
Mineral trioxide aggregate: presentand future developmentsJOSETTE CAMILLERI
Portland cement is used in the building industry to make concrete. It is hydraulic and thus it develops its
properties well in the presence of moisture. The oral environment is inherently wet, however, all dental
materials need a dry field for optimal performance. A mixture of Portland cement and bismuth oxide was
developed and marketed as mineral trioxide aggregate (MTA). The first formulation was gray in color
followed by a white version and eventually by various similar materials, which are all composed of a
tricalcium silicate-based cement and radiopacifier. The MTA was originally suggested for particular clinical
uses, such as root-end filling and perforation repair, where maintenance of a dry field is difficult. The
suggested uses were extended to apexification and dressing over pulpotomies, pulp capping and also as a
sealer cement. The multipurpose use of MTA necessitated the development of improved formulations
where material additives were included to the original cement/radiopacifier formulation. These additives
supposedly enhance the material’s properties and improve its function. Furthermore, the original Portland
cement formulation was replaced with tricalcium silicate to avoid the inclusion of an aluminum phase and
eliminate the inclusion of trace elements. The bismuth oxide was also replaced with alternative
radiopacifiers. The multifaceted use of MTA allows the material to come into contact with different oral
environmental conditions, including blood, saliva, tissue fluids, dental restorative materials, tooth structure
and even air. These different conditions affect the properties and setting of the material. Future
developments should further investigate the material’s interactions and strive to create materials which are
suited to a specific use.
Received 6 March 2015; accepted 22 March 2015.
Introduction
Mineral trioxide aggregate is a mixture of Portland
cement and bismuth oxide. The physical properties
of most dental materials deteriorate when in contact
with moisture. Portland cement, used in the con-
struction industry, has hydraulic properties and was
therefore introduced as a dental material in order to
counteract this problem. The bismuth oxide was
added to Portland cement to enhance the material’s
radiopacity (1).
Portland cement is manufactured from limestone
and shale. These raw materials are burnt in a kiln to
produce tricalcium silicate, dicalcium silicate, and tri-
calcium aluminate. Other trace oxides, namely mag-
nesium oxide and phosphorous pentoxide, are
commonly found with calcium carbonate mineral
deposits. Other accessory oxides in Portland cement
are sodium oxide, potassium oxide, titanium oxide,
manganese oxide, nickel oxide, barium oxide, chro-
mium oxide and fluoride. These are usually in quan-
tities lower than 0.5%, and many lower than 100
ppm. The sodium oxide, potassium oxide, sulfates
(from the raw materials or fuel) and fluoride act as
fluxing agents, reducing the firing temperature for
Portland cement and therefore reducing the cost of
the cement production. Traces of arsenic, lead and
chromium are also present in the material (2). The
clinker is interground with calcium sulfate thus
forming Portland cement.
The first reported use of Portland cement in
dental literature dates to 1878, when Dr. Witte in
31
Endodontic Topics 2015, 32, 31–46All rights reserved
© 2015 John Wiley & Sons A/S.
Published by John Wiley & Sons Ltd
ENDODONTIC TOPICS
1601-1538

Germany published a case report on using Portland
cement to fill root canals (3). Portland cement was
invented in 1824 by Joseph Aspdin in England.
Over a century later Dr. Mahmoud Torabinejad at
Loma Linda University and his co-inventor Dean
White obtained two US patents (4,5) for a Portland
cement-based endodontic material, which became
known as Mineral Trioxide Aggregate (MTA).
The original MTA was dark gray in color and
was commercialized as ProRoot� MTA (Dentsply,
Tulsa Dental, Johnson City, TN, USA) in 1998. In
2002, the “tooth-colored ProRoot MTA” was
introduced and later patented (6). The gray and
white versions of ProRoot MTA have similar com-
positions, but the tooth-colored ProRoot MTA
uses white Portland cement, which contains less
iron. Iron is part of the calcium alumino-ferrite
phase in Portland cement. During manufacture the
ferrite phase functions as a fluxing material, thus
keeping the temperatures during clinkering low,
and results in a more efficient manufacturing pro-
cess. Clinkering of white cement requires the addi-
tion of a fluxing agent. Usually alumino-silicate is
added to the raw feed and allows material clinker-
ing at low temperatures. Regardless of the presence
of alumino-silicate in the white cement, the bio-
compatibility of the gray and white versions has not
been altered (7). However, in contrast other
researchers have reported that white MTA exhibited
less biocompatibility when tested using osteosar-
coma cells than the gray version (8).
Composition of the unhydratedmaterial
The original MTA patents were registered in 1993
and 1995 (4,5) and stated, ‘MTA consists of 50-75%
(wt) calcium oxide and 15-25% silicon dioxide. These
two components together comprise 70-95% of the
cement. When these raw materials are blended, they
produce tricalcium silicate, dicalcium silicate, trical-
cium aluminate, and tetracalcium aluminoferrite’.
They also stated, ‘MTA is Type 1 Portland cement
(American Society for Testing Materials), with a fine-
ness (Blaine number) in the range of 4500-4600 cm2/
g. A radiopacifier (bismuth oxide) is added to the
cement for dental radiological diagnosis’.
Scanning electron microscopy (SEM) of polished
sections of unhydrated MTA embedded in resin shows
distinctive cement grains and bismuth oxide particles,
which are separated from one another. This feature
indicates that the material is composed of a simple mix-
ture of the two components (Fig. 1). The elemental
composition of MTA as shown by energy dispersive
spectroscopy (EDS) indicates the presence of calcium,
silicon and oxygen with minor peaks for aluminum,
potassium, magnesium and bismuth.
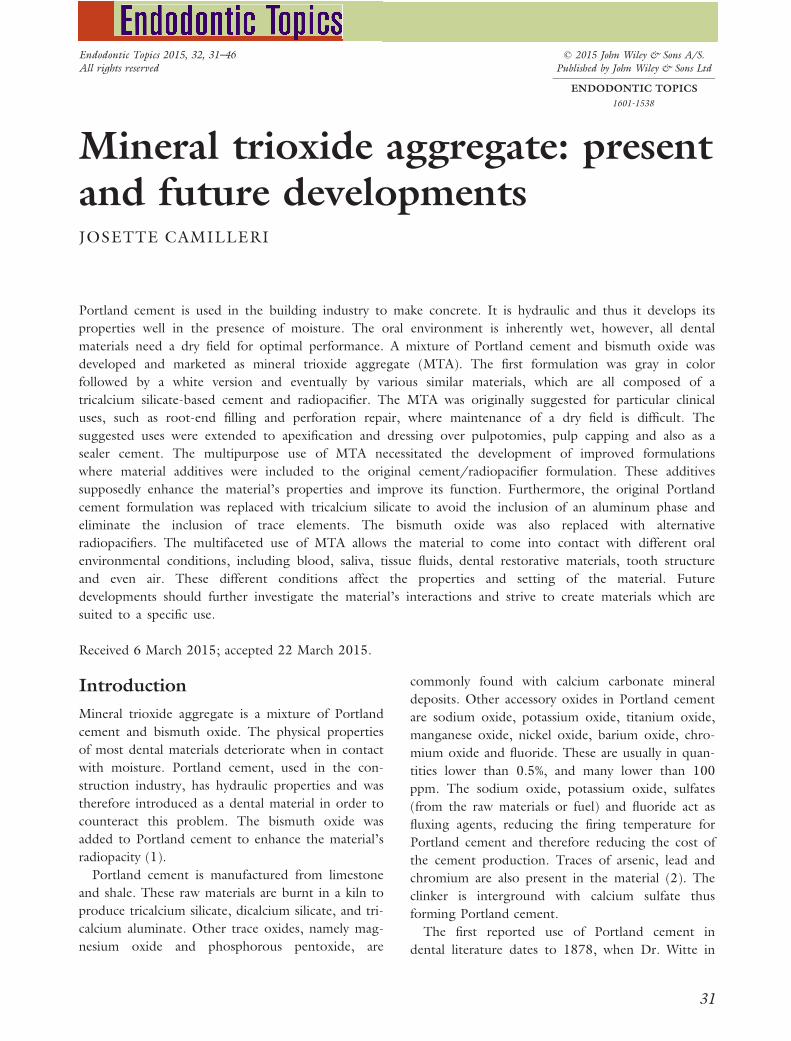
The phases present in MTA are determined by
X-ray diffraction analysis. Using this method of
analysis, unhydrated MTA exhibits peaks for trical-
cium silicate, dicalcium silicate and bismuth oxide.
Using a copper Ka tube, each phase has a particular
pattern, as shown in Figure 2, which can be subse-
quently searched and matched with data derived
from the International Centre of Diffraction. MTA
contains other phases such as dicalcium silicate and
tricalcium aluminate in minimal quantities. X-ray
diffraction analysis of MTA eliminates the myth that
MTA is composed mainly of oxides. Thus, the term
“trioxide aggregate” is essentially a misnomer. In
the first publication on MTA composition, calcium
phosphate was stated to be the main constituent of
MTA (9). In the publication, MTA was purportedly
reported to be composed of “calcium oxide and
calcium phosphate. Further analysis demonstrated
that the former appeared as discrete crystals and the
latter as an amorphous structure with no apparent
crystal growth but a granular appearance. The mean
value of the prisms was 87% calcium and 2.47% sil-
ica, the remainder being oxygen. In areas of amor-
phous structure, there seemed to be 33% calcium, 49%
Fig. 1. Back scatter scanning electron micrograph ofpolished surface of MTA powder 800X magnification.Reproduced from Camilleri (11).
32
Camilleri
phosphate, 2% carbon, 3% chloride, and 6% silica”.
This was discredited in a later publication where it
was shown that the phosphate phase was due to
material contamination from processing for SEM
evaluation (10).
Setting reaction
Mineral trioxide aggregate hydrates when it comes
into contact with water and undergoes two main
reactions. The tricalcium silicate and dicalcium sili-
cate react with water to form calcium silicate hydrate
and calcium hydroxide. The tricalcium aluminate
reacts with water, and in the presence of calcium sul-
fate initially produces ettringite. When the sulfate
containing phases are depleted, a monosulfate phase
is formed (11, 12).
The reactions that occur in MTA after hydration
are the same reactions which are seen in Portland
cement. During the initial stages of the reaction,
calcium silicate hydrate is formed, coating the
cement particles and preventing further reactions.
Tricalcium aluminate dissolves and reacts with the
calcium and sulfate ions present in the liquid phase
to produce ettringite, which also precipitates on the
cement particle surface. The initial phase is followed
by a dormant period, wherein the hydrate coating
on the cement grains prevents further hydration.
The dormant period lasts for 1-2 hours, which is a
period of relative inactivity and the cement is plastic
and workable. Following the completion of the dor-
mant period, setting of the cement proceeds to the
acceleration stage, where the hydration process accel-
erates again. The rate of tricalcium silicate hydration
increases and more calcium silicate hydrate gel is
formed. Hydration of dicalcium silicate also increases
at this stage. Sulfate ions are depleted and
monosulfate forms from ettringite. Crystalline
calcium hydroxide also precipitates from the liquid
phase (11).
Fig. 2. X-ray diffractogram of unhydrated MTA showing the main phases present.
2ð3CaO.SiO2Þ þ 6H2O �! 3CaO.2SiO2:3H2Oþ 3Ca(OH)2tricalcium silicate + water calcium silicate hydrate + calcium hydroxide
2ð2CaO.SiO2Þ þ 4H2O �! 3CaO.2SiO2:3H2Oþ Ca(OH)2dicalcium silicate + water calcium silicate hydrate + calcium hydroxide
3CaO.Al2O3 þ CaSO4 þH2O �! 3CaO.Al2O3:3CaSO4:31H2Otricalcium aluminate + gypsum + water ettringite
33
MTA: present and future developments

Reaction by-products produced upon hydration of
the cement are deposited around the periphery of
the unhydrated cement particles. As hydration pro-
ceeds, there is evidence of more reaction by-products
(11,13). The hydration reaction takes several years
to complete, although the cement mass would have
achieved the final hardening and maximum physical
and mechanical properties by 28 days. Hydrating
MTA can be observed on back-scatter scanning elec-
tron micrographs of polished cement specimens
(Fig. 3a). The formation of cement by-products can
be monitored by scanning electron microscopy. Cal-
cium silicate hydrate exhibits a typical honeycomb
appearance, while calcium hydroxide is deposited in
the form of hexagonal plates (Fig. 3b).
Material hydration can be monitored using X-ray
diffraction analysis, since most of the hydration by-
products are crystalline. As hydration progresses, a
rise in calcium hydroxide peak (ICDD: 44-1481) is
seen at 18 and 34°2h using a copper Ka X-ray radia-
tion. The unhydrated tricalcium silicate phase
(ICDD: 86-0402) at 29.4, 32.1, 32.5, 32.6, 34.3
and 41.2°2h usually reduces in intensity (Fig. 4).
Quantitative measurements of the different phases of
MTA may be performed using Rietveld refinement
of X-ray diffraction plots (Table 1). This quantitative
assessment verifies the reduction in tricalcium silicate
and dicalcium silicate levels of the unhydrated
cement as hydration proceeds with the formation of
calcium silicate hydrate. Calcium hydroxide and low
levels of ettringite are also produced (13).
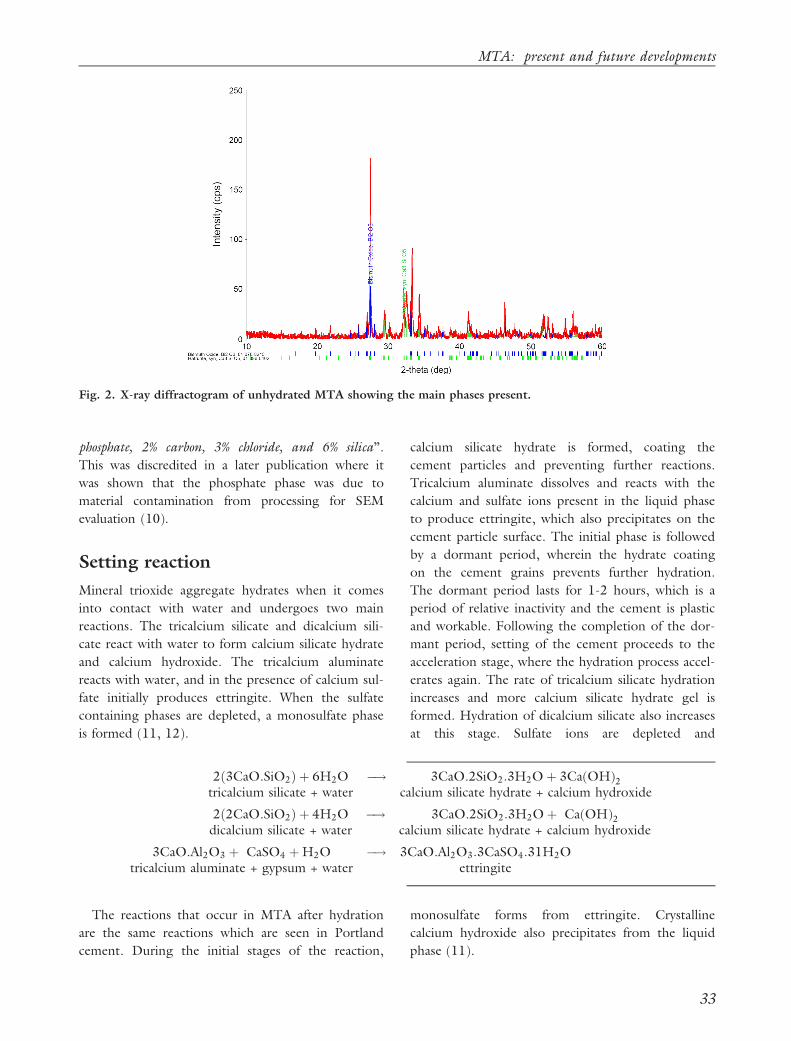
If MTA is left exposed to the environment, the
calcium hydroxide reacts with the atmospheric car-
bon dioxide resulting in the deposition of calcium
carbonate on the cement surface (Fig. 5a). These
deposits are commonly mistaken as being an integral
part of the cement microstructure (7). When in con-
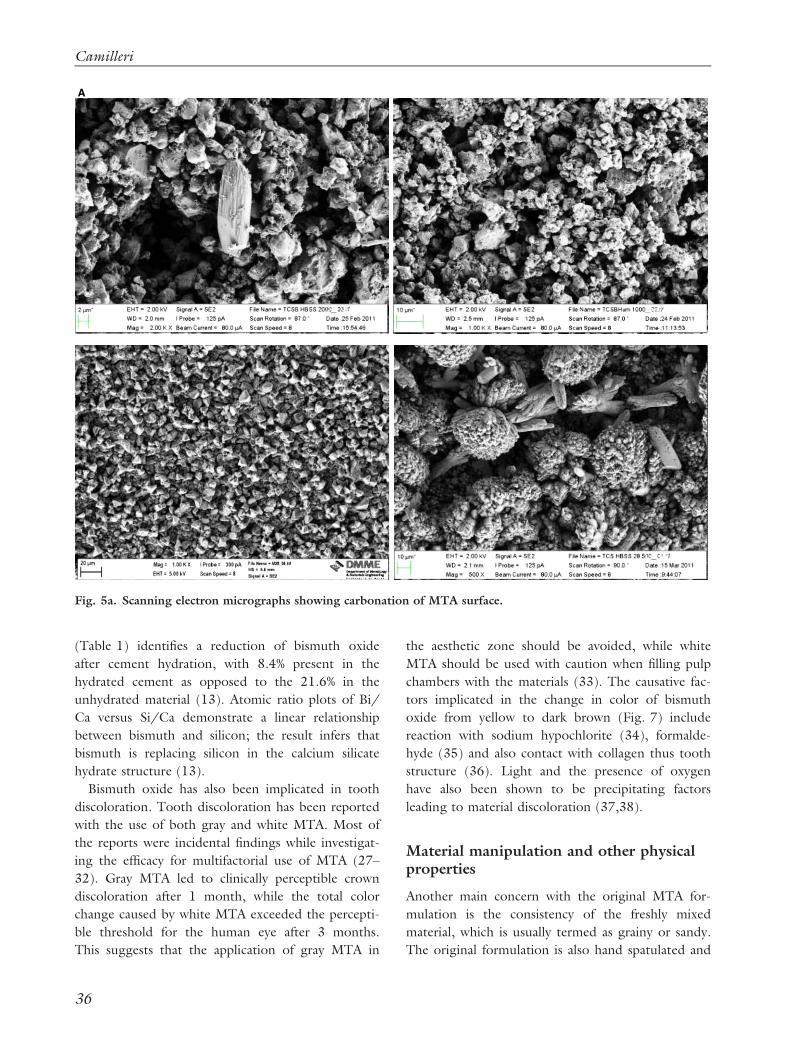
tact with tissue fluids and synthetic tissue fluids,
which contain phosphate ions, the calcium hydroxide
produced, as a by-product of cement hydration,
reacts to form calcium phosphate and is deposited
on the cement surface. Calcium phosphate is crystal-
A
Fig. 3a. Back scatter scanning electron micrograph ofhydrated MTA after immersion for 28 days in watershowing unhydrated cement particle enclosed by a reac-tion rim. Shiny particles are bismuth oxide (X 500mag.).
B
Fig. 3b. Secondary electron scanning electron micro-graph of MTA surface showing calcium silicate hydrate(honeycomb appearance) and calcium hydroxide (hex-agonal plates) deposited on its surface (X 2500 mag.).
Table 1: Quantitative analysis using Rietveld X-raydiffraction of the phases present in unhydrated andhydrated ProRoot MTA. Reproduced from Camilleri(13).
Phases identified
Material type in mass %
Unhydrated Hydrated
Tricalcium silicate 53.1 10.6
Dicalcium silicate 22.5 14.9
Anhydrite 1.5 0.0
Calcium hydroxide 0.0 14.4
Calcium silicate hydrate 0.0 49.5
Ettringite 0.0 2.1
Bismuth oxide 21.6 8.4
34
Camilleri

line and its presence can be demonstrated by X-ray
diffraction analysis (Fig. 5b). The formation of cal-
cium phosphate on the material surface has been
reported to be the reason for the bioactivity shown
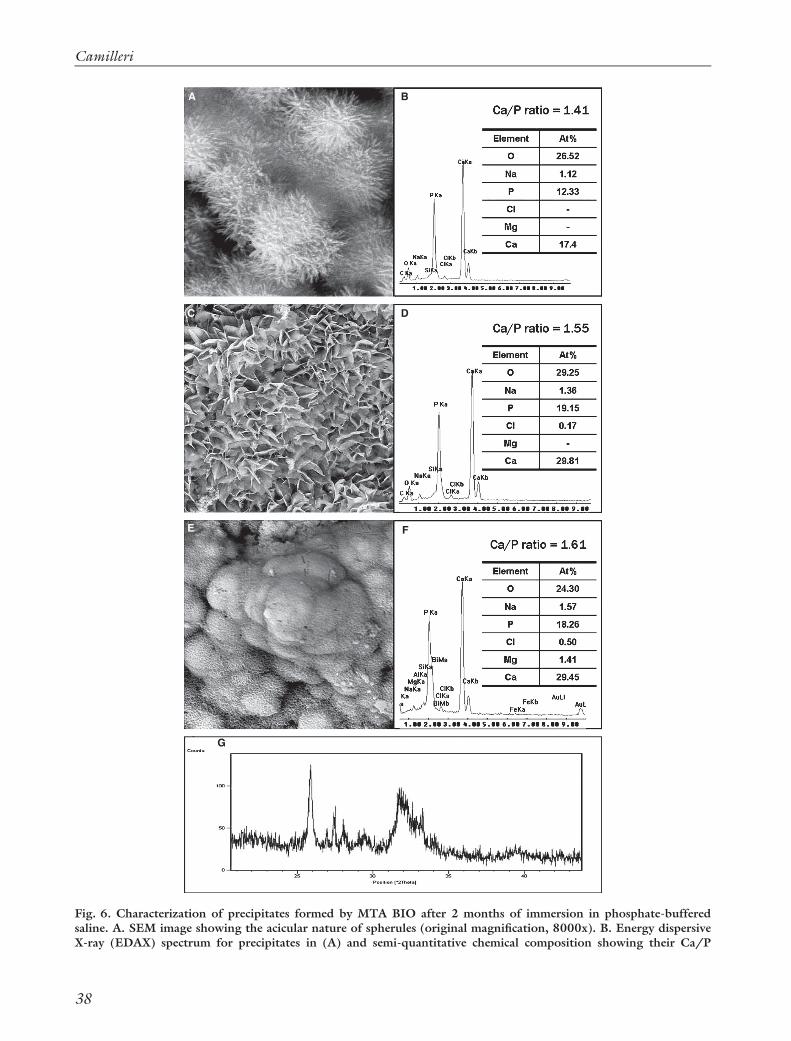
by MTA (Fig. 6). This phenomenon is well
researched (14–18).
Limitations of the originalformulation
The original formulation of MTA is composed of
Portland cement and bismuth oxide in a 4:1 propor-
tion, as specified by the MTA patent (4–6), and mar-
keted by Dentsply as ProRoot MTA, originally as
gray MTA and later as white. Some concerns have
been raised with the original formulation for a num-
ber of reasons and these are listed below.
Trace element inclusion
Since the main constituent of MTA is Portland
cement, some concerns have been raised about the
inclusion of trace elements. Portland cement is man-
ufactured from naturally occurring raw materials in a
kiln. Sometimes, waste materials are used as the raw
materials in the manufacturing of Portland cement
for the construction industry. Additionally, waste
materials are also used as a replacement for primary
fuels in order to keep the manufacturing costs low.
This potentially leads to the inclusion of trace ele-
ments in the final product. Traces of arsenic, lead
and chromium have been reported in both gray and
white MTA (19–25). Although the levels of acid-
extractable trace elements are high, the amounts lea-
ched in the solution are negligible. The inclusion of
heavy metals in Portland cement has raised concerns
regarding its use as a base material for MTA because
when it is applied, the MTA is in contact with both
hard and soft human tissues.
Presence of aluminum
Aluminum is part of the calcium aluminate phase of
the Portland cement. This phase is an integral part
of the cement and cannot be removed as it is pro-
duced during the cement manufacture. Aluminum
is not indorsed in dental and biomaterials due to
risk of Alzheimer’s from excessive exposure to alu-
minum in close contact with the human tissues
(26).
Stability and leaching of bismuth
Bismuth oxide is added to MTA to act as a radiopa-
cifying agent since Portland cement is not sufficiently
radiopaque. Quantitative X-ray diffraction analysis
Fig. 4. X-ray diffractogram of unhydrated and hydrated MTA after 1 and 28 days showing the main phases pres-ent. BO: bismuth oxide, P: Portlandite/calcium hydroxide, TCS: tricalcium silicate.
35
MTA: present and future developments
(Table 1) identifies a reduction of bismuth oxide
after cement hydration, with 8.4% present in the
hydrated cement as opposed to the 21.6% in the
unhydrated material (13). Atomic ratio plots of Bi/
Ca versus Si/Ca demonstrate a linear relationship
between bismuth and silicon; the result infers that
bismuth is replacing silicon in the calcium silicate
hydrate structure (13).
Bismuth oxide has also been implicated in tooth
discoloration. Tooth discoloration has been reported
with the use of both gray and white MTA. Most of
the reports were incidental findings while investigat-
ing the efficacy for multifactorial use of MTA (27–
32). Gray MTA led to clinically perceptible crown
discoloration after 1 month, while the total color
change caused by white MTA exceeded the percepti-
ble threshold for the human eye after 3 months.
This suggests that the application of gray MTA in
the aesthetic zone should be avoided, while white
MTA should be used with caution when filling pulp
chambers with the materials (33). The causative fac-
tors implicated in the change in color of bismuth
oxide from yellow to dark brown (Fig. 7) include
reaction with sodium hypochlorite (34), formalde-
hyde (35) and also contact with collagen thus tooth
structure (36). Light and the presence of oxygen
have also been shown to be precipitating factors
leading to material discoloration (37,38).
Material manipulation and other physicalproperties
Another main concern with the original MTA for-
mulation is the consistency of the freshly mixed
material, which is usually termed as grainy or sandy.
The original formulation is also hand spatulated and
A
Fig. 5a. Scanning electron micrographs showing carbonation of MTA surface.
36
Camilleri
delivery to the operative site is difficult. MTA pre-
sents longer setting time (2 hours and 45 minutes)
in comparison to other retrograde filling materials
such as amalgam, Super-EBA and IRM (9). The
long setting time makes MTA unsuitable for most of
the clinical applications. Different powder-to-water
ratios, which tend to be a frequent occurrence in
clinical practice since the gram supplied is usually
not used in one application, also exerts influence on
MTA’s properties and promoting a longer setting
time (39,40).
Developments
More MTA formulations were introduced after the
ProRoot by Dentsply. The first was introduced by
Angelus, which had both gray and white formula-
tions. The MTA Angelus is also composed of Port-
land cement and bismuth oxide. However the
quantities of tricalcium and dicalcium silicate in
MTA Angelus are different to ProRoot and other
Portland cements (13,41). The difference is due to
variations in the manufacturing of Portland cement,
used as a raw material for preparing MTA. Quantita-
tive phase analysis also showed a percentage of cal-
cium oxide which is responsible for the initial high
heat flux exhibited on calorimetry (41). This calcium
oxide is a result of a raw mix with poor combustibil-
ity and with an unstable thermal profile. Further-
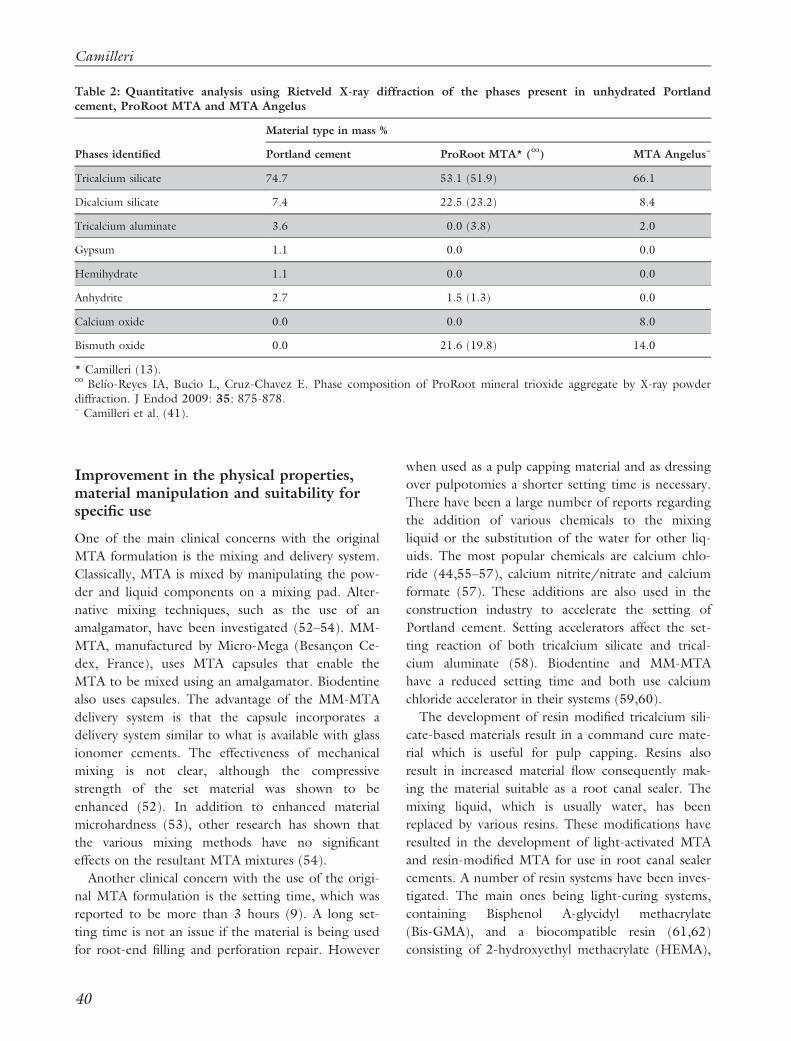
more MTA Angelus was found to contain tricalcium
aluminate but no sulfate-containing phase (Table 2).
The manufacturer claims that the absence of gypsum
reduces the setting time of the material. In fact,
MTA Angelus has been shown to set in less than 50
minutes (42), as opposed to ProRoot MTA which
was reported to have a setting time of over 2 hours
(9,43,44). MTA Angelus also exhibits a lower level
of bismuth oxide when compared to ProRoot MTA
(Table 2) which accounts for the lower radiopacity
of MTA Angelus (18).
More recently, MTA Plus was introduced by an
American company, Avalon Biomed. Both ProRoot
MTA and MTA Angelus were found to have a simi-
lar fineness (1 m2/g) when tested using the Bru-
nauer–Emmett–Teller (BET) gas adsorption method
(12,41). MTA Plus has a specific surface area of
1.537 m2/g, which is higher than the values
obtained for the other MTAs (12). The higher spe-
cific surface area allows more surface availability for
the cement reaction and consequently results in a
more rapid reaction rate.
Replacement of Portland cement
The associated risks to lead, arsenic and chromium
exposure, coupled by the presence of aluminum led
B
Fig. 5b. Glancing angle X-ray diffractogram of MTA analyzing surface deposits on MTA after immersion in waterand Hank’s balanced salt solution for 28 days. In Hank’s balanced salt solution deposits of calcium phosphate wereshown on the cement surface.
37
MTA: present and future developments
A
C D
B
E F
G
Fig. 6. Characterization of precipitates formed by MTA BIO after 2 months of immersion in phosphate-bufferedsaline. A. SEM image showing the acicular nature of spherules (original magnification, 8000x). B. Energy dispersiveX-ray (EDAX) spectrum for precipitates in (A) and semi-quantitative chemical composition showing their Ca/P
38
Camilleri

to the development of materials based on pure trical-
cium silicate. Tricalcium silicate cement is manufac-
tured with laboratory-grade materials using the
sol-gel method. The lack of natural minerals, and
wastes used to fire the kiln, reduces the risk of trace
element contamination.
Materials that use tricalcium silicate as their main
cementious phase include Biodentine and BioAggre-
gate. Tricalcium silicate cement hydrates in a similar
way to Portland cement and produces calcium
hydroxide on hydration (45). The tricalcium silicate-
based materials are collectively known as bioceram-
ics, which distinguishes them from the Portland
cement-based materials and thus signifying a purer
product. In fact, this is incorrect, since the term
ceramics encompasses a wider variety of materials
with a different chemistry.
Replacement of bismuth oxide
The newer MTA variants do not use the bismuth
oxide as radiopacifier. Several alternative radiopacifi-
ers have been investigated and most do not impart
the necessary radiopacity to the final material for-
mulation. Addition of gold powder, silver/tin alloy
(46), barium sulfate (46–48), iodoform (47), zir-
conium oxide (39,47), zinc oxide (46,48), lead
oxide, bismuth subnitrate, bismuth carbonate and
calcium tungstate (48) results in a radiopacity value
of more than 3 mm of the aluminum scale. The
commercial materials use zirconium oxide and tan-
talum oxide. The latter is found in BioAggregate.
Zirconium oxide is found in Biodentine, BioRoot
RCS and EndoSequence BC Sealer and has been
shown to be inert (49). It does not leach and zir-
conium does not take part in the material hydra-
tion to form zirconium-based complexes. Other
alternative radiopacifiers such as barium sulfate and
metallic components, like silver–tin alloys, leach in
to the solution and are therefore not ideal replace-
ments (50). Although gold is inert and imparts
adequate radiopacity, its cost and color limits its
use. Leaching of barium has been demonstrated
from barium zirconate and even when used in
conjunction with tricalcium silicate cement with a
resin matrix (51).
molar ratio. C. SEM image showing petal-like precipitates (original magnification, 1000x). D. EDAX spectrum forprecipitates in (C) revealed a greater Ca/P molar ratio and lattice substitution of Na and Cl. E. SEM image of com-pact lath-like precipitates (original magnification, 1000x). F. Semi-quantitative analysis of the EDAX data derivedfrom (E) indicates that the precipitates have a Ca/P molar ratio of 1.61 with lattice substitution of Na, Cl, andMg. G. X-ray diffraction pattern of the calcium phosphate precipitates obtained after 2 months of immersion inphosphate-buffered saline, revealing the presence of poorly-crystalline apatite. Reproduced from Reyes-Carmona etal. (17).
Fig. 7. Photographs of bismuth oxide powder, ProRoot MTA and Portland cement before and after immersion inthe different solutions. Reproduced from Camilleri (34).
39
MTA: present and future developments
Improvement in the physical properties,material manipulation and suitability forspecific use
One of the main clinical concerns with the original
MTA formulation is the mixing and delivery system.
Classically, MTA is mixed by manipulating the pow-
der and liquid components on a mixing pad. Alter-
native mixing techniques, such as the use of an
amalgamator, have been investigated (52–54). MM-
MTA, manufactured by Micro-Mega (Besanc�on Ce-
dex, France), uses MTA capsules that enable the
MTA to be mixed using an amalgamator. Biodentine
also uses capsules. The advantage of the MM-MTA
delivery system is that the capsule incorporates a
delivery system similar to what is available with glass
ionomer cements. The effectiveness of mechanical
mixing is not clear, although the compressive
strength of the set material was shown to be
enhanced (52). In addition to enhanced material
microhardness (53), other research has shown that
the various mixing methods have no significant
effects on the resultant MTA mixtures (54).
Another clinical concern with the use of the origi-
nal MTA formulation is the setting time, which was
reported to be more than 3 hours (9). A long set-
ting time is not an issue if the material is being used
for root-end filling and perforation repair. However
when used as a pulp capping material and as dressing
over pulpotomies a shorter setting time is necessary.
There have been a large number of reports regarding
the addition of various chemicals to the mixing
liquid or the substitution of the water for other liq-
uids. The most popular chemicals are calcium chlo-
ride (44,55–57), calcium nitrite/nitrate and calcium
formate (57). These additions are also used in the
construction industry to accelerate the setting of
Portland cement. Setting accelerators affect the set-
ting reaction of both tricalcium silicate and trical-
cium aluminate (58). Biodentine and MM-MTA
have a reduced setting time and both use calcium
chloride accelerator in their systems (59,60).
The development of resin modified tricalcium sili-
cate-based materials result in a command cure mate-
rial which is useful for pulp capping. Resins also
result in increased material flow consequently mak-
ing the material suitable as a root canal sealer. The
mixing liquid, which is usually water, has been
replaced by various resins. These modifications have
resulted in the development of light-activated MTA
and resin-modified MTA for use in root canal sealer
cements. A number of resin systems have been inves-
tigated. The main ones being light-curing systems,
containing Bisphenol A-glycidyl methacrylate
(Bis-GMA), and a biocompatible resin (61,62)
consisting of 2-hydroxyethyl methacrylate (HEMA),
Table 2: Quantitative analysis using Rietveld X-ray diffraction of the phases present in unhydrated Portlandcement, ProRoot MTA and MTA Angelus
Phases identified
Material type in mass %
Portland cement ProRoot MTA* (∞) MTA Angelus~
Tricalcium silicate 74.7 53.1 (51.9) 66.1
Dicalcium silicate 7.4 22.5 (23.2) 8.4
Tricalcium aluminate 3.6 0.0 (3.8) 2.0
Gypsum 1.1 0.0 0.0
Hemihydrate 1.1 0.0 0.0
Anhydrite 2.7 1.5 (1.3) 0.0
Calcium oxide 0.0 0.0 8.0
Bismuth oxide 0.0 21.6 (19.8) 14.0
* Camilleri (13).∞ Bel�ıo-Reyes IA, Bucio L, Cruz-Chavez E. Phase composition of ProRoot mineral trioxide aggregate by X-ray powderdiffraction. J Endod 2009: 35: 875-878.~ Camilleri et al. (41).
40
Camilleri

triethylene glycol dimethacrylate (TEGDMA), cam-
phorquinone and ethyl-4-(dimethylamino)benzoate
(EDMAB), with or without polyacrylic co-maeleic
acid (63,64), Bis-GMA, TEGDMA (65) and
Bis-GMA, pyromellitic acid diethylmethacrylate
(PMDM) and HEMA (66). Chemically-cured resins
have also been employed (65,67) and investigated
in vitro. The addition of different resin systems has
shown to alter the hydration mechanism of the
resultant material. Resins are mostly hydrophobic
and limit ion exchange with the surrounding envi-
ronment. This restricts the absorption of fluids and
reduces cement hydration, therefore the calcium
ions, even if formed, would find it difficult to move
along the resin matrix. This modification of hydra-
tion and restricted ion movement has been reported
(51). Thus if hydration is incomplete the use of resin
modified tricalcium silicate is useless as no calcium
hydroxide is released to interact with the pulp.
One light curable tricalcium silicate-based material
marketed for pulp capping is Theracal (Bisco,
Schaumburg, IL, USA). Theracal hydration is
affected by the environmental conditions and fluid
availability. In fact when used as a pulp capping mate-
rial the low fluid availability reduces material hydra-
tion (68). The calcium releasing ability of Theracal is
debatable, in one study it was shown to be compara-
ble to calcium hydroxide (69), while in later investi-
gations no calcium was formed and calcium ion
leaching was shown to be very low compared to
Biodentine (70). Theracal extracts were shown to be
cytotoxic when in contact with pulp cells (71). A
modified MTA-based resin is marketed by Angelus
(Angelus, Londrina, Brazil) as MTA Fillapex. This is
composed of MTA, a salicylate resin (methyl salicy-
late, butylene glycol and colophony) and other addi-
tives. Other proprietary brands such as MTA Obtura
and Endo CPM sealer exist and contain other addi-
tives to the MTA formula which enhances material
flow. In MTA Fillapex, the hydration reaction does
not occur and therefore no calcium hydroxide is lea-
ched to the surrounding tissues (72).
Material flow can be enhanced by the addition of
water-soluble polymers (73–76) as shown in proto-
type materials. ProRoot Endo Sealer is a commercial
formulation using cement particles dispersed in a
water-soluble polymer (77,78). The water-soluble
polymer creates a charge on the cement particles,
resulting in the repulsion of these charged particles,
with reduced flocculation and increased material flow
at low water/cement ratios (58). Biodentine and
BioRoot RCS are both manufactured by Septodont
and have a water soluble polymer which improves
the material handling. Propylene glycol, another sol-
uble polymer, has also been used to improve MTA
flow (79).
Other polymers have been included to reduce the
washout of the unset cement. Anti-washout liquid is
included in the MTA Plus formulation (Avalon Bio-
med Inc., Bradenton, FL, USA). Washout refers to
the tendency of a freshly prepared cement paste to
“disintegrate upon early contact with blood or other
fluids” (80) and is one of the disadvantages of MTA
after it is placed in situ. The addition of an anti-
washout liquid to MTA Plus reduces washout con-
siderably when compared to MTA Angelus (81).
Intermediate Restorative Material (IRM) and dental
amalgam exhibit no washout (82).
Most of the newer formulations contain additives
which enhance material properties. Both Biodentine
and MM-MTA include calcium carbonate and is a
component of Portland cement when used in the
building industry. The addition of calcium carbonate
reduces the material costs and acts as a nucleating
agent, thus enhancing hydration. This has been
demonstrated for Biodentine, where the hydration
product was shown to deposit around the calcium
carbonate particles (83,84). In MM-MTA the cal-
cium carbonate changes the hydration reaction.
Since MM-MTA is Portland cement-based it con-
tains an aluminate phase. The calcium carbonate
affects the formation of ettringite, which is a by-
product of the hydration of tricalcium aluminate,
calcium sulfate and water during hydration, conse-
quently modifying the hydration process. During the
formation of ettringite, the sulfate ions are replaced
by carbonate ions producing calcium carbosilicate
and calcium carboaluminate (60). Calcium carbonate
has been also shown to impede crystallization of cal-
cium hydroxide. In fact no formation of calcium
hydroxide was demonstrated for MM-MTA (60).
BioAggregate, EndoSequence BC Sealer and the
material range from Brasseler contains calcium phos-
phate monobasic (84,85). There is no literature on
the effect of adding phosphate containing materials
to tricalcium silicate-based materials, however a
reduction in the formation of calcium hydroxide
over a period of 28 days was demonstrated for Bio-
41
MTA: present and future developments

aggregate (84). MTA Fillapex contains microsilica,
which affects the hydration of Portland cement. It
reacts with the calcium hydroxide produced during
hydration and forms more calcium silicate hydrate in
the long term and improves the material properties
at the expense of calcium hydroxide formation.
However, MTA Fillapex does not produce calcium
hydroxide as shown by X-ray diffraction analysis
(72). The different additives may potentially affect
the cyto-compatibility of the materials since different
calcium silicate-based materials exhibited different
cytotoxicity to human gingival fibroblasts (85).
Material use and effect of environmentalconditions
Although MTA is a hydraulic material, when used in
clinical dentistry it never comes in contact with
water. The material has been suggested for use as a
root-end filling material, for perforation repair, apex-
ification and pulpotomy procedures and also as a
pulp capping material (87). More recently MTA has
also been developed as a root canal sealer. All the
beneficial properties of MTA are related to its
hydraulic nature and the formation of calcium
hydroxide, as a by-product of material hydration.
Each material application brings MTA in contact
with different environments. Blood comes into con-
tact with MTA when it is used for perforation repair,
as a root-end filling material and to a minor extent
in cases of direct pulp capping. Blood interferes with
material hydration and reduces the MTA microhard-
ness (88–90). Tissue fluids and serum also affect
material properties (91) and failure of material set-
ting (92). The phosphates present in tissue fluids
have been implicated in material bioactivity, as reac-
tion of calcium hydroxide with phosphates results in
the formation of hydroxyl-apatite on the material
surface (14–16). However phosphates have also been
shown to interfere with material setting (12).
The interaction with pulp and dentin also provides
an interesting and beneficial phenomena. MTA
induces pulp healing and regeneration (93). How-
ever MTA does have several drawbacks. The flexural
strength of the tooth when in contact with MTA
was reduced (94) and MTA’s interaction with colla-
gen also caused tooth discoloration. (36). Further-
more the long setting time of MTA makes unset
MTA come in contact with other dental materials
affecting the material hydration and setting (95,96).
The development of tricalcium silicate root canal
sealers is based on the hypothesis of the interaction
of dentin with the tricalcium silicate and biominerali-
zation, consequently forming dentin tags. This is
postulated for the hydrated material. MTA Fillapex
does not produce calcium hydroxide after it sets. En-
doSequence, and materials which are hybrids of tri-
calcium silicate and calcium phosphate, may not
produce calcium hydroxide in the long term. Thus
the hypothesis of biomineralization may be errone-
ous. MTA and related materials are affected by vari-
ous irrigants used during root canal treatment (97),
particularly EDTA which is a calcium chelator (98).
Material and tooth discoloration will result from the
interaction of sodium hypochlorite with bismuth
oxide in MTA (34).
Conclusions
For the past two decades MTA and tricalcium silicate
cement-based materials have become a mainstay in
clinical dentistry and are used for a variety of clinical
applications. The original formulation and modified
cements are still used in these applications. The
materials are reactive and additives tend to affect the
hydration process, which can be deleterious to the
material chemistry and resultant properties of the set
material. Furthermore the materials interact with the
oral environment during use, which changes material
microstructure and even demonstrates setting failure.
Future developments in MTA and related materials
should outline first the particular material use and
then tailor-make the material according to the
desired properties.
References
1. Shah PM, Chong BS, Sidhu SK, Ford TR. Radiopacityof potential root-end filling materials. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1996: 81:476–479.
2. Lea FM, Hewlett PC. Lea’s Chemistry of Cement andConcrete, 4th edn. London, New York: Arnold; Co-published in North, Central, and South America by J.Wiley, 1998.
3. Witte. The filling of a root canal with Portlandcement. German Quarterly for Dentistry; J Cent AssocGerman Dent 1878: 18: 153–154.
4. Torabinejad M, White DJ. Tooth filling material andmethod of use. US Patent 5,415,547; 1993.
42
Camilleri

5. Torabinejad M, White DJ. Tooth filling material andmethod of use. US Patent 5,769,638; 1995.
6. Primus CM. Dental material. US Patent 7,892,342;2011.
7. Camilleri J, Montesin FE, Papaioannou S, McDonaldF, Pitt Ford TR. Biocompatibility of two commercialforms of mineral trioxide aggregate. Int EndodJ 2004: 37: 699–704.
8. P�erez AL, Spears R, Gutmann JL, Opperman LA. Os-teoblasts and MG-63 osteosarcoma cells behave differ-ently when in contact with ProRoot MTA and WhiteMTA. Int Endod J 2003: 36: 564–570.
9. Torabinejad M, Hong CU, McDonald F, Pitt FordTR. Physical and chemical properties of a new root-end filling material. J Endod 1995: 21: 349–353.
10. Camilleri J, Montesin FE, Brady K, Sweeney R, CurtisRV, Ford TR. The constitution of mineral trioxideaggregate. Dent Mater 2005: 21: 297–303.
11. Camilleri J. Hydration mechanisms of mineral trioxideaggregate. Int Endod J 2007: 40: 462–470.
12. Camilleri J, Formosa L, Damidot D. The setting char-acteristics of MTA Plus in different environmentalconditions. Int Endod J 2013: 46: 831–840.
13. Camilleri J. Characterization of hydration products ofmineral trioxide aggregate. Int Endod J 2008: 41:408–417.
14. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawa-shima I. Physicochemical basis of the biologic proper-ties of mineral trioxide aggregate. J Endod 2005: 31:97–100.
15. Bozeman TB, Lemon RR, Eleazer PD. Elementalanalysis of crystal precipitate from gray and whiteMTA. J Endod 2006: 32: 425–428.
16. Tay FR, Pashley DH, Rueggeberg FA, Loushine RJ,Weller RN. Calcium phosphate phase transformationproduced by the interaction of the Portland cementcomponent of white mineral trioxide aggregate with aphosphate-containing fluid. J Endod 2007: 33:1347–1351.
17. Reyes-Carmona JF, Felippe MS, Felippe WT. Biomin-eralization ability and interaction of mineral trioxideaggregate and white Portland cement with dentin in aphosphate-containing fluid. J Endod 2009: 35:731–736.
18. Gandolfi MG, Taddei P, Tinti A, De Stefano DorigoE, Rossi PL, Prati C. Kinetics of apatite formation ona calcium-silicate cement for root-end filling duringageing in physiological-like phosphate solutions. ClinOral Investig 2010: 14: 659–668.
19. Duarte MA, De Oliveira Demarchi AC, Yamashita JC,Kuga MC, De Campos Fraga S. Arsenic release pro-vided by MTA and Portland cement. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2005: 99:648–650.
20. Monteiro Bramante C, Demarchi AC, de Moraes IG,Bernadineli N, Garcia RB, Sp�angberg LS, Duarte MA.Presence of arsenic in different types of MTA andwhite and gray Portland cement. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2008: 106: 909–913.
21. De-Deus G, de Souza MC, Sergio Fidel RA, Fidel SR,de Campos RC, Luna AS. Negligible expression ofarsenic in some commercially available brands of Port-land cement and mineral trioxide aggregate. J Endod2009: 35: 887–890.
22. Schembri M, Peplow G, Camilleri J. Analyses of heavymetals in mineral trioxide aggregate and Portlandcement. J Endod 2010: 36: 1210–1215.
23. Matsunaga T, Tsujimoto M, Kawashima T, TsujimotoY, Fujiwara M, Ookubo A, Hayashi Y. Analysis ofarsenic in gray and white mineral trioxide aggregatesby using atomic absorption spectrometry. J Endod2010: 36: 1988–1990.
24. Chang SW, Baek SH, Yang HC, Seo DG, HongST, Han SH, Lee Y, Gu Y, Kwon HB, Lee W,Bae KS, Kum KY. Heavy metal analysis of orthoMTA and ProRoot MTA. J Endod 2011: 37:1673–1676.
25. Camilleri J, Kralj P, Veber M, Sinagra E. Characteriza-tion and analyses of acid-extractable and leached traceelements in dental cements. Int Endod J 2012: 45:737–743.
26. Forbes WF, Gentleman JF. Risk factors, causality, andpolicy initiatives: the case of aluminum and mentalimpairment. Exp Gerontol 1998: 33: 141–154.
27. Liu H, Zhou Q, Qin M. Mineral trioxide aggregateversus calcium hydroxide for pulpotomy in primarymolars. Chin J Dent Res 2011: 14: 121–125.
28. Moore A, Howley MF, O’Connell AC. Treatment ofopen apex teeth using two types of white mineral tri-oxide aggregate after initial dressing with calciumhydroxide in children. Dent Traumatol 2011: 27:166–173.
29. Jacobovitz M, de Pontes Lima RK. The use of calciumhydroxide and mineral trioxide aggregate on apexifica-tion of a replanted tooth: a case report. Dent Trauma-tol 2009: 25: e32–36.
30. Erdem AP, Ozdas DO, Dincol E, Sepet E, Aren G.Case series: root healing with MTA after horizontalfracture. Eur Arch Paediatr Dent 2009: 10: 110–113.
31. Jacobovitz M, de Lima RK. Treatment of inflamma-tory internal root resorption with mineral trioxideaggregate: a case report. Int Endod J 2008: 41:905–912.
32. Dabbagh B, Alvaro E, Vu DD, Rizkallah J, SchwartzS. Clinical complications in the revascularization ofimmature necrotic permanent teeth. Pediatr Dent2012: 34: 414–417.
33. Ioannidis K, Mistakidis I, Beltes P, Karagiannis V.Spectrophotometric analysis of coronal discolorationinduced by gray and white MTA. Int Endod J 2013:46: 137–144.
34. Camilleri J. The color stability of white mineral triox-ide aggregate in contact with sodium hypochloritesolution. J Endod 2014: 40: 436–440.
35. Marciano MA, Camilleri J, Lia Mondelli RF, PabloAndres Amoroso PA, Cavalini Cavenago B, del CarpioPerochena A, Hungaro Duarte MA. Potential dentalstaining of root canal sealers with formulations con-
43
MTA: present and future developments

taining bismuth oxide and formaldehyde. ENDO-End-odontic Practice Today 2015: in press.
36. Marciano MA, Costa RM, Camilleri J, Mondelli RF,Guimar~aes BM, Duarte MAH. Assessment of colorstability of white MTA Angelus and bismuth oxide incontact with tooth structure. J Endod 2014: 40:1235–1240.
37. Vall�es M, Mercad�e M, Duran-Sindreu F, Bourde-lande JL, Roig M. Color stability of white mineraltrioxide aggregate. Clin Oral Investig 2013: 17:1155–1159.
38. Vall�es M, Mercad�e M, Duran-Sindreu F, BourdelandeJL, Roig M. Influence of light and oxygen on thecolor stability of five calcium silicate-based materials.J Endod 2013: 39: 525–528.
39. Cutajar A, Mallia B, Abela S, Camilleri J. Replacementof radiopacifier in mineral trioxide aggregate; charac-terization and determination of physical properties.Dent Mater 2011: 27: 879–891.
40. Cavenago BC, Pereira TC, Duarte MA, Ordinola-Zapata R, Marciano MA, Bramante CM, Bernard-ineli N. Influence of powder-to-water ratio on ra-diopacity, setting time, pH, calcium ion releaseand a micro-CT volumetric solubility of whitemineral trioxide aggregate. Int Endod J 2014: 47:120–126.
41. Camilleri J, Sorrentino F, Damidot D. Investigation ofthe hydration and bioactivity of radiopacified trical-cium silicate cement, Biodentine and MTA Angelus.Dent Mater 2013: 29: 580–593.
42. Massi S, Tanomaru-Filho M, Silva GF, Duarte MA,Grizzo LT, Buzalaf MA, Guerreiro-Tanomaru JM.pH, calcium ion release, and setting time of an experi-mental mineral trioxide aggregate-based root canalsealer. J Endod 2011: 37: 844–846.
43. Ber BS, Hatton JF, Stewart GP. Chemical modifica-tion of ProRoot MTA to improve handling character-istics and decrease setting time. J Endod 2007: 33:1231–1234.
44. Bortoluzzi EA, Broon NJ, Bramante CM, FelippeWT, Tanomaru Filho M, Esberard RM. The influenceof calcium chloride on the setting time, solubility, dis-integration, and pH of mineral trioxide aggregate andwhite Portland cement with a radiopacifier. J Endod2009: 35: 550–554.
45. Camilleri J. Characterization and hydration kinetics oftricalcium silicate cement for use as a dental biomate-rial. Dent Mater 2011: 27: 836–844.
46. Camilleri J, Gandolfi MG. Evaluation of the radiopaci-ty of calcium silicate cements containing different radi-opacifiers. Int Endod J 2010: 43: 21–30.
47. Bortoluzzi EA, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Duarte MA. Radiographic effect of differentradiopacifiers on a potential retrograde filling material.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2009: 108: 628–632.
48. H�ungaro Duarte MA, de Oliveira El Kadre GD, VivanRR, Guerreiro Tanomaru JM, Tanomaru Filho M, deMoraes IG. Radiopacity of Portland cement associated
with different radiopacifying agents. J Endod 2009:35: 737–740.
49. Camilleri J, Cutajar A, Mallia B. Hydration character-istics of zirconium oxide replaced Portland cement foruse as a root-end filling material. Dent Mater 2011:27: 845–854.
50. Camilleri J. Hydration characteristics of calcium sili-cate cements with alternative radiopacifiers used asroot-end filling materials. J Endod 2010: 36:502–508.
51. Camilleri J. Tricalcium silicate cements with resins andalternative radiopacifiers. J Endod 2014: 40: 2030–2035.
52. Basturk FB, Nekoofar MH, G€unday M, Dummer PM.The effect of various mixing and placement techniqueson the compressive strength of mineral trioxide aggre-gate. J Endod 2013: 39: 111–114.
53. Nekoofar MH, Aseeley Z, Dummer PM. The effect ofvarious mixing techniques on the surface microhard-ness of mineral trioxide aggregate. Int Endod J 2010:43: 312–320.
54. Shahi S, Rahimi S, Yavari HR, Samiei M, Janani M,Bahari M, Abdolrahimi M, Pakdel F, Aghbali A.Effects of various mixing techniques on push-outbond strengths of white mineral trioxide aggregate.J Endod 2012: 38: 501–504.
55. Antunes Bortoluzzi E, Ju�arez Broon N, AntonioHungaro Duarte M, de Oliveira Demarchi AC,Monteiro Bramante C. The use of a setting acceleratorand its effect on pH and calcium ion release of mineraltrioxide aggregate and white Portland cement. J En-dod 2006: 32: 1194–1197.
56. Kogan P, He J, Glickman GN, Watanabe I. Theeffects of various additives on setting properties ofMTA. J Endod 2006: 32: 569–572.
57. Wiltbank KB, Schwartz SA, Schindler WG. Effect ofselected accelerants on the physical properties of min-eral trioxide aggregate and Portland cement. J Endod2007: 33: 1235–1238.
58. Paillere AM, Ben Bassat M, Akman S. Applications ofadmixtures for concrete. RILEM Technical Commit-tees; 2002.
59. Camilleri J, Sorrentino F, Damidot D. Investigation ofthe hydration and bioactivity of radiopacified trical-cium silicate cement, Biodentine and MTA Angelus.Dent Mater 2013: 29: 580–593.
60. Khalil I, Naaman A, Camilleri J. Investigation of anovel mechanically mixed mineral trioxide aggregate(MM-MTATM). Int Endod J 2015: doi:10.1111/iej.12373.
61. Gandolfi MG, Taddei P, Siboni F, Modena E, DeStefano ED, Prati C. Biomimetic remineralization ofhuman dentin using promising innovative calcium-sili-cate hybrid “smart” materials. Dent Mater 2011: 27:1055–1069.
62. Gandolfi MG, Van Landuyt K, Taddei P, Modena E,Van Meerbeek B, Prati C. Environmental scanningelectron microscopy connected with energy dispersivex-ray analysis and Raman techniques to study ProRoot
44
Camilleri
mineral trioxide aggregate and calcium silicate cementsin wet conditions and in real time. J Endod 2010: 36:851–857.
63. Gomes-Filho JE, de Faria MD, Bernab�e PF, Nery MJ,Otoboni-Filho JA, Dezan-J�unior E, de Moraes CostaMM, Cannon M. Mineral trioxide aggregate but notlight-cure mineral trioxide aggregate stimulated miner-alization. J Endod 2008: 34: 62–65.
64. Gomes-Filho JE, de Moraes Costa MT, Cintra LT,Lodi CS, Duarte PC, Okamoto R, Bernab�e PF, NeryMJ, Cannon M. Evaluation of alveolar socket responseto Angelus MTA and experimental light-cure MTA.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2010: 110: e93–97.
65. Formosa LM, Mallia B, Camilleri J. The chemicalproperties of light- and chemical-curing compositeswith mineral trioxide aggregate filler. Dent Mater2013: 29: e11–19.
66. Profeta AC, Mannocci F, Foxton R, Watson TF, Fei-tosa VP, De Carlo B, Mongiorgi R, Valdr�e G, SauroS. Experimental etch-and-rinse adhesives doped withbioactive calcium silicate-based micro-fillers to gener-ate therapeutic resin-dentin interfaces. Dent Mater2013: 29: 729–741.
67. Chung H, Kim M, Ko H, Yang W. Evaluation ofphysical and biologic properties of the mixture of min-eral trioxide aggregate and 4-META/MMA-TBBresin. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2011: 112: e6–11.
68. Camilleri J, Laurent P, About I. BiodentineTM andTheracalTM LC hydration after pulp capping in entiretooth cultures. J Endod 2014: 40: 1846–1854.
69. GandolfiMG, Siboni F, Prati C. Chemical-physical proper-ties of TheraCal, a novel light-curable MTA-like materialfor pulp capping. Int Endod J 2012:45: 571–579.
70. Camilleri J. Hydration characteristics of Biodentineand Theracal used as pulp capping materials. DentMater 2014: 30: 709–715.
71. Hebling J, Lessa FC, Nogueira I, Carvalho RM, CostaCA. Cytotoxicity of resin-based light-cured liners. AmJ Dent 2009: 22: 137–142.
72. Viapiana R, Guerreiro-Tanomaru JM, Tanomaru-FilhoM, Camilleri J. The microstructure and surface mor-phology of sealers based on Portland cement and anepoxy resin with niobium and zirconium radiopacifi-ers. Dent Mater 2014: 40: 555–561.
73. Bryan TE, Khechen K, Brackett MG, Messer RL, El-Awady A, Primus CM, Gutmann JL, Tay FR. In vitroosteogenic potential of an experimental calcium silicate-based root canal sealer. J Endod 2010: 36: 1163–1169.
74. Camilleri J, Gandolfi MG, Siboni F, Prati C. Dynamicsealing ability of MTA root canal sealer. Int Endod J2011: 44: 9–20.
75. Camilleri J. Evaluation of selected properties of min-eral trioxide aggregate sealer cement. J Endod 2009:35: 1412–1417.
76. Camilleri J, Mallia B. Evaluation of the dimensionalchanges of mineral trioxide aggregate sealer. Int En-dod J 2011: 44: 416–424.
77. Huffman BP, Mai S, Pinna L, Weller RN, PrimusCM, Gutmann JL, Pashley DH, Tay FR. Dislocationresistance of ProRoot Endo Sealer, a calcium silicate-based root canal sealer, from radicular dentine. IntEndod J 2009: 42: 34–46.
78. Weller RN, Tay KC, Garrett LV, Mai S, Primus CM,Gutmann JL, Pashley DH, Tay FR. Microscopicappearance and apical seal of root canals filled withgutta-percha and ProRoot Endo Sealer after immer-sion in a phosphate-containing fluid. Int Endod J2008: 41: 977–986.
79. Duarte MA, Alves de Aguiar K, Zeferino MA, VivanRR, Ordinola-Zapata R, Tanomaru-Filho M, Weckw-erth PH, Kuga MC. Evaluation of the propylene gly-col association on some physical and chemicalproperties of mineral trioxide aggregate. Int Endod J2012: 45: 565–570.
80. Wang X, Chen L, Xiang H, Ye J. Influence of anti-washout agents on the rheological properties and in-jectability of a calcium phosphate cement. J BiomedMater Res B Appl Biomater 2007: 81: 410–418.
81. Grech L, Mallia B, Camilleri J. Investigation of thephysical properties of tricalcium silicate cement-basedroot-end filling materials. Dent Mater 2013: 29:e20–28.
82. Formosa LM, Mallia B, Camilleri J. A quantitativemethod for determining the antiwashout characteris-tics of cement-based dental materials including min-eral trioxide aggregate. Int Endod J 2013: 46:179–186.
83. Grech L, Mallia B, Camilleri J. Characterization of setIntermediate Restorative Material, Biodentine, Bioag-gregate and a prototype calcium silicate cement foruse as root-end filling materials. Int Endod J 2013:46: 632–641.
84. Camilleri J, Sorrentino F, Damidot D. Characteriza-tion of unhydrated and hydrated BioAggregateTM andMTA AngelusTM. Clin Oral Investig 2015: 19: 689–698.
85. Zhou HM, Shen Y, Zheng W, Li L, Zheng YF, Haap-asalo M. Physical properties of 5 root canal sealers.J Endod 2013: 39: 1281–1286.
86. Zhou HM, Du TF, Shen Y, Wang ZJ, Zheng YF, Ha-apasalo M. In vitro cytotoxicity of calcium silicate-con-taining endodontic sealers. J Endod 2015: 41: 56–61.
87. Torabinejad M, Chivian N. Clinical applications ofmineral trioxide aggregate. J Endod 1999: 25:197–205.
88. Nekoofar MH, Stone DF, Dummer PM. The effect ofblood contamination on the compressive strength andsurface microstructure of mineral trioxide aggregate.Int Endod J 2010: 43: 782–791.
89. Nekoofar MH, Davies TE, Stone D, Basturk FB,Dummer PM. Microstructure and chemical analysis ofblood-contaminated mineral trioxide aggregate. IntEndod J 2011: 44: 1011–1018.
90. Nekoofar MH, Oloomi K, Sheykhrezae MS, Tabor R,Stone DF, Dummer PM. An evaluation of the effectof blood and human serum on the surface microhard-
45
MTA: present and future developments
ness and surface microstructure of mineral trioxideaggregate. Int Endod J 2010: 43: 849–858.
91. Kang JS, Rhim EM, Huh SY, Ahn SJ, Kim DS, Kim SY,Park SH. The effects of humidity and serum on the sur-face microhardness and morphology of five retrogradefilling materials. Scanning 2012: 34: 207–214.
92. Kim Y, Kim S, Shin YS, Jung IY, Lee SJ. Failure ofsetting of mineral trioxide aggregate in the presenceof fetal bovine serum and its prevention. J Endod2012: 38: 536–540.
93. Paranjpe A, ZhangH, Johnson JD. Effects of mineral tri-oxide aggregate on human dental pulp cells after pulp-capping procedures. J Endod 2010: 36: 1042–1047.
94. Sawyer AN, Nikonov SY, Pancio AK, Niu LN, AgeeKA, Loushine RJ, Weller RN, Pashley DH, Tay FR.Effects of calcium silicate-based materials on the flexuralproperties of dentin. J Endod 2012: 38: 680–683.
95. Camilleri J. Scanning electron microscopic evaluationof the material interface of adjacent layers of dentalmaterials. Dent Mater 2011: 27: 870–878.
96. Kayahan MB, Nekoofar MH, Kazanda�g M, CanpolatC, Malkondu O, Kaptan F, Dummer PM. Effect ofacid-etching procedure on selected physical propertiesof mineral trioxide aggregate. Int Endod J 2009: 42:1004–1014.
97. Hong ST, Bae KS, Baek SH, Kum KY, Shon WJ, LeeW. Effects of root canal irrigants on the push-outstrength and hydration behavior of accelerated mineraltrioxide aggregate in its early setting phase. J Endod2010: 36: 1995–1999.
98. Lee YL, Lin FH, Wang WH, Ritchie HH, Lan WH,Lin CP. Effects of EDTA on the hydration mechanismof mineral trioxide aggregate. J Dent Res 2007: 86:534–538.
46
Camilleri







