

Staff and Consultants:
Ellen Magnis, Vice President, American Stroke Association
Wendy Segrest, Director, American Stroke Association Operations
Debi McGill, Editor-in-Chief
Jon Caswell, Lead Editor
Mike Mills, Writer
Sam Gaines, Writer
Pierce Goetz, Art Director
Michelle Neighbors, Advertising Sales
Copyright 2005 American Heart Association ISSN 1047-014X
Stroke Connection Magazine is published six times a year by the American Stroke Association, a division of the American Heart Association. Material may be reproduced only with appropriate acknowledgment of the source and written permission from the American Heart Association. Please address inquiries to the Editor-in-Chief. The information contained in this publication is provided by the American Stroke Association as a resource. The services or products listed are not owned or provided by the American Stroke Association. Additionally, the products or services have not been evaluated and their listing should not be construed as a recommendation or endorsement of these products or services.1-888-4STROKE (1-888-478-7653) StrokeAssociation.org
contents July/August 2005
16
23 26Stroke Connection Magazine is underwritten
in part by Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership, makers of Plavix.
Feature StoryHealing through Music 14
“I think I should have no other mortal wants, if I could always have plenty of music. It seems to infuse strength into my limbs and ideas into my brain.” — George Eliot
ArticlesDetermined Kathy 11
Kathy Morelli was an avid bicyclist before her stroke. With a little help from
her friends, she’s on the road again.
Advances in Rehab 13Two new, up-and-coming post-stroke therapies.
Stroke. You’re the Cure. 21Find out what ASA is doing and what
you can do to make a difference.
Examining Medicare Reform 23Plain-English explanations of recent changes.
Cholesterol — New Information for High-Risk Patients 26
When it comes to “bad” cholesterol, new guidelines for high-risk patients say “the lower the better.”
DepartmentsLetters to the Editor 1
Stroke Notes 2
Readers Room 6Life at the Curb 28
Introducing a new column from comedian (and survivor) John Kawie.
Everyday Survival 30a division of
Produced and distributed in cooperation with Vitality Communications

July/August 2005 1
mail: c/o Editor-in-Chief Stroke Connection Magazine 7272 Greenville Ave. Dallas, TX 75231
fax: 214-706-5231
e-mail: [email protected]
We Want To Hear From You
Letters may be edited for length and scientific integrity. The opinions presented are those of the individual and do not reflect those of the American Stroke Association.
editor Connecting You to Us
L E T T E R Sto the
I am a hemorrhagic stroke survivor since December 1999, and at present I am suffering thalamic pain syndrome. Endurance is my lifestyle since then. According to my neurologist, my hypothalamus was pushed by a blood clot during my stroke, and it is not easily addressed. Through your magazine I’ve got encouragement that life must go on though tough! Living in pain (left side from ear, eyes to toes), spasms, excruciating pain and lots of it is my daily experience, yet I’ve survived already more than five years. Your magazine really inspires me.
Leobardo Felipe, SurvivorGeneral Santos City, Philippines
Editor’s Note: We investigated thalamic pain in our September/October 2003 issue. That article is now available on our Web site, www.strokeassociation.org.
My wife had a stroke seven years ago and has suffered with lack of interest and terrific headaches all day, every day, since then. Our family doctor says she may gain some interest back, but it’s been seven years. She is very frustrated.
As for the terrible headaches, she’s been trying pain management. If she takes pain pills, they provide some relief but when they wear off, the pain becomes 10 times worse.
If anyone has experienced anything similar, did you find something that helped?
Weldon Power, CaregiverSteweache, NS, Canada
What a great magazine! I am inspired all over again. A year after my stroke, I volunteered to visit some recent survivors. I was discouraged that most only wanted sympathy, rather than working to recover some of what they had lost. I wish I had known about Stroke Connection so I could have added them to the subscriber list.
Rick Davis, SurvivorSalt Lake City, Utah
My husband had a stroke at age 59 in May 2002. He experienced short-term memory loss and has shown improvement. He was unemployed at the time. We had to use what little savings we had for prescriptions and to help with living expenses. He is an only child, both parents deceased, and last February we had to cash an IRA. He wasn’t thinking, I guess, and the bank didn’t remind him that this would be income and now we owe a few thousand dollars in taxes!
He cannot receive disability due to not working at the time of the stroke. We are fearful of the future — will we have money for prescriptions, etc.? He has also been diagnosed with sleep apnea but is unable to wear the device that helps prevent sleep apnea. He takes one or two naps daily and believes his medications make him sleepy. However, his doctor is not too quick to try anything else.
Thus the reason for this letter: Do your readers have any suggestions on relieving the sleepiness so he might feel like doing everyday house errands and help with our financial difficulties? I am 55 and could retire but financially I am unable to. Many of the things in Mary Morgan’s story in March/April issue reminded me of my husband. She is correct, the medical profession does not give the patient or family much information. I believe more should be communicated.
Linda Jennings, CaregiverPennsboro, West Virginia
July/August 20052
notes Connecting You to the World
S T R O K E
Playing interactive virtual reality games significantly improved motor function in a small study of stroke survivors. The technology appears to help reorganize brain functions, allowing survivors to regain some walking ability.
Stroke often impairs one side of the body and walking ability. In many cases survivors compensate for the impaired leg by using the intact leg, which can cause further problems in the weakened limb.
“There have been a number of approaches used in stroke rehabilitation to help patients recover gait function, but outcomes have been variable,” said lead author Sung H. You, P.T., Ph.D., assistant professor of physical therapy at Hampton University in Hampton, Va. “The problem is that we don’t fully understand how recovery after stroke affects the brain. So we investigated how virtual reality intervention affects stroke patients’ brains, and, ultimately, their ability to walk.”
Dr. You studied 10 survivors (average age 57) who had experienced strokes at least a year earlier. All had weakness on one side. They were randomly assigned to a control group, which received no intervention, or a virtual reality (VR) group, which received the computer-assisted training an hour a day, five days a week, for a month.
Three games were used — Stepping Up/Down, Sharkbait and Snowboarding — to build range of motion, balance, mobility, stepping and ambulation skills.
Stepping Up/Down simulates going up and down stairs and helps hip flexion and extension, weight-shifting and balance.
Sharkbait simulates deep-sea diving with sharks, electric eels and other sea creatures, and requires weight-shifting, stepping, protective reflexes and squatting.
Snowboarding simulates snowboarding down a narrow slope, and requires trunk flexing and extending, lateral bending and weight-shifting.
In each game, the patient is positioned in front of an interactive screen which projects a “virtual reality” scenario.
Researchers measured patients’ ability to walk before and after therapy, and did imaging studies of the brains of the five patients who had VR training.
Before therapy, brain imaging showed that movement in the affected leg stimulated activity on both sides of the brain, which is abnormal. After therapy, movement in the affected leg stimulated activity in the opposite hemisphere.
“These are the first findings that suggest that VR training results in a reorganization of brain activation, which is associated with improved gait function,” Dr. You said. The brain reorganization was associated with notable gain in locomotor function.
“Most of the VR-trained subjects reported spontaneous uses and confidence in the affected limb during daily activities such as transferring in and out of the bathtub, putting on trousers and stepping onto a step or curb,” Dr. You said. “These functions were not possible before VR.”
To view a video news release of this story, visit www.strokeassociation.org.
Virtual Reality Games Spark Gains
Freedom to choose where, when and how to explore life is the aspiration
of virtually every American. For many persons with physical disabilities
and special transportation needs, having choices to fit their individual
needs provides a rewarding experience. Ford Mobility Motoring offers
valuable financial and practical assistance, including reimbursement for the
exact amount of vehicle adaptations, up to $1,000 on adaptive equipment
and up to $200 on alerting devices, lumbar support and running boards.*
Ford Credit Mobility Financing — Offering flexible finance terms for
persons with physical disabilities and their families. In addition, they will
finance both the vehicle and the adaptive equipment for qualified customers
enrolled in the Ford Mobility Motoring Program.
Roadside Assistance — Tire changes, towing, fuel delivery, lockout
assistance and jump-starts are now just a phone call away. In times of
need, a 24-hour toll-free number can bring assistance any day of the year.
www.mobilitymotoringprogram.com
In memory of Christopher Reeve.The Christopher Reeve Paralysis Foundation (CRPF) is committed to funding research that develops treatments and cures for paralysiscaused by spinal cord injury and other central nervous system disorders. The Foundation also vigorously works to improve thequality of life for people living with disabilities through its grants program, Paralysis Resource Center and advocacy efforts.
1952 - 2004
*Total reimbursement is not to exceed $1,000. Options available for factory installation are not considered eligible under the terms of the program.
MA8629/12-04/4
1-800-952-22481-800-833-0312 TTY
5752 Ad Stroke 2/22/05 11:04 AM Page 1

July/August 20054
Connecting You to the World
S T R O K E
notes
A coagulation factor called NovoSeven Recombinant Activated Factor VII
(rFVIIa) reduced mortality and hematoma growth, and thus improved clinical outcomes for patients with acute intracerebral brain hemorrhage (ICH), according to a 2004 study.
Norvo Nordisk Inc. announced the promising results at the International Stroke Conference in New Orleans, Louisiana, in February 2005. The coagulant rFVIIa slowed growth of intracerebral hematomas when administered within four hours of symptom onset, researchers found.
“The current medical and surgical treatment options for ICH are not effective,” said lead author Dr. Stephan Mayer, associate professor and director of the Neurological Intensive Care Unit at Columbia University Medical Center.
Mayer said that 35 to 50 percent of ICH patients die within one month, while those who survive live with serious neurological problems. He pointed to the trial results as reason to hope for a more effective treatment. “The current data suggest a possible change in our paradigm for the treatment of ICH,” he said.
Desmoteplase, a genetically engineered blood-clot buster, is showing potential in the treatment of acute
ischemic stroke. According to studies, the medication could be effective up to nine hours after the onset of symptoms.
Current clot-busting treatments must be administered within a three-hour window from symptom onset, and most survivors do not arrive at the hospital in time for effective treatment.
DIAS2, a multinational study initiated by Forest Laboratories in February 2005, aims to corroborate the already promising findings on desmoteplase.
“Preserving brain function and restoring quality of life in patients after acute ischemic stroke is the goal of effective stroke treatment,” said Anthony Furlan, M.D., medical director of the Cleveland Clinic Foundation and primary investigator of the study.
A study published in the February 2005 issue of Environmental Health Perspectives found that
patients with long-term exposure to air pollution are more likely to develop atherosclerosis.
The study is the latest to confirm air pollution’s role in cardiovascular disease and the first to link atherosclerosis with exposure to the fine particulate matter that makes up air pollution. “We’ve known for some time that air pollution leads to lung damage, but this study also emphasizes the role air pollution plays on the arteries,” said Dr. Jim Burkhart, science editor of Environmental Health Perspectives. “Heart disease is a primary cause of death in the Western world, so more research, perhaps focusing on those at highest risk, is important.”
Long-Term Air Pollution
Exposure May Be Bad for
Arteries
New Clot
Buster
Possible Treatment for Brain Hemorrhage
July/August 20056
I am 48 years old, and my stroke affected both optic nerves, the top of my spinal cord and af-fected the right side of my face mostly and the left side of my body.
I have not yet regained the use of the computer and I no longer spell very well, and as far as what I write making sense, sometimes it will, some-times it won’t. I didn’t have my caregivers go
through this letter to make changes. They are the type that say they need no thanks and would not mail it.
Just before I had my stroke at 46 I trained a beautiful dog named Timba to be a service dog. At his checkup before turning him over, they found he had a birth defect and they could not use him. I was allowed to keep him, and he has saved my life many times.
I have friends who loved me before the stroke, and they have helped me in many ways. And they still love me, even though I have changed in many ways. Stroke changes life in many ways, forever.
My family was there at every step to help. My sister paid my bills and the mortgage on my house until I could get set up on disability. Each person took one or two things to help me get through.
It’s been almost two years since my stroke, and my sight is still bad. The doctors think that it’s as good as it is going to get: It’s double vision in a tunnel. I can’t drive, but I have friends that will take me where I need to go. I tried the bus once but got lost. I can’t walk without fall-ing, but I have friends to steady me. I can’t see or remem-ber where I need to go, but I’ve found helping hands at my door. I can’t remember how to write words that others will understand, but there are those who will help me say what I mean. I get depressed but take time to look around and find that I am blessed.
I know this is not written on good paper with no mis-takes, but it is a “thank you” to all my family, friends and animals and a “hang in there” for those who are working through the hard path they’re on. I’ll pray for you.
Karmen Coombs, SurvivorSalt Lake City, Utah
Sneaking a Thank Youroom Connecting You to Others
R E A D E R S
Up Life’s WayTo All the Stroke Survivors and Family —Greetings of Love, Peace and Joy —We keep all in our prayers.
One never knows Life’s twists and turnsCertain woesAs Life’s waySome upSome downYou make the bestYou grow in knowledge Then comes wisdomLook up Look out SmileAnd be thankful To the Creator That made usFor His Love and Kindness.
Ruthann H. Fleming • Phoenix, Arizona
Karmen Coombs and Timba

July/August 2005 7
Item No: B1-K0180 Trim Size: 8 1/4" x 10 3/4" Publication: Stroke Connection
YOU DON’T WANT ANOTHERHEART ATTACK OR ANOTHERSTROKE TO SNEAK UP ON YOU.
PLAVIX HELPS KEEP BLOOD PLATELETSFROM STICKING TOGETHER AND FORMINGCLOTS, WHICH HELPS PROTECT YOU FROMANOTHER HEART ATTACK OR STROKE.If you’ve had a heart attack or stroke, the last thing youneed is another one sneaking up on you. PLAVIX mayhelp. PLAVIX is a prescription medication for peoplewho have had a recent heart attack or recent stroke, orwho have poor circulation in the legs, causing pain.
PLAVIX OFFERS PROTECTION.PLAVIX is proven to help keep blood platelets fromsticking together and forming clots, which helps keepyour blood flowing. This can help protect you fromanother heart attack or stroke.
IMPORTANT INFORMATION: If you have a stomachulcer or other condition that causes bleeding, youshouldn't use Plavix. When taking Plavix alone or withsome medicines including aspirin, the risk of bleedingmay increase.To minimize this risk, talk to your doctorbefore taking aspirin or other medicines with Plavix.Additional rare but serious side effects could occur.
WITHOUT PLAVIX WITH PLAVIX
PROVEN TO HELP PROTECT FROM ANOTHER HEART ATTACK OR STROKE
TALK TO YOUR DOCTOR ABOUT PLAVIX.For more information, visit www.plavix.com or call1-877-700-0701.
YOU DON’T WANT ANOTHERHEART ATTACK OR ANOTHERSTROKE TO SNEAK UP ON YOU.
© 2005 Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership.USA.CLO.05.04.41/May 2005 B1-K0180/05-05Sanofi-Synthelabo Inc., a member of the sanofi-aventis Group
Please see important product information on the following page.
B1K0180_StrokeConnectionAd_Mech 5/19/05 4:27 PM Page 1
July/August 20058
Item No: B1-K0186 Trim Size: 8.25" x 10.75"
PLAVIX®clopidogrel bisulfate tabletsRx onlyBrief Summary of Prescribing Information Rev. November 2004 INDICATIONS AND USAGEPLAVIX (clopidogrel bisulfate) is indicated for the reduction of thrombotic events asfollows:
• Recent MI, Recent Stroke or Established Peripheral Arterial DiseaseFor patients with a history of recent myocardial infarction (MI), recent stroke, orestablished peripheral arterial disease, PLAVIX has been shown to reduce therate of a combined endpoint of new ischemic stroke (fatal or not), new MI (fatalor not), and other vascular death.
• Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI)including patients who are to be managed medically and those who are to bemanaged with percutaneous coronary intervention (with or without stent) orCABG, PLAVIX has been shown to decrease the rate of a combined endpoint ofcardiovascular death, MI, or stroke as well as the rate of a combined endpoint ofcardiovascular death, MI, stroke, or refractory ischemia.
CONTRAINDICATIONSThe use of PLAVIX is contraindicated in the following conditions:
• Hypersensitivity to the drug substance or any component of the product.• Active pathological bleeding such as peptic ulcer or intracranial hemorrhage.
WARNINGSThrombotic thrombocytopenic purpura (TTP): TTP has been reported rarely followinguse of PLAVIX, sometimes after a short exposure (<2 weeks). TTP is a serious condition and requires urgent referral to a hematologist for prompt treatment. It ischaracterized by thrombocytopenia, microangiopathic hemolytic anemia (schistocytes[fragmented RBCs] seen on peripheral smear), neurological findings, renal dysfunc-tion, and fever. TTP was not seen during clopidogrel's clinical trials, which includedover 17,500 clopidogrel-treated patients. In world-wide postmarketing experience,however, TTP has been reported at a rate of about four cases per million patientsexposed, or about 11 cases per million patient-years. The background rate is thoughtto be about four cases per million person-years. (See ADVERSE REACTIONS.)PRECAUTIONSGeneralAs with other antiplatelet agents, PLAVIX prolongs the bleeding time and thereforeshould be used with caution in patients who may be at risk of increased bleeding fromtrauma, surgery, or other pathological conditions (particularly gastrointestinal andintraocular). If a patient is to undergo elective surgery and an antiplatelet effect is notdesired, PLAVIX should be discontinued 5 days prior to surgery.
Due to the risk of bleeding and undesirable hematological effects, blood cell countdetermination and/or other appropriate testing should be promptly considered, when-ever such suspected clinical symptoms arise during the course of treatment (seeADVERSE REACTIONS).
GI Bleeding: In CAPRIE, PLAVIX was associated with a rate of gastrointestinal bleed-ing of 2.0%, vs. 2.7% on aspirin. In CURE, the incidence of major gastrointestinalbleeding was 1.3% vs. 0.7% (PLAVIX + aspirin vs. placebo + aspirin, respectively).PLAVIX should be used with caution in patients who have lesions with a propensity tobleed (such as ulcers). Drugs that might induce such lesions should be used with caution in patients taking PLAVIX.
Use in Hepatically Impaired Patients: Experience is limited in patients with severehepatic disease, who may have bleeding diatheses. PLAVIX should be used with caution in this population.
Use in Renally-impaired Patients: Experience is limited in patients with severe renalimpairment. PLAVIX should be used with caution in this population.Information for PatientsPatients should be told that they may bleed more easily and it may take them longer thanusual to stop bleeding when they take PLAVIX or PLAVIX combined with aspirin, and thatthey should report any unusual bleeding to their physician. Patients should inform physi-cians and dentists that they are taking PLAVIX and/or any other product known to affectbleeding before any surgery is scheduled and before any new drug is taken.Drug InteractionsStudy of specific drug interactions yielded the following results:
Aspirin: Aspirin did not modify the clopidogrel-mediated inhibition of ADP-inducedplatelet aggregation. Concomitant administration of 500 mg of aspirin twice a day for 1day did not significantly increase the prolongation of bleeding time induced by PLAVIX.PLAVIX potentiated the effect of aspirin on collagen-induced platelet aggregation. PLAVIX and aspirin have been administered together for up to one year.
Heparin: In a study in healthy volunteers, PLAVIX did not necessitate modificationof the heparin dose or alter the effect of heparin on coagulation. Coadministration ofheparin had no effect on inhibition of platelet aggregation induced by PLAVIX.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): In healthy volunteers receivingnaproxen, concomitant administration of PLAVIX was associated with increased occultgastrointestinal blood loss. NSAIDs and PLAVIX should be coadministered with caution.
Warfarin: Because of the increased risk of bleeding, the concomitant administration ofwarfarin with PLAVIX should be undertaken with caution. (See PRECAUTIONS–General.)
Other Concomitant Therapy: No clinically significant pharmacodynamic interactionswere observed when PLAVIX was coadministered with atenolol, nifedipine, or bothatenolol and nifedipine. The pharmacodynamic activity of PLAVIX was also not signifi-cantly influenced by the coadministration of phenobarbital, cimetidine or estrogen.
The pharmacokinetics of digoxin or theophylline were not modified by the coad-ministration of PLAVIX (clopidogrel bisulfate).
At high concentrations in vitro, clopidogrel inhibits P450 (2C9). Accordingly, PLAVIXmay interfere with the metabolism of phenytoin, tamoxifen, tolbutamide, warfarin,torsemide, fluvastatin, and many non-steroidal anti-inflammatory agents, but thereare no data with which to predict the magnitude of these interactions. Caution should beused when any of these drugs is coadministered with PLAVIX.
In addition to the above specific interaction studies, patients entered into clinical trials with PLAVIX received a variety of concomitant medications including diuretics,beta-blocking agents, angiotensin converting enzyme inhibitors, calcium antago-nists, cholesterol lowering agents, coronary vasodilators, antidiabetic agents(including insulin), antiepileptic agents, hormone replacement therapy, heparins(unfractionated and LMWH) and GPIIb/IIIa antagonists without evidence of clinicallysignificant adverse interactions. The use of oral anticoagulants, non-study anti-plateletdrug and chronic NSAIDs was not allowed in CURE and there are no data on their concomitant use with clopidogrel.Drug/Laboratory Test InteractionsNone known.Carcinogenesis, Mutagenesis, Impairment of FertilityThere was no evidence of tumorigenicity when clopidogrel was administered for 78 weeksto mice and 104 weeks to rats at dosages up to 77 mg/kg per day, which afforded plasma exposures >25 times that in humans at the recommended daily dose of 75 mg.
Clopidogrel was not genotoxic in four in vitro tests (Ames test, DNA-repair test inrat hepatocytes, gene mutation assay in Chinese hamster fibroblasts, and metaphasechromosome analysis of human lymphocytes) and in one in vivo test (micronucleustest by oral route in mice).
Clopidogrel was found to have no effect on fertility of male and female rats at oral doses up to 400 mg/kg per day (52 times the recommended human dose on amg/m2 basis).PregnancyPregnancy Category B. Reproduction studies performed in rats and rabbits at doses upto 500 and 300 mg/kg/day (respectively, 65 and 78 times the recommended dailyhuman dose on a mg/m2 basis), revealed no evidence of impaired fertility or fetotoxic-ity due to clopidogrel. There are, however, no adequate and well-controlled studies inpregnant women. Because animal reproduction studies are not always predictive of ahuman response, PLAVIX should be used during pregnancy only if clearly needed.Nursing MothersStudies in rats have shown that clopidogrel and/or its metabolites are excreted in themilk. It is not known whether this drug is excreted in human milk. Because many drugsare excreted in human milk and because of the potential for serious adverse reactions innursing infants, a decision should be made whether to discontinue nursing or to dis-continue the drug, taking into account the importance of the drug to the nursing woman.Pediatric UseSafety and effectiveness in the pediatric population have not been established.Geriatric UseOf the total number of subjects in controlled clinical studies, approximately 50% ofpatients treated with PLAVIX were 65 years of age and over. Approximately 16% ofpatients treated with PLAVIX were 75 years of age and over. The observed difference in risk of bleeding events with clopidogrel plus aspirin versusplacebo plus aspirin by age category is provided in the following table (see ADVERSEREACTIONS).
ADVERSE REACTIONSPLAVIX has been evaluated for safety in more than 17,500 patients, including over 9,000patients treated for 1 year or more. The overall tolerability of PLAVIX in CAPRIE was sim-ilar to that of aspirin regardless of age, gender and race, with an approximately equal inci-dence (13%) of patients withdrawing from treatment because of adverse reactions. Theclinically important adverse events observed in CAPRIE and CURE are discussed below.
Hemorrhagic: In CAPRIE patients receiving PLAVIX, gastrointestinal hemorrhageoccurred at a rate of 2.0%, and required hospitalization in 0.7%. In patients receivingaspirin, the corresponding rates were 2.7% and 1.1%, respectively. The incidence ofintracranial hemorrhage was 0.4% for PLAVIX compared to 0.5% for aspirin.
In CURE, PLAVIX use with aspirin was associated with an increase in bleeding com-pared to placebo with aspirin (see table below). There was an excess in major bleed-ing in patients receiving PLAVIX plus aspirin compared with placebo plus aspirin, pri-marily gastrointestinal and at puncture sites. The incidence of intracranial hemorrhage(0.1%), and fatal bleeding (0.2%), were the same in both groups.
The overall incidence of bleeding is described in the table below for patients receiv-ing both PLAVIX and aspirin in CURE, CURE Incidence of bleeding complications (% patients)Event PLAVIX Placebo P-value
(+ aspirin)* (+ aspirin)*(n=6259) (n=6303)
Major bleeding † 3.7 ‡ 2.7 § 0.001Life-threatening bleeding 2.2 1.8 0.13
Fatal 0.2 0.25 g/dL hemoglobin drop 0.9 0.9Requiring surgical intervention 0.7 0.7Hemorrhagic strokes 0.1 0.1Requiring inotropes 0.5 0.5Requiring transfusion (�4 units) 1.2 1.0
Other major bleeding 1.6 1.0 0.005Significantly disabling 0.4 0.3Intraocular bleeding with
significant loss of vision 0.05 0.03Requiring 2-3 units of blood 1.3 0.9
Minor bleeding ¶ 5.1 2.4 <0.001* Other standard therapies were used as appropriate.† Life threatening and other major bleeding.‡ Major bleeding event rate for PLAVIX + aspirin was dose-dependent on aspirin:
<100 mg=2.6%; 100-200 mg= 3.5%; >200 mg=4.9%Major bleeding event rates for PLAVIX + aspirin by age were: <65 years = 2.5%, �65 to <75 years = 4.1%, �75 years 5.9%
§ Major bleeding event rate for placebo + aspirin was dose-dependent on aspirin: <100 mg=2.0%; 100-200 mg= 2.3%; >200 mg=4.0%Major bleeding event rates for placebo + aspirin by age were: <65 years = 2.1%, �65 to <75 years = 3.1%, �75 years 3.6%
¶ Led to interruption of study medication.
Ninety-two percent (92%) of the patients in the CURE study received heparin/LMWH, and the rate of bleeding in these patients was similar to the overall results.
There was no excess in major bleeds within seven days after coronary bypass graftsurgery in patients who stopped therapy more than five days prior to surgery (eventrate 4.4% PLAVIX + aspirin; 5.3% placebo + aspirin). In patients who remained on ther-apy within five days of bypass graft surgery, the event rate was 9.6% for PLAVIX +aspirin, and 6.3% for placebo + aspirin.
Neutropenia/agranulocytosis: Ticlopidine, a drug chemically similar to PLAVIX, isassociated with a 0.8% rate of severe neutropenia (less than 450 neutrophils/µL). InCAPRIE severe neutropenia was observed in six patients, four on PLAVIX and two onaspirin. Two of the 9599 patients who received PLAVIX and none of the 9586 patientswho received aspirin had neutrophil counts of zero. One of the four PLAVIX patients inCAPRIE was receiving cytotoxic chemotherapy, and another recovered and returned tothe trial after only temporarily interrupting treatment with PLAVIX (clopidogrel bisul-fate). In CURE, the numbers of patients with thrombocytopenia (19 PLAVIX + aspirinvs. 24 placebo + aspirin) or neutropenia (3 vs. 3) were similar.
Although the risk of myelotoxicity with PLAVIX (clopidogrel bisulfate) thus appearsto be quite low, this possibility should be considered when a patient receiving PLAVIXdemonstrates fever or other sign of infection.
Gastrointestinal: Overall, the incidence of gastrointestinal events (e.g. abdominalpain, dyspepsia, gastritis and constipation) in patients receiving PLAVIX (clopidogrelbisulfate) was 27.1%, compared to 29.8% in those receiving aspirin in the CAPRIE trial.In the CURE trial the incidence of these gastrointestinal events for patients receivingPLAVIX + aspirin was 11.7% compared to 12.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the incidence of peptic, gastric or duodenal ulcers was 0.7% forPLAVIX and 1.2% for aspirin. In the CURE trial the incidence of peptic, gastric or duo-denal ulcers was 0.4% for PLAVIX + aspirin and 0.3% for placebo + aspirin.
Cases of diarrhea were reported in the CAPRIE trial in 4.5% of patients in the PLAVIX group compared to 3.4% in the aspirin group. However, these were rarelysevere (PLAVIX=0.2% and aspirin=0.1%). In the CURE trial, the incidence of diarrheafor patients receiving PLAVIX + aspirin was 2.1% compared to 2.2% for those receiv-ing placebo + aspirin.
In the CAPRIE trial, the incidence of patients withdrawing from treatment becauseof gastrointestinal adverse reactions was 3.2% for PLAVIX (clopidogrel bisulfate) and4.0% for aspirin. In the CURE trial, the incidence of patients withdrawing from treatment because of gastrointestinal adverse reactions was 0.9% for PLAVIX + aspirincompared with 0.8% for placebo + aspirin.
Rash and Other Skin Disorders: In the CAPRIE trial, the incidence of skin andappendage disorders in patients receiving PLAVIX was 15.8% (0.7% serious); the cor-responding rate in aspirin patients was 13.1% (0.5% serious). In the CURE trial theincidence of rash or other skin disorders in patients receiving PLAVIX + aspirin was4.0% compared to 3.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the overall incidence of patients withdrawing from treatmentbecause of skin and appendage disorders adverse reactions was 1.5% for PLAVIX and 0.8% for aspirin. In the CURE trial, the incidence of patients withdrawing becauseof skin and appendage disorders adverse reactions was 0.7% for PLAVIX + aspirin compared with 0.3% for placebo + aspirin.
Adverse events occurring in �2.5% of patients on PLAVIX in the CAPRIE controlledclinical trial are shown below regardless of relationship to PLAVIX. The median dura-tion of therapy was 20 months, with a maximum of 3 years.Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE
% Incidence (% Discontinuation)Body System PLAVIX AspirinEvent [n=9599] [n=9586]Body as a Whole- general disorders
Chest Pain 8.3 (0.2) 8.3 (0.3)Accidental/Inflicted Injury 7.9 (0.1) 7.3 (0.1)Influenza-like symptoms 7.5 (<0.1) 7.0 (<0.1)Pain 6.4 (0.1) 6.3 (0.1)Fatigue 3.3 (0.1) 3.4 (0.1)
Cardiovascular disorders, generalEdema 4.1 (<0.1) 4.5 (<0.1)Hypertension 4.3 (<0.1) 5.1 (<0.1)
Central & peripheral nervous system disorders
Headache 7.6 (0.3) 7.2 (0.2)Dizziness 6.2 (0.2) 6.7 (0.3)
Gastrointestinal system disordersAbdominal pain 5.6 (0.7) 7.1 (1.0)Dyspepsia 5.2 (0.6) 6.1 (0.7)Diarrhea 4.5 (0.4) 3.4 (0.3)Nausea 3.4 (0.5) 3.8 (0.4)
Metabolic & nutritional disordersHypercholesterolemia 4.0 (0) 4.4 (<0.1)
Musculo-skeletal system disordersArthralgia 6.3 (0.1) 6.2 (0.1)Back Pain 5.8 (0.1) 5.3 (<0.1)
Platelet, bleeding, & clotting disordersPurpura/Bruise 5.3 (0.3) 3.7 (0.1)Epistaxis 2.9 (0.2) 2.5 (0.1)
Psychiatric disordersDepression 3.6 (0.1) 3.9 (0.2)
Respiratory system disordersUpper resp tract infection 8.7 (<0.1) 8.3 (<0.1)Dyspnea 4.5 (0.1) 4.7 (0.1)Rhinitis 4.2 (0.1) 4.2 (<0.1)Bronchitis 3.7 (0.1) 3.7 (0)Coughing 3.1 (<0.1) 2.7(<0.1)
Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE (continued)% Incidence (% Discontinuation)
Body System PLAVIX AspirinEvent [n=9599] [n=9586]Skin & appendage disorders
Rash 4.2 (0.5) 3.5 (0.2)Pruritus 3.3 (0.3) 1.6 (0.1)
Urinary system disordersUrinary tract infection 3.1 (0) 3.5 (0.1)
Incidence of discontinuation, regardless of relationship to therapy, is shown in parentheses.
Adverse events occurring in �2.0% of patients on PLAVIX in the CURE controlledclinical trial are shown below regardless of relationship to PLAVIX.Adverse Events Occurring in �2.0% of PLAVIX Patients in CURE
% Incidence (% Discontinuation)Body System PLAVIX Placebo
(+ aspirin)* (+ aspirin)*Event [n=6259] [n=6303]Body as a Whole- general disorders
Chest Pain 2.7 (<0.1) 2.8 (0.0)Central & peripheral nervous system disorders
Headache 3.1 (0.1) 3.2 (0.1)Dizziness 2.4 (0.1) 2.0 (<0.1)
Gastrointestinal system disordersAbdominal pain 2.3 (0.3) 2.8 (0.3)Dyspepsia 2.0 (0.1) 1.9 (<0.1)Diarrhea 2.1 (0.1) 2.2 (0.1)
*Other standard therapies were used as appropriate.
Other adverse experiences of potential importance occurring in 1% to 2.5% ofpatients receiving PLAVIX (clopidogrel bisulfate) in the CAPRIE or CURE controlledclinical trials are listed below regardless of relationship to PLAVIX. In general, the inci-dence of these events was similar to that in patients receiving aspirin (in CAPRIE) orplacebo + aspirin (in CURE).
Autonomic Nervous System Disorders: Syncope, Palpitation. Body as a Whole-general disorders: Asthenia, Fever, Hernia. Cardiovascular disorders: Cardiac failure.Central and peripheral nervous system disorders: Cramps legs, Hypoaesthesia,Neuralgia, Paraesthesia, Vertigo. Gastrointestinal system disorders: Constipation,Vomiting. Heart rate and rhythm disorders: Fibrillation atrial. Liver and biliary systemdisorders: Hepatic enzymes increased. Metabolic and nutritional disorders: Gout,hyperuricemia, non-protein nitrogen (NPN) increased. Musculo-skeletal system disor-ders: Arthritis, Arthrosis. Platelet, bleeding & clotting disorders: GI hemorrhage,hematoma, platelets decreased. Psychiatric disorders: Anxiety, Insomnia. Red bloodcell disorders: Anemia. Respiratory system disorders: Pneumonia, Sinusitis. Skin andappendage disorders: Eczema, Skin ulceration. Urinary system disorders: Cystitis.Vision disorders: Cataract, Conjunctivitis.
Other potentially serious adverse events which may be of clinical interest but wererarely reported (<1%) in patients who received PLAVIX in the CAPRIE or CURE con-trolled clinical trials are listed below regardless of relationship to PLAVIX. In general,the incidence of these events was similar to that in patients receiving aspirin (inCAPRIE) or placebo + aspirin (in CURE).
Body as a whole: Allergic reaction, necrosis ischemic. Cardiovascular disorders:Edema generalized. Gastrointestinal system disorders: Gastric ulcer perforated, gastri-tis hemorrhagic, upper GI ulcer hemorrhagic. Liver and Biliary system disorders:Bilirubinemia, hepatitis infectious, liver fatty. Platelet, bleeding and clotting disorders:hemarthrosis, hematuria, hemoptysis, hemorrhage intracranial, hemorrhage retroperi-toneal, hemorrhage of operative wound, ocular hemorrhage, pulmonary hemorrhage,purpura allergic, thrombocytopenia. Red blood cell disorders: Anemia aplastic, anemiahypochromic. Reproductive disorders, female: Menorrhagia. Respiratory system disorders: Hemothorax. Skin and appendage disorders: Bullous eruption, rash erythe-matous, rash maculopapular, urticaria. Urinary system disorders: Abnormal renal function, acute renal failure. White cell and reticuloendothelial system disorders:Agranulocytosis, granulocytopenia, leukemia, leukopenia, neutrophils decreased.Postmarketing ExperienceThe following events have been reported spontaneously from worldwide postmarket-ing experience:
• Body as a whole:- hypersensitivity reactions, anaphylactoid reactions
• Central and Peripheral Nervous System disorders:- confusion, hallucinations, taste disorders
• Hepato-biliary disorders:- abnormal liver function test, hepatitis (non-infectious)
• Platelet, Bleeding and Clotting disorders:- cases of bleeding with fatal outcome (especially intracranial, gastrointestinal
and retroperitoneal hemorrhage)- agranulocytosis, aplastic anemia/pancytopenia, thrombotic thrombocytopenic
purpura (TTP) - some cases with fatal outcome – (see WARNINGS).- conjunctival, ocular and retinal bleeding
• Respiratory, thoracic and mediastinal disorders:- bronchospasm
• Skin and subcutaneous tissue disorders:- angioedema, erythema multiforme, Stevens-Johnson syndrome, lichen planus
• Renal and urinary disorders:- glomerulopathy, increased creatinine levels
• Vascular disorders:- vasculitis, hypotension
• Gastrointestinal disorders:- colitis (including ulcerative or lymphocytic colitis), pancreatitis
• Musculoskeletal, connective tissue and bone disorders:- myalgia
OVERDOSAGEOverdose following clopidogrel administration may lead to prolonged bleeding timeand subsequent bleeding complications. Appropriate therapy should be considered ifbleeding is observed. A single oral dose of clopidogrel at 1500 or 2000 mg/kg waslethal to mice and to rats and at 3000 mg/kg to baboons. Symptoms of acute toxicitywere vomiting (in baboons), prostration, difficult breathing, and gastrointestinal hem-orrhage in all species.Recommendations About Specific Treatment:Based on biological plausibility, platelet transfusion may be appropriate to reverse thepharmacological effects of PLAVIX if quick reversal is required.DOSAGE AND ADMINISTRATIONRecent MI, Recent Stroke, or Established Peripheral Arterial DiseaseThe recommended daily dose of PLAVIX is 75 mg once daily.Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI), PLAVIXshould be initiated with a single 300 mg loading dose and then continued at 75 mgonce daily. Aspirin (75 mg-325 mg once daily) should be initiated and continued incombination with PLAVIX. In CURE, most patients with Acute Coronary Syndrome alsoreceived heparin acutely (see CLINICAL STUDIES).
PLAVIX can be administered with or without food.No dosage adjustment is necessary for elderly patients or patients with renal dis-
ease. (See Clinical Pharmacology: Special Populations.)Distributed by:Bristol-Myers Squibb/Sanofi Pharmaceuticals PartnershipNew York, NY 10016
PLAVIX® is a registered trademark of Sanofi-Synthelabo.
Brief Summary of Prescribing Information Rev. November 2004
B1-K0186_IBC 5/19/05 4:05 PM Page 1
July/August 2005 9
Stroke Changes ThingsI was released from the hospital with a stroke
diagnosis on our 50th wedding anniversary. My life has changed in some respects since that happened in September 2002.
For instance, I use a cane now. Whenever I walk with someone, I hold their arm and use my cane. Except at home, I use a cane everywhere.
I take 11 pills each day to prevent future problems. I try to walk two miles every day. I walk only in the daylight now, never at night. At intersections, I turn my head completely both ways to look for cars. I don’t drive — the doctor and my wife both say I should not, so we haven’t bothered the DMV with the problem. I am not allowed to climb ladders, or fall down.
I am uneasy in crowds because I can only see people who are in front of me. Church friends are very good about coming up in front of me before they speak. Eating out is a problem because I can’t see the waitress come up behind me and put the food down or take it away. I’m always afraid I’ll spill something that I don’t know is there.
Now I hold all of our church shepherd group meetings at my home, rather than rotate them through the group each month. This group of 15 has been together for seven years, and they have been very supportive of me.
I am now 76 years old, and my vision has not changed since the stroke. My wife and I have adapted to it and learn every day how to cope with it. The Lord has been good, and we are grateful for every day that we have been given to learn to live with such a minor handicap.
John Mitchell, Survivor • West Covina, California
room Connecting You to Others
R E A D E R S
Item No: B1-K0186 Trim Size: 8.25" x 10.75"
PLAVIX®clopidogrel bisulfate tabletsRx onlyBrief Summary of Prescribing Information Rev. November 2004 INDICATIONS AND USAGEPLAVIX (clopidogrel bisulfate) is indicated for the reduction of thrombotic events asfollows:
• Recent MI, Recent Stroke or Established Peripheral Arterial DiseaseFor patients with a history of recent myocardial infarction (MI), recent stroke, orestablished peripheral arterial disease, PLAVIX has been shown to reduce therate of a combined endpoint of new ischemic stroke (fatal or not), new MI (fatalor not), and other vascular death.
• Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI)including patients who are to be managed medically and those who are to bemanaged with percutaneous coronary intervention (with or without stent) orCABG, PLAVIX has been shown to decrease the rate of a combined endpoint ofcardiovascular death, MI, or stroke as well as the rate of a combined endpoint ofcardiovascular death, MI, stroke, or refractory ischemia.
CONTRAINDICATIONSThe use of PLAVIX is contraindicated in the following conditions:
• Hypersensitivity to the drug substance or any component of the product.• Active pathological bleeding such as peptic ulcer or intracranial hemorrhage.
WARNINGSThrombotic thrombocytopenic purpura (TTP): TTP has been reported rarely followinguse of PLAVIX, sometimes after a short exposure (<2 weeks). TTP is a serious condition and requires urgent referral to a hematologist for prompt treatment. It ischaracterized by thrombocytopenia, microangiopathic hemolytic anemia (schistocytes[fragmented RBCs] seen on peripheral smear), neurological findings, renal dysfunc-tion, and fever. TTP was not seen during clopidogrel's clinical trials, which includedover 17,500 clopidogrel-treated patients. In world-wide postmarketing experience,however, TTP has been reported at a rate of about four cases per million patientsexposed, or about 11 cases per million patient-years. The background rate is thoughtto be about four cases per million person-years. (See ADVERSE REACTIONS.)PRECAUTIONSGeneralAs with other antiplatelet agents, PLAVIX prolongs the bleeding time and thereforeshould be used with caution in patients who may be at risk of increased bleeding fromtrauma, surgery, or other pathological conditions (particularly gastrointestinal andintraocular). If a patient is to undergo elective surgery and an antiplatelet effect is notdesired, PLAVIX should be discontinued 5 days prior to surgery.
Due to the risk of bleeding and undesirable hematological effects, blood cell countdetermination and/or other appropriate testing should be promptly considered, when-ever such suspected clinical symptoms arise during the course of treatment (seeADVERSE REACTIONS).
GI Bleeding: In CAPRIE, PLAVIX was associated with a rate of gastrointestinal bleed-ing of 2.0%, vs. 2.7% on aspirin. In CURE, the incidence of major gastrointestinalbleeding was 1.3% vs. 0.7% (PLAVIX + aspirin vs. placebo + aspirin, respectively).PLAVIX should be used with caution in patients who have lesions with a propensity tobleed (such as ulcers). Drugs that might induce such lesions should be used with caution in patients taking PLAVIX.
Use in Hepatically Impaired Patients: Experience is limited in patients with severehepatic disease, who may have bleeding diatheses. PLAVIX should be used with caution in this population.
Use in Renally-impaired Patients: Experience is limited in patients with severe renalimpairment. PLAVIX should be used with caution in this population.Information for PatientsPatients should be told that they may bleed more easily and it may take them longer thanusual to stop bleeding when they take PLAVIX or PLAVIX combined with aspirin, and thatthey should report any unusual bleeding to their physician. Patients should inform physi-cians and dentists that they are taking PLAVIX and/or any other product known to affectbleeding before any surgery is scheduled and before any new drug is taken.Drug InteractionsStudy of specific drug interactions yielded the following results:
Aspirin: Aspirin did not modify the clopidogrel-mediated inhibition of ADP-inducedplatelet aggregation. Concomitant administration of 500 mg of aspirin twice a day for 1day did not significantly increase the prolongation of bleeding time induced by PLAVIX.PLAVIX potentiated the effect of aspirin on collagen-induced platelet aggregation. PLAVIX and aspirin have been administered together for up to one year.
Heparin: In a study in healthy volunteers, PLAVIX did not necessitate modificationof the heparin dose or alter the effect of heparin on coagulation. Coadministration ofheparin had no effect on inhibition of platelet aggregation induced by PLAVIX.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): In healthy volunteers receivingnaproxen, concomitant administration of PLAVIX was associated with increased occultgastrointestinal blood loss. NSAIDs and PLAVIX should be coadministered with caution.
Warfarin: Because of the increased risk of bleeding, the concomitant administration ofwarfarin with PLAVIX should be undertaken with caution. (See PRECAUTIONS–General.)
Other Concomitant Therapy: No clinically significant pharmacodynamic interactionswere observed when PLAVIX was coadministered with atenolol, nifedipine, or bothatenolol and nifedipine. The pharmacodynamic activity of PLAVIX was also not signifi-cantly influenced by the coadministration of phenobarbital, cimetidine or estrogen.
The pharmacokinetics of digoxin or theophylline were not modified by the coad-ministration of PLAVIX (clopidogrel bisulfate).
At high concentrations in vitro, clopidogrel inhibits P450 (2C9). Accordingly, PLAVIXmay interfere with the metabolism of phenytoin, tamoxifen, tolbutamide, warfarin,torsemide, fluvastatin, and many non-steroidal anti-inflammatory agents, but thereare no data with which to predict the magnitude of these interactions. Caution should beused when any of these drugs is coadministered with PLAVIX.
In addition to the above specific interaction studies, patients entered into clinical trials with PLAVIX received a variety of concomitant medications including diuretics,beta-blocking agents, angiotensin converting enzyme inhibitors, calcium antago-nists, cholesterol lowering agents, coronary vasodilators, antidiabetic agents(including insulin), antiepileptic agents, hormone replacement therapy, heparins(unfractionated and LMWH) and GPIIb/IIIa antagonists without evidence of clinicallysignificant adverse interactions. The use of oral anticoagulants, non-study anti-plateletdrug and chronic NSAIDs was not allowed in CURE and there are no data on their concomitant use with clopidogrel.Drug/Laboratory Test InteractionsNone known.Carcinogenesis, Mutagenesis, Impairment of FertilityThere was no evidence of tumorigenicity when clopidogrel was administered for 78 weeksto mice and 104 weeks to rats at dosages up to 77 mg/kg per day, which afforded plasma exposures >25 times that in humans at the recommended daily dose of 75 mg.
Clopidogrel was not genotoxic in four in vitro tests (Ames test, DNA-repair test inrat hepatocytes, gene mutation assay in Chinese hamster fibroblasts, and metaphasechromosome analysis of human lymphocytes) and in one in vivo test (micronucleustest by oral route in mice).
Clopidogrel was found to have no effect on fertility of male and female rats at oral doses up to 400 mg/kg per day (52 times the recommended human dose on amg/m2 basis).PregnancyPregnancy Category B. Reproduction studies performed in rats and rabbits at doses upto 500 and 300 mg/kg/day (respectively, 65 and 78 times the recommended dailyhuman dose on a mg/m2 basis), revealed no evidence of impaired fertility or fetotoxic-ity due to clopidogrel. There are, however, no adequate and well-controlled studies inpregnant women. Because animal reproduction studies are not always predictive of ahuman response, PLAVIX should be used during pregnancy only if clearly needed.Nursing MothersStudies in rats have shown that clopidogrel and/or its metabolites are excreted in themilk. It is not known whether this drug is excreted in human milk. Because many drugsare excreted in human milk and because of the potential for serious adverse reactions innursing infants, a decision should be made whether to discontinue nursing or to dis-continue the drug, taking into account the importance of the drug to the nursing woman.Pediatric UseSafety and effectiveness in the pediatric population have not been established.Geriatric UseOf the total number of subjects in controlled clinical studies, approximately 50% ofpatients treated with PLAVIX were 65 years of age and over. Approximately 16% ofpatients treated with PLAVIX were 75 years of age and over. The observed difference in risk of bleeding events with clopidogrel plus aspirin versusplacebo plus aspirin by age category is provided in the following table (see ADVERSEREACTIONS).
ADVERSE REACTIONSPLAVIX has been evaluated for safety in more than 17,500 patients, including over 9,000patients treated for 1 year or more. The overall tolerability of PLAVIX in CAPRIE was sim-ilar to that of aspirin regardless of age, gender and race, with an approximately equal inci-dence (13%) of patients withdrawing from treatment because of adverse reactions. Theclinically important adverse events observed in CAPRIE and CURE are discussed below.
Hemorrhagic: In CAPRIE patients receiving PLAVIX, gastrointestinal hemorrhageoccurred at a rate of 2.0%, and required hospitalization in 0.7%. In patients receivingaspirin, the corresponding rates were 2.7% and 1.1%, respectively. The incidence ofintracranial hemorrhage was 0.4% for PLAVIX compared to 0.5% for aspirin.
In CURE, PLAVIX use with aspirin was associated with an increase in bleeding com-pared to placebo with aspirin (see table below). There was an excess in major bleed-ing in patients receiving PLAVIX plus aspirin compared with placebo plus aspirin, pri-marily gastrointestinal and at puncture sites. The incidence of intracranial hemorrhage(0.1%), and fatal bleeding (0.2%), were the same in both groups.
The overall incidence of bleeding is described in the table below for patients receiv-ing both PLAVIX and aspirin in CURE, CURE Incidence of bleeding complications (% patients)Event PLAVIX Placebo P-value
(+ aspirin)* (+ aspirin)*(n=6259) (n=6303)
Major bleeding † 3.7 ‡ 2.7 § 0.001Life-threatening bleeding 2.2 1.8 0.13
Fatal 0.2 0.25 g/dL hemoglobin drop 0.9 0.9Requiring surgical intervention 0.7 0.7Hemorrhagic strokes 0.1 0.1Requiring inotropes 0.5 0.5Requiring transfusion (�4 units) 1.2 1.0
Other major bleeding 1.6 1.0 0.005Significantly disabling 0.4 0.3Intraocular bleeding with
significant loss of vision 0.05 0.03Requiring 2-3 units of blood 1.3 0.9
Minor bleeding ¶ 5.1 2.4 <0.001* Other standard therapies were used as appropriate.† Life threatening and other major bleeding.‡ Major bleeding event rate for PLAVIX + aspirin was dose-dependent on aspirin:
<100 mg=2.6%; 100-200 mg= 3.5%; >200 mg=4.9%Major bleeding event rates for PLAVIX + aspirin by age were: <65 years = 2.5%, �65 to <75 years = 4.1%, �75 years 5.9%
§ Major bleeding event rate for placebo + aspirin was dose-dependent on aspirin: <100 mg=2.0%; 100-200 mg= 2.3%; >200 mg=4.0%Major bleeding event rates for placebo + aspirin by age were: <65 years = 2.1%, �65 to <75 years = 3.1%, �75 years 3.6%
¶ Led to interruption of study medication.
Ninety-two percent (92%) of the patients in the CURE study received heparin/LMWH, and the rate of bleeding in these patients was similar to the overall results.
There was no excess in major bleeds within seven days after coronary bypass graftsurgery in patients who stopped therapy more than five days prior to surgery (eventrate 4.4% PLAVIX + aspirin; 5.3% placebo + aspirin). In patients who remained on ther-apy within five days of bypass graft surgery, the event rate was 9.6% for PLAVIX +aspirin, and 6.3% for placebo + aspirin.
Neutropenia/agranulocytosis: Ticlopidine, a drug chemically similar to PLAVIX, isassociated with a 0.8% rate of severe neutropenia (less than 450 neutrophils/µL). InCAPRIE severe neutropenia was observed in six patients, four on PLAVIX and two onaspirin. Two of the 9599 patients who received PLAVIX and none of the 9586 patientswho received aspirin had neutrophil counts of zero. One of the four PLAVIX patients inCAPRIE was receiving cytotoxic chemotherapy, and another recovered and returned tothe trial after only temporarily interrupting treatment with PLAVIX (clopidogrel bisul-fate). In CURE, the numbers of patients with thrombocytopenia (19 PLAVIX + aspirinvs. 24 placebo + aspirin) or neutropenia (3 vs. 3) were similar.
Although the risk of myelotoxicity with PLAVIX (clopidogrel bisulfate) thus appearsto be quite low, this possibility should be considered when a patient receiving PLAVIXdemonstrates fever or other sign of infection.
Gastrointestinal: Overall, the incidence of gastrointestinal events (e.g. abdominalpain, dyspepsia, gastritis and constipation) in patients receiving PLAVIX (clopidogrelbisulfate) was 27.1%, compared to 29.8% in those receiving aspirin in the CAPRIE trial.In the CURE trial the incidence of these gastrointestinal events for patients receivingPLAVIX + aspirin was 11.7% compared to 12.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the incidence of peptic, gastric or duodenal ulcers was 0.7% forPLAVIX and 1.2% for aspirin. In the CURE trial the incidence of peptic, gastric or duo-denal ulcers was 0.4% for PLAVIX + aspirin and 0.3% for placebo + aspirin.
Cases of diarrhea were reported in the CAPRIE trial in 4.5% of patients in the PLAVIX group compared to 3.4% in the aspirin group. However, these were rarelysevere (PLAVIX=0.2% and aspirin=0.1%). In the CURE trial, the incidence of diarrheafor patients receiving PLAVIX + aspirin was 2.1% compared to 2.2% for those receiv-ing placebo + aspirin.
In the CAPRIE trial, the incidence of patients withdrawing from treatment becauseof gastrointestinal adverse reactions was 3.2% for PLAVIX (clopidogrel bisulfate) and4.0% for aspirin. In the CURE trial, the incidence of patients withdrawing from treatment because of gastrointestinal adverse reactions was 0.9% for PLAVIX + aspirincompared with 0.8% for placebo + aspirin.
Rash and Other Skin Disorders: In the CAPRIE trial, the incidence of skin andappendage disorders in patients receiving PLAVIX was 15.8% (0.7% serious); the cor-responding rate in aspirin patients was 13.1% (0.5% serious). In the CURE trial theincidence of rash or other skin disorders in patients receiving PLAVIX + aspirin was4.0% compared to 3.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the overall incidence of patients withdrawing from treatmentbecause of skin and appendage disorders adverse reactions was 1.5% for PLAVIX and 0.8% for aspirin. In the CURE trial, the incidence of patients withdrawing becauseof skin and appendage disorders adverse reactions was 0.7% for PLAVIX + aspirin compared with 0.3% for placebo + aspirin.
Adverse events occurring in �2.5% of patients on PLAVIX in the CAPRIE controlledclinical trial are shown below regardless of relationship to PLAVIX. The median dura-tion of therapy was 20 months, with a maximum of 3 years.Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE
% Incidence (% Discontinuation)Body System PLAVIX AspirinEvent [n=9599] [n=9586]Body as a Whole- general disorders
Chest Pain 8.3 (0.2) 8.3 (0.3)Accidental/Inflicted Injury 7.9 (0.1) 7.3 (0.1)Influenza-like symptoms 7.5 (<0.1) 7.0 (<0.1)Pain 6.4 (0.1) 6.3 (0.1)Fatigue 3.3 (0.1) 3.4 (0.1)
Cardiovascular disorders, generalEdema 4.1 (<0.1) 4.5 (<0.1)Hypertension 4.3 (<0.1) 5.1 (<0.1)
Central & peripheral nervous system disorders
Headache 7.6 (0.3) 7.2 (0.2)Dizziness 6.2 (0.2) 6.7 (0.3)
Gastrointestinal system disordersAbdominal pain 5.6 (0.7) 7.1 (1.0)Dyspepsia 5.2 (0.6) 6.1 (0.7)Diarrhea 4.5 (0.4) 3.4 (0.3)Nausea 3.4 (0.5) 3.8 (0.4)
Metabolic & nutritional disordersHypercholesterolemia 4.0 (0) 4.4 (<0.1)
Musculo-skeletal system disordersArthralgia 6.3 (0.1) 6.2 (0.1)Back Pain 5.8 (0.1) 5.3 (<0.1)
Platelet, bleeding, & clotting disordersPurpura/Bruise 5.3 (0.3) 3.7 (0.1)Epistaxis 2.9 (0.2) 2.5 (0.1)
Psychiatric disordersDepression 3.6 (0.1) 3.9 (0.2)
Respiratory system disordersUpper resp tract infection 8.7 (<0.1) 8.3 (<0.1)Dyspnea 4.5 (0.1) 4.7 (0.1)Rhinitis 4.2 (0.1) 4.2 (<0.1)Bronchitis 3.7 (0.1) 3.7 (0)Coughing 3.1 (<0.1) 2.7(<0.1)
Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE (continued)% Incidence (% Discontinuation)
Body System PLAVIX AspirinEvent [n=9599] [n=9586]Skin & appendage disorders
Rash 4.2 (0.5) 3.5 (0.2)Pruritus 3.3 (0.3) 1.6 (0.1)
Urinary system disordersUrinary tract infection 3.1 (0) 3.5 (0.1)
Incidence of discontinuation, regardless of relationship to therapy, is shown in parentheses.
Adverse events occurring in �2.0% of patients on PLAVIX in the CURE controlledclinical trial are shown below regardless of relationship to PLAVIX.Adverse Events Occurring in �2.0% of PLAVIX Patients in CURE
% Incidence (% Discontinuation)Body System PLAVIX Placebo
(+ aspirin)* (+ aspirin)*Event [n=6259] [n=6303]Body as a Whole- general disorders
Chest Pain 2.7 (<0.1) 2.8 (0.0)Central & peripheral nervous system disorders
Headache 3.1 (0.1) 3.2 (0.1)Dizziness 2.4 (0.1) 2.0 (<0.1)
Gastrointestinal system disordersAbdominal pain 2.3 (0.3) 2.8 (0.3)Dyspepsia 2.0 (0.1) 1.9 (<0.1)Diarrhea 2.1 (0.1) 2.2 (0.1)
*Other standard therapies were used as appropriate.
Other adverse experiences of potential importance occurring in 1% to 2.5% ofpatients receiving PLAVIX (clopidogrel bisulfate) in the CAPRIE or CURE controlledclinical trials are listed below regardless of relationship to PLAVIX. In general, the inci-dence of these events was similar to that in patients receiving aspirin (in CAPRIE) orplacebo + aspirin (in CURE).
Autonomic Nervous System Disorders: Syncope, Palpitation. Body as a Whole-general disorders: Asthenia, Fever, Hernia. Cardiovascular disorders: Cardiac failure.Central and peripheral nervous system disorders: Cramps legs, Hypoaesthesia,Neuralgia, Paraesthesia, Vertigo. Gastrointestinal system disorders: Constipation,Vomiting. Heart rate and rhythm disorders: Fibrillation atrial. Liver and biliary systemdisorders: Hepatic enzymes increased. Metabolic and nutritional disorders: Gout,hyperuricemia, non-protein nitrogen (NPN) increased. Musculo-skeletal system disor-ders: Arthritis, Arthrosis. Platelet, bleeding & clotting disorders: GI hemorrhage,hematoma, platelets decreased. Psychiatric disorders: Anxiety, Insomnia. Red bloodcell disorders: Anemia. Respiratory system disorders: Pneumonia, Sinusitis. Skin andappendage disorders: Eczema, Skin ulceration. Urinary system disorders: Cystitis.Vision disorders: Cataract, Conjunctivitis.
Other potentially serious adverse events which may be of clinical interest but wererarely reported (<1%) in patients who received PLAVIX in the CAPRIE or CURE con-trolled clinical trials are listed below regardless of relationship to PLAVIX. In general,the incidence of these events was similar to that in patients receiving aspirin (inCAPRIE) or placebo + aspirin (in CURE).
Body as a whole: Allergic reaction, necrosis ischemic. Cardiovascular disorders:Edema generalized. Gastrointestinal system disorders: Gastric ulcer perforated, gastri-tis hemorrhagic, upper GI ulcer hemorrhagic. Liver and Biliary system disorders:Bilirubinemia, hepatitis infectious, liver fatty. Platelet, bleeding and clotting disorders:hemarthrosis, hematuria, hemoptysis, hemorrhage intracranial, hemorrhage retroperi-toneal, hemorrhage of operative wound, ocular hemorrhage, pulmonary hemorrhage,purpura allergic, thrombocytopenia. Red blood cell disorders: Anemia aplastic, anemiahypochromic. Reproductive disorders, female: Menorrhagia. Respiratory system disorders: Hemothorax. Skin and appendage disorders: Bullous eruption, rash erythe-matous, rash maculopapular, urticaria. Urinary system disorders: Abnormal renal function, acute renal failure. White cell and reticuloendothelial system disorders:Agranulocytosis, granulocytopenia, leukemia, leukopenia, neutrophils decreased.Postmarketing ExperienceThe following events have been reported spontaneously from worldwide postmarket-ing experience:
• Body as a whole:- hypersensitivity reactions, anaphylactoid reactions
• Central and Peripheral Nervous System disorders:- confusion, hallucinations, taste disorders
• Hepato-biliary disorders:- abnormal liver function test, hepatitis (non-infectious)
• Platelet, Bleeding and Clotting disorders:- cases of bleeding with fatal outcome (especially intracranial, gastrointestinal
and retroperitoneal hemorrhage)- agranulocytosis, aplastic anemia/pancytopenia, thrombotic thrombocytopenic
purpura (TTP) - some cases with fatal outcome – (see WARNINGS).- conjunctival, ocular and retinal bleeding
• Respiratory, thoracic and mediastinal disorders:- bronchospasm
• Skin and subcutaneous tissue disorders:- angioedema, erythema multiforme, Stevens-Johnson syndrome, lichen planus
• Renal and urinary disorders:- glomerulopathy, increased creatinine levels
• Vascular disorders:- vasculitis, hypotension
• Gastrointestinal disorders:- colitis (including ulcerative or lymphocytic colitis), pancreatitis
• Musculoskeletal, connective tissue and bone disorders:- myalgia
OVERDOSAGEOverdose following clopidogrel administration may lead to prolonged bleeding timeand subsequent bleeding complications. Appropriate therapy should be considered ifbleeding is observed. A single oral dose of clopidogrel at 1500 or 2000 mg/kg waslethal to mice and to rats and at 3000 mg/kg to baboons. Symptoms of acute toxicitywere vomiting (in baboons), prostration, difficult breathing, and gastrointestinal hem-orrhage in all species.Recommendations About Specific Treatment:Based on biological plausibility, platelet transfusion may be appropriate to reverse thepharmacological effects of PLAVIX if quick reversal is required.DOSAGE AND ADMINISTRATIONRecent MI, Recent Stroke, or Established Peripheral Arterial DiseaseThe recommended daily dose of PLAVIX is 75 mg once daily.Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI), PLAVIXshould be initiated with a single 300 mg loading dose and then continued at 75 mgonce daily. Aspirin (75 mg-325 mg once daily) should be initiated and continued incombination with PLAVIX. In CURE, most patients with Acute Coronary Syndrome alsoreceived heparin acutely (see CLINICAL STUDIES).
PLAVIX can be administered with or without food.No dosage adjustment is necessary for elderly patients or patients with renal dis-
ease. (See Clinical Pharmacology: Special Populations.)Distributed by:Bristol-Myers Squibb/Sanofi Pharmaceuticals PartnershipNew York, NY 10016
PLAVIX® is a registered trademark of Sanofi-Synthelabo.
Brief Summary of Prescribing Information Rev. November 2004
B1-K0186_IBC 5/19/05 4:05 PM Page 1
I survived a hemorrhagic stroke in May 2001. After my stroke I could not talk or write, and I lost my memory. My legs were spared, so I could walk. Initially I was depressed, but over the next several months, with the help of therapists, friends and
family, I relearned some very basic things, like how to use utensils and how to sign my name.
I worked with a speech therapist three times a week for the first six weeks. Progress seemed very slow, but I was determined to get better. I fought this stroke with speech therapy sessions every Monday and I worked hard. My teacher gave me progressively more difficult homework. In time, it became easier for me.
It’s been three years and I’m still working at my therapy, and now I can communicate with people. I am 80 years old, a retired optometrist, and I wrote this poem.
Emergence of Light
It was years ago,When a suddenEruption of hotBlood in my head.
It was in the night,When an artery blew Asunder my nerves To die.
I could not speak,I could not write,I could not communicate With people.
“Aphasia,” Said the doctor.“Therapy,” Said the doctor.
Many years of therapy,Working very hard.I seek for the bright Emergence of light.
Edward Riaboy, SurvivorEllicott City, Maryland
Edward Riaboy
July/August 200510
Have you or someone you know
suffered a stroke?Select stroke centers nationwide are seeking
individuals who have suffered a stroke
(even if your stroke was many months or
years ago) that has caused weakness in
one hand and/or arm to participate in an
investigational research study.
Purpose: The study will assess the safety andeffectiveness of an implanted device* in treating patientswho have reduced hand and/or arm function after stroke.
Participation Criteria: Patients at least 21 years of agewho have suffered a stroke, which has caused weaknessin one hand and/or arm, may be eligible for this study.
Study Sponsor: Northstar Neuroscience, Seattle WA.www.northstarneuro.com
Please call today for more information: 888-546-9779 (24 hr. support)
*Caution: Investigational device. Limited by Federal (or United States) law to investigational use.
All costs related to the study and rehabilitation (including local transportation) will be covered for those who qualify.
room Connecting You to Others
R E A D E R S
The average person has many personalities that are all interwoven and blended. Their expression is
determined by what is held back and what is not. A stroke separates all those personalities and displays all of them in dramatic mood swings. I have found that all my moods can come out in as little as an hour. You feel everything from anger to depression, bitter to happy and content, and the cycle just keeps repeating.
You don’t want to get stuck in a bad mood because you will just have a tougher time and just have to live through it. That is when you should get help. And remember, you move
along at a frustrating snail’s pace.There are two attitudes that
occur after a stroke, if you want to continue living.
First, because of the losses, you are a different person. You must start over or die.
Second, hang onto everything that still works. Retain a positive attitude and let the rest go. You must let go of your past life as if it died.
If you can improve anything to above average, it will give you a sense of accomplishment and a reason to live. Now, there must be something you can work on or you would be in a coma. Get busy.
Joe Zwijack, SurvivorMokena, Illinois
25 Years of Stroke Survival
Joe Zwijack
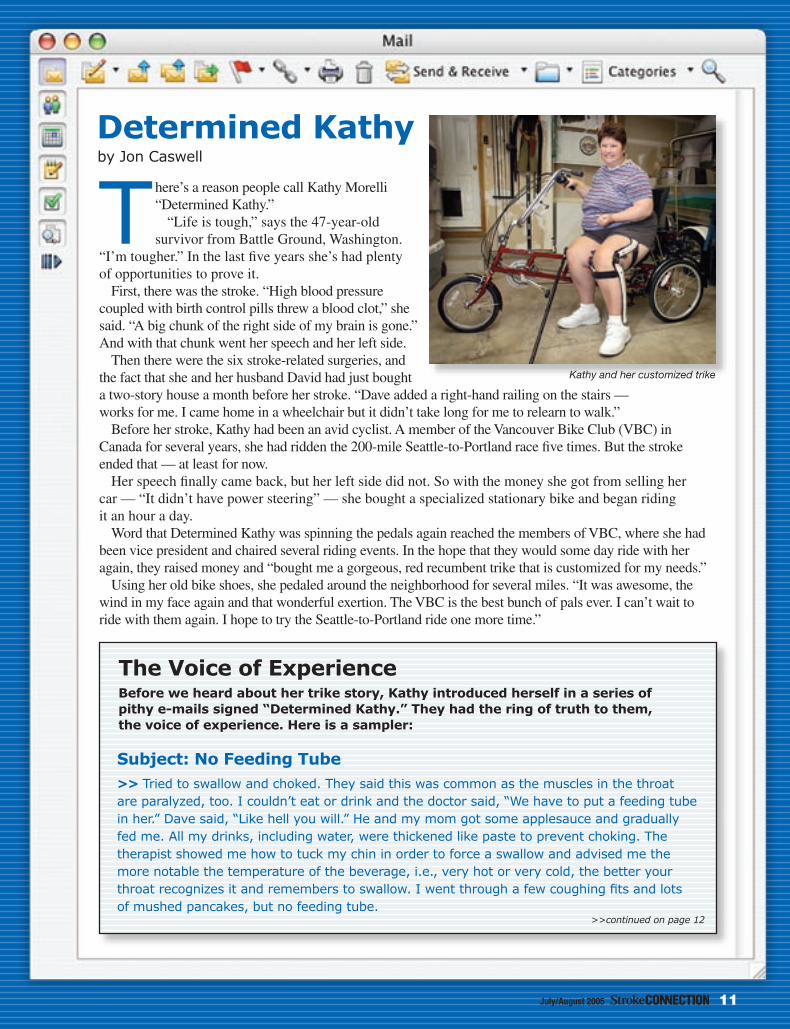
There’s a reason people call Kathy Morelli “Determined Kathy.”
“Life is tough,” says the 47-year-old survivor from Battle Ground, Washington.
“I’m tougher.” In the last five years she’s had plenty of opportunities to prove it.
First, there was the stroke. “High blood pressure coupled with birth control pills threw a blood clot,” she said. “A big chunk of the right side of my brain is gone.” And with that chunk went her speech and her left side.
Then there were the six stroke-related surgeries, and the fact that she and her husband David had just bought a two-story house a month before her stroke. “Dave added a right-hand railing on the stairs — works for me. I came home in a wheelchair but it didn’t take long for me to relearn to walk.”
Before her stroke, Kathy had been an avid cyclist. A member of the Vancouver Bike Club (VBC) in Canada for several years, she had ridden the 200-mile Seattle-to-Portland race five times. But the stroke ended that — at least for now.
Her speech finally came back, but her left side did not. So with the money she got from selling her car — “It didn’t have power steering” — she bought a specialized stationary bike and began riding it an hour a day.
Word that Determined Kathy was spinning the pedals again reached the members of VBC, where she had been vice president and chaired several riding events. In the hope that they would some day ride with her again, they raised money and “bought me a gorgeous, red recumbent trike that is customized for my needs.”
Using her old bike shoes, she pedaled around the neighborhood for several miles. “It was awesome, the wind in my face again and that wonderful exertion. The VBC is the best bunch of pals ever. I can’t wait to ride with them again. I hope to try the Seattle-to-Portland ride one more time.”
Determined Kathyby Jon Caswell
The Voice of ExperienceBefore we heard about her trike story, Kathy introduced herself in a series of pithy e-mails signed “Determined Kathy.” They had the ring of truth to them, the voice of experience. Here is a sampler:
Subject: No Feeding Tube>> Tried to swallow and choked. They said this was common as the muscles in the throat are paralyzed, too. I couldn’t eat or drink and the doctor said, “We have to put a feeding tube in her.” Dave said, “Like hell you will.” He and my mom got some applesauce and gradually fed me. All my drinks, including water, were thickened like paste to prevent choking. The therapist showed me how to tuck my chin in order to force a swallow and advised me the more notable the temperature of the beverage, i.e., very hot or very cold, the better your throat recognizes it and remembers to swallow. I went through a few coughing fits and lots of mushed pancakes, but no feeding tube.
July/August 2005 11
>>continued on page 12
Kathy and her customized trike
Subject: Peeing, Rebirth & Velcro>> After running water, soaking my fingers in warm water and concentrating very hard, I learned to pee again. I still struggle with that four years later. I no longer get physically aroused either, that part of the brain is dead, too. A stroke impacts more than just the obvious, it’s like a rebirth of sorts. Everything you knew has to be relearned, unless you need two hands to do it — thank heavens for Velcro.
Subject: The Good Go to Heaven>> I was in a nursing home and then a rehab center for a while. Because of the stroke my knee hyper-extends and my foot drops and the ankle twists. My therapist wrapped my foot, pulling the toes up so I wouldn’t trip, and had me shuffle down the hall. I was hanging onto the railings for dear life — a death grip. I was scared, and this from a woman that has jumped out of an airplane! Then I went to a rehab center. They fitted me for a brace and gave me a cane — first a sturdy four-prong, then a wimpy single prong.
The day I left there, the therapist took me to the emergency stairs and said, “OK, Kathy, we’re gonna learn stairs now.” I gulped and she said, “Remember this: the good go to heaven, meaning your good foot goes up first. The bad go to hell, meaning your weak leg goes down first.” That’s how I learned steps before I moved back into our two-story house.
Subject: A Tornado through the Brain>> Everyone was surprised I felt things in my paralyzed hand, then I realized they thought I have no feeling on the side affected by my stroke. It’s paralyzed from movement but I still have feeling there; in fact, sometimes pain. A stroke is like a tornado through the message center of your brain. It’s a major communication breakdown between brain and body, for some even breathing is lost. For me it was movement, swallowing, peeing and short term memory that were most affected.
July/August 200512
July/August 2005 13
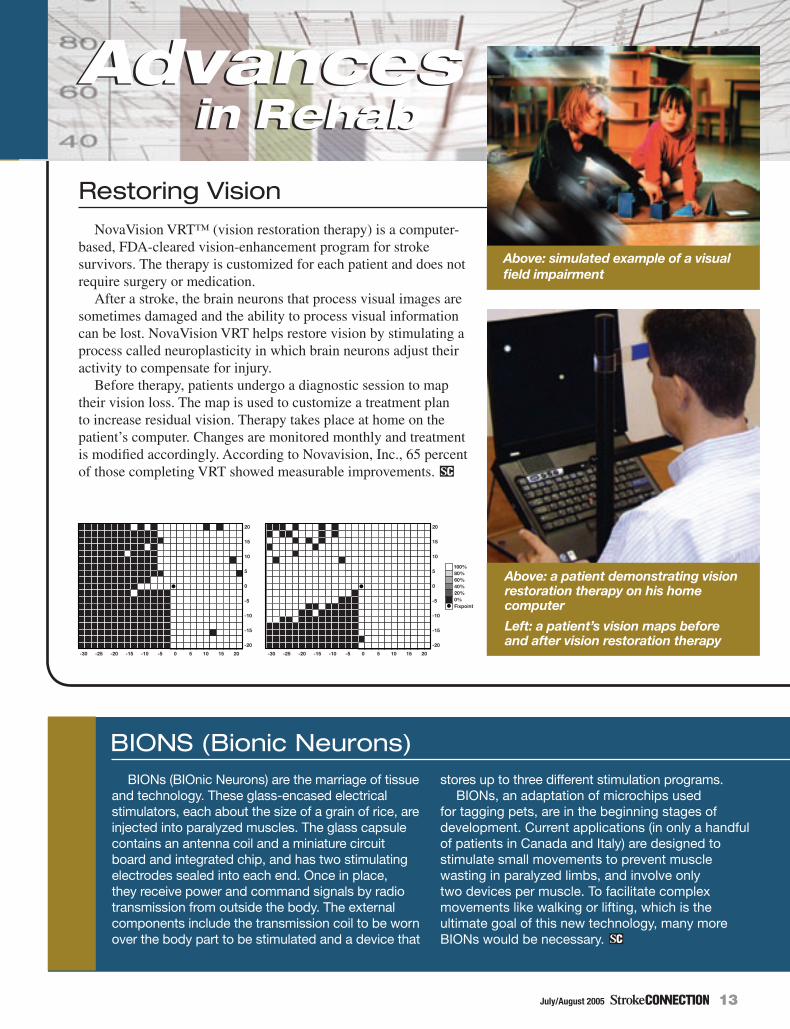
Restoring VisionNovaVision VRT™ (vision restoration therapy) is a computer-
based, FDA-cleared vision-enhancement program for stroke survivors. The therapy is customized for each patient and does not require surgery or medication.
After a stroke, the brain neurons that process visual images are sometimes damaged and the ability to process visual information can be lost. NovaVision VRT helps restore vision by stimulating a process called neuroplasticity in which brain neurons adjust their activity to compensate for injury.
Before therapy, patients undergo a diagnostic session to map their vision loss. The map is used to customize a treatment plan to increase residual vision. Therapy takes place at home on the patient’s computer. Changes are monitored monthly and treatment is modified accordingly. According to Novavision, Inc., 65 percent of those completing VRT showed measurable improvements.
in Rehab
BIONs (BIOnic Neurons) are the marriage of tissue and technology. These glass-encased electrical stimulators, each about the size of a grain of rice, are injected into paralyzed muscles. The glass capsule contains an antenna coil and a miniature circuit board and integrated chip, and has two stimulating electrodes sealed into each end. Once in place, they receive power and command signals by radio transmission from outside the body. The external components include the transmission coil to be worn over the body part to be stimulated and a device that
stores up to three different stimulation programs. BIONs, an adaptation of microchips used
for tagging pets, are in the beginning stages of development. Current applications (in only a handful of patients in Canada and Italy) are designed to stimulate small movements to prevent muscle wasting in paralyzed limbs, and involve only two devices per muscle. To facilitate complex movements like walking or lifting, which is the ultimate goal of this new technology, many more BIONs would be necessary.
����������������
��
��� ��� � �� �� ��������������
���
�
��
���
���
��
��
�
����������
Advances
����������������
��
��� ��� � �� �� ��������������
���
�
��
���
���
��
��
�
����������
in RehabAdvances
BIONS (Bionic Neurons)
Above: simulated example of a visual field impairment
Above: a patient demonstrating vision restoration therapy on his home computer
Left: a patient’s vision maps before and after vision restoration therapy
July/August 200514
F E A T U R E
Healing through
Music
usic touches
special places in almost
everyone — from the church
music we heard as children
to the rock ‘n’ roll we danced
to as teenagers. For these
survivors, music has taken on
a healing role, a way to get
beyond their deficits and find
joy where once there was only
despair. Whether they’ve
played before or are
learning anew,
music has helped
them make
connections
in their brains
and in their
communities.
by Jon Caswell
Healing through
Music

July/August 2005 15
Music is life for John Hopkins.A jazz pianist, the former Army sergeant-first class has
played for presidents and generals around the world, first as a member of the U.S. Army band system. After his military experience, he performed at musical venues throughout Europe and Asia. His performances came to a sudden and permanent end in October 1999.
As he was about to go onstage at the famous Grill Room of the Grand Hyatt Hotel in Tokyo, John had an embolic stroke that left him in a coma for 10 days. He was 46 years old. Doctors gave him 48 hours to live, and his sons, both in the military, flew in to be by his side.
“While I was in the coma,” John said, “my father, who had died of Alzheimer’s several years before, came to me. He said, ‘If you are ready to go, I will take you, but God has something else for you to do. He’s not ready for you to leave yet.’ I told him that I wasn’t ready to go, and at that moment I sat up in bed. For the first time in weeks I had a conversation that could be understood and made sense.”
John was in the Tokyo hospital for three months, but because he didn’t have insurance, he didn’t receive any therapy. Paralyzed on his right side, he also lost his speech,
or at least part of it. Then, on Christmas day 1999, with financial help from some friends, John flew out of Tokyo, lying down and still attached to medical equipment.
He arrived at his son’s home in Washington State, where he began therapy at a local hospital. That was interrupted when he went to Russia to be
with his life partner who was working in Moscow at that time. “When I went to Russia, I was in a wheelchair,” John said. “They worked with me there, and when I came back to the U.S. two months later, I was walking.”
He settled in Leavenworth, Kansas, to be near his son and a VA hospital. He could walk, but he still couldn’t use his right hand, and he knew his professional playing days were over. Restless and ready to be purposeful again, John began looking for another way to share his music with the
world. “So many friends and family members had helped me, I wanted to give something back.”
Out of this commitment, and in honor of his father, John contacted a local aging center. “My idea was to teach music to seniors, to stimulate the minds, bodies and spirits of people with mental and physical handicaps,” he said. Out of those visits, John has developed Age & Play, a nonprofit organization dedicated to teaching music to seniors.
In the three years since John started teaching, he has shared music with many handicapped seniors. Lessons last about 30 minutes, but are shorter for Alzheimer’s patients.
At one of the nursing homes, nurses told John of a woman who had not spoken for 15 years but who had taken piano lessons when she was younger. When he sat her down at the piano, she played beautifully, much to everyone’s surprise. “She’s still playing regularly,” said John.
John now teaches at three locations in Leavenworth, and the program has expanded to Kansas City, Kansas, and Colorado Springs, Colorado, where Age & Play board member Don Wagler handles the teaching duties. “We have recitals for our students so they can play for family and friends,” said John. “It gives them something to aim for.”
It gives something special to John, too. “When I see the courage and confidence my students have developed, when they perform before an audience of strangers or when my physically challenged students can memorize the terms that are meant to strengthen their minds, then I know we have achieved success. This is God’s way of saying to me, ‘Well done,’ and what more does one need?”
Jazzing Up Life for Others
H E A L I N G T H R O U G H M U S I C
“When I see the courage and
confidence my students have
developed, then I know we have
achieved success.”
John Hopkins working with an Age & Play client
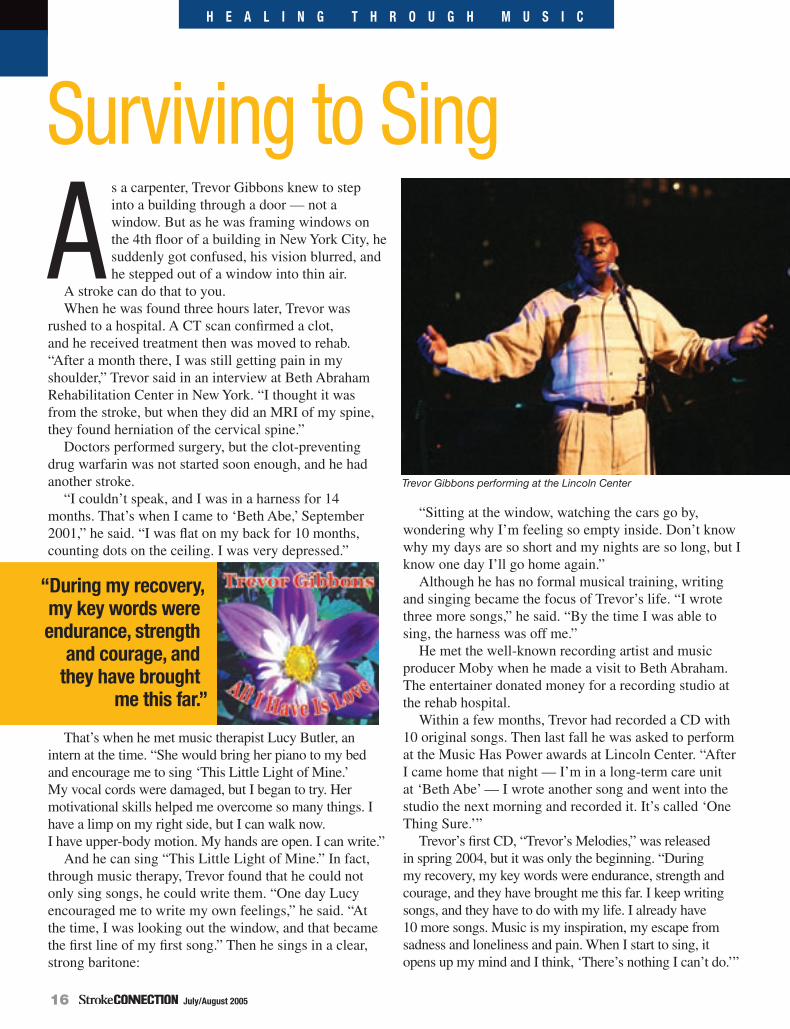
July/August 200516
As a carpenter, Trevor Gibbons knew to step into a building through a door — not a window. But as he was framing windows on the 4th floor of a building in New York City, he suddenly got confused, his vision blurred, and he stepped out of a window into thin air.
A stroke can do that to you. When he was found three hours later, Trevor was
rushed to a hospital. A CT scan confirmed a clot, and he received treatment then was moved to rehab. “After a month there, I was still getting pain in my shoulder,” Trevor said in an interview at Beth Abraham Rehabilitation Center in New York. “I thought it was from the stroke, but when they did an MRI of my spine, they found herniation of the cervical spine.”
Doctors performed surgery, but the clot-preventing drug warfarin was not started soon enough, and he had another stroke.
“I couldn’t speak, and I was in a harness for 14 months. That’s when I came to ‘Beth Abe,’ September 2001,” he said. “I was flat on my back for 10 months, counting dots on the ceiling. I was very depressed.”
That’s when he met music therapist Lucy Butler, an intern at the time. “She would bring her piano to my bed and encourage me to sing ‘This Little Light of Mine.’ My vocal cords were damaged, but I began to try. Her motivational skills helped me overcome so many things. I have a limp on my right side, but I can walk now. I have upper-body motion. My hands are open. I can write.”
And he can sing “This Little Light of Mine.” In fact, through music therapy, Trevor found that he could not only sing songs, he could write them. “One day Lucy encouraged me to write my own feelings,” he said. “At the time, I was looking out the window, and that became the first line of my first song.” Then he sings in a clear, strong baritone:
“Sitting at the window, watching the cars go by, wondering why I’m feeling so empty inside. Don’t know why my days are so short and my nights are so long, but I know one day I’ll go home again.”
Although he has no formal musical training, writing and singing became the focus of Trevor’s life. “I wrote three more songs,” he said. “By the time I was able to sing, the harness was off me.”
He met the well-known recording artist and music producer Moby when he made a visit to Beth Abraham. The entertainer donated money for a recording studio at the rehab hospital.
Within a few months, Trevor had recorded a CD with 10 original songs. Then last fall he was asked to perform at the Music Has Power awards at Lincoln Center. “After I came home that night — I’m in a long-term care unit at ‘Beth Abe’ — I wrote another song and went into the studio the next morning and recorded it. It’s called ‘One Thing Sure.’”
Trevor’s first CD, “Trevor’s Melodies,” was released in spring 2004, but it was only the beginning. “During my recovery, my key words were endurance, strength and courage, and they have brought me this far. I keep writing songs, and they have to do with my life. I already have 10 more songs. Music is my inspiration, my escape from sadness and loneliness and pain. When I start to sing, it opens up my mind and I think, ‘There’s nothing I can’t do.’”
Surviving to SingH E A L I N G T H R O U G H M U S I C
“During my recovery, my key words were endurance, strength
and courage, and they have brought
me this far.”
Trevor Gibbons performing at the Lincoln Center
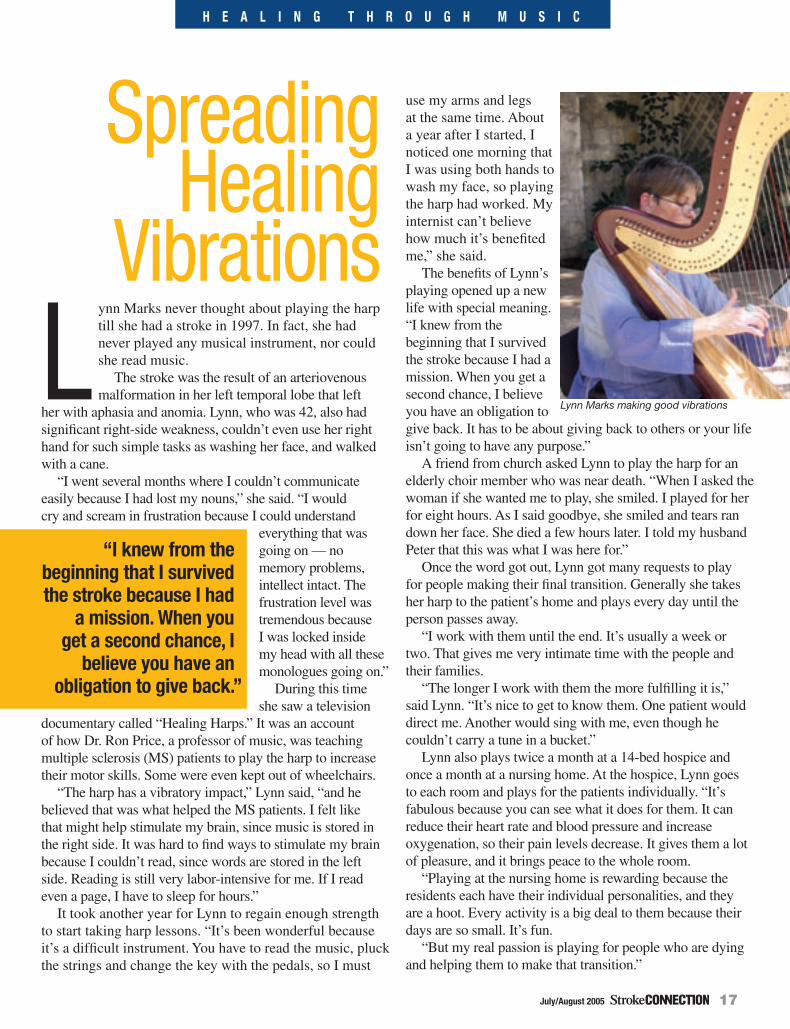
July/August 2005 17
Lynn Marks never thought about playing the harp till she had a stroke in 1997. In fact, she had never played any musical instrument, nor could she read music.
The stroke was the result of an arteriovenous malformation in her left temporal lobe that left
her with aphasia and anomia. Lynn, who was 42, also had significant right-side weakness, couldn’t even use her right hand for such simple tasks as washing her face, and walked with a cane.
“I went several months where I couldn’t communicate easily because I had lost my nouns,” she said. “I would cry and scream in frustration because I could understand
everything that was going on — no memory problems, intellect intact. The frustration level was tremendous because I was locked inside my head with all these monologues going on.”
During this time she saw a television
documentary called “Healing Harps.” It was an account of how Dr. Ron Price, a professor of music, was teaching multiple sclerosis (MS) patients to play the harp to increase their motor skills. Some were even kept out of wheelchairs.
“The harp has a vibratory impact,” Lynn said, “and he believed that was what helped the MS patients. I felt like that might help stimulate my brain, since music is stored in the right side. It was hard to find ways to stimulate my brain because I couldn’t read, since words are stored in the left side. Reading is still very labor-intensive for me. If I read even a page, I have to sleep for hours.”
It took another year for Lynn to regain enough strength to start taking harp lessons. “It’s been wonderful because it’s a difficult instrument. You have to read the music, pluck the strings and change the key with the pedals, so I must
use my arms and legs at the same time. About a year after I started, I noticed one morning that I was using both hands to wash my face, so playing the harp had worked. My internist can’t believe how much it’s benefited me,” she said.
The benefits of Lynn’s playing opened up a new life with special meaning. “I knew from the beginning that I survived the stroke because I had a mission. When you get a second chance, I believe you have an obligation to give back. It has to be about giving back to others or your life isn’t going to have any purpose.”
A friend from church asked Lynn to play the harp for an elderly choir member who was near death. “When I asked the woman if she wanted me to play, she smiled. I played for her for eight hours. As I said goodbye, she smiled and tears ran down her face. She died a few hours later. I told my husband Peter that this was what I was here for.”
Once the word got out, Lynn got many requests to play for people making their final transition. Generally she takes her harp to the patient’s home and plays every day until the person passes away.
“I work with them until the end. It’s usually a week or two. That gives me very intimate time with the people and their families.
“The longer I work with them the more fulfilling it is,” said Lynn. “It’s nice to get to know them. One patient would direct me. Another would sing with me, even though he couldn’t carry a tune in a bucket.”
Lynn also plays twice a month at a 14-bed hospice and once a month at a nursing home. At the hospice, Lynn goes to each room and plays for the patients individually. “It’s fabulous because you can see what it does for them. It can reduce their heart rate and blood pressure and increase oxygenation, so their pain levels decrease. It gives them a lot of pleasure, and it brings peace to the whole room.
“Playing at the nursing home is rewarding because the residents each have their individual personalities, and they are a hoot. Every activity is a big deal to them because their days are so small. It’s fun.
“But my real passion is playing for people who are dying and helping them to make that transition.”
Spreading Healing
Vibrations
H E A L I N G T H R O U G H M U S I C
“I knew from the beginning that I survived the stroke because I had
a mission. When you get a second chance, I
believe you have an obligation to give back.”
Lynn Marks making good vibrations
July/August 200518
����������������������������
�������������������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������
���������������������������������������������������������
�������������������������
����������������������������������������������������������������������������������������������������������������������������������������������������������
���������������������� ���������������������
Kay Breslin had always had music in her life.
She had been studying jazz with piano teacher Mark Miller for several years, when an arteriovenous malformation ruptured in August 1998 and paralyzed her left side. “After a lot of prayer and therapy, I got back on my feet,” she said from her home in Barrington, Illinois. But her left hand didn’t come back, and she gave up the piano because there’s not much music for one-handed piano players.
“Despite the urging of friends and family to get back to music, I wouldn’t even give it a try,” she said. Then a friend called Mark and commissioned him to make a musical arrangement for one hand as a birthday present for Kay. Intrigued by the gift, she started to practice.
H E A L I N G T H R O U G H M U S I C
In Tune with One-Handed Jazz
July/August 2005 19
Every thoughtful husband and wife knows the time eventually will come when one of them will have to carry on alone, and perhaps spend many years as a widow or widower. The American Heart Association has prepared a practical, supportive brochure to help spouses prepare for life without their marriage partner. It will help you be ready “when the time comes” not only to handle the details and decisions that follow a spouse’s death, but also to deal with financial and practical matters – in short, to resume life as effectively as possible.
For more information, please visit us at americanheart.org/plannedgiving or e-mail us at [email protected].
Please send to: American Stroke Association Planned Giving Department 7272 Greenville Avenue Dallas, TX 75231-4596
c Please send me the free booklet When the TimeComes. (CCA)
c Please have a representative contact me to discuss how charitable estate planning can benefit me. (CCD)
c I am considering a gift to the American Stroke Association through my estate plan. (CCC)
c I have already included the American Stroke Association in my will/estate plan. (CCB)
KC-0154
06APGAA
When the time comes for one of you to carry on.
IAD SC 07/05
Name
Address
City
State ZIP
Phone
Birthdate E-mail
H E A L I N G T H R O U G H M U S I C
“It took about a week for me to master that piece,” said Kay. “When I saw that I was able to do it, I had Mark start coming to the house every week. I spend two hours a day practicing the pieces he brings. I’ve probably learned 20 to 25 pieces. Each arrangement seemed to get a little more difficult, so I was always being challenged. I’m always working on something new.”
Mark has worked with several stroke survivors like Kay. Although he goes to her house, he also gives lessons over the phone. And on a recent visit to Scottsdale, Arizona, Kay took her lessons long distance. “It was great,” she said, “because I got to continue my progress.”
Mark enjoys teaching people to play with one hand, but he notes that there aren’t many
arrangements. “And 95 percent of those that are available are for classical pieces and are written for the left hand only, so they wouldn’t have been much good to Kay,” said Mark. “Writing for one hand necessitates putting both harmony and melody within the reach of just one hand, which is about eight keys.”
Although Kay was a musician before her stroke, Mark is certain that a survivor without prior musical training could learn to play with one hand. “I write the arrangement to match the skill level of the individual student,” said Mark. “If they have a phone and a keyboard, they can learn to play jazz piano.”
For more information, contact Mark at [email protected] or 1-800-327-4266.

July/August 200520
H E A L I N G T H R O U G H M U S I C
revor Gibbons (“Surviving to Sing,” p. 16) benefited
from the specific intervention of a music therapist. History is on his side.
Interest in the therapeutic value of music goes back about 2,400 years to Plato and Aristotle, but the modern professional discipline began only after WW II. Today music therapy is used in a wide range of rehab settings.
Dr. Connie Tomaino, who is both a doctor of music therapy and a board-certified music therapist (MT-BC), is vice president of music therapy at Beth Abraham Family of Health Services in New York City. She explained that music therapy can be part of rehab from assessment through treatment.
Music therapy has proven effective in improving balance
and gait as well as improving speech, memory function, attention and focus.
“The end result of music therapy is not necessarily to play music but to enhance mental function, speech production and breathing,” she said recently. “Music therapy helps patients who can’t control their muscles to organize motor movement.
“When people are spontaneously involved in an activity, they may move in ways they couldn’t if they thought about
it. That’s because in a lot of head injuries, there’s damage to what is called executive function, which is the ability to plan out and perform a task. Although there may be functionality that allows the muscle to move, the person may be more likely to move it if we can stimulate the muscle through a different network.
“When a person is encouraged to use their affected side, say with a keyboard,” said Dr. Tomaino, “they have to acknowledge that limb exists. Calling attention to that neglected side increases the chance that they will move that side at will.”
Survivors who can’t talk may be able to sing, as was the case with Trevor, who also regained his speech. “These abilities — whether speech or rhythmic movement
— are stored in people. The trick is how to get those networks lit up.
“Singing and speech use a parallel mechanism, so skills used to sing words may carry over to regular speech. Songs with predictable lyrics, popular songs and songs from childhood may be easier for survivors to sing than unfamiliar music.”
Many patients with brain injuries lack the attention span to perform a series of steps. But when music is added, often they can focus long enough to accomplish the movement. “Following is less difficult than initiating, so they can accomplish the same physical goals without having to instruct themselves how to do them,” Dr. Tomaino said.
Music, whether playing, singing, listening or writing, is always involved in a music therapy session. The goal is to involve the patient in responding. “We use a wide range of instruments. We use a lot of digital instruments because you can adjust the output. For instance, turning up the volume on digital drums allows someone who is weak to hear the effect, which can be very motivating.”
Insurance reimbursement for music therapy varies from state to state.
Accredited music therapists must earn a college degree in music therapy and pass a national certification exam. They carry the MT-BC credential. For help in locating a music therapist, contact the American Music Therapy Association at 301-589-3300 or send an e-mail to [email protected].
What is Music Therapy?
Dr. Connie Tomaino
July/August 2005 21
American Heart Association and American Stroke Association are passionate about stopping heart disease and stroke, and they
want others to share that passion. That’s why they recently launched Heart Disease and Stroke. You’re the Cure, a campaign to motivate volunteers to take action on important legislative issues.
Along with the new look and feel for the association’s advocacy efforts, the AHA/ASA has also developed a more effective approach to communicate its advocacy messages by evoking passion through its new grassroots You’re the Cure network.
“The new advocacy theme denotes action and makes individuals feel that by being an advocate for the AHA/ASA they are a part of the solution to the problems of heart disease and stroke,” said Katherine Krause, AHA’s executive vice president of advocacy. “We hope that by acting, networkers will feel that they have achieved something meaningful for themselves and their families.”
Lobbyist.
The AHA/ASA have worked to convince the National Institutes of Health to increase stroke research funding, and are currently lobbying on behalf of the STOP Stroke Act, which would increase public awareness of stroke and promote improved treatment measures.
Over the years, the AHA/ASA have achieved numerous health policy victories. In large part, these victories are due to dedicated volunteers and advocates across the country. These supporters are not lobbyists by profession, however, they are survivors and caregivers, healthcare professionals, as well as everyday people who realize that small actions can make a huge difference in the fight to save lives.
AHA/ASA network advocates have sent over 30,000 e-mails and have placed nearly 3,000 calls to lawmakers during the past year alone. This April, over 500 of them participated in AHA’s annual Lobby Day in Washington, D.C. The You’re the Cure network aims to increase participation and instill greater passion
in AHA/ASA’s efforts to support public health policies that fight heart disease and stroke.
As a stroke survivor, caregiver or family member, you have first-hand experience of the devastating effects cardiovascular disease can have. Therefore, we need you to lend your voice to important stroke issues. With just a quick phone call or e-mail to your legislators, you can inform them how the disease has affected you personally and why it’s essential to pass the STOP Stroke Act. Your voice and those of other stroke survivors can and will be heard.
Taking part in this new initiative will provide additional meaning to you and your family, as well as the American Stoke Association. Please detach the sign-up form on the next page or visit www.americanheart.org/yourethecure and join today!
“We hope that by acting, networkers will feel that they
have achieved something meaningful for themselves
and their families.”
Stroke. You’re the Cure.
July/August 200522
July/August 2005 23
y now, you probably have heard a lot about Medicare reform — the Medicare Prescription Drug Improvement and
Modernization Act of 2003. Digesting the facts of the entire program would be like binging on a large meal, but breaking down the new provisions into small nuggets makes the information more palatable.
If you have Medicare, or plan to apply for it when you reach age 65, this information will help you make good healthcare decisions. Remember
that Medicare Part A, which helps cover hospital stays, skilled nursing care, home health care and hospice care, requires no monthly premium for most people who paid Medicare taxes while working. Part B, which helps cover doctor bills, outpatient care and some expenses not covered in Part A, requires a monthly premium in 2005 of $78.20 and an annual deductible of $110, up from $100 for the past 14 years.
These parts make up the standard Medicare plan, called the Original Medicare Plan. This fee-for-service plan in which most Medicare
recipients are enrolled usually pays 80 percent of an approved amount, after the deductible, for most services.
Changes mentioned here fall into three categories: prescription drug plans, preventive benefits and health plan choices.
The prescription drug plans, perhaps the most talked-about change in the law, are either the best innovation since sliced bread or the worst thing that could happen to Medicare, depending on who is talking. But we will stick to basics here and leave the debate to the politicians and analysts.
Examining Medicare
Reformby Mike Mills
Prescription Drug Plans
This Medicare Part D program starts in 2006 and is entirely voluntary (see chart on page 24):
1. A prescription drug plan requires a monthly premium of about $35. The actual premium can vary by plan and geographic area.
2. After paying the first $250 for medicine in a calendar year, you pay 25 percent up to $2,250.
3. This is where the “doughnut hole” deductible begins — you pay 100 percent of your prescriptions until the total reaches $5,100. At this point, you will have paid $3,600 out-of-pocket (plus the $35 monthly premium).
4. For expenses beyond $5,100, you pay about 5 percent and Medicare picks up the rest.
5. Low-income people will get extra help to pay their drug bills. Multiple levels of low-income assistance exist. In one example, seniors with incomes below $12,123 in annual income for an individual or $16,362 for a couple and with assets under $6,000 for an individual or $9,000 for a couple (not including the value of a home or car) will be able to buy drugs for $1 to $2 for generic prescriptions and for $3 to $5 for brand names.
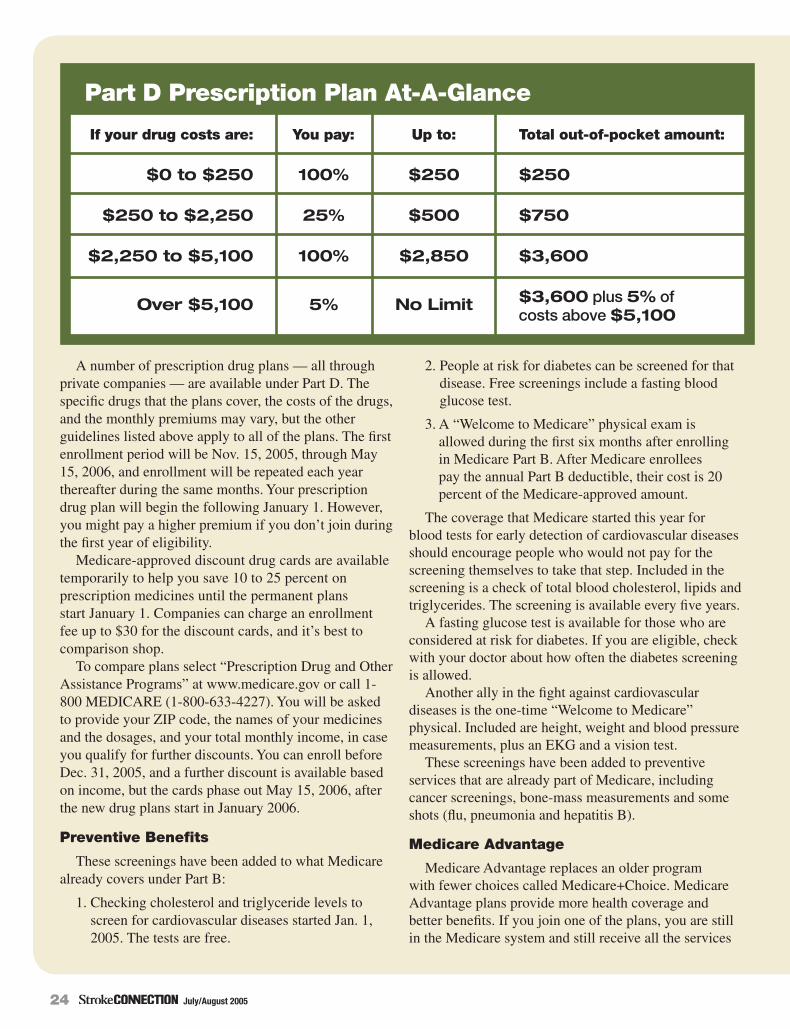
July/August 200524
A number of prescription drug plans — all through private companies — are available under Part D. The specific drugs that the plans cover, the costs of the drugs, and the monthly premiums may vary, but the other guidelines listed above apply to all of the plans. The first enrollment period will be Nov. 15, 2005, through May 15, 2006, and enrollment will be repeated each year thereafter during the same months. Your prescription drug plan will begin the following January 1. However, you might pay a higher premium if you don’t join during the first year of eligibility.
Medicare-approved discount drug cards are available temporarily to help you save 10 to 25 percent on prescription medicines until the permanent plans start January 1. Companies can charge an enrollment fee up to $30 for the discount cards, and it’s best to comparison shop.
To compare plans select “Prescription Drug and Other Assistance Programs” at www.medicare.gov or call 1-800 MEDICARE (1-800-633-4227). You will be asked to provide your ZIP code, the names of your medicines and the dosages, and your total monthly income, in case you qualify for further discounts. You can enroll before Dec. 31, 2005, and a further discount is available based on income, but the cards phase out May 15, 2006, after the new drug plans start in January 2006.
Preventive Benefits
These screenings have been added to what Medicare already covers under Part B:
1. Checking cholesterol and triglyceride levels to screen for cardiovascular diseases started Jan. 1, 2005. The tests are free.
2. People at risk for diabetes can be screened for that disease. Free screenings include a fasting blood glucose test.
3. A “Welcome to Medicare” physical exam is allowed during the first six months after enrolling in Medicare Part B. After Medicare enrollees pay the annual Part B deductible, their cost is 20 percent of the Medicare-approved amount.
The coverage that Medicare started this year for blood tests for early detection of cardiovascular diseases should encourage people who would not pay for the screening themselves to take that step. Included in the screening is a check of total blood cholesterol, lipids and triglycerides. The screening is available every five years.
A fasting glucose test is available for those who are considered at risk for diabetes. If you are eligible, check with your doctor about how often the diabetes screening is allowed.
Another ally in the fight against cardiovascular diseases is the one-time “Welcome to Medicare” physical. Included are height, weight and blood pressure measurements, plus an EKG and a vision test.
These screenings have been added to preventive services that are already part of Medicare, including cancer screenings, bone-mass measurements and some shots (flu, pneumonia and hepatitis B).
Medicare Advantage
Medicare Advantage replaces an older program with fewer choices called Medicare+Choice. Medicare Advantage plans provide more health coverage and better benefits. If you join one of the plans, you are still in the Medicare system and still receive all the services
If your drug costs are:
Part D Prescription Plan At-A-Glance
$0 to $250
$250 to $2,250
$2,250 to $5,100
Over $5,100
100%
25%
100%
5%
$250
$500
$2,850
No Limit
$250
$750
$3,600
$3,600 plus 5% of costs above $5,100
You pay: Up to: Total out-of-pocket amount:
July/August 2005 25
that Medicare covers. Advantage consists of four plans: managed care, preferred provider organizations (PPOs), private fee-for-service and specialty.
1. Managed care plans require you to see doctors in a network. You may need to choose a primary care doctor and get a referral to see a specialist. Co-payments usually are lower than those under the Original Medicare Plan.
2. Preferred provider organization plans (PPOs) allow you to see any doctor without referral, but seeing doctors in the network costs less. In 2006, regional PPOs will limit the out-of-network amount that members pay.
3. A private fee-for-service plan allows you to see any doctor that accepts the plan’s payment.
4. Specialty plans provide more focused care for certain people.
The Advantage Plans are all part of Medicare, and anyone who already has Medicare Part A and Part B can choose any of them. A plan may require you to pay an extra premium for the extra benefits you receive, or it may pay part or all of your Part B premium. The specialty plans, designed to treat people with special medical conditions, may not be available everywhere.
No one is required to use any plan other than the Original Medicare Plan. You will stay in the Original Plan unless you join an Advantage Plan. Medicare enrollees continue to use their red, white and blue cards.
Therapy Caps Moratorium
In 1997, Congress placed a $1,500 cap on benefits for outpatient physical and speech therapy, and a $1,500 cap on occupational therapy benefits. Congress has blocked their enforcement ever since 1998. The current two-year moratorium expires at the end of this year and would force some seniors and people with disabilities to pay out-of-pocket expenses for therapy or alter the course of their care by changing providers or facilities.
Congress is working on a bill now to get rid of the caps for good. “We are confident that Congress will do what is right and do away with this burden for Medicare beneficiaries once and for all by passing this legislation,” Ben F. Massey Jr., president of the American Physical Therapy Association, said recently.
What Is Not Covered
Medicare coverage seems so comprehensive that it may be helpful to point out a few of the areas that lack coverage under the Original Plan. Of course, additional benefits from the Advantage Plans may cover some of these expenses.
Not covered by Parts A and B in the Original Plan:
Acupuncture
Custodial care (help with bathing, dressing, eating, using the bathroom) in the home or in a nursing home
Deductibles, coinsurance and co-payments
Dental care, dentures
Hearing aids and hearing screenings
Long-term care (such as custodial care)
Routine or annual physical examinations
Routine eye care and most eyeglasses
Routine foot care
Screening and lab tests (except those listed on pages 26-28 of “Medicare and You 2005”)
Shots and vaccinations (except those listed under Preventive Benefits)
Some diabetic supplies
Find Out More
The www.medicare.gov Web site provides excellent information about what Medicare covers. To see answers to questions you may have, try the link “Frequently Asked Questions.” Going to www.medicare.gov/publications/pubs/pdf/10050.pdf will start a download of “Medicare and You 2005,” the official government handbook on Medicare. It’s well organized and easy to read. Or call 1-800 MEDICARE (633-2273) to ask questions.
July/August 200526
“The lower the better for high-risk people — that’s the message on bad (LDL) cholesterol from recent clinical trials,” said Scott Grundy, M.D., Ph.D.
Dr. Grundy, director of the Center for Human Nutrition at the University of Texas Southwestern Medical Center in Dallas, was commenting on guidelines from the National Cholesterol Education Program (NCEP) that were updated earlier this year. The guidelines now urge more intensive cholesterol treatment for people at high risk for stroke, heart attack and death from cardiovascular disease.
September is National Cholesterol Awareness Month. High cholesterol is a major risk factor for cardiovascular disease.
After examining five major clinical trials involving cholesterol-lowering medications, the panel concluded that people at high risk could benefit from even lower LDL numbers, below 70 mg/dL. This means that high-risk patients may still be considered for cholesterol-lowering drug therapy, even if their cholesterol is below 100. (For definitions of high and very high risk, see “What Is High Risk” on p. 27.)
Two SourcesIn a recent survey, 77 percent of the respondents
(representing more than 1,000 patients reported as having high cholesterol) stated incorrectly that the food they eat contributes the most to high cholesterol. In fact, the cholesterol in the bloodstream is not just absorbed from food; the majority is produced naturally in the body.
“The fact is that both diet and heredity play a critical role in your cholesterol levels,” said Dr. David Cohen, director of hepatology at Brigham and Women’s Hospital in Boston. “While diet can contribute significantly to elevated cholesterol, the body’s natural chemistry can often produce dangerously high levels of LDL cholesterol based on heredity alone. When working with a physician to manage your condition, it is important to understand that there are two sources of cholesterol and in many cases both need to be addressed.”
Because cholesterol is used in all the body’s cells, it travels through the bloodstream. But cholesterol and other fats cannot dissolve in the blood and must travel to and from the cells via special carriers called lipoproteins. These are the famous “siblings” HDL (high-density lipoprotein) and LDL (low-density lipoprotein).
Since there are two sources of cholesterol, there are at least two ways of treating hypercholesterolemia — or too much cholesterol.
“Beyond lifestyle considerations, there are many effective treatment options available for control of high cholesterol,” said Dr. Cohen. “I always counsel patients to discuss treatment options with their doctor. Patients with high cholesterol should make an extra effort to be as informed about their cholesterol levels as possible. Knowing about the sources of cholesterol is a key step in this process.”
A cholesterol-lowering plan should include lifestyle steps as well as drug therapies to lower risk, members of the Adult Treatment Panel of NCEP said.
Maintaining a heart-healthy lifestyle is important. “The idea that you can use cholesterol-lowering drugs without lifestyle changes is incorrect,” said Dr. Grundy. “Lifestyle changes have enormous benefits beyond lowering LDL cholesterol, such as raising good cholesterol, lowering triglycerides, improving diabetes and reducing inflammation.”
New Information for High-Risk Patientsby Jon Caswell
Cholesterol:
July/August 2005 27
What is High Risk? In the NCEP study, the high-risk category includes people who have
• A history of heart attack
• Carotid artery disease, a transient ischemic attack (TIA) or an ischemic stroke
• Unstable angina
• Previous coronary artery procedures, such as angioplasty or bypass surgery
• Peripheral artery disease
• Abdominal aortic aneurysm
• Diabetes
Those who have two or more risk factors (smoking, uncontrolled hypertension, diabetes, obesity) with
a greater than 20 percent risk of heart attack or death in the next 10 years are also considered to be at high risk.
The recommendations call for those at high risk, to reduce their LDL numbers below 100 mg/dL (milligrams per deciliter).
What is Very High Risk? Patients are considered at very high risk if they already have cardiovascular disease plus
• Diabetes
• Persistent cigarette smoking
• Poorly controlled hypertension
• Multiple risk factors of the metabolic syndrome (high triglycerides, low levels of “good” HDL cholesterol, obesity)
• Individuals are also at high risk immediately after a heart attack.
For those who are at very high risk, the recommendations call for reducing their LDL numbers below 70 mg/dL.
For an online assessment of your risk, take the “Learn and Live” quiz at www.americanheart.org.
July/August 200528
Lifeat the
curb
I had my stroke on my honeymoon and lost the use of my left arm and leg. I was in two different hospitals for a total of two months, 47 years old, and facing what seemed to me an eternity of rehab. I couldn’t wait to escape and get back home to my apartment in New York City. Even though I knew I wasn’t magically cured (after all, I was still in a wheelchair), I was learning to walk with a cane. Still, I was no Lance Armstrong.
Before my release date, the hospital, apparently concerned for my well-being, sent a team of therapists to my apartment to make sure it was physically safe for me. Evidently they were going to stroke-proof it, like you child-proof an apartment. I thought these must be the CVA FSST: The Cerebral Vascular Accident Feng Shui Stroke Team.
Here is what I expect the guidelines must be to complete a stroke-proofing procedure. (Insert Mission Impossible music)
9 a.m.: Enter apartment. Immediately notice area rugs just lying there waiting to be tripped over. Instantly spring into action and rip duct tape off the rolls hanging off your toolbelt. Secure the area (rugs, that is) by taping them to the floor. Use as much tape as possible because the hospital is paying for it and this guy’s insurance is paying the hospital. The survivor may complain his apartment looks like it’s being shipped to Anchorage, Alaska. Suggest that he take his name off the door and write “Fragile. This end up.”
11 a.m.: Having run out of tape, hit the bathroom. The priority here is the toilet. Replace the regular toilet seat with the higher stroke survivor regulation seat. Code name: The Matterhorn.
The survivor may complain because he’ll need a ladder to get to the toilet and he probably can’t
even go up stairs yet. Ease his mind by telling him once he gets on the toilet his feet will dangle like he is potty training again, allowing him to relive those innocent moments of his youth, though he may need Dramamine to go to the bathroom.
12 p.m.: Turn your attention to the shower. Install bars in the shower. No need to concern yourself with where to install the bars, just install them all over. The survivor may feel like he’s showering in a jungle gym. Reassure him that all he needs is a slide coming off the toilet and his whole bathroom would be a playscape. Again, just like when he was a kid.
1 p.m.: Recommend the survivor have a healthcare attendant with him at all times because it’s not safe for him to be alone in his own apartment. Well, the hospital calls them healthcare attendants. But after meeting my first one, Maurice, I call them babysitters or convicted felons. But that’s a whole other story…
Editor’s Note: Read John’s personal stroke story, “Life is at the Curb,” from the September/October 2003 issue of Stroke Connection at strokeassociation.org/strokeconnection, or book his one-man show about stroke recovery, “Brain Freeze,” by contacting him at [email protected].
John Kawie’s
Ladies and gentlemen...please welcome comedian and stroke survivor john
kawie as we debut his regular humor column,
“Life at the curb.”
Operation“Stroke-Proof”
The hospital sent to my apartment the CVA FSST: The Cerebral Vascular
Accident Feng Shui Stroke Team.
John Kawie

July/August 2005 29
Call Us Toll Free: 888-274-2742 www.aphasia.com
Do you have aphasia?
Never stop recovering. Simple to use, powerful and effective—the Lingraphica provides clinically proven communication and practice for adults with aphasia.
Covered by Medicare.
New design addresses a wide range of motor issues.
Touch screen available
• Sudden numbness or weakness of the face, arm or leg, especially on one side of the body
• Sudden confusion, trouble speaking or understanding
• Sudden trouble seeing in one or both eyes
• Sudden trouble walking, dizziness, loss of balance or coordination
• Sudden, severe headache with no known cause
know...THE WARNING SIGNS OF STROKE:
July/August 200530
survival Connecting You to Helpful Ideas
E V E R Y D A Y
Medicines sold without a prescription are called over-the-counter (OTC) medicines.
About 1,000 active ingredients are present in more than 100,000 OTC products, reported the Consumer Healthcare Products Association in 2001. Retail sales for OTC meds reached $17.2 billion in 2002 — and that doesn’t include Wal-Mart, according to ACNielsen researchers.
The positive impact that OTC medications have on our health is also considerable. Northwestern University researchers found that OTCs used to treat upper respiratory infections saved consumers $4.75 billion in 2004.
Because OTC medications are so readily accessible and affordable, we often think little of taking them. While OTC medicines are safe, they can present problems if taken with prescription medications that can
interact with their active ingredients. That’s why it’s so important to tell your doctor and pharmacist what OTC medications you use, and to keep them up to date.
Types of OTC MedicationsOTC medicines most commonly used fall into four main categories:
Pain relievers: Commonly used for treating everything from minor headaches and chronic pain to fever. Aspirin is the most familiar type, but the category also includes nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen, as well as acetaminophen.
Antihistamines: Effective in fighting cold, flu and allergy symptoms, especially the itching, sneezing and runny nose that often accompany these ailments.
Decongestants: Contain pseudoephedrine to narrow the blood vessels in the lining of your nose, reducing the amount of swelling in your nasal passages.
Cough medicines: Two types — antitussives (which suppress coughing) and expectorants (which clear mucus from the airways, so coughing is better able to clear it away).
Medicine Dos and Don’tsSafety is the key word for all medicines. You can be sure you’re using medicine safely by following a few basic guidelines:
• Do read the label carefully.
• Do take your medicine exactly as your doctor tells you to.
• Do make sure that each of your doctors and your pharmacist has a list of all the medicines you’re taking.
• Do ask your doctor or pharmacist questions about your medications, supplements and any possible interactions.
• Do make sure everyone you live with knows what medicines you’re taking and when you’re supposed to take each one.
• Don’t combine prescription medicines with OTC medicines unless your doctor says it is OK.
Without a Prescription:What You Need to Know About OTC Medicines by Sam Gaines
July/August 2005 31
• Don’t take anyone else’s medicine.
• Don’t use medicine after its expiration date.
• Don’t crush, break or chew tablets or capsules unless your doctor tells you to. Some medicines aren’t effective unless they are swallowed whole.
Get Informed, Stay InformedUnderstanding your OTC medicines and how they may
interact with your prescription medications is essential. Of course, the more prescription medications you take, the more important it is to understand how they interact, and how they may interact with any OTC medicines you are considering.
One good way to get information about your OTC medicine is to read the label. If you understand what you’re looking at, you might find answers to your questions there. Here’s what to look for:
Active ingredient. This is the chemical compound that does the actual work of the medicine. Sometimes there is more than one.
Uses. Sometimes called “indications,” these are the symptoms that the medicine is supposed to treat. The FDA must approve these listings.
Warnings. Pay close attention to this information. It’s a listing of what medicines, foods or situations to avoid while using this medication.
Directions. This information will tell you how much and when to take the medicine.
Other information. If there are any other special instructions for how to store or use the medicine, they will appear here.
Inactive ingredients. Every medicine includes some compounds that, while serving no purpose in treating symptoms, play important roles in holding the compounds together, preserving the active ingredients, etc.
Questions or comments. Here’s where you find the toll-free number to call if you have any questions or comments about the medicine.
It’s a good idea to get help from family or friends with understanding and taking your medications. It’s also smart to keep a record that shows clearly what each medicine is, how often you should take it, any special instructions about taking it, and when you are taking each medicine each day.
Effects and InteractionsAny drug can cause side effects. Many side effects are mild, but some can be severe. In addition, many drugs can interact with other drugs, or even with food or OTC medicines. These interactions can also range from minor to life-threatening. That’s why taking care to avoid dangerous interactions is always a smart idea.
Here are a few well-known drug-drug and drug-food interactions:
Aspirin and blood-thinners, such as warfarin, can lead to excessive bleeding.
Certain antacids can prevent some medications, such as antibiotics, blood-thinners and heart medications, from being properly absorbed into the blood, making the medicine less effective than it should be — or completely ineffective.
Decongestants can interact with anti-hypertension drugs or MAO-inhibiting antidepressants to cause harmful increases in blood pressure.
Some herbal supplements can interact with medications to cause significant problems, too. For example, ginkgo inhibits blood clotting, which can cause serious problems if taken by someone on anticoagulants or blood thinners. Also, kava kava can add to the effects of muscle relaxants, sedatives and antidepressants.
Vitamins and minerals can also interact with your medicines. Ferrous sulfate — a type of iron — can cancel out the effects of tetracycline, a frequently prescribed antibiotic.
Certain foods and beverages can also interfere with the effectiveness of your medicines. For example, grapefruit juice can cause problems with some blood pressure-lowering medicines, the antihistamine terfenadine and the transplant rejection-countering drug cyclosporine. And alcohol can interact negatively with a variety of prescription and OTC medicines.
The best ways to learn about what effects and potential interactions your OTC medicines, herbal supplements, and vitamins and minerals may cause is to read the labels carefully and talk with your doctor and pharmacist.
Sources:
http://nihseniorhealth.gov/takingmedicines/toc.html
http://www.fda.gov/cder/consumerinfo/WhatsRightForYou.htm
http://familydoctor.org/otc.xml
http://www.fda.gov/cder/consumerinfo/OTClabel.htm
http://www.niapublications.org/engagepages/medicine.asp
July/August 200532
Herbal Remedies and Dietary Supplements: Buyer BewareThey often look professionally packaged and carefully labeled with health information, but the fact is that herbal remedies and dietary supplements are not governed by the same rigorous testing and requirements that prescription medicines must go through. Thus, there is no way of knowing for sure whether what the label says is the same as what’s actually in the product.
If you use these products, be sure to tell your doctor and pharmacist what you’re using, how much and how often. Even if supplements and herbal remedies are truthfully labeled and properly manufactured, there’s no guarantee they’re safe. Just because something is advertised as “organic” or “natural” doesn’t mean it’s good for your health.
survival Connecting You to Helpful Ideas
E V E R Y D A Y
The National Council on Patient Information and EducationA March 2005 Harris Interactive Poll found that 33 percent of Americans report that they often or very often do not comply with their prescription’s directions. The National Council on Patient Information and Education wants to change that.
A 22-year-old patient advocacy group, NCPIE is a diverse coalition of more than 130 organizations dedicated to safer, more effective medicine use through better communication. The council’s TalkAboutRx.org Web site helps consumers make sound decisions about using their prescription medications. A companion site, BeMedWise.org, does the same for over-the-counter medications.
http://www.talkaboutrx.org
http://www.bemedwise.org
NCPIE4915 Saint Elmo Ave., Suite 505Bethesda, MD 20814-6082(301) 656-8565
MedlinePlus Drug Information ListingsAn A to Z listing of prescription and OTC medications (both by brand name and generic name), this site within the National Library of Medicine’s Web presence is a comprehensive database of indications, known side effects, storage guidelines, special instructions and much more for every medicine on the market now. If you lose the patient information sheet that comes with medications, you can look up the information here any time you like.
http://www.nlm.nih.gov/medlineplus/druginformation.html
U.S. National Library of Medicine8600 Rockville PikeBethesda, MD 20894Toll free: 1-888-FIND-NLM (346-3656)Local and international calls: (301) 594-5983
Item No: B1-K0186 Trim Size: 8.25" x 10.75"
PLAVIX®clopidogrel bisulfate tabletsRx onlyBrief Summary of Prescribing Information Rev. November 2004 INDICATIONS AND USAGEPLAVIX (clopidogrel bisulfate) is indicated for the reduction of thrombotic events asfollows:
• Recent MI, Recent Stroke or Established Peripheral Arterial DiseaseFor patients with a history of recent myocardial infarction (MI), recent stroke, orestablished peripheral arterial disease, PLAVIX has been shown to reduce therate of a combined endpoint of new ischemic stroke (fatal or not), new MI (fatalor not), and other vascular death.
• Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI)including patients who are to be managed medically and those who are to bemanaged with percutaneous coronary intervention (with or without stent) orCABG, PLAVIX has been shown to decrease the rate of a combined endpoint ofcardiovascular death, MI, or stroke as well as the rate of a combined endpoint ofcardiovascular death, MI, stroke, or refractory ischemia.
CONTRAINDICATIONSThe use of PLAVIX is contraindicated in the following conditions:
• Hypersensitivity to the drug substance or any component of the product.• Active pathological bleeding such as peptic ulcer or intracranial hemorrhage.
WARNINGSThrombotic thrombocytopenic purpura (TTP): TTP has been reported rarely followinguse of PLAVIX, sometimes after a short exposure (<2 weeks). TTP is a serious condition and requires urgent referral to a hematologist for prompt treatment. It ischaracterized by thrombocytopenia, microangiopathic hemolytic anemia (schistocytes[fragmented RBCs] seen on peripheral smear), neurological findings, renal dysfunc-tion, and fever. TTP was not seen during clopidogrel's clinical trials, which includedover 17,500 clopidogrel-treated patients. In world-wide postmarketing experience,however, TTP has been reported at a rate of about four cases per million patientsexposed, or about 11 cases per million patient-years. The background rate is thoughtto be about four cases per million person-years. (See ADVERSE REACTIONS.)PRECAUTIONSGeneralAs with other antiplatelet agents, PLAVIX prolongs the bleeding time and thereforeshould be used with caution in patients who may be at risk of increased bleeding fromtrauma, surgery, or other pathological conditions (particularly gastrointestinal andintraocular). If a patient is to undergo elective surgery and an antiplatelet effect is notdesired, PLAVIX should be discontinued 5 days prior to surgery.
Due to the risk of bleeding and undesirable hematological effects, blood cell countdetermination and/or other appropriate testing should be promptly considered, when-ever such suspected clinical symptoms arise during the course of treatment (seeADVERSE REACTIONS).
GI Bleeding: In CAPRIE, PLAVIX was associated with a rate of gastrointestinal bleed-ing of 2.0%, vs. 2.7% on aspirin. In CURE, the incidence of major gastrointestinalbleeding was 1.3% vs. 0.7% (PLAVIX + aspirin vs. placebo + aspirin, respectively).PLAVIX should be used with caution in patients who have lesions with a propensity tobleed (such as ulcers). Drugs that might induce such lesions should be used with caution in patients taking PLAVIX.
Use in Hepatically Impaired Patients: Experience is limited in patients with severehepatic disease, who may have bleeding diatheses. PLAVIX should be used with caution in this population.
Use in Renally-impaired Patients: Experience is limited in patients with severe renalimpairment. PLAVIX should be used with caution in this population.Information for PatientsPatients should be told that they may bleed more easily and it may take them longer thanusual to stop bleeding when they take PLAVIX or PLAVIX combined with aspirin, and thatthey should report any unusual bleeding to their physician. Patients should inform physi-cians and dentists that they are taking PLAVIX and/or any other product known to affectbleeding before any surgery is scheduled and before any new drug is taken.Drug InteractionsStudy of specific drug interactions yielded the following results:
Aspirin: Aspirin did not modify the clopidogrel-mediated inhibition of ADP-inducedplatelet aggregation. Concomitant administration of 500 mg of aspirin twice a day for 1day did not significantly increase the prolongation of bleeding time induced by PLAVIX.PLAVIX potentiated the effect of aspirin on collagen-induced platelet aggregation. PLAVIX and aspirin have been administered together for up to one year.
Heparin: In a study in healthy volunteers, PLAVIX did not necessitate modificationof the heparin dose or alter the effect of heparin on coagulation. Coadministration ofheparin had no effect on inhibition of platelet aggregation induced by PLAVIX.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): In healthy volunteers receivingnaproxen, concomitant administration of PLAVIX was associated with increased occultgastrointestinal blood loss. NSAIDs and PLAVIX should be coadministered with caution.
Warfarin: Because of the increased risk of bleeding, the concomitant administration ofwarfarin with PLAVIX should be undertaken with caution. (See PRECAUTIONS–General.)
Other Concomitant Therapy: No clinically significant pharmacodynamic interactionswere observed when PLAVIX was coadministered with atenolol, nifedipine, or bothatenolol and nifedipine. The pharmacodynamic activity of PLAVIX was also not signifi-cantly influenced by the coadministration of phenobarbital, cimetidine or estrogen.
The pharmacokinetics of digoxin or theophylline were not modified by the coad-ministration of PLAVIX (clopidogrel bisulfate).
At high concentrations in vitro, clopidogrel inhibits P450 (2C9). Accordingly, PLAVIXmay interfere with the metabolism of phenytoin, tamoxifen, tolbutamide, warfarin,torsemide, fluvastatin, and many non-steroidal anti-inflammatory agents, but thereare no data with which to predict the magnitude of these interactions. Caution should beused when any of these drugs is coadministered with PLAVIX.
In addition to the above specific interaction studies, patients entered into clinical trials with PLAVIX received a variety of concomitant medications including diuretics,beta-blocking agents, angiotensin converting enzyme inhibitors, calcium antago-nists, cholesterol lowering agents, coronary vasodilators, antidiabetic agents(including insulin), antiepileptic agents, hormone replacement therapy, heparins(unfractionated and LMWH) and GPIIb/IIIa antagonists without evidence of clinicallysignificant adverse interactions. The use of oral anticoagulants, non-study anti-plateletdrug and chronic NSAIDs was not allowed in CURE and there are no data on their concomitant use with clopidogrel.Drug/Laboratory Test InteractionsNone known.Carcinogenesis, Mutagenesis, Impairment of FertilityThere was no evidence of tumorigenicity when clopidogrel was administered for 78 weeksto mice and 104 weeks to rats at dosages up to 77 mg/kg per day, which afforded plasma exposures >25 times that in humans at the recommended daily dose of 75 mg.
Clopidogrel was not genotoxic in four in vitro tests (Ames test, DNA-repair test inrat hepatocytes, gene mutation assay in Chinese hamster fibroblasts, and metaphasechromosome analysis of human lymphocytes) and in one in vivo test (micronucleustest by oral route in mice).
Clopidogrel was found to have no effect on fertility of male and female rats at oral doses up to 400 mg/kg per day (52 times the recommended human dose on amg/m2 basis).PregnancyPregnancy Category B. Reproduction studies performed in rats and rabbits at doses upto 500 and 300 mg/kg/day (respectively, 65 and 78 times the recommended dailyhuman dose on a mg/m2 basis), revealed no evidence of impaired fertility or fetotoxic-ity due to clopidogrel. There are, however, no adequate and well-controlled studies inpregnant women. Because animal reproduction studies are not always predictive of ahuman response, PLAVIX should be used during pregnancy only if clearly needed.Nursing MothersStudies in rats have shown that clopidogrel and/or its metabolites are excreted in themilk. It is not known whether this drug is excreted in human milk. Because many drugsare excreted in human milk and because of the potential for serious adverse reactions innursing infants, a decision should be made whether to discontinue nursing or to dis-continue the drug, taking into account the importance of the drug to the nursing woman.Pediatric UseSafety and effectiveness in the pediatric population have not been established.Geriatric UseOf the total number of subjects in controlled clinical studies, approximately 50% ofpatients treated with PLAVIX were 65 years of age and over. Approximately 16% ofpatients treated with PLAVIX were 75 years of age and over. The observed difference in risk of bleeding events with clopidogrel plus aspirin versusplacebo plus aspirin by age category is provided in the following table (see ADVERSEREACTIONS).
ADVERSE REACTIONSPLAVIX has been evaluated for safety in more than 17,500 patients, including over 9,000patients treated for 1 year or more. The overall tolerability of PLAVIX in CAPRIE was sim-ilar to that of aspirin regardless of age, gender and race, with an approximately equal inci-dence (13%) of patients withdrawing from treatment because of adverse reactions. Theclinically important adverse events observed in CAPRIE and CURE are discussed below.
Hemorrhagic: In CAPRIE patients receiving PLAVIX, gastrointestinal hemorrhageoccurred at a rate of 2.0%, and required hospitalization in 0.7%. In patients receivingaspirin, the corresponding rates were 2.7% and 1.1%, respectively. The incidence ofintracranial hemorrhage was 0.4% for PLAVIX compared to 0.5% for aspirin.
In CURE, PLAVIX use with aspirin was associated with an increase in bleeding com-pared to placebo with aspirin (see table below). There was an excess in major bleed-ing in patients receiving PLAVIX plus aspirin compared with placebo plus aspirin, pri-marily gastrointestinal and at puncture sites. The incidence of intracranial hemorrhage(0.1%), and fatal bleeding (0.2%), were the same in both groups.
The overall incidence of bleeding is described in the table below for patients receiv-ing both PLAVIX and aspirin in CURE, CURE Incidence of bleeding complications (% patients)Event PLAVIX Placebo P-value
(+ aspirin)* (+ aspirin)*(n=6259) (n=6303)
Major bleeding † 3.7 ‡ 2.7 § 0.001Life-threatening bleeding 2.2 1.8 0.13
Fatal 0.2 0.25 g/dL hemoglobin drop 0.9 0.9Requiring surgical intervention 0.7 0.7Hemorrhagic strokes 0.1 0.1Requiring inotropes 0.5 0.5Requiring transfusion (�4 units) 1.2 1.0
Other major bleeding 1.6 1.0 0.005Significantly disabling 0.4 0.3Intraocular bleeding with
significant loss of vision 0.05 0.03Requiring 2-3 units of blood 1.3 0.9
Minor bleeding ¶ 5.1 2.4 <0.001* Other standard therapies were used as appropriate.† Life threatening and other major bleeding.‡ Major bleeding event rate for PLAVIX + aspirin was dose-dependent on aspirin:
<100 mg=2.6%; 100-200 mg= 3.5%; >200 mg=4.9%Major bleeding event rates for PLAVIX + aspirin by age were: <65 years = 2.5%, �65 to <75 years = 4.1%, �75 years 5.9%
§ Major bleeding event rate for placebo + aspirin was dose-dependent on aspirin: <100 mg=2.0%; 100-200 mg= 2.3%; >200 mg=4.0%Major bleeding event rates for placebo + aspirin by age were: <65 years = 2.1%, �65 to <75 years = 3.1%, �75 years 3.6%
¶ Led to interruption of study medication.
Ninety-two percent (92%) of the patients in the CURE study received heparin/LMWH, and the rate of bleeding in these patients was similar to the overall results.
There was no excess in major bleeds within seven days after coronary bypass graftsurgery in patients who stopped therapy more than five days prior to surgery (eventrate 4.4% PLAVIX + aspirin; 5.3% placebo + aspirin). In patients who remained on ther-apy within five days of bypass graft surgery, the event rate was 9.6% for PLAVIX +aspirin, and 6.3% for placebo + aspirin.
Neutropenia/agranulocytosis: Ticlopidine, a drug chemically similar to PLAVIX, isassociated with a 0.8% rate of severe neutropenia (less than 450 neutrophils/µL). InCAPRIE severe neutropenia was observed in six patients, four on PLAVIX and two onaspirin. Two of the 9599 patients who received PLAVIX and none of the 9586 patientswho received aspirin had neutrophil counts of zero. One of the four PLAVIX patients inCAPRIE was receiving cytotoxic chemotherapy, and another recovered and returned tothe trial after only temporarily interrupting treatment with PLAVIX (clopidogrel bisul-fate). In CURE, the numbers of patients with thrombocytopenia (19 PLAVIX + aspirinvs. 24 placebo + aspirin) or neutropenia (3 vs. 3) were similar.
Although the risk of myelotoxicity with PLAVIX (clopidogrel bisulfate) thus appearsto be quite low, this possibility should be considered when a patient receiving PLAVIXdemonstrates fever or other sign of infection.
Gastrointestinal: Overall, the incidence of gastrointestinal events (e.g. abdominalpain, dyspepsia, gastritis and constipation) in patients receiving PLAVIX (clopidogrelbisulfate) was 27.1%, compared to 29.8% in those receiving aspirin in the CAPRIE trial.In the CURE trial the incidence of these gastrointestinal events for patients receivingPLAVIX + aspirin was 11.7% compared to 12.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the incidence of peptic, gastric or duodenal ulcers was 0.7% forPLAVIX and 1.2% for aspirin. In the CURE trial the incidence of peptic, gastric or duo-denal ulcers was 0.4% for PLAVIX + aspirin and 0.3% for placebo + aspirin.
Cases of diarrhea were reported in the CAPRIE trial in 4.5% of patients in the PLAVIX group compared to 3.4% in the aspirin group. However, these were rarelysevere (PLAVIX=0.2% and aspirin=0.1%). In the CURE trial, the incidence of diarrheafor patients receiving PLAVIX + aspirin was 2.1% compared to 2.2% for those receiv-ing placebo + aspirin.
In the CAPRIE trial, the incidence of patients withdrawing from treatment becauseof gastrointestinal adverse reactions was 3.2% for PLAVIX (clopidogrel bisulfate) and4.0% for aspirin. In the CURE trial, the incidence of patients withdrawing from treatment because of gastrointestinal adverse reactions was 0.9% for PLAVIX + aspirincompared with 0.8% for placebo + aspirin.
Rash and Other Skin Disorders: In the CAPRIE trial, the incidence of skin andappendage disorders in patients receiving PLAVIX was 15.8% (0.7% serious); the cor-responding rate in aspirin patients was 13.1% (0.5% serious). In the CURE trial theincidence of rash or other skin disorders in patients receiving PLAVIX + aspirin was4.0% compared to 3.5% for those receiving placebo + aspirin.
In the CAPRIE trial, the overall incidence of patients withdrawing from treatmentbecause of skin and appendage disorders adverse reactions was 1.5% for PLAVIX and 0.8% for aspirin. In the CURE trial, the incidence of patients withdrawing becauseof skin and appendage disorders adverse reactions was 0.7% for PLAVIX + aspirin compared with 0.3% for placebo + aspirin.
Adverse events occurring in �2.5% of patients on PLAVIX in the CAPRIE controlledclinical trial are shown below regardless of relationship to PLAVIX. The median dura-tion of therapy was 20 months, with a maximum of 3 years.Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE
% Incidence (% Discontinuation)Body System PLAVIX AspirinEvent [n=9599] [n=9586]Body as a Whole- general disorders
Chest Pain 8.3 (0.2) 8.3 (0.3)Accidental/Inflicted Injury 7.9 (0.1) 7.3 (0.1)Influenza-like symptoms 7.5 (<0.1) 7.0 (<0.1)Pain 6.4 (0.1) 6.3 (0.1)Fatigue 3.3 (0.1) 3.4 (0.1)
Cardiovascular disorders, generalEdema 4.1 (<0.1) 4.5 (<0.1)Hypertension 4.3 (<0.1) 5.1 (<0.1)
Central & peripheral nervous system disorders
Headache 7.6 (0.3) 7.2 (0.2)Dizziness 6.2 (0.2) 6.7 (0.3)
Gastrointestinal system disordersAbdominal pain 5.6 (0.7) 7.1 (1.0)Dyspepsia 5.2 (0.6) 6.1 (0.7)Diarrhea 4.5 (0.4) 3.4 (0.3)Nausea 3.4 (0.5) 3.8 (0.4)
Metabolic & nutritional disordersHypercholesterolemia 4.0 (0) 4.4 (<0.1)
Musculo-skeletal system disordersArthralgia 6.3 (0.1) 6.2 (0.1)Back Pain 5.8 (0.1) 5.3 (<0.1)
Platelet, bleeding, & clotting disordersPurpura/Bruise 5.3 (0.3) 3.7 (0.1)Epistaxis 2.9 (0.2) 2.5 (0.1)
Psychiatric disordersDepression 3.6 (0.1) 3.9 (0.2)
Respiratory system disordersUpper resp tract infection 8.7 (<0.1) 8.3 (<0.1)Dyspnea 4.5 (0.1) 4.7 (0.1)Rhinitis 4.2 (0.1) 4.2 (<0.1)Bronchitis 3.7 (0.1) 3.7 (0)Coughing 3.1 (<0.1) 2.7(<0.1)
Adverse Events Occurring in �2.5% of PLAVIX Patients in CAPRIE (continued)% Incidence (% Discontinuation)
Body System PLAVIX AspirinEvent [n=9599] [n=9586]Skin & appendage disorders
Rash 4.2 (0.5) 3.5 (0.2)Pruritus 3.3 (0.3) 1.6 (0.1)
Urinary system disordersUrinary tract infection 3.1 (0) 3.5 (0.1)
Incidence of discontinuation, regardless of relationship to therapy, is shown in parentheses.
Adverse events occurring in �2.0% of patients on PLAVIX in the CURE controlledclinical trial are shown below regardless of relationship to PLAVIX.Adverse Events Occurring in �2.0% of PLAVIX Patients in CURE
% Incidence (% Discontinuation)Body System PLAVIX Placebo
(+ aspirin)* (+ aspirin)*Event [n=6259] [n=6303]Body as a Whole- general disorders
Chest Pain 2.7 (<0.1) 2.8 (0.0)Central & peripheral nervous system disorders
Headache 3.1 (0.1) 3.2 (0.1)Dizziness 2.4 (0.1) 2.0 (<0.1)
Gastrointestinal system disordersAbdominal pain 2.3 (0.3) 2.8 (0.3)Dyspepsia 2.0 (0.1) 1.9 (<0.1)Diarrhea 2.1 (0.1) 2.2 (0.1)
*Other standard therapies were used as appropriate.
Other adverse experiences of potential importance occurring in 1% to 2.5% ofpatients receiving PLAVIX (clopidogrel bisulfate) in the CAPRIE or CURE controlledclinical trials are listed below regardless of relationship to PLAVIX. In general, the inci-dence of these events was similar to that in patients receiving aspirin (in CAPRIE) orplacebo + aspirin (in CURE).
Autonomic Nervous System Disorders: Syncope, Palpitation. Body as a Whole-general disorders: Asthenia, Fever, Hernia. Cardiovascular disorders: Cardiac failure.Central and peripheral nervous system disorders: Cramps legs, Hypoaesthesia,Neuralgia, Paraesthesia, Vertigo. Gastrointestinal system disorders: Constipation,Vomiting. Heart rate and rhythm disorders: Fibrillation atrial. Liver and biliary systemdisorders: Hepatic enzymes increased. Metabolic and nutritional disorders: Gout,hyperuricemia, non-protein nitrogen (NPN) increased. Musculo-skeletal system disor-ders: Arthritis, Arthrosis. Platelet, bleeding & clotting disorders: GI hemorrhage,hematoma, platelets decreased. Psychiatric disorders: Anxiety, Insomnia. Red bloodcell disorders: Anemia. Respiratory system disorders: Pneumonia, Sinusitis. Skin andappendage disorders: Eczema, Skin ulceration. Urinary system disorders: Cystitis.Vision disorders: Cataract, Conjunctivitis.
Other potentially serious adverse events which may be of clinical interest but wererarely reported (<1%) in patients who received PLAVIX in the CAPRIE or CURE con-trolled clinical trials are listed below regardless of relationship to PLAVIX. In general,the incidence of these events was similar to that in patients receiving aspirin (inCAPRIE) or placebo + aspirin (in CURE).
Body as a whole: Allergic reaction, necrosis ischemic. Cardiovascular disorders:Edema generalized. Gastrointestinal system disorders: Gastric ulcer perforated, gastri-tis hemorrhagic, upper GI ulcer hemorrhagic. Liver and Biliary system disorders:Bilirubinemia, hepatitis infectious, liver fatty. Platelet, bleeding and clotting disorders:hemarthrosis, hematuria, hemoptysis, hemorrhage intracranial, hemorrhage retroperi-toneal, hemorrhage of operative wound, ocular hemorrhage, pulmonary hemorrhage,purpura allergic, thrombocytopenia. Red blood cell disorders: Anemia aplastic, anemiahypochromic. Reproductive disorders, female: Menorrhagia. Respiratory system disorders: Hemothorax. Skin and appendage disorders: Bullous eruption, rash erythe-matous, rash maculopapular, urticaria. Urinary system disorders: Abnormal renal function, acute renal failure. White cell and reticuloendothelial system disorders:Agranulocytosis, granulocytopenia, leukemia, leukopenia, neutrophils decreased.Postmarketing ExperienceThe following events have been reported spontaneously from worldwide postmarket-ing experience:
• Body as a whole:- hypersensitivity reactions, anaphylactoid reactions
• Central and Peripheral Nervous System disorders:- confusion, hallucinations, taste disorders
• Hepato-biliary disorders:- abnormal liver function test, hepatitis (non-infectious)
• Platelet, Bleeding and Clotting disorders:- cases of bleeding with fatal outcome (especially intracranial, gastrointestinal
and retroperitoneal hemorrhage)- agranulocytosis, aplastic anemia/pancytopenia, thrombotic thrombocytopenic
purpura (TTP) - some cases with fatal outcome – (see WARNINGS).- conjunctival, ocular and retinal bleeding
• Respiratory, thoracic and mediastinal disorders:- bronchospasm
• Skin and subcutaneous tissue disorders:- angioedema, erythema multiforme, Stevens-Johnson syndrome, lichen planus
• Renal and urinary disorders:- glomerulopathy, increased creatinine levels
• Vascular disorders:- vasculitis, hypotension
• Gastrointestinal disorders:- colitis (including ulcerative or lymphocytic colitis), pancreatitis
• Musculoskeletal, connective tissue and bone disorders:- myalgia
OVERDOSAGEOverdose following clopidogrel administration may lead to prolonged bleeding timeand subsequent bleeding complications. Appropriate therapy should be considered ifbleeding is observed. A single oral dose of clopidogrel at 1500 or 2000 mg/kg waslethal to mice and to rats and at 3000 mg/kg to baboons. Symptoms of acute toxicitywere vomiting (in baboons), prostration, difficult breathing, and gastrointestinal hem-orrhage in all species.Recommendations About Specific Treatment:Based on biological plausibility, platelet transfusion may be appropriate to reverse thepharmacological effects of PLAVIX if quick reversal is required.DOSAGE AND ADMINISTRATIONRecent MI, Recent Stroke, or Established Peripheral Arterial DiseaseThe recommended daily dose of PLAVIX is 75 mg once daily.Acute Coronary SyndromeFor patients with acute coronary syndrome (unstable angina/non-Q-wave MI), PLAVIXshould be initiated with a single 300 mg loading dose and then continued at 75 mgonce daily. Aspirin (75 mg-325 mg once daily) should be initiated and continued incombination with PLAVIX. In CURE, most patients with Acute Coronary Syndrome alsoreceived heparin acutely (see CLINICAL STUDIES).
PLAVIX can be administered with or without food.No dosage adjustment is necessary for elderly patients or patients with renal dis-
ease. (See Clinical Pharmacology: Special Populations.)Distributed by:Bristol-Myers Squibb/Sanofi Pharmaceuticals PartnershipNew York, NY 10016
PLAVIX® is a registered trademark of Sanofi-Synthelabo.
Brief Summary of Prescribing Information Rev. November 2004
B1-K0186_IBC 5/19/05 4:05 PM Page 1
© 2005 Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership.
PLAVIX HELPS KEEP BLOOD PLATELETSFROM STICKING TOGETHER AND FORMINGCLOTS, WHICH HELPS PROTECT YOU FROMANOTHER HEART ATTACK OR STROKE.If you’ve had a heart attack or stroke, the last thing youneed is another one sneaking up on you. PLAVIX mayhelp. PLAVIX is a prescription medication for peoplewho have had a recent heart attack or recent stroke, orwho have poor circulation in the legs, causing pain.
PLAVIX OFFERS PROTECTION.PLAVIX is proven to help keep blood platelets fromsticking together and forming clots, which helps keepyour blood flowing. This can help protect you fromanother heart attack or stroke.
IMPORTANT INFORMATION: If you have a stomachulcer or other condition that causes bleeding, youshouldn't use Plavix. When taking Plavix alone or withsome medicines including aspirin, the risk of bleedingmay increase.To minimize this risk, talk to your doctorbefore taking aspirin or other medicines with Plavix.Additional rare but serious side effects could occur.
WITHOUT PLAVIX WITH PLAVIX
PROVEN TO HELP PROTECT FROM ANOTHER HEART ATTACK OR STROKE
Item No: B1-K0186 Trim Size: 7.75" x 10.75" (back cover) Publication: Stroke Connection
USA.CLO.05.04.76/May 2005 B1-K0186/05-05Sanofi-Synthelabo Inc., a member of the sanofi-aventis Group
TALK TO YOUR DOCTOR ABOUT PLAVIX.
For more information, visit www.plavix.com or call1-877-700-0701.
YOU DON’T WANT ANOTHERHEART ATTACK OR ANOTHERSTROKE TO SNEAK UP ON YOU.
YOU DON’T WANT ANOTHERHEART ATTACK OR ANOTHERSTROKE TO SNEAK UP ON YOU.
Please see important product information on the inside page.
B1-K0186_cvr 5/19/05 4:15 PM Page 1
NON-PROFIT ORG.
U.S. POSTAGE PAID
PERMIT NO. 4
LONG PRAIRIE, MN
National Center7272 Greenville AvenueDallas, TX 75231-4596





![Jesus heals[1]](https://static.documents.pub/doc/80x56/55a660951a28ab56538b468c/jesus-heals1.jpg)

