

Mandatory program for Mandatory program for hospital professional staffhospital professional staff
Update infection control on SARS
Management of Norovirus outbreak
Infection Control Team
26 November 2003

Standard Precautions & Standard Precautions & Transmission Based PrecautionsTransmission Based Precautions

1970 first CDC isolation recommendation
1983 CDC guideline for prevention and control of nosocomial infections
Strict isolation, respiratory isolation, enteric precautions, contact isolation, tuberculosis(AFB) isolation, drainage / secretion precautions, and blood / body fluid precatuions.
1987 Universal precautions ( Universal blood and body fluid precautions ) - UPBody substance isolation ( BSI )
1996 New CDC isolation guideline – Standard precautions ( combines UP & BSI )


Guideline for Isolation Guideline for Isolation Precautions in hospitals - CDCPrecautions in hospitals - CDC
Two tiers of precautionsStandard PrecautionsTransmission Based Precautions
- Airborne
- Droplet
- Contact
Standard PrecautionsStandard Precautions
Apply to all patients regardless of diagnosis or known infection status.
Applicable to blood, all body fluids, secretions, and excretions, whether they contain visible blood or not ( except sweat ).

Fundamentals of Standard PrecautionsFundamentals of Standard Precautions
Hand washing
Gloves
Clean, non-sterile gloves when touching blood, body fluids, secretions, excretions and contaminated items.
Mask, eye protection, face shield
Protect mucous membrane of eyes, nose and mouth if activities that are likely to generate splashes or spray of blood, body fluid, secretion and excretion.
Gown
Clean, non-sterile gown to prevent soiling of clothing.
Patient care equipment
Reusable equipment should be cleaned and reprocessed appropriately before and after use on patient.

Environmental control Adequate routine cleaning, disinfection of environmental surfaces, equipment and frequently touched surface.
LinenHandle, transport and process of soiled linen with care.
Prevent sharp injuriesNever recap used needle, bend or break the needle. Single-handed technique or mechanical device if recapping necessary.Use mouth pieces, resuscitation bag or other ventilation devices as alternative to mouth-to-mouth resuscitation method.
Patient placementPlace in private room if likely to contaminate the environment. E.g. poor hygiene.
HousekeepingRoutine daily cleaning. Airing of room or delay in admitting next patient is not needed.

Airborne PrecautionsAirborne Precautions
For patients known or suspected to be infected with microorganisms transmitted by air borne droplet nuclei ( small-particle residue ie. 5 um or smaller in size )
e.g. measles ( rubeola ), varicella ( chicken pox ) including disseminated zoster, TB.

Airborne PrecautionsAirborne PrecautionsIn addition to Standard PrecautionsIn addition to Standard Precautions
1. Patient placement
Private room
~ negative pressure in relation to surrounding area.
~ 6-12 air changes per hour.
~ appropriate discharge of air outdoors or high- efficiency filtration of air if recirculate. ( HEPA )
~ Door kept closed.
Anteroom – extra measure, no adequate data regarding the need.

2. Respiratory protection Wear respiratory protection when entering the room
of patient with known or suspected TB – N95 particulate respirator.
Susceptible persons should not enter room of patient known or suspected to have measles or chicken pox.
Persons immuned need not wear respiratory protection.
3. Patient transport Limit movement. Minimize patient dispersal of dro
plet nuclei by wearing a surgical mask.

Prevention of Airborne Prevention of Airborne TransmissionTransmissionN95 respirator tested by HA: regular size (3M-1860R, 3M-8210); small size (3M-1860S, 3M- 9210, 3M-9320), Gerson brand model 2735S, and Kimberly Clark ‘duckbill’ models
Aerosol (Cough) Generating Procedure: •Negative Pressure Room•PPE

Droplet precautionsDroplet precautions
For patient known or suspected to be infected with microorganisms transmitted by large- particle droplets ( > 5 um in diameter ) that can be generated by patient during coughing, sneezing or talking, or performance of procedures.
Transmission via close contact within 3 ft.
e.g. meningococcal meningitis, influenza, parvovirus B19, rubella, mumps.

Droplet precautionsDroplet precautionsIn addition to Standard precautionsIn addition to Standard precautions
1. Patient placement
If private room or cohorting is not possible, place at least 3 ft. from other patients.
2. Mask
When working within 3 ft. of patient.
3. Patient transport
Minimize dispersal of droplet by wearing a mask.

Contact PrecautionsContact Precautions
For patients known or suspected to be infected or colonized with epidemio-logically important microorganisms that can be transmitted by direct or indirect contact.
e.g. G.I, respiratory, skin or wound infection with multi-resistant bacteria.
Contact PrecautionsContact PrecautionsIn addition to Standard PrecautionsIn addition to Standard Precautions
1. Patient placement
If private room or cohorting not achievable, consider the epidemiology of the microorganism and patient population.
2. Gloves and handwashing
Wear gloves when enter the room and remove before leaving patient environment.
Handwashing after gloves removed.

3. Gown
Remove gown before leaving patient’s environment.
4. Patient transport
Minimize risk of contamination of environment surface or equipment.
5. Patient care equipment
When possible, dedicate use of non-critical patient-care equipment to a single patient.
For reuse of common equipment,clean and disinfect before use on another patient.

Faecal Oral TransmissionFaecal Oral Transmission
Areas requiring special attention:•Handling bed pans•Flushing of toilets•Clean up Spillage•Specimens Handling

•Clean up Spillage
•Specimens Handling

Standard Precautions
Contact Precautions
Droplet Precautions
Airborne Precautions
Indications All patients Faecal-oral, fomite, contact
Droplets(>5 in size)
Droplet nuclei, 1-5 in size
Handwashing After contact bld, BF, Sec, Exc, & cont. items
Wash with antiseptics upon gloves removal
Gloves For contact bld, BF, Sec, Exc, & cont. items
When enter the room
Mask, Eye protection/ Face Shield,Gown
Procedure splashes of bld, bf, sec & exc likely
Mask within 3 feet of patient
N95 upon entering the room
Environment
Routine cleaning/disinfection
Private room
Patients with poor hygiene
optional If NA, cohorting Negative pressure, 6-12 ACH
Others Dedicated use of non-critical item
Surgical mask for patients during transport
Surgical mask for patients during transport
Hand washiHand washingng

AA SourceSource of undesired microorganisof undesired microorganisms (multiplying in and being shed froms (multiplying in and being shed from skin)m skin)
Main microbial vectorMain microbial vector of spread of in of spread of infection.fection.
Your hand is . . .Your hand is . . .

CharacteristicsCharacteristicsTransientTransient(noncolonizing orcontaminating flora)
ResidentResident((colonizing flora)
Isolated fromIsolated from Skin from most of peopleSkin from most of people Skin from most of peopleSkin from most of people
PresentPresent Not persistentlyNot persistently but can be but can be readily trans. by handreadily trans. by hand
PersistentlyPersistently
MultiplicationMultiplication
on the skinon the skin
UnableUnable to multiply to multiply
(usually do not survive for (usually do not survive for very long time)very long time)
MultiplyMultiply on the upper on the upper regions of the hair follicleregions of the hair follicle
Removed by Removed by mechanical mechanical meansmeans
EasilyEasily removed by handwa removed by handwashing for shing for 1 min1 min. by soap & . by soap & waterwater
DifficultDifficult by normal by normal techniquetechnique
e.g.e.g. MRSA, Ps. aureginosa, AciMRSA, Ps. aureginosa, Acine. spp., Salmonella spp, E.ne. spp., Salmonella spp, E. coli. etc coli. etc
Staph. spp, other Gm –ve bacStaph. spp, other Gm –ve bacteria on moist skinteria on moist skin


Therefore . . .Therefore . . .
Effective handwashing is the Effective handwashing is the single msingle most importantost important infection control meas infection control measure to ure to protect patientsprotect patients in clinical are in clinical areas from hospital acquired and cross-ias from hospital acquired and cross-infections.nfections.
Hand washingHand washingObjective :Objective :1.1. Prevent hand-borne infectionPrevent hand-borne infection2.2. Remove dirt, organic material and majority Remove dirt, organic material and majority
of transient flora.of transient flora.3.3. by unmedicated detergent and water.by unmedicated detergent and water.Factors affecting proper handwashingFactors affecting proper handwashing1.1. Availability of handwashing facilities : Availability of handwashing facilities :
basin, water tap, ( water flow, temp.) detergbasin, water tap, ( water flow, temp.) detergent dispenser, towel.ent dispenser, towel.
2.2. Compliance : lack of timeCompliance : lack of time Infectious lesions must be healed before hands regarded aInfectious lesions must be healed before hands regarded a
s safe.s safe.

IC practice: Handwashing A matter of Motivation and Convenience ?
Setting YearAverage compliance
Medical Wards HK
June 2003
78%
ICU 1999 36%Emergency Room
1994 32%
ICU 1992 40%ICU 1990 32%All Wards 1983 45%
• frequent• consistent• after gloves removal• antiseptics if indicated

Effective hand washingEffective hand washing
CDC & HICPAC recommendationCDC & HICPAC recommendation::
Soaps (medicated / unmedicated) & watSoaps (medicated / unmedicated) & water should be used if hands are er should be used if hands are visibly sovisibly soilediled
If no visible dirt, use of waterless, If no visible dirt, use of waterless, alcohoalcohol-based hand rubl-based hand rub for routine antisepsis for routine antisepsis
presurgical hand antisepsis, either methpresurgical hand antisepsis, either methods are suitableods are suitable
HICPAC: Hospital Infection Control Practices Advisory CommitteeHICPAC: Hospital Infection Control Practices Advisory Committee

Time Time takentaken
+ + Agents Agents useuse
+ + TechniqueTechnique
Time Time takentaken
+ + Agents Agents useuse
+ + TechniqueTechnique
====Efficacy Efficacy
ofofEfficacy Efficacy
ofofHandwashingHandwashingHandwashingHandwashing

Interrupting transmission of micrInterrupting transmission of microorganismsoorganisms
Agents Agents useuse

Types of HandwashingTypes of Handwashing
1.1. Social handwaSocial handwashingshing
2. Hygienic hand d2. Hygienic hand disinfectionisinfection
3. Surgical hand di3. Surgical hand disinfectionsinfection(Surgical scrub)(Surgical scrub)
A. Hygienic hand wash A. Hygienic hand wash B. Hygienic hand B. Hygienic hand rub rub
TechniqueTechnique

1. Social handwashing1. Social handwashing
Why Maintain the hands socially Maintain the hands socially cleancleanRemove transient floraRemove transient flora
How Thorough wash +Thorough wash +a bar or liquid soapa bar or liquid soap
When All routine tasks within general All routine tasks within general wardswards

2. Hygienic hand disinfection2. Hygienic hand disinfection(hygienic hand wash & (hygienic hand wash & hand rubhand rub))
Why To remove majority of transient flora To remove majority of transient flora and part of resident flora by and part of resident flora by skin skin antiseptic antiseptic
Wash
Rub
How A thorough or defined wash for A thorough or defined wash for 15-30 sec15-30 sec wi with an antiseptic soap or detergent e.g. idiopth an antiseptic soap or detergent e.g. idiophors, chlorhexidine gluconate, triclosanhors, chlorhexidine gluconate, triclosanAlternatively, apply an Alternatively, apply an alcoholic hand-rubalcoholic hand-rub t to disinfect clean handso disinfect clean hands
When 1.1. During outbreaksDuring outbreaks
2.2. In high risk areas In high risk areas
3.3. When contact with infectious When contact with infectious materialsmaterials
4.4. Before procedures & after leaving Before procedures & after leaving isolation roomisolation room

… … cont’d (Hygienic hand wash)cont’d (Hygienic hand wash)
1.1. Wet hands first with waterWet hands first with water2.2. Apply soap/ antiseptic lotionsApply soap/ antiseptic lotions3.3. Rub hands together Rub hands together
vigorouslyvigorously ~ ~ 15sec15sec4.4. Rinse with waterRinse with water5.5. Dry Dry thoroughlythoroughly with with
disposable toweldisposable towel6.6. Use towel to Use towel to turn offturn off the the
faucet.faucet.7.7. Avoid using Avoid using hothot water water
(increase risk of dermatitis)(increase risk of dermatitis)


… … cont’d (Hygienic hand rub)cont’d (Hygienic hand rub)Rubbing small portions ( Rubbing small portions (
3-5 ml ) of antiseptic with 3-5 ml ) of antiseptic with all areas of hands & fingerall areas of hands & fingers to be covered, till s to be covered, till hands hands drydry..
Alcoholic rubs well suited Alcoholic rubs well suited for hygienic hand disinfectfor hygienic hand disinfection :ion :1.1. Antimicrobial perfAntimicrobial performance is excellent.ormance is excellent.2.2. No wash basinNo wash basin

… … cont’d cont’d (Hygienic hand wash Vs Hand (Hygienic hand wash Vs Hand rub)rub)A recent study conducted in Switzerland confirms the A recent study conducted in Switzerland confirms the effectiveness of hand rub: effectiveness of hand rub: Lancet 2000; 356: 1307-12Lancet 2000; 356: 1307-12
Handrub solution (alcohol-based 0.5% chlorhexidine gluconHandrub solution (alcohol-based 0.5% chlorhexidine gluconate and skin emollients) were distributed to all wards, ate and skin emollients) were distributed to all wards,
Holders were mounted on all beds to facilitate access, Holders were mounted on all beds to facilitate access, HCWs were encouraged to carry a bottle in their pocket, HCWs were encouraged to carry a bottle in their pocket,
Outcomes: Outcomes: Overall nosocomial infection decreasedOverall nosocomial infection decreased (16.9% in 1994 to 9.9 (16.9% in 1994 to 9.9
% in 1998); % in 1998); MRSA rates decreasedMRSA rates decreased (2.16 to 0.93 per 10,000 patient-days) (2.16 to 0.93 per 10,000 patient-days) Handwashing compliance increasedHandwashing compliance increased to 48-66%. to 48-66%.
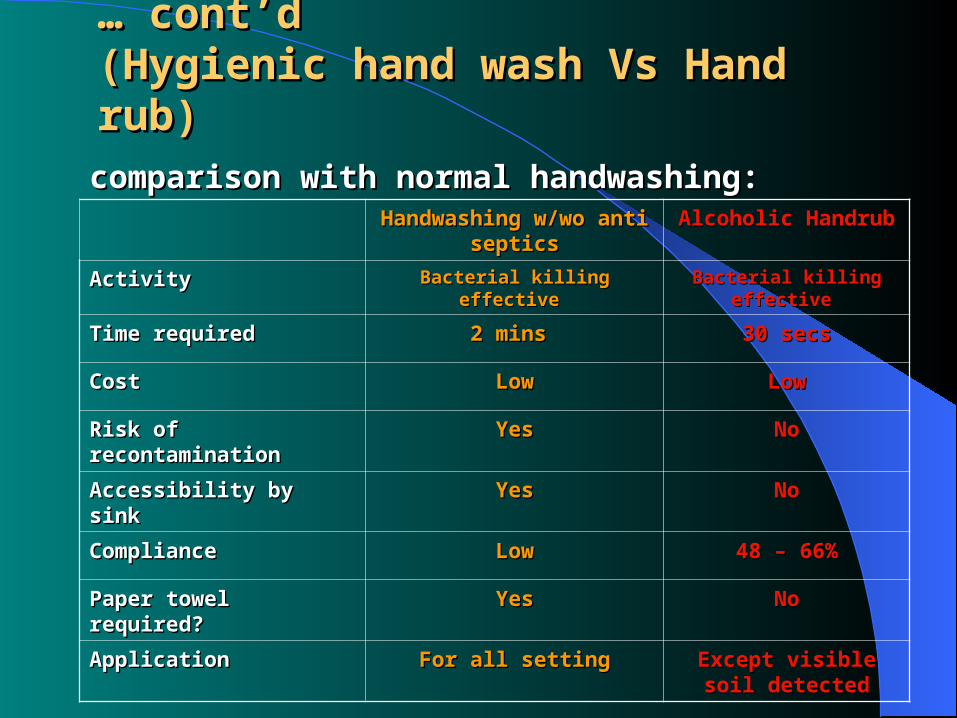
… … cont’d cont’d (Hygienic hand wash Vs Hand (Hygienic hand wash Vs Hand rub)rub)
comparison with normal handwashing:comparison with normal handwashing: Handwashing w/wo antiseHandwashing w/wo antise
pticspticsAlcoholic HandrubAlcoholic Handrub
ActivityActivity Bacterial killing effective Bacterial killing effective Bacterial killing Bacterial killing effective effective
Time required Time required 2 mins 2 mins 30 secs30 secs
CostCost LowLow LowLow
Risk of Risk of recontamination recontamination
YesYes NoNo
Accessibility by sinkAccessibility by sink YesYes NoNo
ComplianceCompliance LowLow 48 – 66%48 – 66%
Paper towel required?Paper towel required? YesYes NoNo
ApplicationApplication For all settingFor all setting Except visible soil Except visible soil detecteddetected

Point to note : Point to note : Skin dryness & irritation -Skin dryness & irritation - by applying lotions & creams by applying lotions & creams irritant contact dermatitis due to handwa irritant contact dermatitis due to handwa
shing or hand antisepsisshing or hand antisepsis
Nail polish –Nail polish – No artificial fingernails or extenders when having direct contact with pts No artificial fingernails or extenders when having direct contact with pts
at high risk (e.g. ICU, O.T.)at high risk (e.g. ICU, O.T.) Keep natural nails tips short (<1/4-inch long)Keep natural nails tips short (<1/4-inch long)
Glove use -Glove use - Do not wear same glove for > one ptDo not wear same glove for > one pt Change glove during pt care if moving from contaminated site to clean Change glove during pt care if moving from contaminated site to clean
body site.body site. Handwashing still require after removal of glove because contamination Handwashing still require after removal of glove because contamination
by small, undetected holes on glovesby small, undetected holes on gloves
Wearing of jewellery –Wearing of jewellery – Should be limitedShould be limited
Topping up of antiseptics – Topping up of antiseptics – Do not add soap to a partially empty soap dispenserDo not add soap to a partially empty soap dispenser. .
bacterial contamination of soap. (strongly recommended)bacterial contamination of soap. (strongly recommended)

Update for Update for prevention of prevention of
SARSSARS

Effective Infection Control
Guidelines &Directives
AdequateFacilities &
Supplies
Communication&
Training
Enforcement&
Drill
Review&
Update

SARS:SARS: Prevention StrategiesPrevention Strategies
Hospital level
Case Detection
InfectionControl
HCW Visitors
•Alert System
•High Index of suspicion
•Lab. Dx
•Reporting to HAHO & DH
• Patient Triage
• Standard Precautions for ALL patients
• Procedure & Risk related PPEs
• SARS Alert• Health
surveillance• Influenza
Vaccination• Training &
Drill
• No visit in HR areas•Limit & Register in non-HR•Mask if symptomatic
Intelligence

SARS:SARS: Mode of transmissionMode of transmission Contact secretions and excretions
– Sources: fomites, patients BABF, Droplets Droplets and aerosols
– Portal of entry: Eye, mouth– Portal of Entry: Respiratory tract – Sources: Aerosols generated by nebuliser, cough..
Special Attentions to: – Environment decontamination, esp. after spillage– Patient specimens handling
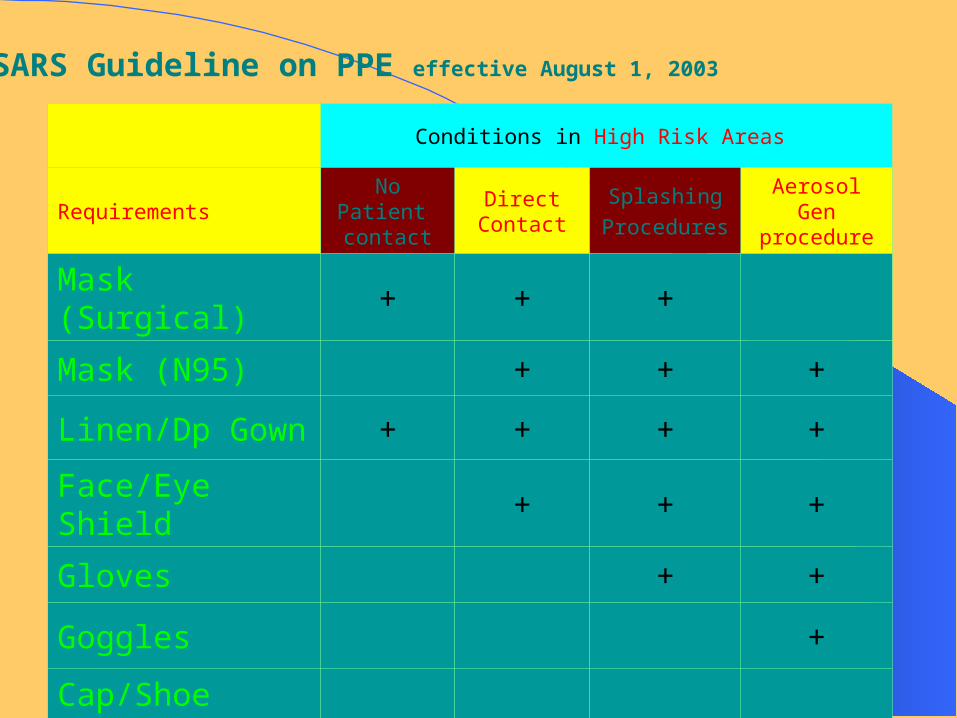
Conditions in High Risk Areas
RequirementsNo Patient contact
Direct Contact
SplashingProcedures
Aerosol Gen procedure
Mask (Surgical) + + +Mask (N95) + + +
Linen/Dp Gown + + + +
Face/Eye Shield + + +Gloves + +
Goggles +
Cap/Shoe cover
SARS Guideline on PPE effective August 1, 2003

Conditions in Non-High Risk Areas
RequirementsNo Patient contact
Direct Contact
SplashingProcedures
Aerosol Gen procedure
Mask (Surgical) + + + +Mask (N95) +
Linen/Dp Gown + +
Face/Eye Shield + +Gloves + +
Goggles
Dp Cap
SARS Guideline on PPE effective August 1, 2003(continued)

• Handwashing is most important
• Use alcohol-based hand rub as alternative
• Do not touch mask or face (esp. eyes, nose & mouth) without 1st washing hands thoroughly
• Gloves must be changed after procedure and between patients.
• No wash gloves & double gloves• Wash immediately and thoroughly if
contaminated by patient’s body fluid or excretions
• N95:
• Should be fit checked every time when used.
• Cautions when reuse
Notes on Practices

Notes on Practices ( cont.)
• Barrier-man is NOT recommended• Mask for patients and Visitors with respiratory
symptoms • No visitors in High Risk areas• Limit and register visitors in other areas• Precautions in performing high risk procedures• Portering high risk patients with PPE and
disinfection after use

職 員 初 期 病 徵 預 警 系 統
姓 名 ︰ K O N G , M A N Y I N G
實 際 工 作 地 點
聯 網 K O W L O O N C E N T R A L C L U S T E R
醫 院 Q E H - Q U E E N E L I Z A B E T H H O S P I T A L
專 科 /部 門
病 房 /單 位 工 作 位 置 ( 非 必 要 )
病 徵
染 病 時 段 /病 假 ︰
由 / / 至
/ / ( 日 /月 /年 )
發 燒 ( 攝 氏 3 7 . 5 度 或 以 上 )
發 冷 ( 在 室 溫 下 全 身 顫 抖 )
流 鼻 水 ( 從 鼻 腔 流 出 水 狀 的 分 泌 物 )
乾 咳
有 痰 的 咳
喉 嚨 痛 ( 喉 嚨 有 火 燒 的 感 覺 )
肌 肉 酸 痛 ( 肌 肉 疼 痛 , 酸 痛 的 感 覺 )
X光 肺 片 有 陰 影
腹 瀉 ( 每 天 排 出 稀 爛 或 水 狀 的 大 便 多 過 三 次 )
入 院 治 療
是
否
住 院 名 稱 ︰
其 他 醫 院 ︰
非 典 型 肺 炎 血 清 測 試
測 試 已 送 出
沒 有 做 測 試 不 清 楚
測 試 日 期 ︰ / / ( 日 /月 /年 )
化 驗 室 名 稱 ︰
有 多 少 家 庭 成 員 有 類 似 病 徵 ︰ 0
表 單 的 底 部

Sick staff profile at Paediatrics department on 24/9/03
WorkplaceStaff nameRank Resp.Inf. Fever G.I.Inf. Attend Sick Date
no. ofsick
leave Remarks:CHEUNG WAN SZEEN Cough,
runningnose
No GP 24/09/2003 1
LEUNG HOI YEERN No Diarrhoea GP 24/09/2003 1LEUNG WING YANRN Cough,
runningnose,SOB dueto asthma
37.2c - 37.5c GP 24/9/2003 - 25/9/20032 Call backto AEDRS clinic
HUI SUK YIN MANDYFamily MedSorethroat,musclepain
Yes 2003/9/23-2003/9/242 Call backto AEDRS clinic
TANG SAU SHEKMO Headache,sore throat
No 24/09/2003 1
Staff Infectious Sickness Surveillance

HA Outbreak Response PlanHA Outbreak Response Plan Outbreak: An increase of infection above the normal level, for that period and in that place.
Alert Conditions Actions
GREEN
Abnormal pattern in Community/Hosp. Guidelines in place Local actions are adequate e.g. Scabies outbreak, ILI in OAH
outbreak investigation local measures CCE/HCE in command HAHO & DH notified
YELLOW
Abnormal pattern with territory-wide implications/ HA response is needed e.g. H5N1 avian Flu
Alert Duty Microbiologist & chairman of HA CCID HA Director in command HCE liaise DH on control
RED Outbreak has widespread territory wide implications e.g. SARS Alert, re-emergence of SARS
CE in command HA Central Command Committee activated

Management of NoroviManagement of Norovirus outbreakrus outbreak

Family Caliciviridae Genus: Noroviruses
– 4 genotypes Other names:
– Norwalk-like viruses (NLV), after the strain responsible for an outbreak of GE infection in a school in Norwalk, Ohio, USA in 1968
– Small Round Structured Viruses (SRSV). Survives freezing, temperatures as high as
60ºC, up to 10 ppm chlorine
The virus
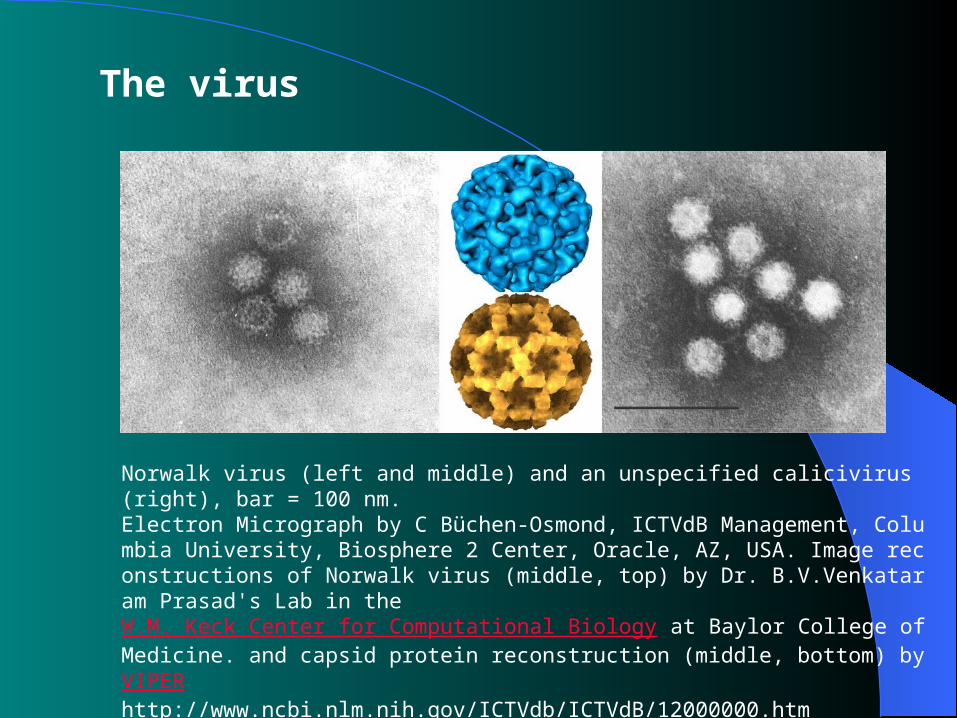
Norwalk virus (left and middle) and an unspecified calicivirus (right), bar = 100 nm. Electron Micrograph by C Büchen-Osmond, ICTVdB Management, Columbia University, Biosphere 2 Center, Oracle, AZ, USA. Image reconstructions of Norwalk virus (middle, top) by Dr. B.V.Venkataram Prasad's Lab in the W.M. Keck Center for Computational Biology at Baylor College of Medicine. and capsid protein reconstruction (middle, bottom) by VIPERhttp://www.ncbi.nlm.nih.gov/ICTVdb/ICTVdB/12000000.htm
The virus

Management of Norovirus OutbreakManagement of Norovirus Outbreak
All age groups are susceptible. The disease usually occurs as
epidemics in winter (winter vomiting disease).
Outbreaks in nursing homes, restaurants, cruise ships and schools.

Recent outbreaks in November 2003:Recent outbreaks in November 2003: 5-17 Nov: Sacred Heart Cannosian School
(277/1835 students) 10-14 Nov: ESF-QBS (51/732 students;
0/60 staff) 11-12 Nov: PWH-7C ward (6 of 34
inpatients, 0/20 staff) 14-16 Nov: DDU, CMC (16/64 inmates;
4/30 staff) 12-18 Nov: TKO, HKSPC-SWSM Day Centre
(27/112 children; 0/16 staff)

Route & mode of Route & mode of transmissiontransmission
Foodborne disease – contaminated food or drink by food handler or
at source which usually are shellfish e.g. oyster
Person to person faecal-oral route aerosolization of vomitus (especially in institut
es such as nursing homes or day care centres) Contact of contaminated environment
patient environment / swimming pool or fomite

TransmissibilityTransmissibility The infective dose can be less than 100 Aerosolization of vomitus leading to
extensive environmental contamination by droplets, resulting in secondary spread among contacts is common.
Shedding begins with onset of symptoms Shedding might continue for 2 weeks after
recovery

Clinical featuresClinical features Incubation period: 12 - 50 hours. Presenting symptoms:
Acute onset Vomiting Watery non-bloody diarrhoea, with abdominal cram
p Nausea Low grade Fever may be present.
Dehydration may occur in the young elderly. Symptoms last for 1-3 days with no chronic seq
ualae.
DiagnosisDiagnosisOutbreak suggestive of viral origin
(Kaplan’s criteria)– Illness duration 12-60 hrs.– Incubation period 24-48 hrs.– >50% people with vomiting– No bacterial agents found.

DiagnosisDiagnosisRT-PCR on specimens of:
– Stool– Vomitus– Environmental samples
Electron microscopy: insensitive. Culture and serology: Not
available.

Preventive Measures Preventive Measures
Heighten vigilance on Gastroenteritis– Information of community outbreak from D
H – Cluster of GE should be reported to HAHO a
nd Regional Office of DH – Fact sheet on Norovirus should be widely pr
omulgated to hospital staff. – Briefing sessions for frontline staff

Preventive Measures Preventive Measures
Clinical Awareness on Gastroenteritis– Compatible CF, patients from institutes,
OAH or school clusters– Inform ICT– Laboratory diagnosis for enteric pathoge
ns, and vomitus/stool for Norovirus PCR by GVU-DH
Preventive Measures Preventive Measures
Enhance infection control measures– Isolate suspected cases – Ensure a stringent infection control;– Hand washing is the most important measure
s; – Extensive disinfection (Na hypocholorite 1:4
9 dilution) of environment and objects;– Visitors should adopt similar precautions

Preventive MeasuresPreventive Measures
Wards with hospital acquired gastroenteritis outbreak should – stop all admissions and discharges – surveillance on both staff and patients for 3
days from the date of onset of last patient

Preventive Measures Preventive Measures
Ensure provision of appropriate PPE to staff– gloves, disposal gowns, and surgical masks in
direct contact with patients' vomitus or excreta;– During the cleansing of vomitus or excreta, put
on face shield;– Caring patients with on-going vomiting attack,
put on face shield to prevent inoculation of droplets onto mucosal surfaces.

High Risk AreasHigh Risk AreasAED, Paediatrics, Medical, Long-stayAdditional measures:
– Bag for anticipated vomiting;– Increase frequency and intensity of routine clea
nsing;– Early reporting of vomiting among staff– Strict hygienic measures in food and potable wa
ter handling







