Drug-induced “heat stoke”
Altered judgment leads to excessive sun/heat exposure
Anticholinergic drugs prevent sweating
Excessive muscle hyperactivity from seizures, or from extreme agitation

Malignant hyperthermia
Rare, familial myopathy Triggered by general anesthesia
• Succinylcholine• Inhalational agents (eg, Halothane)
Muscle rigidity, hypermetabolic state Treatment: dantrolene

Neuroleptic Malignant Syndrome
Patient on dopamine-blocking drugs • Haloperidol classic cause• Also with newer agents (eg, clozapine)
Rigidity (lead-pipe) Autonomic instability Hyperthermia

Serotonin Syndrome
Current “hot” diagnosis Serotonin-enhancing Rx
• SSRIs in OD or multiple combos• MAOI + serotonin-ergic drug
Hypertonicity/clonus (esp. lower extr.) Autonomic instability Hyperthermia

Hyperthermia treatment Act quickly!
• Remove clothing spray and fan• Sedation and anticonvulsants PRN• Neuromuscular paralysis if T >40 C• Dantrolene if NM paralysis ineffective• Consider bromocriptine, cyproheptadine

One more common one
A 17 year old boy takes a bottle of “aspirin” after he gets his SAT score
Next morning, he is vomiting In the ED, normal vital signs Aspirin (salicylate) = negative

Acetaminophen
Very common overdose May be overlooked
• “It’s just aspirin” (OTC’s can’t kill you..?)• Hidden ingredient in many drug combos• No specific findings after OD• Delayed illness/lab abnormalities

Acetaminophen (APAP)
Glucuronidation(non toxic)
Sulfation(non toxic)
NAPQI
P-450
~ 5%
Glutathione + NAPQInontoxic product
Liver cell damage
NAC
++

N-acetylcysteine (NAC) Start within 8 hrs if possible Vomiting often interferes w/oral
dosing• Antiemetics (ondansetron, etc)• Can dribble in by NG tube
IV form now available (Acetadote™)• Caution: hypotension w/rapid infusion
Gut decontamination after OD
Goal: reduce systemic absorption• Induce vomiting?• Pump the stomach?• Activated charcoal

Ipecac-induced emesis
Easy to perform, butnot very effective
Contraindicated:• Comatose/convulsing• Ingested corrosive or hydrocarbon
Bottom line: nobody uses it anymore

Pumping the stomach
Cooperation not required MD sense of
“control” Punitive value?
Gastric lavage
May stimulate gagging, vomiting Risky if airway reflexes dulled Lack of proven efficacy Bottom line: used only rarely

Activated charcoal
Finely divided powdered material• Huge surface area
Binds most drugs/poisons• Exceptions:
• Lithium• Iron
Activated charcoal
More effective than SI, GL First choice for most ODs
Whole bowel irrigation
Mechanical flush Balanced salt solution with PEG
• No net fluid gain/loss Good for:
• Iron• Lithium• Sustained-release pills,
foreign bodies

Antidotes:
The best antidote is supportive care Examples of antidotes:
• Digoxin-specific antibodies• Atropine & 2-PAM• N-acetylcysteine• Vitamin B-6 (pyridoxine)

Call the Poison Center
1-800-222-1222 - 24 hours Immediate consultation by
clinical pharmacists Back-up by MD toxicologists Identify pills, discuss diagnosis & Rx
“I don’t think we should go up there, especially without a paddle”







