

Reflections on our vanguard programme
Paul Gray Programme Director, North East Hampshire and Farnham PACS Vanguard Director, Consilium Partners Ltd
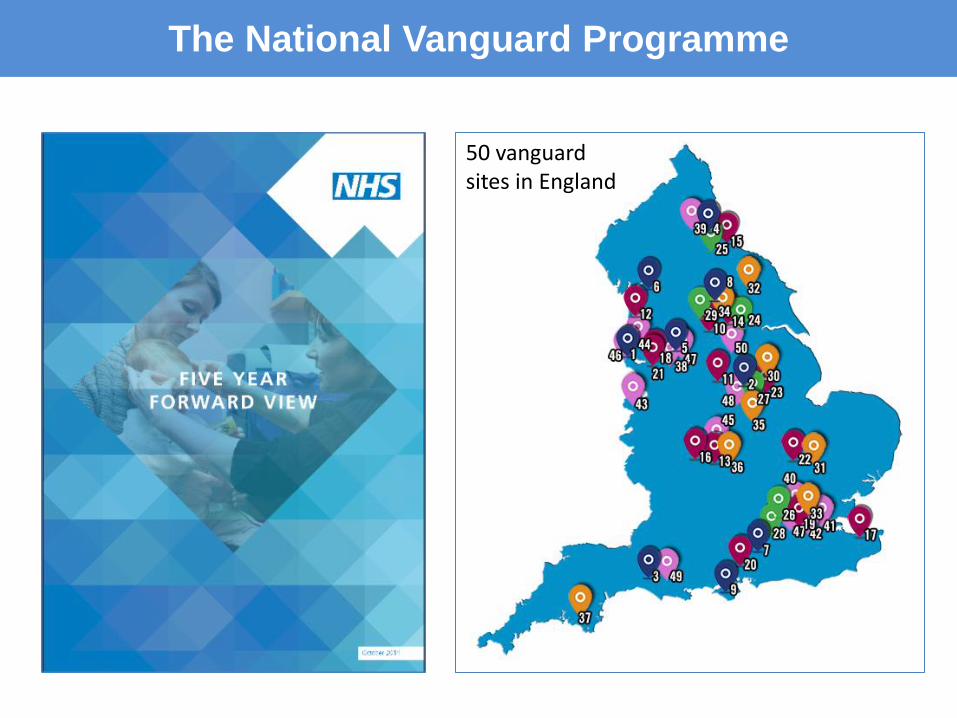
The National Vanguard Programme
50 vanguard sites in England

Just another system redesign programme?
Ingredients for success?
Culture that allows failure
Rigour through logic models
Focus on evaluation and
replication
Money and support
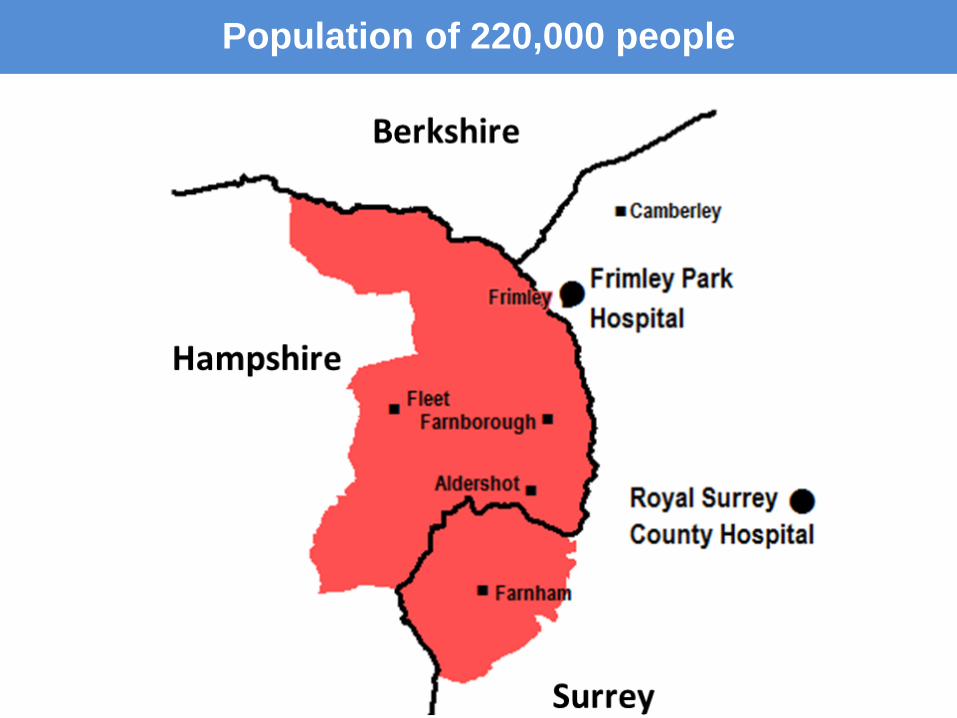
Population of 220,000 people
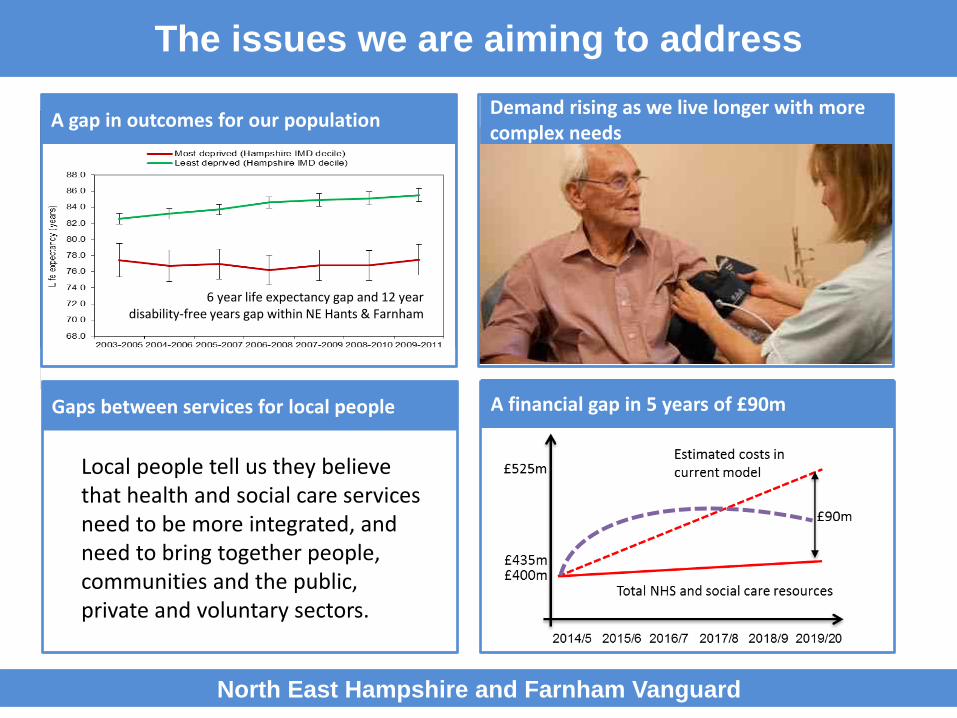
The issues we are aiming to address
North East Hampshire and Farnham Vanguard
A gap in outcomes for our population Demand rising as we live longer with more complex needs
A financial gap in 5 years of £90m
6 year life expectancy gap and 12 year disability-free years gap within NE Hants & Farnham
Gaps between services for local people
Local people tell us they believe that health and social care services need to be more integrated, and need to bring together people, communities and the public, private and voluntary sectors.

A shared vision to improve health and wellbeing
North East Hampshire and Farnham Vanguard
OU
R V
ISIO
N
Our vision is that local people are supported to improve their own health and wellbeing, and that when people are ill or need help, they receive the best possible joined up care

Secondary Care Highlights Our programme
North East Hampshire and Farnham Vanguard
A new model
of care
A new commissioning
model
Designed by care professionals and local
people
Commissioners pooling budgets and aligning
incentives
A new provider model
Providers collaborating to manage population
health
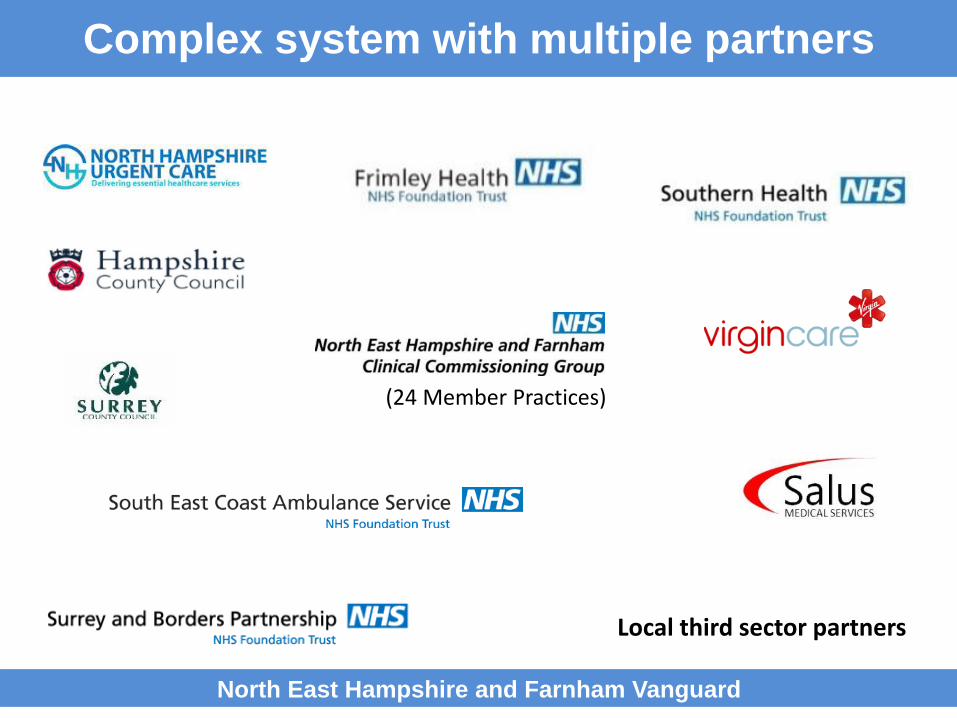
Complex system with multiple partners
North East Hampshire and Farnham Vanguard
Local third sector partners
(24 Member Practices)

New model of care outcomes
North East Hampshire and Farnham Vanguard
Theme Impact of the new model of care
Happy. Improved wellbeing, and better experience of care for
local people
Healthy. Better health and social care outcomes, and improved
quality of life
At Home. More care delivered at home and in the community,
local people spending less time in hospital
Better Value
for Money
Lower costs per head of population, enabling the system
to better meet future demand within the available
resources
The new care model is designed to address the challenges we face
Logic Models
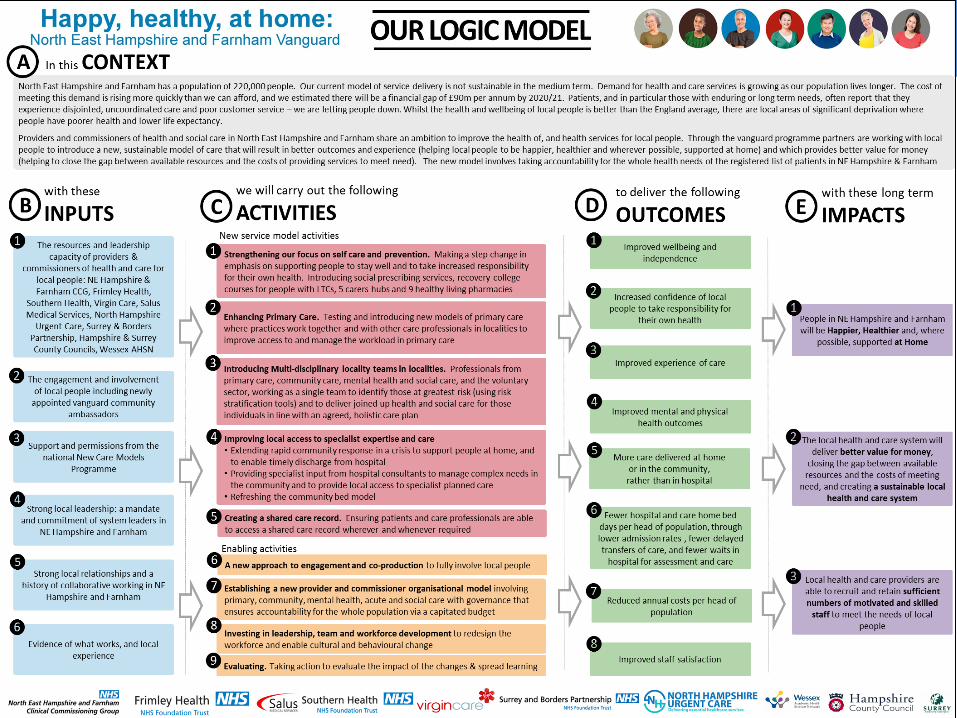
We have invested in logic model development to provide a robust basis for our testing of new approaches
Wessex AHSN who have considerable expertise in this area are leading this work
Each proposal we consider is underpinned by a logic model: “If we do XXX then we expect YYY to happen which will give us ZZZ benefits”
Logic Models

Logic Models

Engagement with local people
Our thinking has been developed with local people over the last 2-3 years – now accelerated by Vanguard
Large scale events with 100+ local people
Community Ambassadors Collaborative pairs and trios
with the Kings Fund A toolkit to support local
engagement

A new care model, designed with local people
North East Hampshire and Farnham Vanguard
OU
R N
EW C
AR
E M
OD
EL 1. Preventing ill health, and supporting people
to take increased responsibility for their own health
2. Improving access to joined up primary and community care, supporting people to stay well at home
3. Ensuring people receive timely and appropriate complex planned and emergency acute care, supporting people in crisis
Prevention and self care
North East Hampshire and Farnham Vanguard
Action to prevent ill health and to promote healthy choices; education and support for self-care; and action to promote mental wellbeing
In addition to our existing prevention activity we have invested in a system wide initiative which will deliver:
Social prescribing services available by the end of March 2016 A first healthy living pharmacy open by the beginning of 2016,
with 9 operating by 31 July Recovery college courses available for people with Long Term
Conditions from March 2016 A carers forum established by January 2016, and carers hubs
open in all 5 localities by March 2016

Crisis Café
North East Hampshire and Farnham Vanguard
Integrated out of hospital care
North East Hampshire and Farnham Vanguard
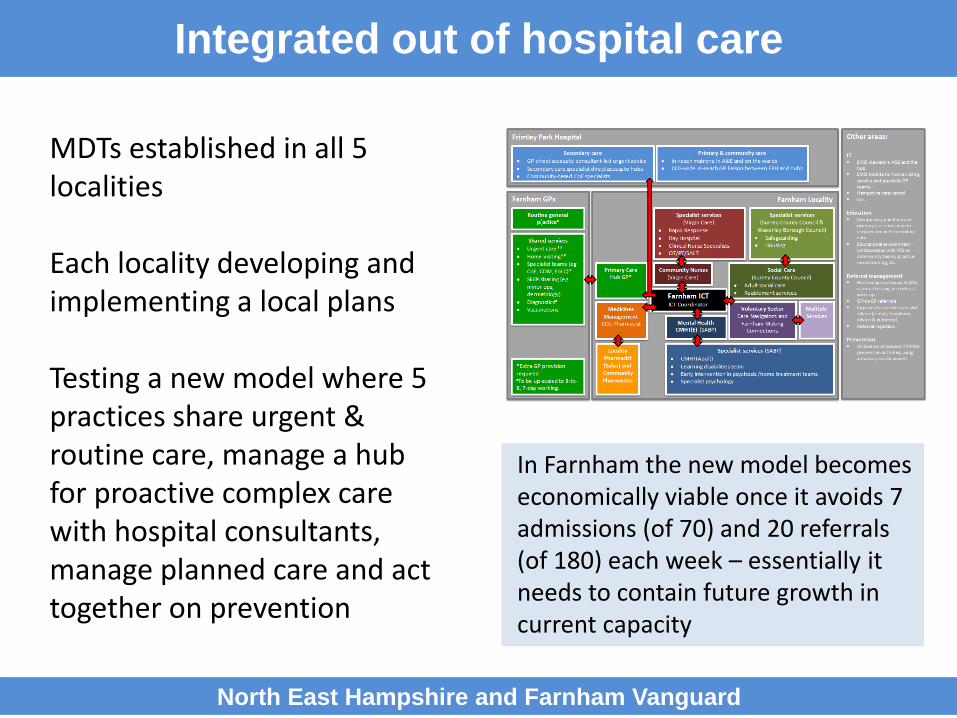
MDTs established in all 5 localities Each locality developing and implementing a local plans Testing a new model where 5 practices share urgent & routine care, manage a hub for proactive complex care with hospital consultants, manage planned care and act together on prevention
In Farnham the new model becomes economically viable once it avoids 7 admissions (of 70) and 20 referrals (of 180) each week – essentially it needs to contain future growth in current capacity

Primary and Acute Care
North East Hampshire and Farnham Vanguard
Frimley Park Hospital consultants supporting complex care in the community
GPs involved in the care and discharge of patients from Frimley Park Hospital

First draft whole system dashboard Measuring and Evaluating Change Sep-15
Domain MetricsTarget /
Standard
Current
Perf.RAG Sparkline Direction Red Amber Green
Happy Friends & Fami ly Test - Recommend Rate (IP & A&E) TBC 93.7% Happy 1 0 2 Total R A G
Friends & Fami ly Test - Recommend Rate (Community) Healthy 0 0 0 9 56% 0% 44% 56%
Friends & Fami ly Test - Recommend Rate (Primary Care) Home 0 0 1 - Green Rated
VFM 4 0 1
Healthy Admiss ion rates for #NOF (fa l l s ) TBC 37 Data Source to be determineTotal 5 0 4
Diabetes (HBA1C) TBC 79
Respiratory Emergency Admiss ions TBC 55 Data Source to be determine
Emergency admiss ions for cancer TBC 23 Data Source to be determine
Emergency CVD admiss ions TBC 46 Data Source to be determine
Dementia diagnos is rates 66.7% 61.0% Data Source to be determine
Qual i ty of l i fe with LTC 20% 25% Data Source to be determine
Cardiovascular Morta l i ty Social Care - Data Source to be determine
Data Source to be determine
Home A&E Attendances TBC
Proportion of people s ti l l at home after 91 days TBC 87.7%
Community Bed Days TBC 756
Perm. Admiss ions 65+ to res/nurs ing per 100,000 TBC 390
Supported to l ive at home TBC 38% Data Source to be determine% of socia l care cl ients who fel t their hops i ta l
discharge was wel l co-ordinatedTBC 19% TBC
VFMDelayed Transfer of Care (a l l ) per 100,000 pop TBC 12.1
Al l Emergency Admiss ions - Rate per 1,000 pop 166.5 262.9
Advoidable Emergency Admiss ion - Rate per 1,000 pop 39.4 59.9
Emergency Admiss ions for fa l l s - Rate per 1,000 pop 21.7 28.7
Admiss ions by Conditions 65-74 (Yearly)
Angina TBC 18
COPD TBC 147
Congested Heart Fa i lure (CHF) TBC 41
Convuls ions and Epi lepsy (C&E) TBC 72
Other TBC 23
Admiss ions by Conditions 75+ (Yearly)
Angina TBC 37
COPD TBC 162
Congested Heart Fa i lure (CHF) TBC 128
Convuls ions and Epi lepsy (C&E) TBC 128
Other TBC 83
Occupied Bed Days
Elective TBC 8261
Non Elective TBC 969
Metrics Performance
Placeholder
Placeholder
Executive Happy AllExecutive Healthy Home VFM
44%= Green RAG
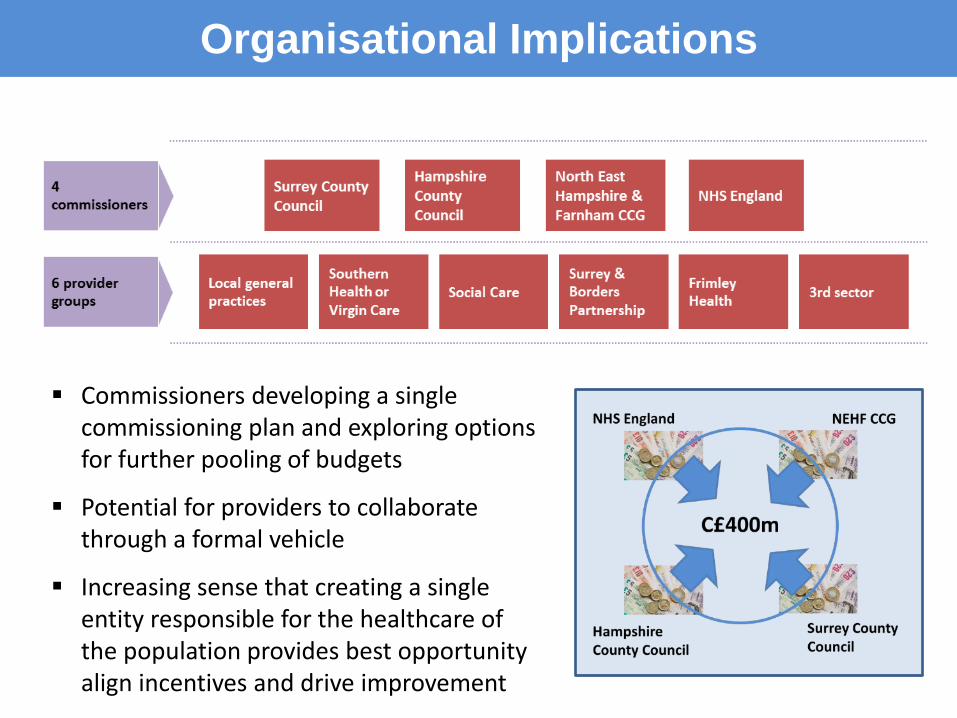
Organisational Implications
Commissioners developing a single commissioning plan and exploring options for further pooling of budgets
Potential for providers to collaborate through a formal vehicle
Increasing sense that creating a single entity responsible for the healthcare of the population provides best opportunity align incentives and drive improvement

Reflections
North East Hampshire and Farnham Vanguard
An opportunity to engage the whole system in innovation and learning
Evaluating the impact of the changes quickly, and adapting as we go is key
Using the spread methodology to replicate Rigour coupled with permissive culture … a balance! Population based and system based approach
requires organisations to cede sovereignty Requirement for a new regulatory regime
increasingly clear Justifiable scepticism about organisational change Ultimately its about people and behaviour

Happier, Healthier, At Home, Better Value







