
Pimples and Boils!!
Dr Nathan HarveyAnatomical Pathology, PathWest

Overview & Learning Objectives
• Review the cardinal signs/symptoms of acute inflammation
• Review the histological features of acute inflammation• Overview of the possible outcomes of acute inflammation• Understand the clinical signs/symptoms, pathological
mechanisms and histological features of common acute inflammatory disorders of the skin:– Impetigo– Acne vulgaris– Folliculitis– Furuncle– Erysipelas/cellulitis


Neutrophils
What is Pus?
• A protein-rich fluid produced as a product of inflammation
• It comprises:– Leukocytes (white blood cells)– Debris from dead cells– Tissue elements which have been liquified
by the action of neutrophil enzymes
• Bacteria that cause pus formation are called suppurative, pyogenic or purulent

www.siumed.edu

Microscopic Structure of the Skin
Stratum Corneum
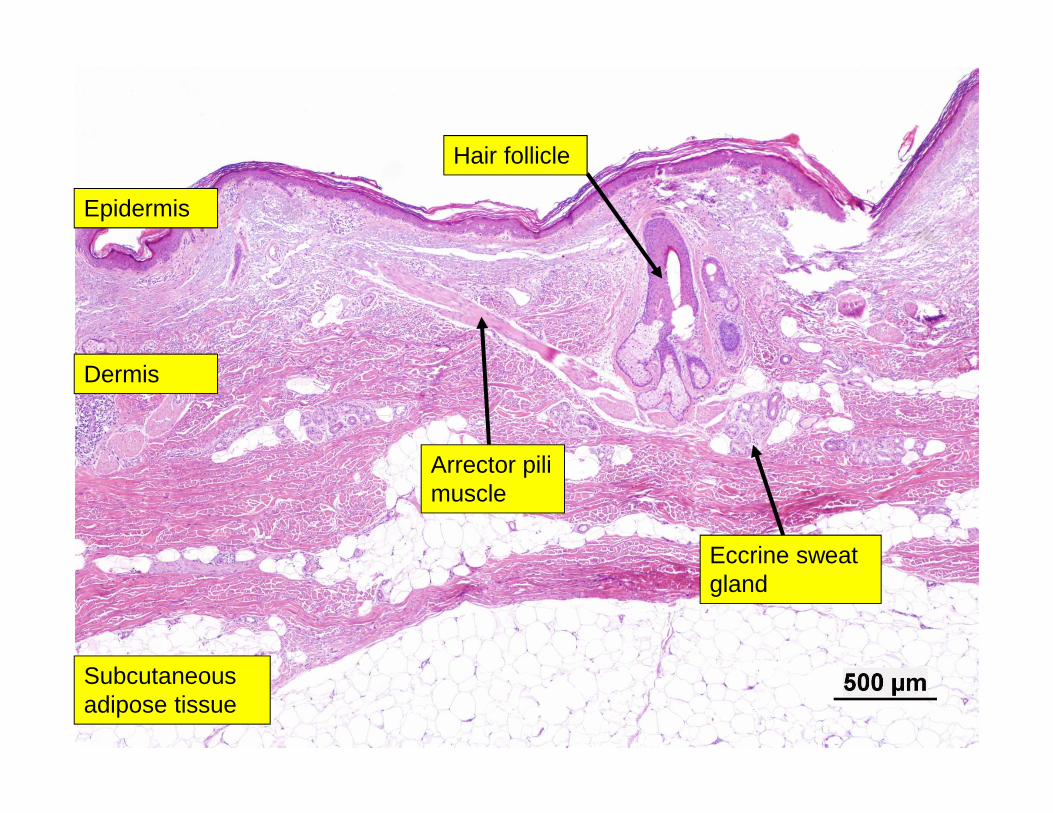
Epidermis
Dermis
Subcutaneous adipose tissue
Hair follicle
Arrector pili muscle
Eccrine sweat gland
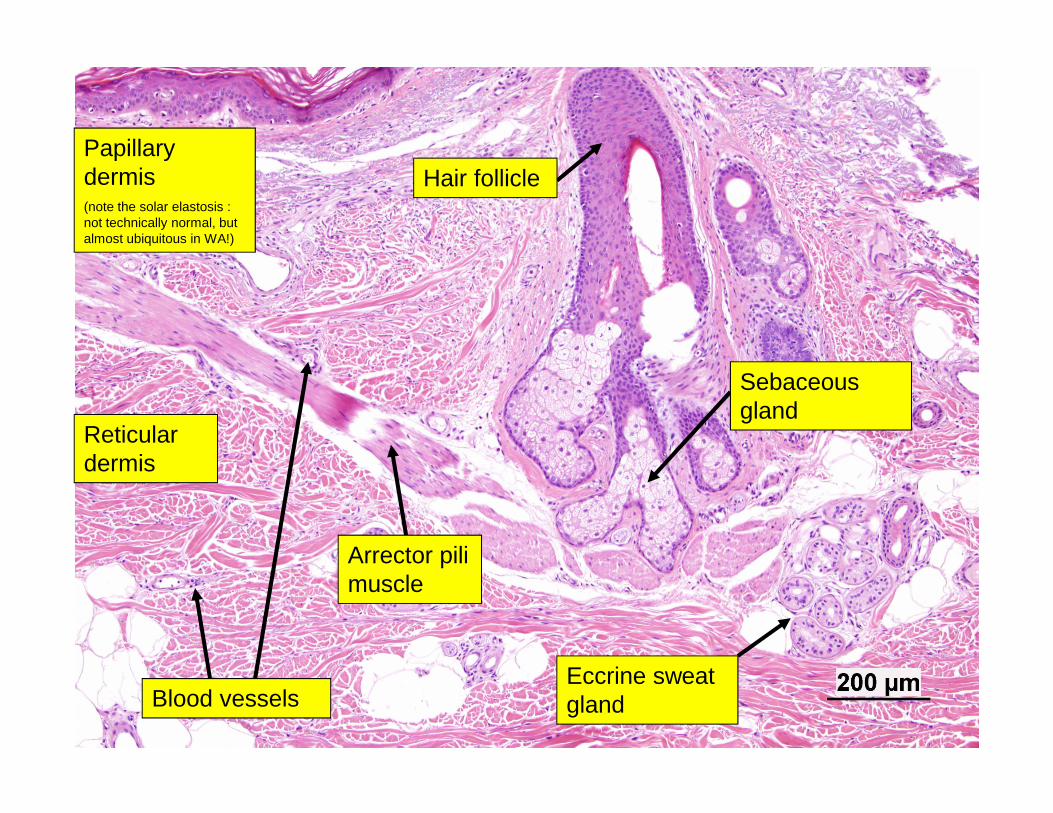
Papillary dermis(note the solar elastosis : not technically normal, but almost ubiquitous in WA!)
Reticular dermis
Hair follicle
Arrector pili muscle
Eccrine sweat gland
Sebaceous gland
Blood vessels
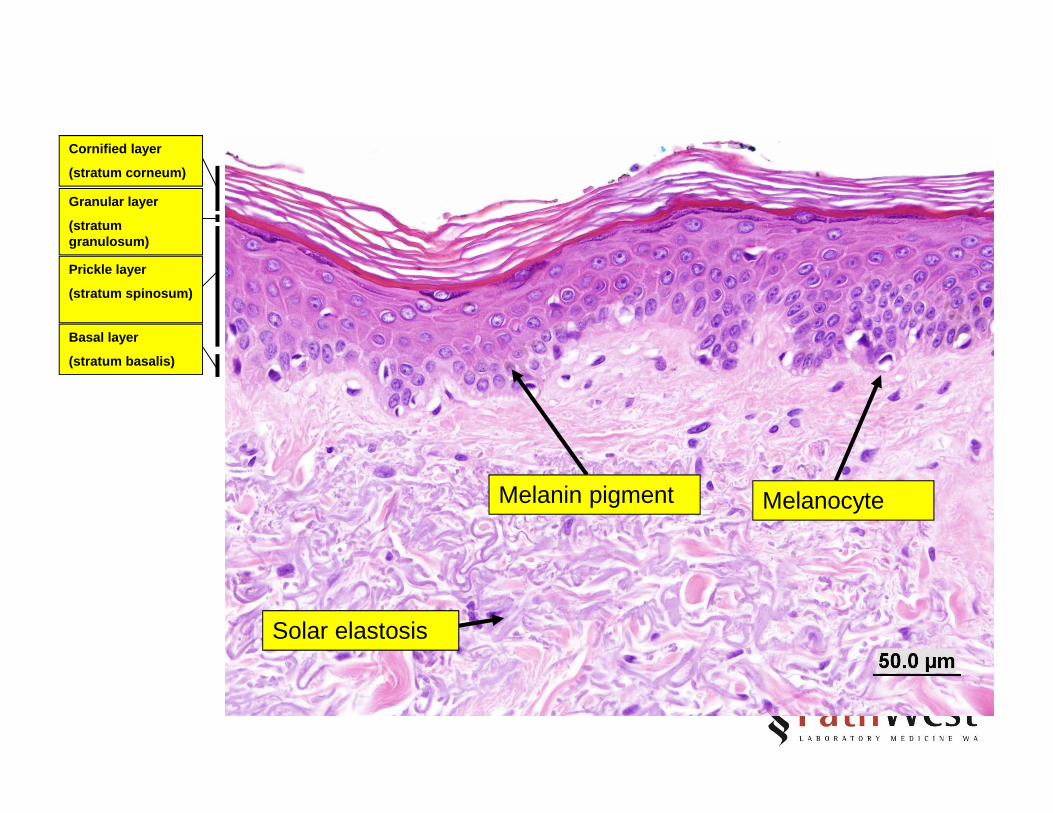
Cornified layer
(stratum corneum)
Solar elastosis
Melanin pigment Melanocyte
Granular layer
(stratum granulosum)
Prickle layer
(stratum spinosum)
Basal layer
(stratum basalis)

Cutaneous Bacterial Infections
• Pyogenic infections– Staphylococcus aureus– Streptococcus
• Corynebacteria• Neisseria• Mycobacteria• Chlamydia• Rickettsia
Impetigo
• Acute superficial infection of the skin• Most common bacterial skin infection of
childhood• Adults can also be affected
– Athletes– Military– Institutions
• Predisposing factors– Minor trauma– Poor hygiene– Warm, humid climate

Impetigo
• Organism is often Staphylococcus aureus (esp in bullous subtype)
• Also Streptococcus, anaerobes• Staphylococcus aureus may produce
exfoliative toxins

Impetigo• Common Impetigo
– “School sores”– Thin walled vesicles or pustules– Rupture to form a thick golden crust– Solitary or clustered, face or extremities
• Bullous Impetigo– Erosions and flaccid bullae– Caused by an exotoxin which results in
keratinocytes falling apart and blister formation

Histopathology
• Subcorneal (ie under the stratum corneum) collection of neutrophils
• Can see more neutrophils migrating upwards through the epidermis
• Surface crust of serum and dying neutrophils
• May see bacterial colonies
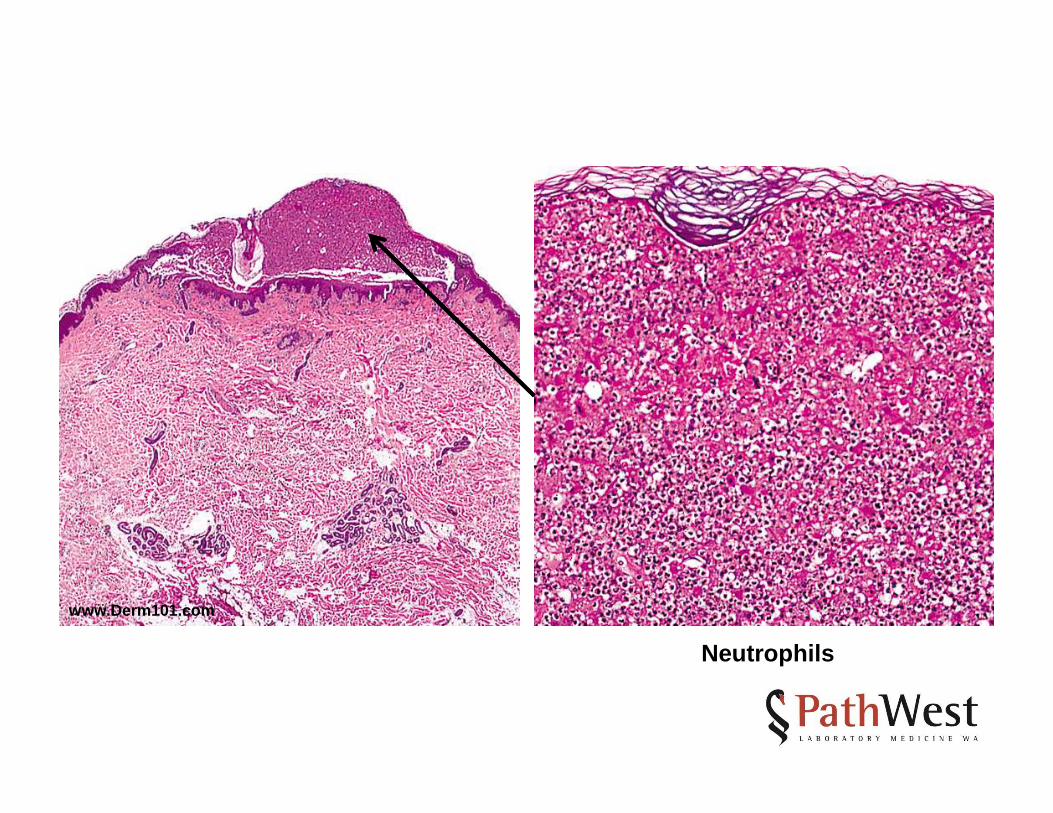
Neutrophils
www.Derm101.com

Staphylococcal Scalded Skin Syndrome
• Another blistering disorder caused by Staphylococcus aureus, but with a different mechanism
• Occurs in infants• Widespread blisters that rupture easily• No bacteria in the blisters• Caused by an endotoxin that is made by
the bacteria elsewhere and is transported via the bloodstream
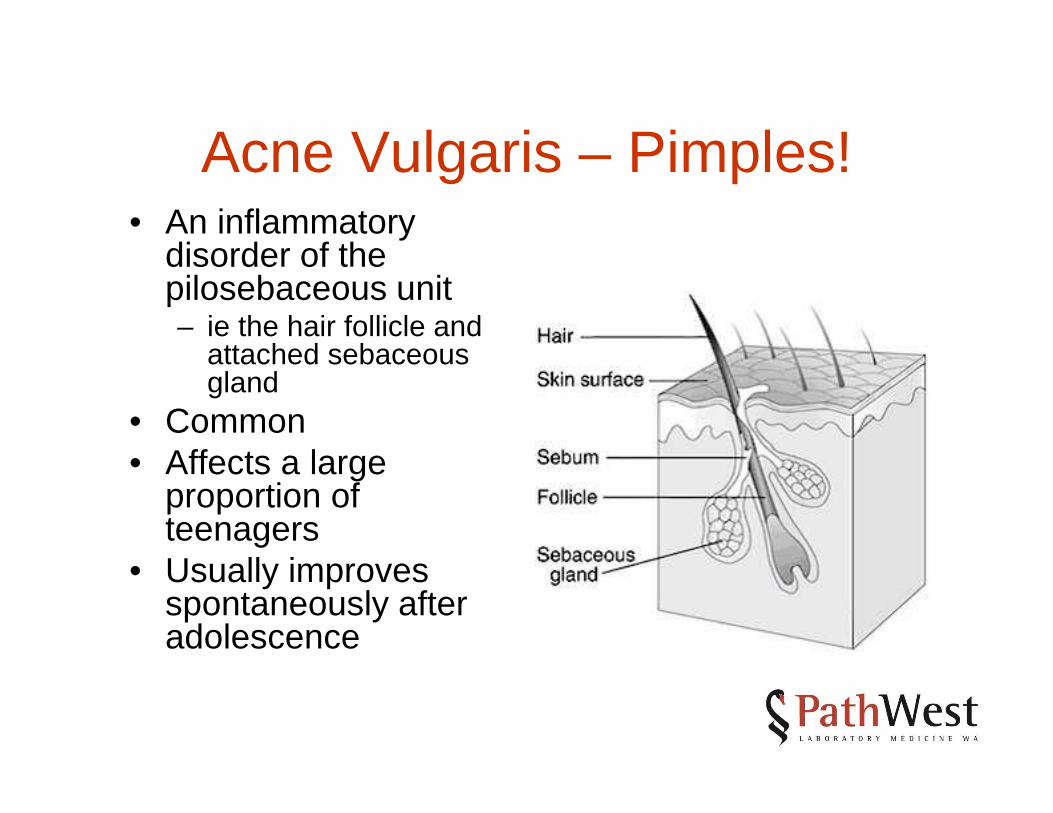
Acne Vulgaris – Pimples!• An inflammatory
disorder of the pilosebaceous unit– ie the hair follicle and
attached sebaceous gland
• Common• Affects a large
proportion of teenagers
• Usually improves spontaneously after adolescence
Clinical Appearances• The lesions that make up acne are
variable and include:– Comedones– Papules– Pustules– Cysts– Sinuses– Scars
Clinical Appearances
• Comedones are widened hair follicles which are filled with keratin, other debris, bacteria and sebum– Closed : “whiteheads”– Open: “blackheads”

www.Derm101.com www.Derm101.com

Open comedones
Inflamed papule
Scars
www.Derm101.com

Pathogenesis• Four inter-related factors
– Abnormal follicular keratinisation, with retention of keratin within the follicle
• This process is the precursor to comedoneformation
• May be aided by a bacterial ‘biofilm’
– Increased sebum production• Androgens
– Presence of bacteria: Propionibacteriumacnes
– Inflammation
Pathogenesis• Ongoing dilation of comedo leads to the wall of the
follicle becoming very thin• Eventually it ruptures• The keratin, sebum and bacteria incite an acute
inflammatory response• Predominantly neutrophils at first – pustule
formation• Followed by granulomatous inflammation and
fibrosis (scarring)• The acute inflammatory focus can enlarge into an
abscess. Sinus tracts result when the epidermis grows down in an attempt to ‘wall off’ the inflammation

Plugged and dilated follicle
Neutrophils
Superficial Folliculitis• Typically affects the superficial part of the hair
follicle, called the ‘infundibulum’– Thus, perhaps more correctly should be called
‘infundibulitis’• May be related to bacterial infection (eg
Staphylococcus aureus)• Neutrophils under the statum corneum and
around the infundibulum• ‘pseudofolliculitis’ is a term used to describe a
foreign body response to hair shafts that have ruptured out of the follicle into the surrounding dermis

Small pustules around hair follicles
www.Derm101.com

Neutrophils
www.Derm101.com

Furuncle – “Boils”• A deeper infectious inflammatory process
centred on the pilosebaceous unit• Typical locations include the back of the neck,
buttocks and thighs– Sites of friction with clothing
• Begins as a painful papule with surrounding erythema (redness) and swelling
• The centre becomes soft, yellow and may discharge pus
• A ‘carbuncle’ is a coalescence of several furuncles

Histological features
• A deep dermal abscess (ie neutrophilsagain!) centred around a hair follicle
• The follicle may be destroyed although residual hair shafts may be seen
• The surrounding inflammation may extend into the deeper tissues
• The surface oftens shows a ‘crust’ of serum and dying neutrophils

www.Derm101.com

Acute inflammation (ieneutrophils) in the deeper parts of the follicle
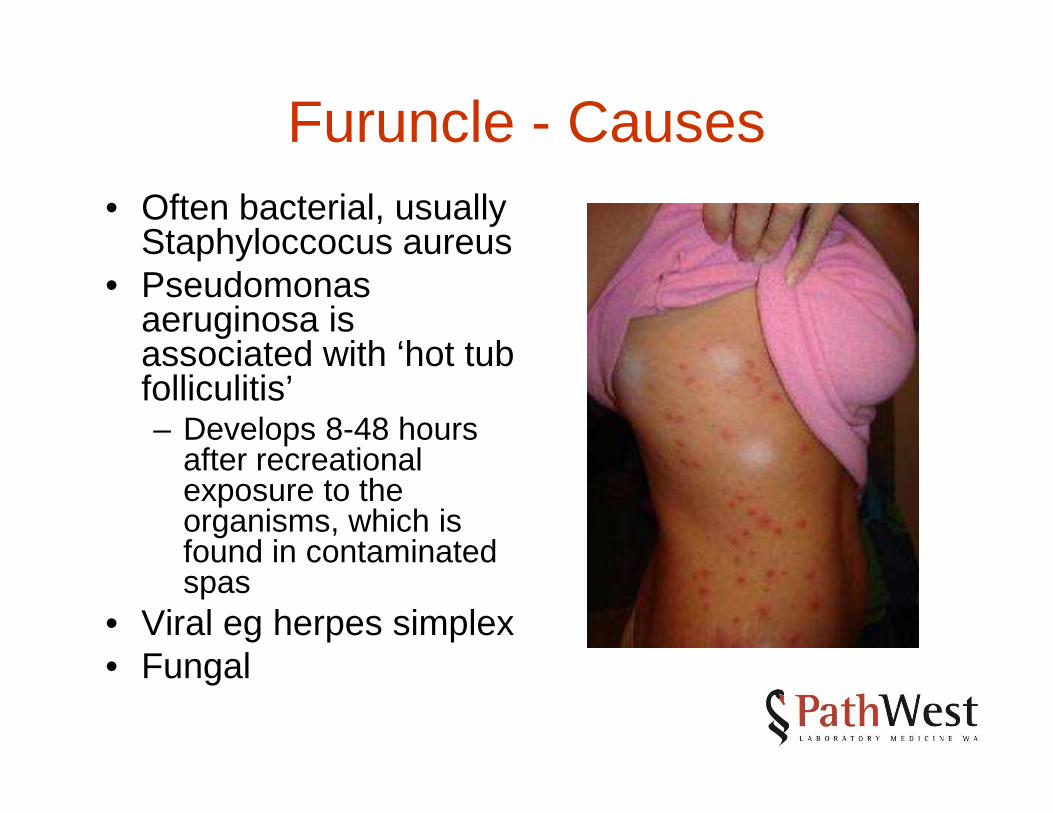
Furuncle - Causes• Often bacterial, usually
Staphyloccocus aureus• Pseudomonas
aeruginosa is associated with ‘hot tub folliculitis’– Develops 8-48 hours
after recreational exposure to the organisms, which is found in contaminated spas
• Viral eg herpes simplex• Fungal

Erysipelas/Cellulitis• Erysipelas is an acute inflammatory
process within the dermis which is usually caused by Streptococcus pyogenes
• Oedematous, tender, hot, well demarcated red plaques
• Often accompanied by a fever• Face, feet, hands and lower limbs are
most affected

Erysipelas/Cellulitis
• Cellulitis is a similar processs which involves slightly deeper tissues
• More often occurs on the legs• Expanding area of erythema• S pyogenes is again usually the
causative organism
Predisposing Factors
• Minor trauma• Peripheral vascular disease• Diabetes• Lymphoedema• Alcohol abuse
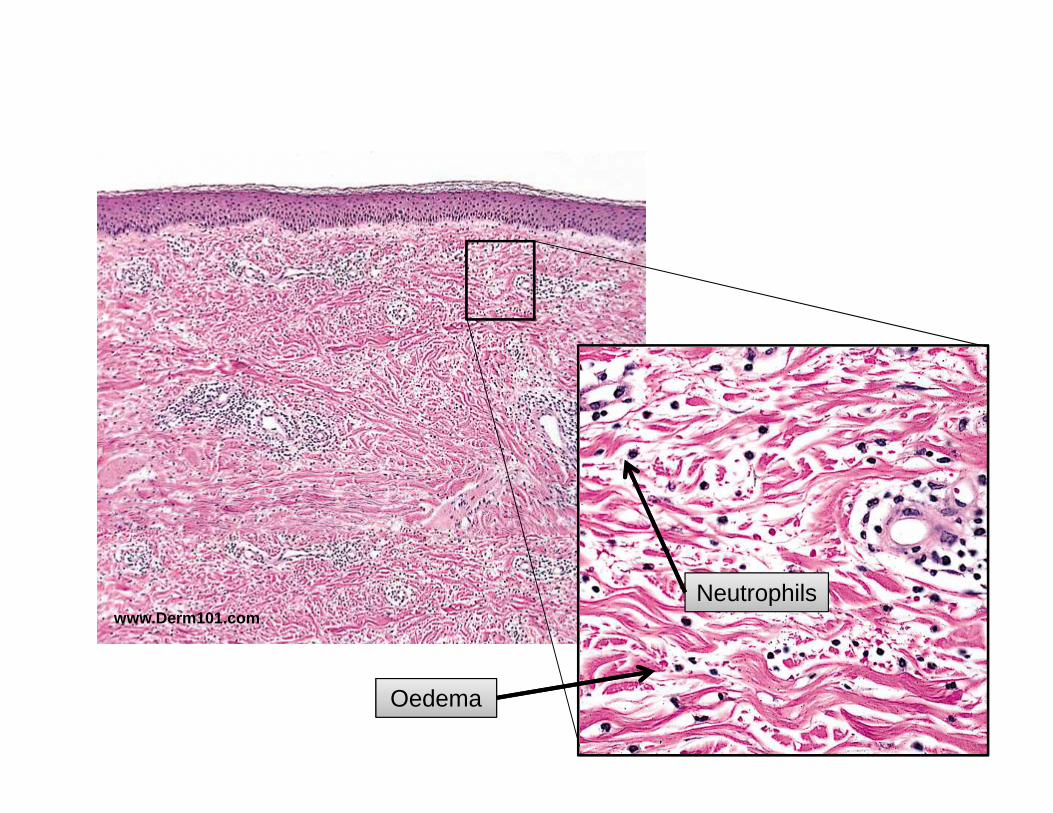
Histology
• Dermal oedema and lymphatic dilatation• Diffuse infiltrate of neutrophils

Erysipelas
www.Derm101.com
www.Derm101.com
www.Derm101.com
Oedema
Neutrophils

Summary
• Remember: – the cardinal signs & symptoms of acute inflammation– The histological features– The possible sequelae
• By applying the above to different anatomical components of the skin:– Impetigo– Acne vulgaris– Folliculitis– Furuncle– Erysipelas/cellulitis







