

Dr Shaikh Mohd MudassirDNB AnaesthesiaSaifee Hospital, Mumbai.

Intra and post operative nausea and vomiting(IONV& PONV) are common during caesarean delivery.
Incidence of IONV has been reported to be 60-80% as per various studies.

Multifactorial
Progesterone induced reduction in lower esophageal sphincter(LOS) tone.
Increased intra gastric pressure.
Hypotension
Exteriorization of uterus.
Visceral stimulation.
Use of neuraxial opiods


Prokinetic drug.
Increases tone of lower esophageal sphincter
Increase gastric and small intestinal motility
Relaxation of pylorus and duodenum during stomach contraction
Antidopaminergic action at chemoreceptor trigger zone
At higher doses has antiserotonergic activity
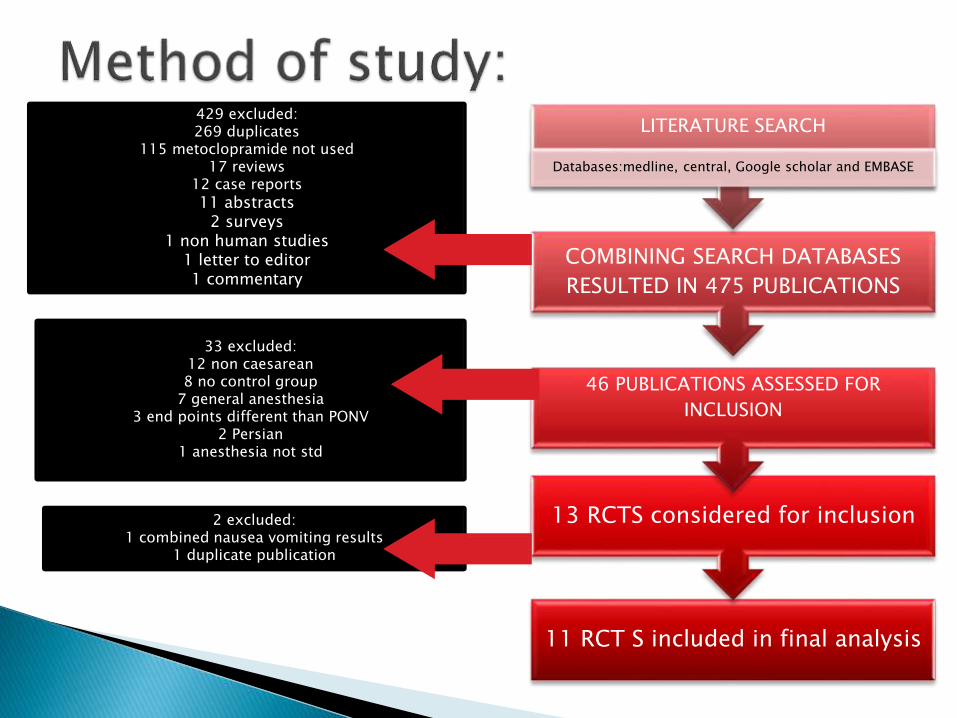
11 RCT S included in final analysis
13 RCTS considered for inclusion
46 PUBLICATIONS ASSESSED FOR
INCLUSION
COMBINING SEARCH DATABASES
RESULTED IN 475 PUBLICATIONS
LITERATURE SEARCH
Databases:medline, central, Google scholar and EMBASE
429 excluded:269 duplicates
115 metoclopramide not used17 reviews
12 case reports
11 abstracts2 surveys
1 non human studies1 letter to editor1 commentary
33 excluded:12 non caesarean8 no control group
7 general anesthesia3 end points different than PONV
2 Persian1 anesthesia not std
2 excluded:1 combined nausea vomiting results
1 duplicate publication

Total 11 studies were included in final analysis.
Total number of patients were 702(349 received metoclopramide and 353 received placebo)
Spinal anesthesia was used in nine studies and epidural in two studies
Metoclopramide was used in a dose of 10mg before block placement in 4 studies and after clamping umbilical cord in seven studies

In three studies where perinorm was given before block placement, there was statistically significant reduction in incidence of ION& IOV(RR 0.27;95% CI 0.16,0.45)

In six studies where perinorm was used after delivery, four used spinal anesthesia and two used epidural anesthesia. Pooled results from these six studies showed statistically significant reduction in incidence of post delivery ION & IOV in metoclopramide group(RR 0.38;95% CI 0.20,0.75).

•Only one study where perinorm was given before block placement reported on use of rescue antiemetic with no difference between the groups.
• In two studies where perinorm was given after clamping the cord there was statistically significant reduction in use of rescue antiemetic treatment when compared to placebo.

Three studies reported on early post operative nausea and vomiting. Spinal was used in two studies and epidural in one study. combining results of all three studies showed statistically significant reduction in incidence of PON & POV in metoclopramide treated patients.
Extra pyramidal side effects were evaluated in six studies, with no reported occurrence in any patients.
Sedation was studied in three studies with no difference in the two groups.
Anxiety scores were similar in both study and control groups

This meta-analysis suggests that the administration of metoclopramide causes a significant reduction in the incidence of IONV & PONV in women undergoing cesarean section under neuraxial anesthesia with no significant side effects.
In general surgical population the anti emetic effects of metoclopramide in a dose of 10mg are uncertain with 50% studies reporting this dose to be no better than placebo. Higher doses of 20-50mg ,however were reported to be effective.

•The reasons for this difference are unclear, but may be related to the impact of physiological changes in pregnancy. Metoclopramide increases the tone of lower esophageal sphicter,which is reduced during pregnancy which accounts for higher incidence of reflux in these patients. since reflux is associated with nausea the increase in LOS with metoclopramide might account for its effective anti emetic effect in this patient population.
•Furthermore its Prokinetic effect decreases gastric volume.

The review suggests that the administration of metoclopramide in a dose of 10mg is effective, safe and cost effective for the prophylaxis against IONV&PONV in parturient undergoing LSCS under neuraxial anesthesia.

Thank you







