OUTPATIENT CARDIAC REHABILITATION health professionals
1
Foreword
Coronary Heart Disease is a national and state health priority. CoronaryHeart Disease is responsible for significant morbidity and mortality, whichimpacts on the Queensland Health system, and more importantly, on thelives of those with coronary heart disease, their families and carers.
Queensland Health acknowledges that cardiac rehabilitation is animportant component of management following a cardiac event orintervention. The following guidelines have been developed to assist healthprofessionals deliver these services.
The Best Practice Guidelines for Outpatient Cardiac Rehabilitation identify:- evidence based practices in the area of cardiac rehabilitation- options for efficient service delivery; and- services that can be provided by a range of accredited service providers
These guidelines support the Health Outcomes Plan for CardiovascularHealth: Coronary Heart Disease 2000–2004 through implementation ofstrategies within the plan. They should be used in conjunction with theHealth Outcomes Plan to provide coordinated services to people withcoronary heart disease.
Queensland Health is committed to providing efficient and effectiveservices to people with coronary heart disease and these guidelinesprovide a blueprint for best practice in this area.
I recognise the significant work undertaken by health professionals andprofessional associations involved in the development of these guidelinesand thank all those involved in this process for their collaboration andsupport.
I am pleased to endorse these Guidelines and ask that health professionalsinvolved in the care of people with coronary heart disease become familiarwith this document and encourage its use.
Dr J YoungmanGeneral Manager, Health ServicesQueensland Health
ISBN:1-876532-62-9
health professionals OUTPATIENT CARDIAC REHABILITATION
2
Acknowledgments
The Health Advisory Unit in Queensland Health initiated the development ofOutpatient Cardiac Rehabilitation Best Practice Guidelines for healthprofessionals. Expressions of interest in being involved in developing theseguidelines were sought from members of cardiac rehabilitation centres,professional associations and universities throughout Queensland. Focusgroups were formed that consisted of a range of health professionals throughoutQueensland with an interest in the development of cardiac rehabilitationguidelines. The following people were members of focus groups that contributedto the development of the best practice guidelines for Outpatient CardiacRehabilitation – Best Practice Guidelines for Health Professionals.
Steven Bartlett St Andrew’s HospitalNicole Bellet The Prince Charles HosptialSueann Case National Heart FoundationLisa Cowen St Andrew’s HospitalHelen Curran The Prince Charles HospitalJoanne Ede Princess Alexandra HospitalLyndal Forbe-Smith The Prince Charles HospitalPam Fung The Prince Charles HospitalAnna Hawkes North Queensland Rural Division of General PracticeNicole Heath The Prince Charles HospitalHelen Higgins Queensland University of TechnologyMarcy Holdsworth North Queensland Rural Division of General PracticeAloysa Hourigan Logan Area Division of General PracticeDr Justin Kenardy The University of QueenslandEleanor Kerr The Prince Charles HospitalSandy McKellar The Wesley HospitalAlison Mahoney Princess Alexandra HospitalLibby Morrow National Heart Foundation/Health Outcomes UnitJan Payne Queensland University of TechnologyAndrea Quinn Griffith UniversityEve Radford Redcliffe HospitalDr Carrie Ritchie The University of QueenslandRosemary Robinson Princess Alexandra HospitalVickie Scells Redlands HospitalLea-Anne Smith Ipswich and West Moreton Division of General PracticeEsben Strodl Ipswich HospitalJudith Trevan-Hawke James Cook UniversityConnie Tunny The Prince Charles HospitalAns Van Erp Toowoomba Base HospitalSue Woods Cairns Base Hospital
OUTPATIENT CARDIAC REHABILITATION health professionals
3
Contents
Acknowledgments 2
1. Aim of this document 51.1 Other sources of information 5
2. Evidence 52.1 Evidence basis of document 52.2 Evidence regarding the benefits of cardiac rehabilitation 6
3. Cardiac Rehabilitation 62.1 Aims of cardiac rehabilitation 72.2 Phases of cardiac rehabilitation 7
4. Menu based approach to outpatient cardiac rehabilitation 84.1 Application at the local level 8
4.1.1 How to use this document 84.1.2 Prioritisation 94.1.3 Multidisciplinary teams 9
5. Standards of practice 95.1 Professional competence 95.2 Skill mix 95.3 Training 10
5.2.1 Indigenous health workers 10
6. Referrals 106.1 Referral to cardiac rehabilitation 106.2 Benefit of cardiac rehabilitation to others 10
7. Models of service delivery 117.1 Group programs 117.2 Barriers to group participation 117.3 Alternative models of delivery of cardiac rehabilitation 12
8. Elements of outpatient cardiac rehabilitation 128.1 Integration of cardiac rehabilitation elements 128.2 General Assessment 13
9. Physical activity 139.1 Introduction 13
9.1.1 Definitions 139.2 Aims of exercise 159.3 Factors to consider on referral 15
9.3.1 Exclusion from exercise – criteria 159.3.2 Other patient complications 159.3.3 Consultation with the treating physician 16
9.4 Low to moderate intensity exercise 169.5 Other factors 16
9.5.1 Safety procedures 169.6 Assessments and interventions 17
health professionals OUTPATIENT CARDIAC REHABILITATION
4
10. Education, discussion and counselling 2010.1 Importance of education discussion and counselling 2010.2 Education 20
10.2.1 Effectiveness 2010.2.2 Education topics 21
10. 3 Counselling 24
11. Progression to the maintenance phase of cardiacrehabilitation 2611.1 Ongoing maintenance 27
Glossary 27
References 28
Appendices
Appendix 1 31Further information
Appendix 2 32Outpatient cardiac rehabilitation – local area contacts
Appendix 3 33Minimum data set collection standards
Appendix 4 34Screening tools
Appendix 5 35Guide to exercise and physical activity levels
Appendix 6 36Borg rating of percieved exertion scale
Appendix 7 37Desired outcomes and objectives of nutrition interventions
OUTPATIENT CARDIAC REHABILITATION health professionals
5
1. Aim of this document
The expectation for the development of anyclinical practice guidelines is that thedocumented assessment and managementstrategies are supported by evidence showingthat the listed practices produce positiveoutcomes.
These cardiac rehabilitation guidelines do notaim to review the literature to reproduceevidence based documents. They aim tosource evidence based information includingmeta-analyses and systematic reviews toinform health professionals about practices inoutpatient cardiac rehabilitation that areevidence based.
1.1 Other sources ofinformation
These guidelines are designed to assist thehealth professional deliver efficient andeffective services based on patient needs andthe resources available. They are not designedto educate the health professional in the areaof cardiac rehabilitation.
For more information on the content ofthorough assessments and interventions forcardiac rehabilitation, refer to Appendix 1.
2. Evidence
2.1 Evidence basis ofdocument
A large amount of research has been publishedon the subject of outpatient cardiac rehabilitation.To obtain evidence based systematic reviews and
meta-analyses regarding outpatient rehab-ilitation, searches were done of CochraneDatabases, the NHS Centre for Reviews andDissemination – University of York, EvidenceBased Medicine Review Database and Medline.Medline searches were also used to obtainconsensus statements and reviews.
Existing guidelines on cardiac rehabilitationwere also sought. A number of sources (NSWHealth1, Heart Research Centre, Victoria2, U.S.Department of Health and Human Services3,NHS Centre for Reviews and Dissemination4)have reviewed this literature and produced anevidence basis to practice guidelines forcardiac rehabilitation. NSW Health1 and theHeart Research Centre3, have assignedevidence using the NHMRC Quality ofEvidence rating scale5. This scale has beenused to support information presented withinthis document and is explained below.
I Evidence obtained from a systematicreview of randomised controlled trials,providing that it includes at least twoproperly designed trials of moderatesize or a systematic review that doesnot include trails which it could bereasonably argued could not effect thefindings of the review
II Evidence obtained from a least oneproperly designed randomisedcontrolled trial.
III Evidence obtained from a welldesigned controlled trial withoutrandomisation, from well designedcohort or case – controlled analyticstudies, preferably from more than onecentre or research group or frommultiple time series with or withoutintervention.
IV Opinions of respected authorities,based on clinical experience,descriptive studies or reports of expertcommittees.
health professionals OUTPATIENT CARDIAC REHABILITATION
6
2.2 Evidence regarding thebenefits of cardiacrehabilitation
Goble and Worcester2,6 reviewed availableliterature to determine evidence of the benefitsof cardiac rehabilitation. They concluded thatcardiac rehabilitation could be of benefit in:
Risk factor outcomes- reduced smoking (level of evidence 2)- improved lipids (level of evidence 2)- reduced weight (level of evidence 2)- lower blood pressure (level of evidence 2)- improved subsequent exercise habits (level
of evidence 3)
Physical outcomes- improved exercise tolerance (Level of
evidence 1)- improved muscular strength (level of
evidence 1)- reduced symptoms (level of evidence 1)- reduced morbidity (level of evidence 1)- reduced mortality (level of evidence 2)- retardation of atherosclerosis (level of
evidence 2)
Psychosocial outcomes- less anxiety (level of evidence 1)- less depression (level of evidence 1)- improved wellbeing (level of evidence 1)- improved social functioning (level of
evidence 1)- greater knowledge (level of evidence 2)- reduced stress (level of evidence 3)- increased return to work (level of evidence 3)
(from: Goble and Worcester (1999)6 Best PracticeGuidelines for Cardiac Rehabilitation and SecondaryPrevention: A synopsis. Heart Reseach Centre.Melbourne, on behalf of the Department of HumanServices Victoria).
This evidence indicates that exercise, physicalactivity, nutritional, education, discussion andcounselling interventions can be used in
combination to have substantial impact on aperson’s wellbeing.
The processes, personnel and organisation ofservices required to provide outpatient cardiacrehabilitation detailed in this document is basedon the following evidence:- access to outpatient cardiac rehabilitation
should be offered to all patients (level ofevidence 12)
- components of cardiac rehabilitation can beof benefit to spouse/family/support person/carer (level of evidence 32,4)
- group programs are effective for exercise/physical activity (level of evidence 22)
- group sessions are effective for education,discussion and counselling (level ofevidence 42)
- alternative models of service delivery shouldbe implemented where appropriate (level ofevidence 21)
- most effective cardiac rehabilitationprograms involve the integration ofcomponents (level of evidence 23,4)
- multidisciplinary teams should be usedwhere possible to provide outpatient cardiacrehabilitation (level of evidence 41,2)
3. Cardiac rehabilitationLevel of evidence 11,2,3,7
Coronary heart disease is responsible forsignificant morbidity and mortality withinAustralia. Queensland Health acknowledgesthat cardiac rehabilitation is an importantcomponent of the rehabilitation process forpeople with coronary heart disease.
Appropriate education, counselling, physicalactivity and exercise following a cardiac eventor intervention has been shown to havebeneficial physical, social and psychological
OUTPATIENT CARDIAC REHABILITATION health professionals
7
effects. Therefore, these outpatient cardiacrehabilitation guidelines for health profes-sionals have been developed to assist healthprofessionals in the delivery of these services.
The National Heart Foundation of Australia7
describes cardiac rehabilitation as including “allmeasures used to help cardiac patients returnto an active and satisfying life and to preventthe recurrence of cardiac events”. Cardiacrehabilitation “should be an integral componentof the long-term, comprehensive care of acardiac patient”7.
3.1 Aims of cardiacrehabilitation
The National Heart Foundation7 states that thegeneral aims of cardiac rehabilitation include:- maximising physical, psychological and
social functioning to enable patients to liveproductively and with confidence
- assisting and encouraging behaviours thatmay minimise the risk of further cardiacevents and conditions
This document supports the above aims andfocuses on assisting health professionalsinvolved in outpatient cardiac rehabilitation toachieve them.
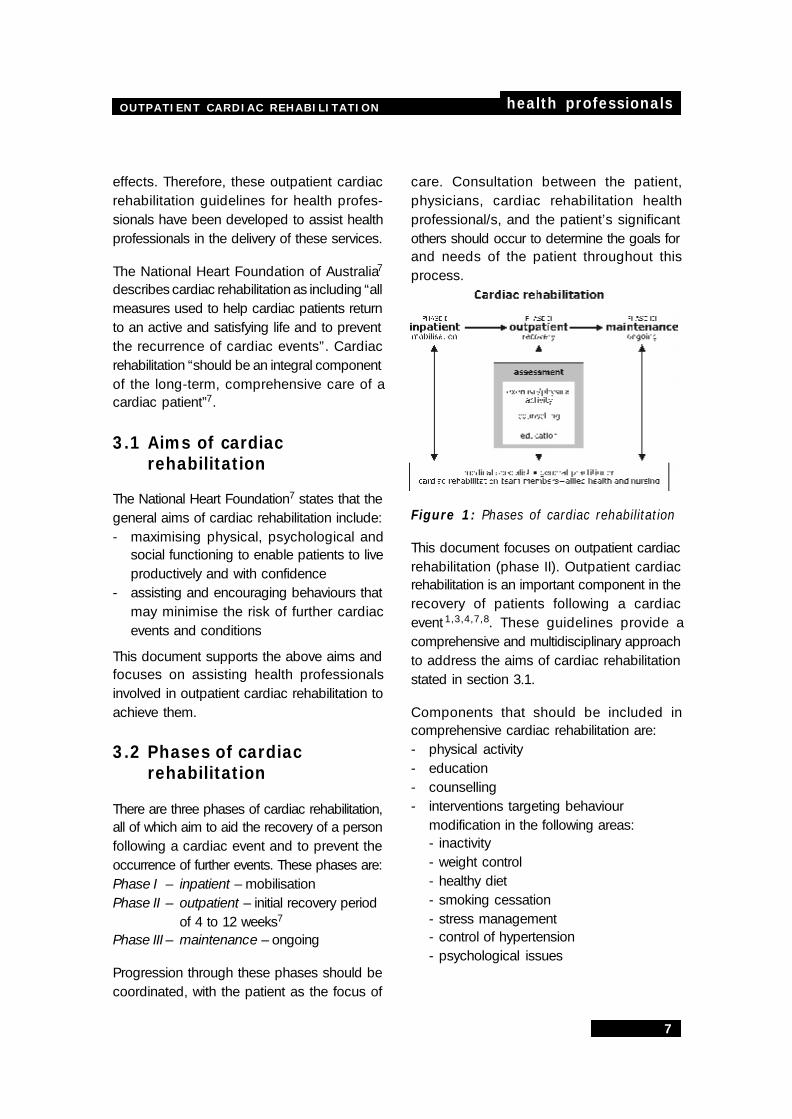
3.2 Phases of cardiacrehabilitation
There are three phases of cardiac rehabilitation,all of which aim to aid the recovery of a personfollowing a cardiac event and to prevent theoccurrence of further events. These phases are:Phase I – inpatient – mobilisationPhase II – outpatient – initial recovery period
of 4 to 12 weeks7
Phase III – maintenance – ongoing
Progression through these phases should becoordinated, with the patient as the focus of
care. Consultation between the patient,physicians, cardiac rehabilitation healthprofessional/s, and the patient’s significantothers should occur to determine the goals forand needs of the patient throughout thisprocess.
Figure 1: Phases of cardiac rehabilitation
This document focuses on outpatient cardiacrehabilitation (phase II). Outpatient cardiacrehabilitation is an important component in therecovery of patients following a cardiacevent 1,3,4,7,8. These guidelines provide acomprehensive and multidisciplinary approachto address the aims of cardiac rehabilitationstated in section 3.1.
Components that should be included incomprehensive cardiac rehabilitation are:- physical activity- education- counselling- interventions targeting behaviour
modification in the following areas:- inactivity- weight control- healthy diet- smoking cessation- stress management- control of hypertension- psychological issues
health professionals OUTPATIENT CARDIAC REHABILITATION
8
4. Menu based approachto outpatient cardiacrehabilitation
These best practice guidelines provideflexibility within an evidence based frame-work. They aim to assist health profes-sionals working in the area of cardiacrehabilitation to manage a patient throughthe cardiac rehabilitation outpatientprogram, to assess prospective clientsand appropriately intervene in patient careto meet the individual needs and goals ofpatients. Health professionals shouldselect assessments and interventions thatare appropriate for individual patients.
As well as clinical decision makingconsiderations, this document alsoemphasises the effectiveness of a multi-factorial integrated approach to cardiacrehabilitation and highlights managementconsiderations regarding access to anddelivery of services.
It is recognised that circumstances mayarise that necessitate variation fromparticular aspects in these guidelines. Inthese instances, it is recommended thathealth professionals exercise independentjudgement as to what is appropriate forindividual patients or groups of patients inspecific circumstances.
4.1 Application at the locallevel
4.1.1 How to use this document
To assist health professionals navigate theirway through the document the following guidehas been provided. Steps to consider at thelocal level would be to:
1. negotiate a referral process to ensureappropriate referrals are received (section6)
2. gather general clinical data (Table 1,Section 8)
3. prioritise delivery of services if necessary(Section 4.1.2)
4. determine the appropriate method ofservice delivery (Section 7)
5. discuss with health professionalsavailable, those most skilled to carry outtasks (Section 5)
6. provide education on topics related toCHD (Table 6, Section 10)
7. assess the needs of the patient in areasof physical activity/exercise andcounselling/risk factor modification, usingselected assessments as necessary(Table 2, Section 9 and Table 7, Section10)
8. determine areas requiring intervention –select interventions (Tables 3 and 4,Section 9 and Table 7, Section 10) andrefer on if necessary
9. discuss patient progress with patient’sgeneral practitioner and medicalspecialists throughout the outpatientphase as necessary
10. reassess and modify interventionsaccording to the changing needs of thepatient
11. at the completion of the outpatientphase, discuss the long term needs andmaintenance phase options with thepatient and family, medical specialistand/or general practitioner (Section 11)

OUTPATIENT CARDIAC REHABILITATION health professionals
9
4.1.2 Prioritisation
The aim of any service is to provide timelyintervention for all people requiring cardiacrehabilitation. It is important to note that priorityof access to comprehensive outpatient cardiacrehabilitation may vary according to theindividual’s personal health and well being, riskstatus, the resources available and healthprofessional availability.
Prioritisation can only be determined at thelocal level and should be guided by clinicaljudgement as individuals requiring cardiacrehabilitation are identified. For example, healthprofessionals may need to prioritise interven-tions for a patient following a myocardialinfarction who smokes, has borderline hyper-tension, is inactive and overweight.
4.1.3 Multidisciplinary teams
The World Health Organisation9 recommendsthat for best practice, a multidisciplinary teamof health professionals should conduct cardiacrehabilitation programs in ‘intermediatefacilities’ such as metropolitan and large ruralcentre hospitals/community health centres9.
Goble and Worcester2 suggest that whereaccess to group programs is difficult, outpatientcardiac rehabilitation may be conducted by asingle health professional with support fromother regional health professionals. This isconsistent with the appropriate staffing of a‘basic facility’ as described by the World HealthOrganisation8.
Appendix 2 has been included to record thedetails of health professionals within a localarea with the capacity to participate in cardiacrehabilitation.
5. Standards of practice
5.1 Professional competence
These guidelines are provided to assist trainedhealth professionals provide care to individualsrequiring outpatient cardiac rehabilitation.These health professionals include those witha degree, diploma or a certificate of registrationin exercise physiology, medicine, nursing,occupational therapy, nutrition and dietetics,physiotherapy, psychology or social work.
These guidelines should not be used by peoplewho have not completed the appropriate levelof training. This may lead to information withinthe guidelines being applied incorrectly and/or out of context.
Ultimately, the responsibility for deliveringservices which meet the appropriate standardof care lies with the health professional. It isthe individual health professionals’ respon-sibility to ensure they adhere to and work withintheir personal skill level and scope of practiceoutlined by their professional boards andassociations. Therefore, the health professionalis responsible for referring patients toappropriate health professionals when theexpertise required is outside their skill level.
5.2 Skill mix
Many different health professionals contributeto the cardiac rehabilitation of an individual.These individuals have training and expertisein specific areas of cardiac rehabilitation.However, in some parts of Queensland accessto all professionals is not available.
Skill mix can be defined as the range of healthprofessionals with the knowledge and skillsnecessary to deliver specific components of

health professionals OUTPATIENT CARDIAC REHABILITATION
10
outpatient cardiac rehabilitation. Analphabetical list of health professionals hasbeen included in the skill mix columns of theclinical activity tables which follow. They havebeen included to help the health professionalidentify the appropriate professionals forspecific parts of the program. If appropriateprofessionals are available, these guidelinesrecommend they be included in the cardiacrehabilitation team.
Health professionals involved in outpatientcardiac rehabilitation should educate eachother on their role and scope of practice. Thiswill enable appropriate referrals, coordinationof patient care and support, and complementmedical care provided by cardiac specialistsand general practitioners.
5.3 Training
The Heart Foundation of Australia7
recommends that health professionalsproviding cardiac rehabilitation shouldhave training and/or work experiencethat includes education and physicalactivity components of cardiac rehab-ilitation in addition to their professionalqualifications.
Training may be appropriate in some instancesto increase the level of knowledge and skills ofthose professionals providing cardiacrehabilitation programs. There are a variety ofaccredited courses available that may fulfilthese needs.
5.2.1 Indigenous health workers
If identified by the patient as appropriate,Indigenous health workers should beincluded in the cardiac rehabilitation teamto work with other health professionals toprovide best practice cardiac rehabilitationservices to Indigenous people.
In these guidelines it is assumed thatIndigenous health workers who provideinformation regarding cardiac rehab-ilitation have undergone appropriatetraining. An example of one suchprogram is the VETEC accreditedprogram “Course in Cardiac Rehab-ilitation and Secondary Prevention forIndigenous Health Workers”10.
6. Referrals
6.1 Referral to cardiacrehabilitationLevel of evidence 12
Cardiac rehabilitation, includingoutpatient rehabilitation1,2,7,8 should beavailable to anyone who has had anacute myocardial infarction, coronaryartery bypass grafts, coronaryangioplasty or other cardiovasculardisease2. Cardiac rehabilitation plays acrucial role in secondary prevention aswell as aiding individuals to return to aproductive and satisfying life.
In most cases, patient are referred tocardiac rehabilitation by their cardiacphysican, surgeon, or generalpractitioner. Negotiation of pathwaysand methods of referral should bedetermined at the local level.
6.2 Benefit of cardiacrehabilitation to othersLevel of evidence 32
The benefits of cardiac rehabilitationshould not be limited to people who havesuffered a cardiac event, but shouldinvolve the patient’s family/carer/ supportperson/spouse. There is some evidence
OUTPATIENT CARDIAC REHABILITATION health professionals
11
to demonstrate that the inclusion offamilies and carers in the cardiacrehabilitation process can improve patientoutcomes and that access, uptake ofinformation and adherence is more likelywhen partners are involved4,11
Education of patients and their partnershas been reported to result in improvedknowledge, decreased disability andhealth behaviour modification4.
In addition, families and support peoplemay suffer considerable changes to theirlifestyle and emotional status due to thepatient’s cardiac status4, and levels ofanxiety and depression seen in spousesmay equal those seen in patients. Asthese key individuals play a vital role inthe cardiac rehabilitation process, theyshould be included where appropriate,and should themselves be considered forintervention if necessary.
7. Models of servicedelivery
As each person is an individual with differentneeds, the method of service delivery forcardiac rehabilitation is different for eachperson. It is therefore essential to assess theappropriate method for delivering outpatientcardiac rehabilitation ie. in groups, individually,by reading material, by video or audiotape.Ongoing assessment should occur todetermine if changes in service delivery needto be made.
7.1 Group programsLevel of evidence 22 (exercise)Level of evidence 42 (counsellingand education)
At present, evidence is available to indicate thatgroup programs are effective for counselling,education and exercise in the context ofoutpatient cardiac rehabilitation. The benefitsof group participation include improved socialinteraction and support, which may enhanceself-efficacy and motivation.
In some instances, practitioners may identifypeople who require individual intervention orlong term management in some areas.Therefore group sessions may precede orfollow individual sessions. Referral on toappropriate health professional/s should occurif identified as appropriate and should beconducted in a manner that does not diminishor challenge an individual’s right to privacy.
Group sessions can involve the patient and/orthe patient’s family/carer/ support person/spouse (level of evidence 33). Benefits to thisgroup have been discussed in section 6.
7.2 Barriers to groupparticipation
Many factors may dictate other modes of servicedelivery for all or some aspects of comprehensiveoutpatient cardiac rehabilitation.
Factors which may prevent individuals fromparticipating in a group situation include:- the absence of a structured cardiac
rehabilitation program- times of programs- travelling time to attend cardiac
rehabilitation programs- access and the availability of transport- financial constraints- the number of health professionals available
Factors impacting on an individual’s ability togain the full benefit from group sessions couldinclude:

health professionals OUTPATIENT CARDIAC REHABILITATION
12
- cultural issues- high risk patients- co-morbidities which influence recovery/
rehabilitation- work issues/early return to work- language and literacy/communication
barriers- physical/cognitive/ behavioural issues- psychosocial issues- discomfort disclosing problems in a group
environment- major barriers to change- the individual’s needs and goals- personal motivation- professional discretion- individual’s choice
Therefore, individually tailored componentsshould be implemented in addition to groupactivity where appropriate. Specialconsideration should also be given toindividuals who are unable to derive the fullbenefit from written handout material becauseof literacy problems, visual impairment or ifEnglish is a second language.
7.3 Alternative models ofdelivery of cardiacrehabilitationLevel of evidence 21
The Health Outcomes Plan for CardiovascularHealth: Coronary Heart Disease 2000-200412
states that Queensland Health is workingtowards providing a comprehensive mix ofsecondary prevention services to meet theneeds of all patients with known coronary heartdisease, after an acute coronary event orsurgical procedure. To ensure that patientshave equal access to cardiac rehabilitationoutpatient programs suitable to individualneeds, alternative models of service deliveryneed to be explored to encourage participation.
The following (non-exhaustive) list ofalternative models may help healthprofessionals determine the most effectivemethod of service delivery for theirparticular area:- use of home-based programs which
may include written educationmodules, regular telephone contact,videos (level of evidence 21,4)
- cardiac rehabilitation provided at timesthat suit working patients (ie – out ofworking hours)
- accelerated cardiac rehabilitationprograms provided for some patienttypes (eg. four week cardiacrehabilitation programs for angioplastypatients) (level of evidence 32)
- regular individual consultations/appointments if necessary (eg. forcounselling) (level of evidence 21)
- comprehensive discharge plan andregular telephone contact
- use of video link-ups with largercentres
- use of visiting regional healthprofessionals
- outreach programs with the generalpractitioner as the facilitator
8. Elements of outpatientcardiac rehabilitation
8.1 Integration of cardiacrehabilitation elementsLevel of evidence 24
Outpatient cardiac rehabilitation consistsof a number of components including riskfactor management, education,counselling, behaviour change, nutrition,exercise and physical activity. Integrationof these components occurs naturally incardiac rehabilitation programs.

OUTPATIENT CARDIAC REHABILITATION health professionals
13
In order to provide patient focusedinterventions, health professionals needto combine these areas to achieve thepatient’s goals and needs. Thecombination of these interventionsappears to be more beneficial thanbenefits achieved from interventionsfrom a single modality4. It should bestressed that these components, whentaken in isolation, are not considered toprovide comprehensive care to thecardiac patient.
To ensure that all individuals referred foroutpatient cardiac rehabilitation receiveappropriate, timely and tailoredinterventions, it is recommended thathealth professionals:- consult with the individual’s medical
specialist and general practitioner- perform a general assessment to
determine the patients needs (seeSection 8.1)
- consult with other members of thecardiac rehabilitation team and referto health professionals in the area ofphysical activity/exercise, diet,counselling and education forassessment to determineappropriate interventions (seesections 9 and 10)
- consider appointing a cardiacrehabilitation coordinator to assistwith coordinated delivery of cardiacrehabilitation throughout all phases
8.2 General assessment
When an individual is referred tooutpatient cardiac rehabilitation, generalinformation should be obtained, if notalready available, by health professional/sinvolved in the area of cardiacrehabilitation. Consultation with, or referralby, the individual’s medical specialist and/
or general practitioner should occur, asthe medical officer is responsible for theoverall management of the patient.
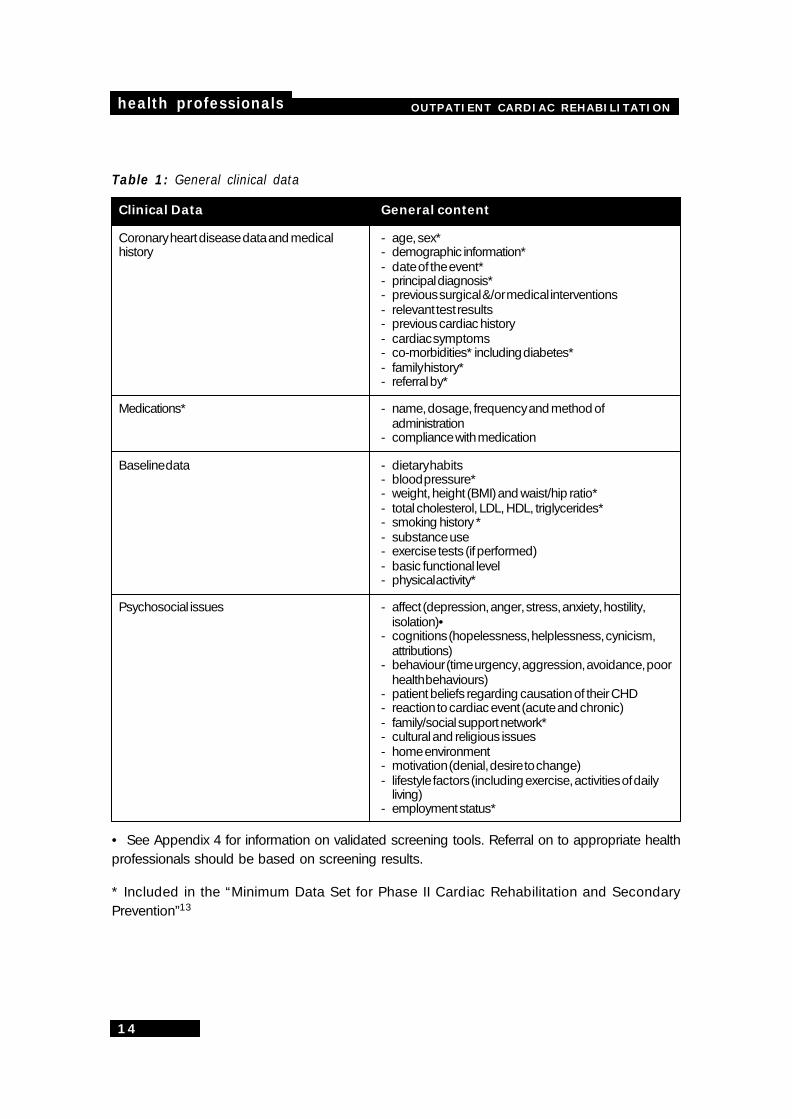
The general clinical information detailedin Table 1 (page 14) covers a range ofareas and is considered to be theoptimal level of information needed todevelop a patient profile. Theinformation can be used to highlightareas to be addressed by theappropriate members of the cardiacrehabilitation team.
Items identified with a * are thoseincluded in the “Minimum Data Set forPhase II Cardiac Rehabilitation andSecondary Prevention”13 developed bythe Queensland Cardiac RehabilitationAssociation and the Heart Foundation ofAustralia (Queensland). Please refer toAppendix 3 for a copy of this minimumdata set.
9. Physical activity
9.1 Introduction
Physical activity and exercise are importantcomponents of cardiac rehabilitation. The aimof physical activity and exercise includesreturning the individual to an appropriate levelof function, improving the individual’s qualityof life, providing risk factor modification as wellas meeting the client’s goals and needs.
9.1.1 Definitions
This document supports the followingdefinitions of physical activity and exercise asdescribed in “Physical activity for people withheart disease”14.
health professionals OUTPATIENT CARDIAC REHABILITATION
14
Table 1: General clinical data
Clinical Data General content
Coronary heart disease data and medical - age, sex*history - demographic information*
- date of the event*- principal diagnosis*- previous surgical &/or medical interventions- relevant test results- previous cardiac history- cardiac symptoms- co-morbidities* including diabetes*- family history*- referral by*
Medications* - name, dosage, frequency and method ofadministration
- compliance with medication
Baseline data - dietary habits- blood pressure*- weight, height (BMI) and waist/hip ratio*- total cholesterol, LDL, HDL, triglycerides*- smoking history *- substance use- exercise tests (if performed)- basic functional level- physical activity*
Psychosocial issues - affect (depression, anger, stress, anxiety, hostility,isolation)•
- cognitions (hopelessness, helplessness, cynicism,attributions)
- behaviour (time urgency, aggression, avoidance, poorhealth behaviours)
- patient beliefs regarding causation of their CHD- reaction to cardiac event (acute and chronic)- family/social support network*- cultural and religious issues- home environment- motivation (denial, desire to change)- lifestyle factors (including exercise, activities of daily
living)- employment status*
• See Appendix 4 for information on validated screening tools. Referral on to appropriate healthprofessionals should be based on screening results.
* Included in the “Minimum Data Set for Phase II Cardiac Rehabilitation and SecondaryPrevention”13
OUTPATIENT CARDIAC REHABILITATION health professionals
15
Physical activity: any bodily movementproduced by skeletal muscles that results inenergy expenditure.
Exercise: planned, structured and repetitivemovement which is done to improve or maintainone or more components of physical fitness.
Therefore, exercise is a component of physicalactivity.
For some individuals with low activity tolerance,tasks classified as physical activity (such asshowering and sweeping) are exercise. Forthese guidelines, they are to be classified asphysical activity and it is recommended thathealth professionals highlight the inclusion ofthese activities as exercise to appropriatepatients. A table highlighting comparable levelsof activity across a range of areas can be seenin Appendix 5.
9.2 Aims of exercise
In a formal structured program, outpatientcardiac rehabilitation is generally consideredto span 4-12 weeks7.
Aims of the physical activity/exercisecomponent of cardiac rehabilitation are to:- create exercise habits both in the group
situation (if appropriate) and at home, thatcan be sustained long term
- achieve an improvement in exercisecapacity
- return the patient to their pre-morbid activitylevel or to improve on this level
A home program of exercise prescribed forpatients unable to attend outpatient exercisesessions, or in addition to these sessions, isan important component of cardiacrehabilitation.
9.3 Factors to consider onreferral
9.3.1 Exclusion from exercise –criteria
These guidelines concur with the view of TheAmerican College of Sports Medicine15, thatstates that patients should be excluded fromexercise in the following instances:- significant hypertension or hypotension- severe aortic stenosis- the following uncontrolled conditions:
arrhythmia, congestive heart failure,diabetes or metabolic disturbance
- high grade atrioventricular block withoutpacemaker
- current pericarditis or myocarditis- recent pulmonary or other embolism- recent stroke or transient ischaemic attack- recent major surgery- terminal illness or severe disabling
concurrent illness- acute febrile or systemic illness- physical or psychological disability
preventing participation- physician refusal- patient refusal
This publication15 should be consulted for moreinformation on this topic. Clinical judgementshould also be used in determining ifparticipation in structured exercise programsis appropriate.
9.3.2 Other patient complications
Patients with impaired ventricular function,controlled cardiac failure and symptomatic orasymptomatic residual ischaemia weretraditionally excluded from exercise training. Ithas recently been stated that low to moderateintensity exercise is of benefit to these patients(level of evidence 11,2,3,4.).

health professionals OUTPATIENT CARDIAC REHABILITATION
16
Patients excluded from exercise could beconsidered for participation in low level physicalactivity programs and should still be involvedin other areas of cardiac rehabilitation (ie.education, discussion and counselling) asrequired.
9.3.3 Consultation with the treatingphysician
It is recommended that health professionalsconsult and collaborate with the patient’streating physician to ensure patients excludedfrom participating in exercise training areinvolved in the exercise and/or physical activitycomponents of cardiac rehabilitation as soonas they are physically able.
9.4 Low to moderate intensityexerciseLevel of evidence 21,2
The exercise/physical activity component ofcardiac rehabilitation can be provided to a largerange of individuals who have had surgical and/or medical interventions. The types of physicalactivity or exercise that individuals can performvary considerably.
These guidelines recommend low to moderateintensity exercise for outpatient cardiacrehabilitation. Evidence suggests no additionalbenefits are gained from high intensity exercise.Techniques used to monitor exercise intensityare detailed in Table 4. Refer to Appendix 6 forinformation on the Borg Rating of PerceivedExertion Scale.
If high intensity exercise is prescribed, a pre-program maximum exercise stress test,medical clearance and a higher degree ofmonitoring is required during exercise to safelymanage these patients2.
In addition to exercise in the cardiac
rehabilitation setting, it has been shown thatbenefits can be achieved through physicalactivity as well as structured exercise9,17 TheNational Heart Foundation17 and others16,17, 19
recommend the inclusion of regular moderateintensity physical activity for at least 30 minuteson most, if not all, days of the week. This activitycould be achieved in a single session, oraccumulated in multiple bouts of shortersessions throughout the day16,18.
Therefore, in general, exercise and physicalactivity prescription should aim for moderateactivity, as specified above. However individualpatients’ self care, occupational or leisureneeds may require modification of this. Issuesto be considered prior to the prescription ofany exercise/activity program are detailed inTables 1 and 2.
9.5 Other factors
9.5.1 Safety proceduresLevel of evidence 41,2,7,8
When planning physical activity and exercisegroup sessions, health professionals shouldensure that:- an emergency protocol is established and
documented and where appropriate,emergency equipment is accessible
- health professionals supervising thesessions should have a current CPRaccreditation/competency
- the number of health professionalssupervising the session is appropriate forthe number of and diagnosis of the groupparticipants, also taking into considerationthe type of exercise sessions planned(eg.one person to 10 patients for low tomoderate intensity – level of evidence 42)
OUTPATIENT CARDIAC REHABILITATION health professionals
17
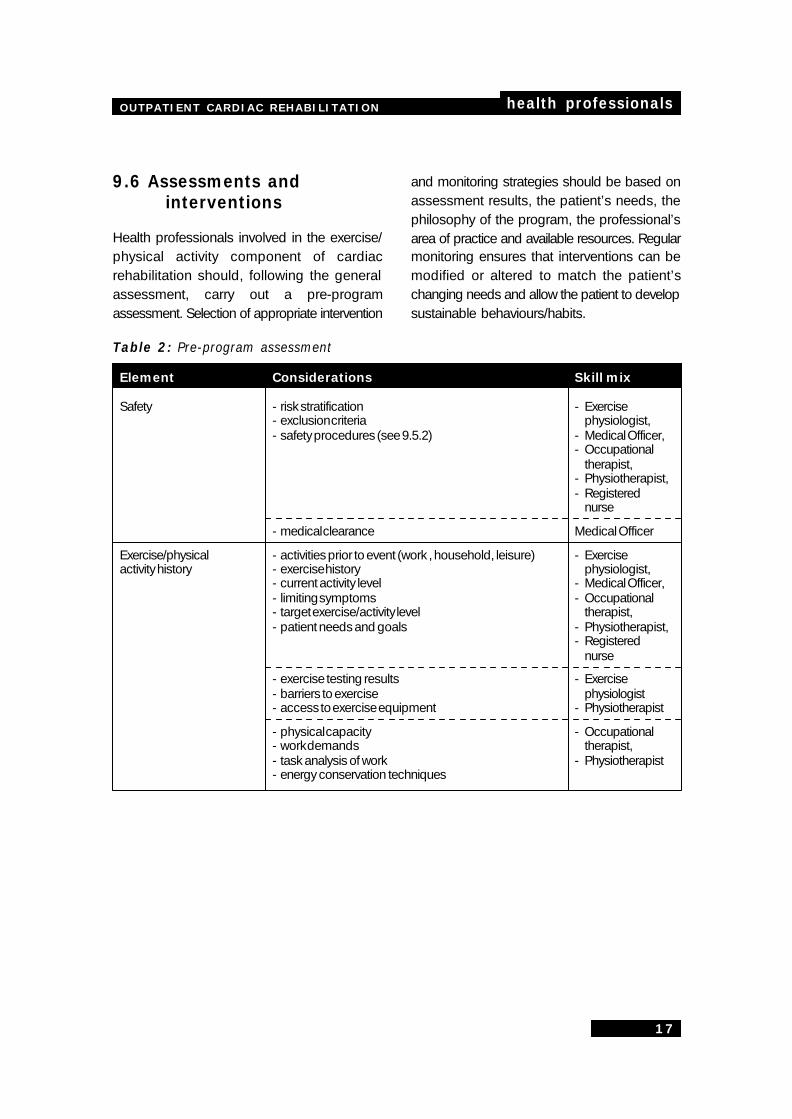
9.6 Assessments andinterventions
Health professionals involved in the exercise/physical activity component of cardiacrehabilitation should, following the generalassessment, carry out a pre-programassessment. Selection of appropriate intervention
and monitoring strategies should be based onassessment results, the patient’s needs, thephilosophy of the program, the professional’sarea of practice and available resources. Regularmonitoring ensures that interventions can bemodified or altered to match the patient’schanging needs and allow the patient to developsustainable behaviours/habits.
Table 2: Pre-program assessment
Element Considerations Skill mix
Safety - risk stratification - Exercise- exclusion criteria physiologist,- safety procedures (see 9.5.2) - Medical Officer,
- Occupationaltherapist,
- Physiotherapist,- Registered
nurse
- medical clearance Medical Officer
Exercise/physical - activities prior to event (work , household, leisure) - Exerciseactivity history - exercise history physiologist,
- current activity level - Medical Officer,- limiting symptoms - Occupational- target exercise/activity level therapist,- patient needs and goals - Physiotherapist,
- Registerednurse
- exercise testing results - Exercise- barriers to exercise physiologist- access to exercise equipment - Physiotherapist
- physical capacity - Occupational- work demands therapist,- task analysis of work - Physiotherapist- energy conservation techniques
health professionals OUTPATIENT CARDIAC REHABILITATION
18
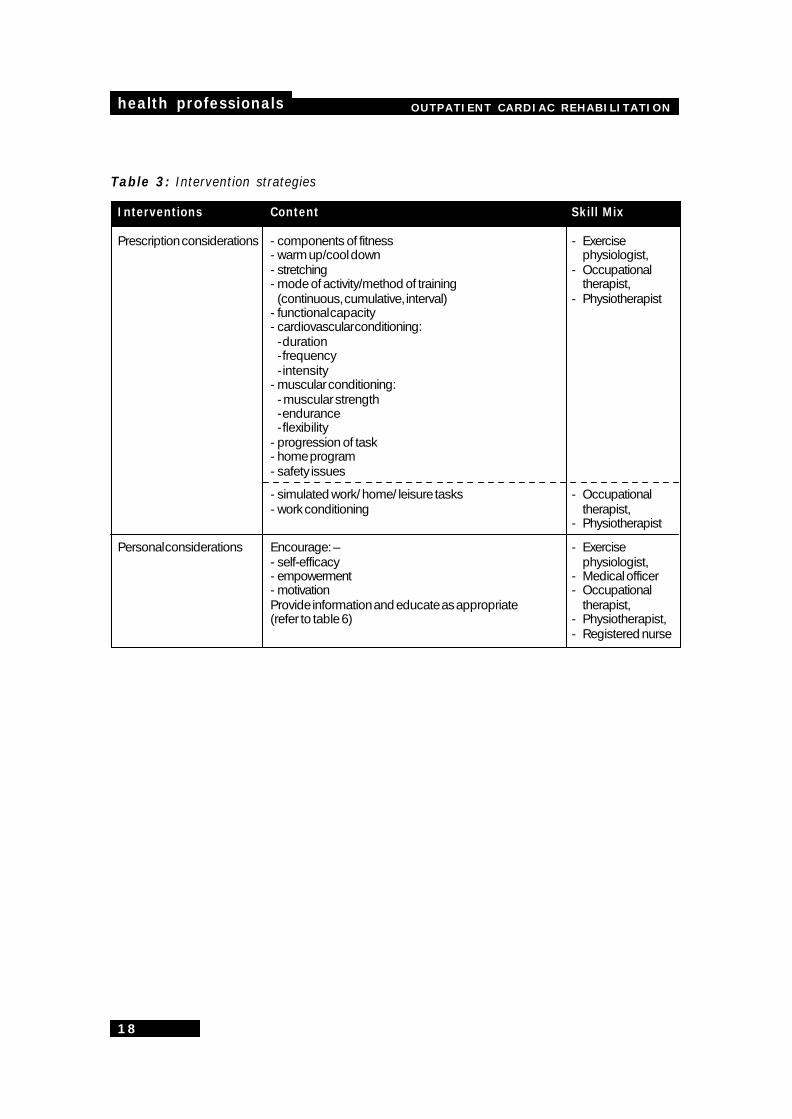
Table 3: Intervention strategies
Interventions Content Skill Mix
Prescription considerations - components of fitness - Exercise- warm up/cool down physiologist,- stretching - Occupational- mode of activity/method of training therapist,
(continuous, cumulative, interval) - Physiotherapist- functional capacity- cardiovascular conditioning:
- duration- frequency- intensity
- muscular conditioning:- muscular strength- endurance- flexibility
- progression of task- home program- safety issues
- simulated work/ home/ leisure tasks - Occupational- work conditioning therapist,
- Physiotherapist
Personal considerations Encourage:– - Exercise- self-efficacy physiologist,- empowerment - Medical officer- motivation - OccupationalProvide information and educate as appropriate therapist,(refer to table 6) - Physiotherapist,
- Registered nurse
OUTPATIENT CARDIAC REHABILITATION health professionals
19
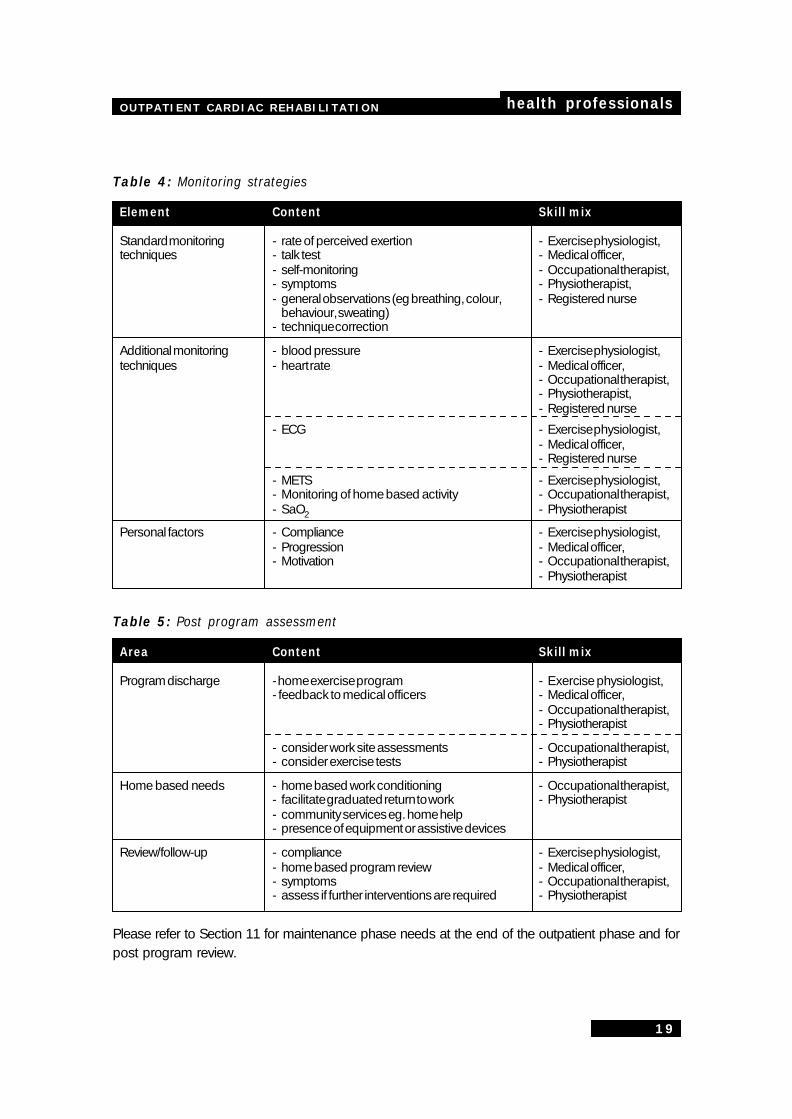
Table 4: Monitoring strategies
Element Content Skill mix
Standard monitoring - rate of perceived exertion - Exercise physiologist,techniques - talk test - Medical officer,
- self-monitoring - Occupational therapist,- symptoms - Physiotherapist,- general observations (eg breathing, colour, - Registered nurse
behaviour, sweating)- technique correction
Additional monitoring - blood pressure - Exercise physiologist,techniques - heart rate - Medical officer,
- Occupational therapist,- Physiotherapist,- Registered nurse
- ECG - Exercise physiologist,- Medical officer,- Registered nurse
- METS - Exercise physiologist,- Monitoring of home based activity - Occupational therapist,- SaO2 - Physiotherapist
Personal factors - Compliance - Exercise physiologist,- Progression - Medical officer,- Motivation - Occupational therapist,
- Physiotherapist
Table 5: Post program assessment
Area Content Skill mix
Program discharge - home exercise program - Exercise physiologist,- feedback to medical officers - Medical officer,
- Occupational therapist,- Physiotherapist
- consider work site assessments - Occupational therapist,- consider exercise tests - Physiotherapist
Home based needs - home based work conditioning - Occupational therapist,- facilitate graduated return to work - Physiotherapist- community services eg. home help- presence of equipment or assistive devices
Review/follow-up - compliance - Exercise physiologist,- home based program review - Medical officer,- symptoms - Occupational therapist,- assess if further interventions are required - Physiotherapist
Please refer to Section 11 for maintenance phase needs at the end of the outpatient phase and forpost program review.

health professionals OUTPATIENT CARDIAC REHABILITATION
20
10. Education, discussionand counselling
10.1 Importance ofeducation discussionand counsellingLevel of evidence 21,2,3,4
Cardiac rehabilitation is more than improvingphysical fitness and returning the patient towork. There is good evidence that negativeemotions and poor health behaviours arerelated to poorer health outcomes for cardiacpatients. Counselling, confidence building,education, risk factor management andsecondary prevention are also key elementsof cardiac rehabilitation.
Helping patients and families understand thecardiac condition and build skills to alter lifestylefactors that negatively impact on cardiac health,involves education, behaviour modificationtechniques and counselling1,4. Assisting patientsand their families to reduce significant levels ofnegative emotions is an essential part of cardiacrehabilitation, which will improve not just theirquality of life but also their health outcomes. Thissection of the document aims to assist healthprofessionals select appropriate interventionsbased on the patient’s needs.
10.2 EducationLevel of evidence 21,3,4,20
Education involves more than the transfer ofinformation. It is not confined to formaleducation sessions, but is an integralcomponent of physical activity and exerciseprescriptions, counselling sessions andinformal gatherings such as morning teas.Individuals can benefit from the experiencesof others in similar situations so time should
be allowed for group members to share theirexperiences either in a formal or informal way.
10.2.1 Effectiveness
To be effective, information should be presentedin a manner that enhances learning for all.
To achieve this, health professionals should:- employ adult learning principles (level of
evidence 21)- encourage group disclosure and sharing of
experiences- understand group work principles- encourage the group to generate their own
solutions to encourage ownership ofknowledge
- use theories and strategies for behaviourchange (level of evidence 21)
- tailor the education mode to suit individualneeds
- assess knowledge and learning style/preferences
- address misconceptions- establish/provide a supportive learning
environment- address knowledge, attitude, beliefs and skills
of the individual- develop client-set, client-focussed learning
objectives in collaboration with the healthprofessional
- provide written confirmation of informationprovided
- regularly conduct process, impact andoutcome evaluations
Within the group environment, healthprofessionals need to be aware of group processtheories (level of evidence 21) to assess andevaluate group dynamics and participantbehaviour and to foster a positive learningenvironment for all. It is also important to identifyclients who may require further individualintervention in a particular area.
OUTPATIENT CARDIAC REHABILITATION health professionals
21
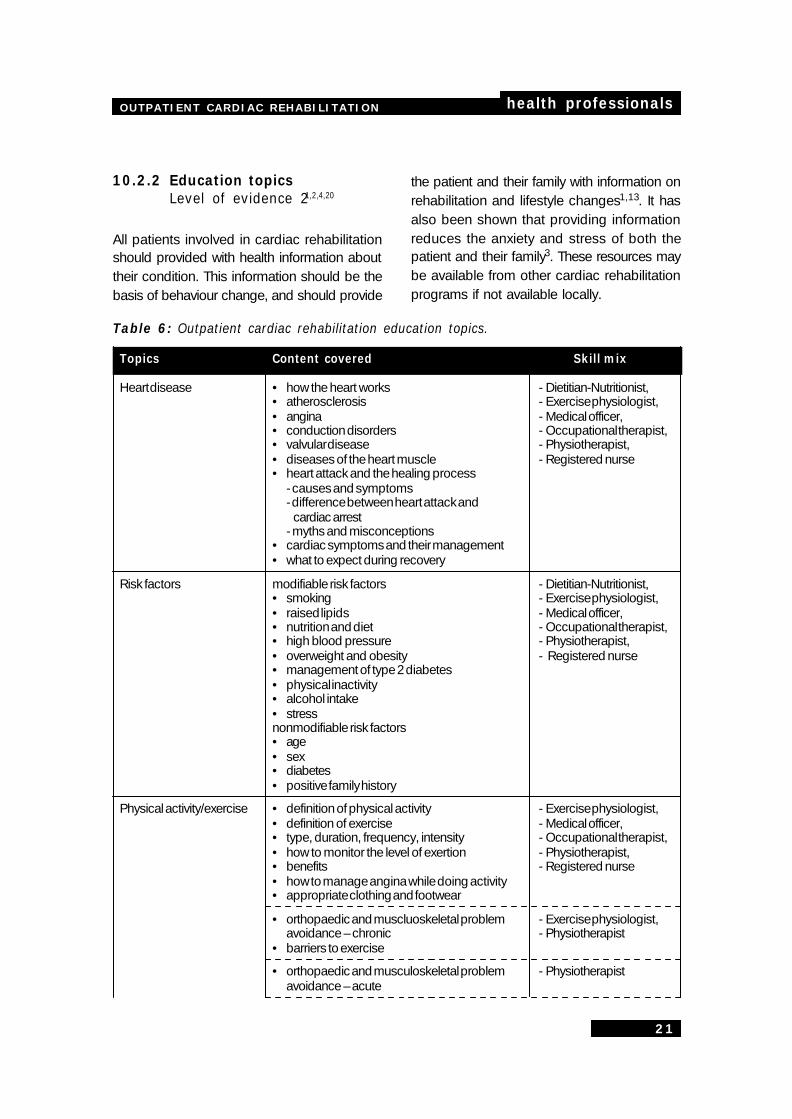
10.2.2 Education topicsLevel of evidence 21,2,4,20
All patients involved in cardiac rehabilitationshould provided with health information abouttheir condition. This information should be thebasis of behaviour change, and should provide
Table 6: Outpatient cardiac rehabilitation education topics.
Topics Content covered Skill mix
Heart disease • how the heart works - Dietitian-Nutritionist,• atherosclerosis - Exercise physiologist,• angina - Medical officer,• conduction disorders - Occupational therapist,• valvular disease - Physiotherapist,• diseases of the heart muscle - Registered nurse• heart attack and the healing process
- causes and symptoms- difference between heart attack and
cardiac arrest- myths and misconceptions
• cardiac symptoms and their management• what to expect during recovery
Risk factors modifiable risk factors - Dietitian-Nutritionist,• smoking - Exercise physiologist,• raised lipids - Medical officer,• nutrition and diet - Occupational therapist,• high blood pressure - Physiotherapist,• overweight and obesity - Registered nurse• management of type 2 diabetes• physical inactivity• alcohol intake• stressnonmodifiable risk factors• age• sex• diabetes• positive family history
Physical activity/exercise • definition of physical activity - Exercise physiologist,• definition of exercise - Medical officer,• type, duration, frequency, intensity - Occupational therapist,• how to monitor the level of exertion - Physiotherapist,• benefits - Registered nurse• how to manage angina while doing activity• appropriate clothing and footwear
• orthopaedic and muscluoskeletal problem - Exercise physiologist,avoidance – chronic - Physiotherapist
• barriers to exercise
• orthopaedic and musculoskeletal problem - Physiotherapistavoidance – acute
the patient and their family with information onrehabilitation and lifestyle changes1,13. It hasalso been shown that providing informationreduces the anxiety and stress of both thepatient and their family3. These resources maybe available from other cardiac rehabilitationprograms if not available locally.
health professionals OUTPATIENT CARDIAC REHABILITATION
22
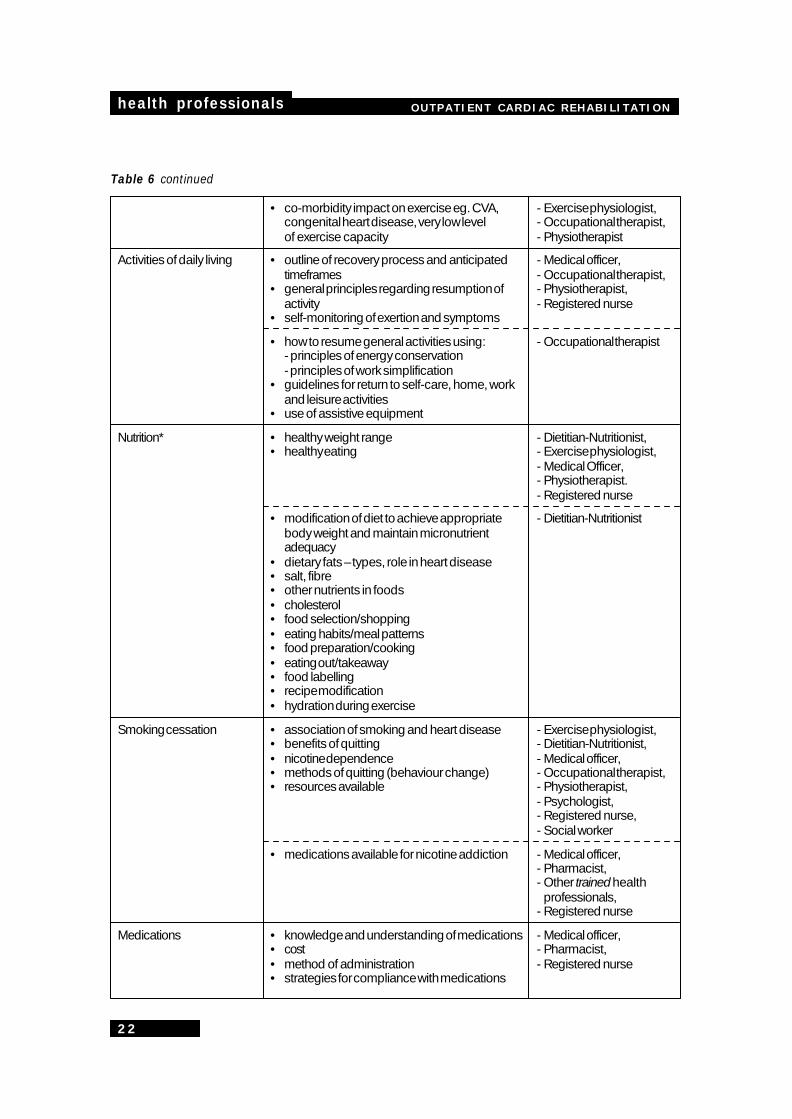
Table 6 continued
• co-morbidity impact on exercise eg. CVA, - Exercise physiologist,congenital heart disease, very low level - Occupational therapist,of exercise capacity - Physiotherapist
Activities of daily living • outline of recovery process and anticipated - Medical officer,timeframes - Occupational therapist,
• general principles regarding resumption of - Physiotherapist,activity - Registered nurse
• self-monitoring of exertion and symptoms
• how to resume general activities using: - Occupational therapist- principles of energy conservation- principles of work simplification
• guidelines for return to self-care, home, workand leisure activities
• use of assistive equipment
Nutrition* • healthy weight range - Dietitian-Nutritionist,• healthy eating - Exercise physiologist,
- Medical Officer,- Physiotherapist.- Registered nurse
• modification of diet to achieve appropriate - Dietitian-Nutritionistbody weight and maintain micronutrientadequacy
• dietary fats – types, role in heart disease• salt, fibre• other nutrients in foods• cholesterol• food selection/shopping• eating habits/meal patterns• food preparation/cooking• eating out/takeaway• food labelling• recipe modification• hydration during exercise
Smoking cessation • association of smoking and heart disease - Exercise physiologist,• benefits of quitting - Dietitian-Nutritionist,• nicotine dependence - Medical officer,• methods of quitting (behaviour change) - Occupational therapist,• resources available - Physiotherapist,
- Psychologist,- Registered nurse,- Social worker
• medications available for nicotine addiction - Medical officer,- Pharmacist,- Other trained health
professionals,- Registered nurse
Medications • knowledge and understanding of medications - Medical officer,• cost - Pharmacist,• method of administration - Registered nurse• strategies for compliance with medications
OUTPATIENT CARDIAC REHABILITATION health professionals
23
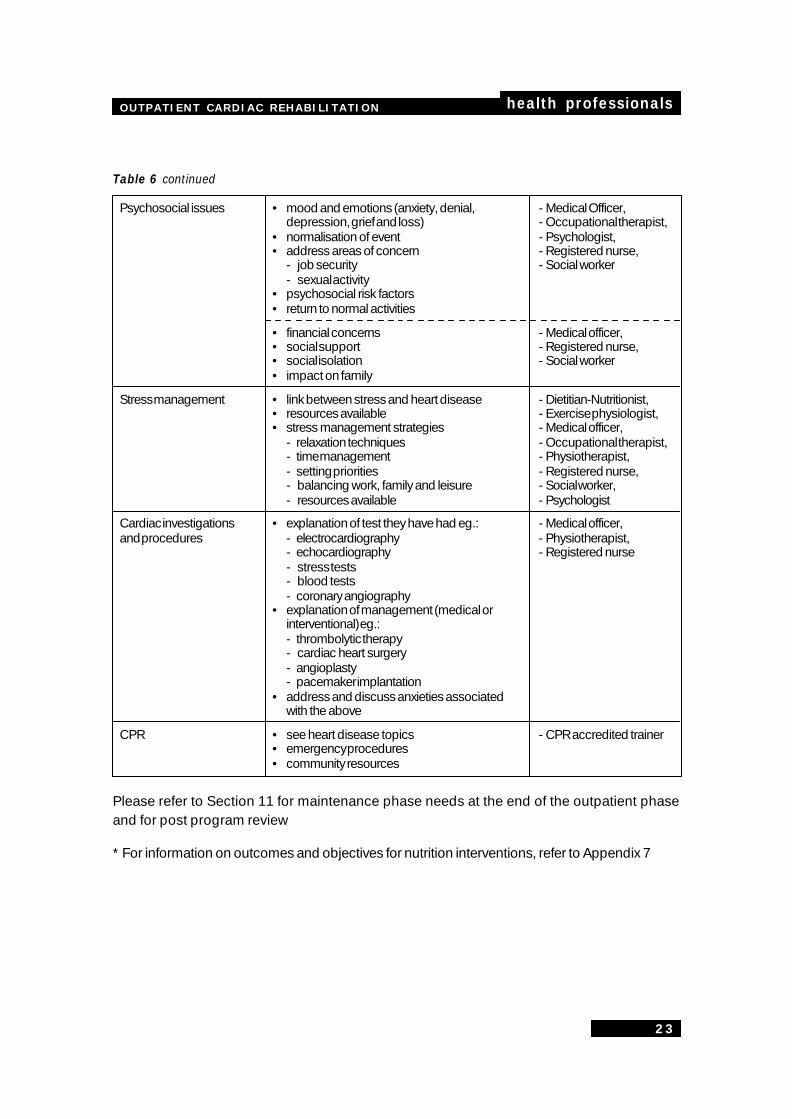
Table 6 continued
Psychosocial issues • mood and emotions (anxiety, denial, - Medical Officer,depression, grief and loss) - Occupational therapist,
• normalisation of event - Psychologist,• address areas of concern - Registered nurse,
- job security - Social worker- sexual activity
• psychosocial risk factors• return to normal activities
• financial concerns - Medical officer,• social support - Registered nurse,• social isolation - Social worker• impact on family
Stress management • link between stress and heart disease - Dietitian-Nutritionist,• resources available - Exercise physiologist,• stress management strategies - Medical officer,
- relaxation techniques - Occupational therapist,- time management - Physiotherapist,- setting priorities - Registered nurse,- balancing work, family and leisure - Social worker,- resources available - Psychologist
Cardiac investigations • explanation of test they have had eg.: - Medical officer,and procedures - electrocardiography - Physiotherapist,
- echocardiography - Registered nurse- stress tests- blood tests- coronary angiography
• explanation of management (medical orinterventional) eg.:- thrombolytic therapy- cardiac heart surgery- angioplasty- pacemaker implantation
• address and discuss anxieties associatedwith the above
CPR • see heart disease topics - CPR accredited trainer• emergency procedures• community resources
Please refer to Section 11 for maintenance phase needs at the end of the outpatient phaseand for post program review
* For information on outcomes and objectives for nutrition interventions, refer to Appendix 7
health professionals OUTPATIENT CARDIAC REHABILITATION
24
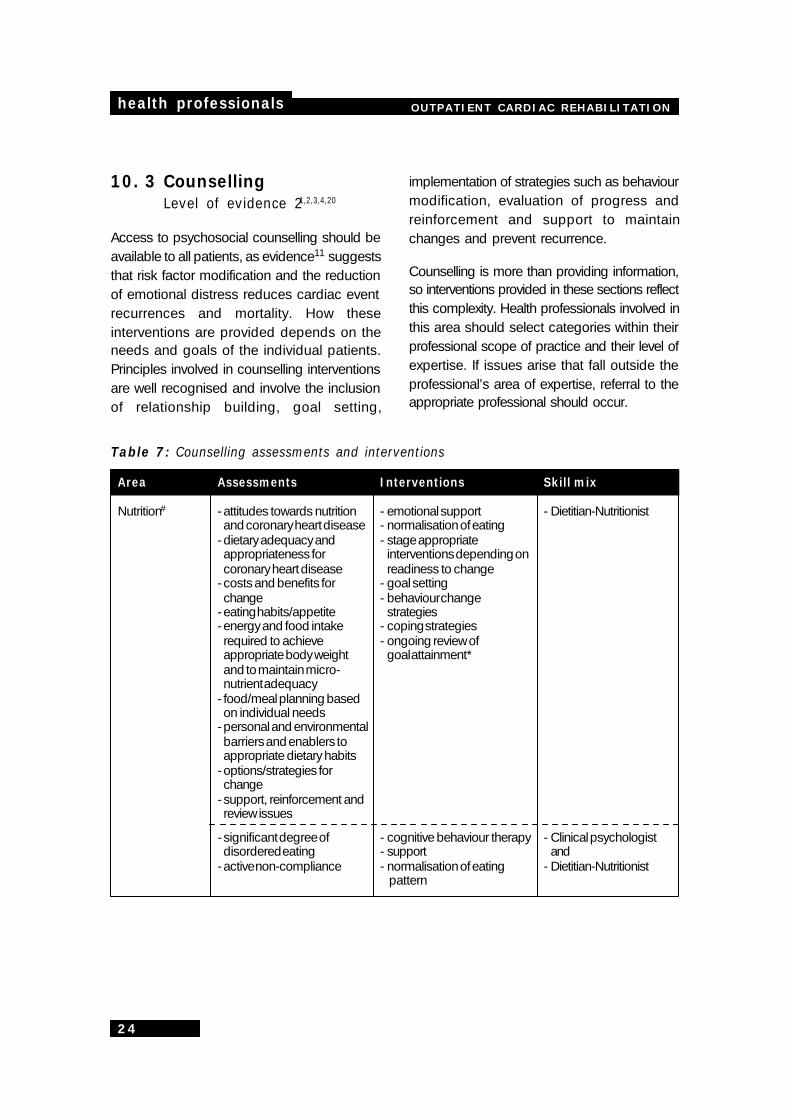
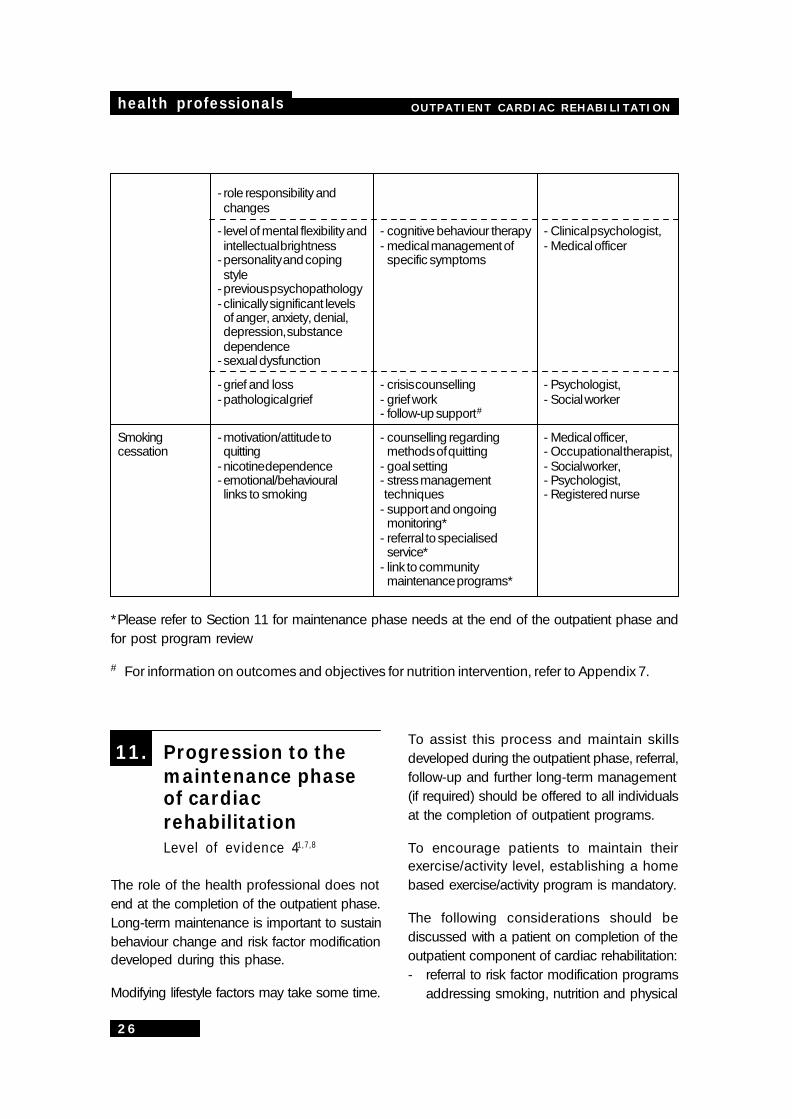
10. 3 CounsellingLevel of evidence 21,2,3,4,20
Access to psychosocial counselling should beavailable to all patients, as evidence11 suggeststhat risk factor modification and the reductionof emotional distress reduces cardiac eventrecurrences and mortality. How theseinterventions are provided depends on theneeds and goals of the individual patients.Principles involved in counselling interventionsare well recognised and involve the inclusionof relationship building, goal setting,
implementation of strategies such as behaviourmodification, evaluation of progress andreinforcement and support to maintainchanges and prevent recurrence.
Counselling is more than providing information,so interventions provided in these sections reflectthis complexity. Health professionals involved inthis area should select categories within theirprofessional scope of practice and their level ofexpertise. If issues arise that fall outside theprofessional’s area of expertise, referral to theappropriate professional should occur.
Table 7: Counselling assessments and interventions
Area Assessments Interventions Skill mix
Nutrition# - attitudes towards nutrition - emotional support - Dietitian-Nutritionistand coronary heart disease - normalisation of eating
- dietary adequacy and - stage appropriateappropriateness for interventions depending oncoronary heart disease readiness to change
- costs and benefits for - goal settingchange - behaviour change
- eating habits/appetite strategies- energy and food intake - coping strategiesrequired to achieve - ongoing review ofappropriate body weight goal attainment*and to maintain micro-nutrient adequacy
- food/meal planning basedon individual needs
- personal and environmentalbarriers and enablers toappropriate dietary habits
- options/strategies forchange
- support, reinforcement andreview issues
- significant degree of - cognitive behaviour therapy - Clinical psychologistdisordered eating - support and
- active non-compliance - normalisation of eating - Dietitian-Nutritionist pattern
OUTPATIENT CARDIAC REHABILITATION health professionals
25
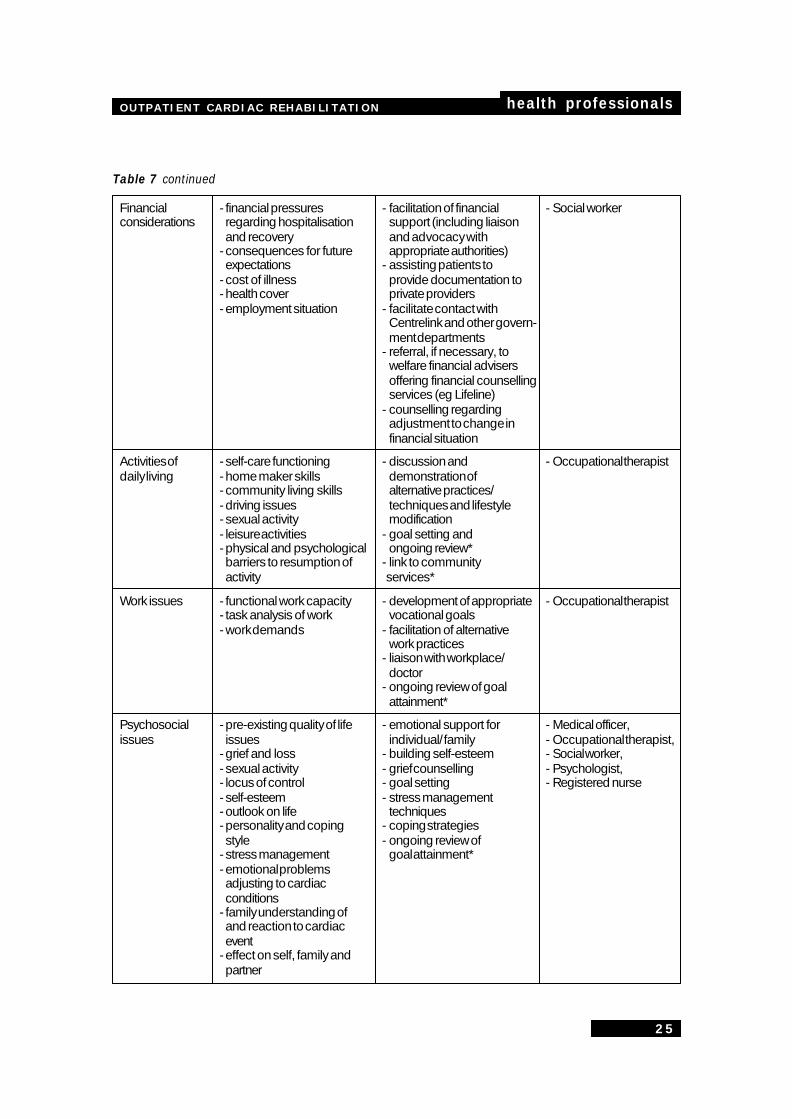
Table 7 continued
Financial - financial pressures - facilitation of financial - Social workerconsiderations regarding hospitalisation support (including liaison
and recovery and advocacy with- consequences for future appropriate authorities)expectations - assisting patients to
- cost of illness provide documentation to- health cover private providers- employment situation - facilitate contact with
Centrelink and other govern-ment departments
- referral, if necessary, towelfare financial advisersoffering financial counsellingservices (eg Lifeline)
- counselling regardingadjustment to change infinancial situation
Activities of - self-care functioning - discussion and - Occupational therapistdaily living - home maker skills demonstration of
- community living skills alternative practices/- driving issues techniques and lifestyle- sexual activity modification- leisure activities - goal setting and- physical and psychological ongoing review*barriers to resumption of - link to communityactivity services*
Work issues - functional work capacity - development of appropriate - Occupational therapist- task analysis of work vocational goals- work demands - facilitation of alternative
work practices- liaison with workplace/
doctor- ongoing review of goal
attainment*
Psychosocial - pre-existing quality of life - emotional support for - Medical officer,issues issues individual/ family - Occupational therapist,
- grief and loss - building self-esteem - Social worker,- sexual activity - grief counselling - Psychologist,- locus of control - goal setting - Registered nurse- self-esteem - stress management- outlook on life techniques- personality and coping - coping strategiesstyle - ongoing review of
- stress management goal attainment*- emotional problemsadjusting to cardiacconditions
- family understanding ofand reaction to cardiacevent
- effect on self, family andpartner
health professionals OUTPATIENT CARDIAC REHABILITATION
26
- role responsibility andchanges
- level of mental flexibility and - cognitive behaviour therapy - Clinical psychologist,intellectual brightness - medical management of - Medical officer
- personality and coping specific symptomsstyle
- previous psychopathology- clinically significant levelsof anger, anxiety, denial,depression, substancedependence
- sexual dysfunction
- grief and loss - crisis counselling - Psychologist,- pathological grief - grief work - Social worker
- follow-up support#
Smoking - motivation/attitude to - counselling regarding - Medical officer,cessation quitting methods of quitting - Occupational therapist,
- nicotine dependence - goal setting - Social worker,- emotional/behavioural - stress management - Psychologist,links to smoking techniques - Registered nurse
- support and ongoingmonitoring*
- referral to specialisedservice*
- link to communitymaintenance programs*
*Please refer to Section 11 for maintenance phase needs at the end of the outpatient phase andfor post program review
# For information on outcomes and objectives for nutrition intervention, refer to Appendix 7.
11. Progression to themaintenance phaseof cardiacrehabilitationLevel of evidence 41,7,8
The role of the health professional does notend at the completion of the outpatient phase.Long-term maintenance is important to sustainbehaviour change and risk factor modificationdeveloped during this phase.
Modifying lifestyle factors may take some time.
To assist this process and maintain skillsdeveloped during the outpatient phase, referral,follow-up and further long-term management(if required) should be offered to all individualsat the completion of outpatient programs.
To encourage patients to maintain theirexercise/activity level, establishing a homebased exercise/activity program is mandatory.
The following considerations should bediscussed with a patient on completion of theoutpatient component of cardiac rehabilitation:- referral to risk factor modification programs
addressing smoking, nutrition and physical
OUTPATIENT CARDIAC REHABILITATION health professionals
27
activity- identification of support groups and other
resources in the community- access to education and discussion
sessions as necessary6
- home and/or community based programsto maintain exercise and physical activity
- the necessity of long term management bycardiac rehabilitation team members orother health professionals
- referral to other health professionals (asnecessary)
- regular follow-up and review by cardiacrehabilitation team members
- referral back to the patients’ generalpractitioners (GPs) for regular monitoring bythe GP or other medical specialist
11.1 Ongoing maintenance
As general practitioners and medicalspecialists are involved in the ongoingmanagement of the patient, healthprofessionals involved in outpatientrehabilitation should consult with the treatingphysician regarding the patient.
Formal communication should occur betweencardiac rehabilitation team members and theindividual patient’s general practitioner andmedical specialists throughout the outpatientphase and at the completion of this phase ofthe rehabilitation process. This communicationaids in the transfer of information and informsphysicians of the need for ongoing interventionand/or assistance in specific areas of thecardiac rehabilitation process.
Glossary
Activities of daily livingexertion required to perform normal life tasks
BMI – body mass indexmathematical measurement used todetermine the relationship between heightand weight as a measurement of body mass.
CHDcoronary heart disease
ECGelectro-cardiogram – measurement of theelectronic signals of the heart
HDL Cholesterolhigh density lipoprotein cholesterol –commonly referred to as the “good”cholesterol as it reduces fatty deposits(atheroma) in arteries
LDL Cholesterollow density lipoprotein cholesterol –commonly referred to as the “bad”cholesterol. Too much LDL in the blood canclog the arteries (atherosclerosis)
LDL/HDL ratiomeasurement between the “bad” and the“good” fats present in the bloodstream –used to determine risk for heart disease andmonitor the effectiveness of treatments
METmetabolic equivalent – a measure of oxygenthrough the lungs
Rate of perceived exertionphysical activity self assessment tool used toindicate the level of exertion as perceived bythe individual
SaO2percentage of haemoglobin molecules thatare carrying oxygen molecules
health professionals OUTPATIENT CARDIAC REHABILITATION
28
References
1. NSW Health Department (1997). NSWPolicy Standards for CardiacRehabilitation. NSW Health Department.
2. Goble, A.J. and Worcester, M.U.C.(1999). Best Practice Guidelines forCardiac Rehabilitation and SecondaryPrevention. Heart Research Centre.Melbourne, on behalf of Department ofHuman Services Victoria.
3. Wegner NK, Froelicher ES, Smith LK, et.al. (1995). Cardiac Rehabilitation asSecondary Prevention. Clinical PracticeGuideline. Quick Reference Guide forClinicians, No. 17. Rockville, MD: U.S.Department of Health and Humanservices, Public Health Service, Agencyfor Health Care Policy and Researchand National Heart, Lung and BloodInstitute. AHCPR Pub. No. 96-0673.
4. NHS centre for Reviews andDissemination. University of York (1998).Cardiac Rehabilitation. Effective HealthCare 4(4):1-12.
5. National Health and Medical ResearchCouncil of Australia (1995). Quality ofCare and Health Outcomes Committee:Guidelines for the development ofclinical practice guidelines. Canberra:Australian Government PublishingService, 1995.
6. Goble and Worcester (1999) BestPractice Guidelines for CardiacRehabilitation and SecondaryPrevention: A synopsis. Heart ReseachCentre. Melbourne, on behalf of theDepartment of Human Services Victoria.
7. National Cardiac Rehabilitation AdvisoryCommittee of the Heart Foundation(1998). Recommendations for CardiacRehabilitation 1998. Heart Foundation.
8. Australian Cardiac RehabilitationAssociation (1999). A practitioner’sGuide to Cardiac Rehabilitation. RenardMarketing.
9. World Health Organisation ExpertCommittee (1993). Rehabilitation aftercardiovascular diseases, with specialemphasis on developing countries.Technical report series number 831.Geneva: World Health Organisation.
10. North Queensland Rural Health TrainingUnit (1999). “Course in CardiacRehabilitation and SecondaryPrevention for Indigenous HealthWorkers”. Vocational Education, Trainingand Employment Commission.
11. Dinnes, J., Kleijnen, J. et. al. (1999).Cardiac rehabilitation. Quality in HealthCare. 8: 65-71.
12. Queensland Health (1999). Draft – HealthOutcomes Plan for Cardiovascular Health:Coronary Heart Disease in Queensland2000 – 2004. Queensland Health
13. Queensland Cardiac RehabilitationAssociation and Heart Foundation ofAustralia (Qld) (1999). Minimum DataSet for Cardiac Rehabilitation andSecondary Prevention.
14. Heart Foundation of Australia (Qld)(1999). Physical Activity for People withHeart Disease. Heart Foundation ofAustralia
OUTPATIENT CARDIAC REHABILITATION health professionals
29
15. American College of Sports Medicine(2000). Guidelines for Exercise Testingand Programming. 6th Edition. Lea andFebiger, London.
16. University of Western Australia and theCentre for Health Promotion andResearch, Sydney (1999). NationalPhysical Activity Guidelines forAustralians. Commonwealth Departmentof Health and Aged Care.
17. Department of Health and HumanServices (1996). Physical activity andhealth: a report of the US SurgeonGeneral. National Centres for DiseaseControl. Atlanta, Georgia.
18. The Heart Foundation National PhysicalActivity Program Committee (2000). Aposition paper – Physical Activity Policyand Recommendations. HeartFoundation of Australia.
19. Anderson, R.E., et. al. (1999). Effects oflifestyle activities vs. structured aerobicexercise in obese women: a randomisedtrial. Journal of the American MedicalAssociation. 281:335-340.
20. Dusseldorp, E., et. al. (1999). A Meta-Analysis of Psychoeducational Programsfor Coronary Heart Disease Patients.Health Psychology 18(5):506-519.
21. Houston Miller, N et. al. (1990). Positionpaper of the American Association ofCardiovascular and PulmonaryRehabilitation. The efficacy of risk factorintervention and psychosoical aspects ofcardiac rehabilitation. Journal ofCardiopulmonary Rehabilitation. 10:198-209.
22. Fraser-Smith, N., Lesperance, F., Talajic,M. (1993). Depression following
myocardial infarction: impact on 6month survival. Journal of the AmericanMedical Association. 270: 1819-1825
23 Barefoot, J.C., Helms, M.J., Mark, D.B.,Bluementhal, J.A., Califf, R.M., Haney,T.L., O’Connor, C.M., Siegler, I.C., &Willliams, R.B. (1996). Depression andlong-term mortality risk in patients withcoronary artery disease. AmericanJournal of Cardiology 78: 613-617.
24 Kawachi, I., Sparrow, D., Vokonas, P.S.,& Weiss, S.T. (1994). Symptoms ofanxiety and risk of coronary disease.Circulation 90: 2225-2229.
25 Beck AT, Ward CH, Mendelson M, MockJ, Erbaugh J (1961). An inventory formeasuring depression. Archives ofGeneral Psychiatry. 4: 561-571.
26 Hare D.L. (1996). Cardiac DepressionScale Validation. Journal ofPsychosomatic Research 40:379-386.
27 Zung W.W.K. (1965). A self-ratingdepression scale. Archives of GeneralPsychiatry. 12: 63-70.
28 Zigmond, A.S., & Snaith, R.P. (1983). TheHospital Anxiety Depression Scale. ActaPsychiatrica Scandinavica 67:361-370.
29 Speilberger, CD (1996). State Tray AngerExpression Inventory (STAXI).Professional Manual of PsychologyAssocation Resource Inc.
30 Cook, W.W and Medley, D.N. (1994).Proposed Post and Tharisaic-virtueScales for the MMP. Journal of AppliedPsychology 38:444-448.
31 Saunders, J.B. et. al. (1993).Development of the Alcohol Use
health professionals OUTPATIENT CARDIAC REHABILITATION
30
Disorders Identification Test (AUDIT):WHO collaborative project on earlydetection of persons with harmfulalcohol consumption – II. Addiction88:791-904.
32 Heatherton, T.F. et. al. (1991). TheFagerstrom Test for NicotineDependence: a Revision of theFagerstrom Tolerance questionnaire.British Journal of Addiction 86:1118-1127.
33 Borg, G.A. (1982). Psychophysicalbases for perceived exertion. MedicalScience of Sports Exercise. 14:377-387.
34 Queensland Health (2000). BestPractice Guidelines for the Managementof Type 2 Diabetes for Dietitians.Queensland Health.
35 National Heart Foundation (1999). Draft-Guide to risk reduction for patients with/or ‘At Risk’ of cardiovascular disease.Heart Foundation of Australia.
36 Expert Panel on the Identification,Evaluation and Treatment of Overweightin Adults (1998). Clinical Guidelines onthe Identyification, Evaluation andTreatment of Overweight and Obesity inAdults: Executive Summary. AmericanJournal of Clinical Nutrition 68:899-917.
OUTPATIENT CARDIAC REHABILITATION health professionals
31
Appendix 1Further information
Sources of detailed information which mayprovide background information on elements ofcardiac rehabilitation.
Evidence based informationregarding cardiac rehabilitation
- Goble, A.J. and Worcester, M.U.C. (1999).Best Practice Guidelines for CardiacRehabilitation and Secondary Prevention.Heart Research Centre. Melbourne, on behalfof Department of Human Services Victoria.
- NSW Health Department (1997). NSW PolicyStandards for Cardiac Rehabilitation. NSWHealth Department
Recommendations for cardiacrehabilitation programs
- National Cardiac Rehabilitation AdvisoryCommittee of the Heart Foundation (1998).
Recommendations for Cardiac Rehabilitation1998. Heart Foundation.
- Heart Foundation of Australia (1997). Howto Plan a Cardiac Rehabilitation Program.Heart Foundation of Australia (NSWDivision)
Components of cardiac rehabilitation
- Australian Cardiac Rehabilitation Association.(1999). A Practitioner’s Guide to CardiacRehabilitation. Renard Marketing.
- Heart Foundation (1999). All about hearthealth. Promoting Heart Health: Aneducational resource manual for rural andremote health workers. Heart Foundation.
- American College of Sports Medicine. (2000).Guidelines for Exercise Testing andPrescription. 6th Edition. Lea and Febiger,London.
health professionals OUTPATIENT CARDIAC REHABILITATION
32
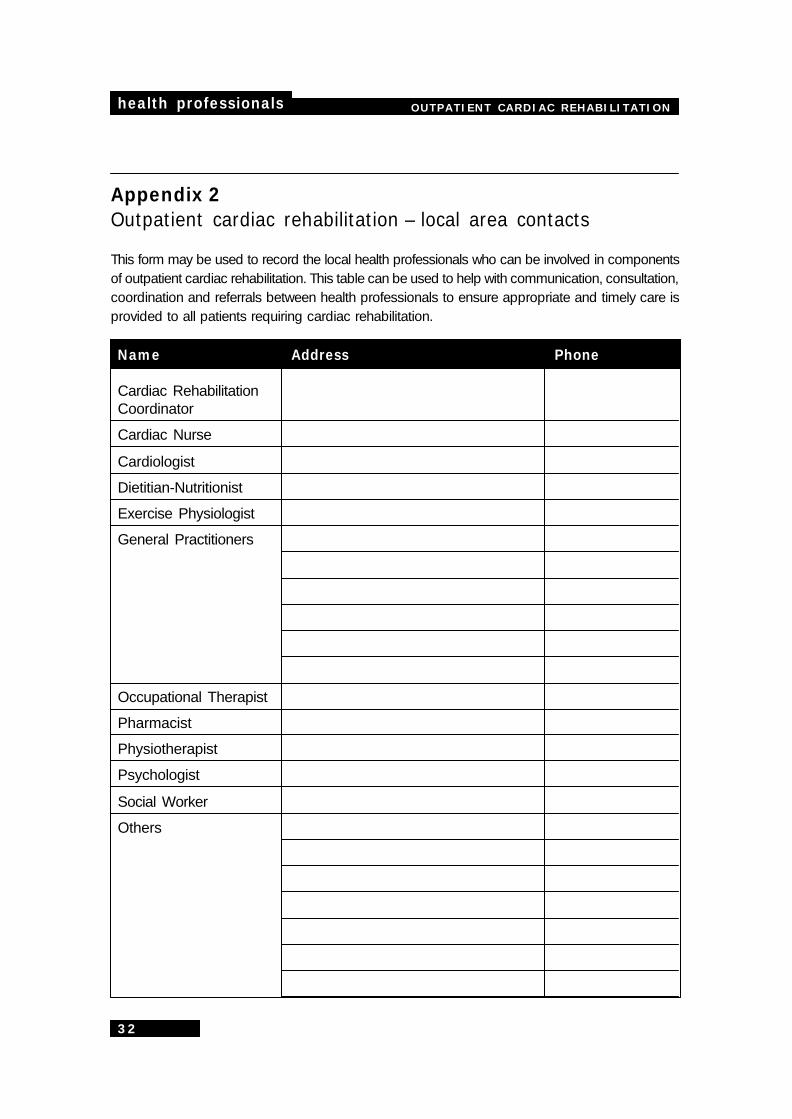
Appendix 2Outpatient cardiac rehabilitation – local area contacts
This form may be used to record the local health professionals who can be involved in componentsof outpatient cardiac rehabilitation. This table can be used to help with communication, consultation,coordination and referrals between health professionals to ensure appropriate and timely care isprovided to all patients requiring cardiac rehabilitation.
Name Address Phone
Cardiac RehabilitationCoordinator
Cardiac Nurse
Cardiologist
Dietitian-Nutritionist
Exercise Physiologist
General Practitioners
Occupational Therapist
Pharmacist
Physiotherapist
Psychologist
Social Worker
Others
OUTPATIENT CARDIAC REHABILITATION health professionals
33
Appendix 3Minimum data set collectionstandards
[Reproduced with permission from theQueensland Cardiac Rehabilitation Assoc-iation and Heart Foundation of Australia(Queensland)13]
The following document standardises datacollection for the minimum data set and contains28 compulsory items and one additional(optional) item. These are:
1. date of birth2. gender3. postcode4. suburb5. country of origin6. social support7. principal diagnosis8. second diagnosis9. medications
10. date of event11. phase 1 cardiac rehabilitation12. date commenced phase 2 cardiac
rehabilitation program13. phase 2 completed
14. date commenced phase 3 cardiacrehabilitation program
15. referral method16. reasons for non attendance17. family history18. comorbidities19. diabetes20. smoking21. lipid profile22. blood pressure23. body composition (BMI, waist to hip ratio)24. physical activity25. hospital readmission/re-event26. return to work27. employment status28. return to normal activityAdditional Items29. SF-36
Please contact the Queensland CardiacRehabilitation Association or the HeartFoundation of Australia (Queensland Branch)for a copy of the collection sheet and standardsfor this list.
health professionals OUTPATIENT CARDIAC REHABILITATION
34
Appendix 4Screening tools
After a cardiac event, psychosocial issues mayarise which, if not addressed, can prolong oraffect recovery. Screening tools should be usedand, if significant results found, referral forfurther long-term management by trainedhealth professionals should be offered21.Consultation with appropriate healthprofessionals should occur if information on theuse and interpretation of these tools is required.
Screening for depression andanxietyLevel of evidence 120
A meta-analyis by Dusseldorp and others20
demonstrates that anxiety and depression havea big impact on the onset and progression ofcoronary artery disease.
Several studies22,23 have shown that significantdepression is a predictor of increased risk ofcardiac death and that anxiety levels can alsoaffect an increase in the risk of a cardiacevent24.
Individuals with clinically significant levels ofdepression or anxiety should be referred tospecifically trained health professionals (levelof evidence 21).
Depression- Beck Depression Inventory25
- Cardiac Depression Scale26
- Zung Self-rating Depression Scale27
- Hospital Anxiety and Depression Scale28
Anxiety- State Anxiety Inventory29
Other screening tools
Anger and hostility- Speilberger Anger and Hostility Scale
(STAXI)29
- Cook and Medley Scale30
Substance use- Alcohol Use Disorder Identification Test
(AUDIT)31
SmokingThe Fagerstrom Nicotine Tolerance Scale32
OUTPATIENT CARDIAC REHABILITATION health professionals
35
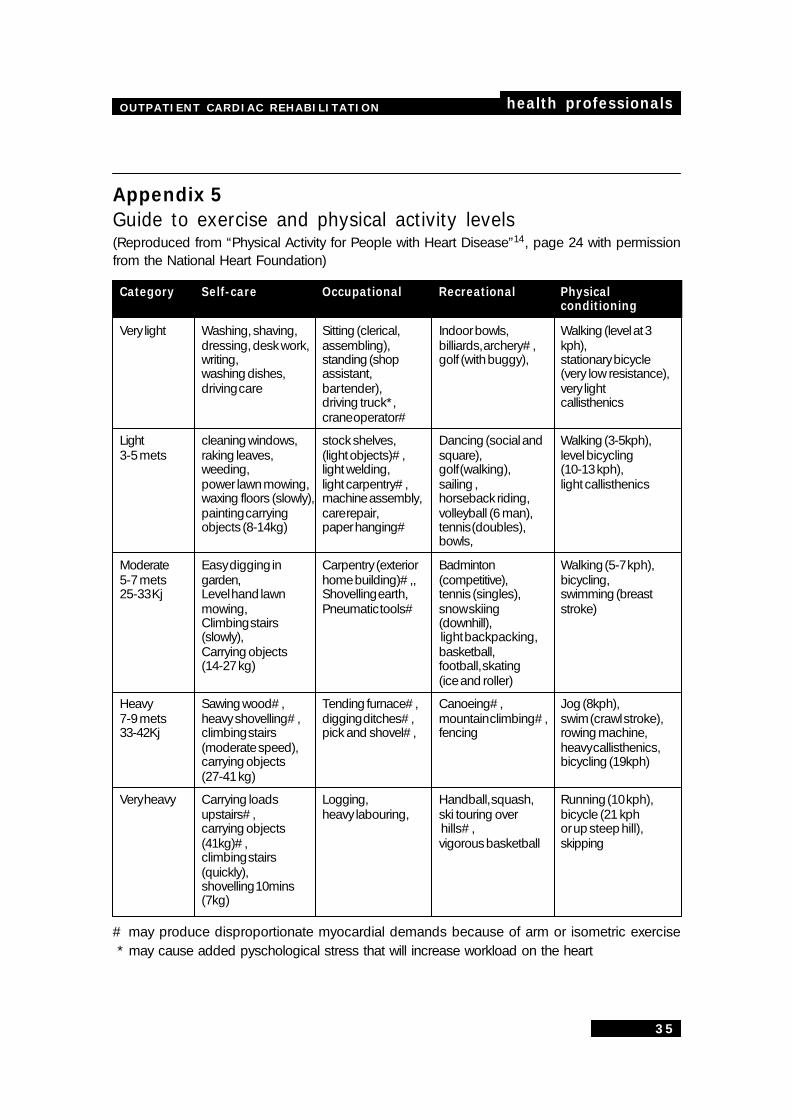
Appendix 5Guide to exercise and physical activity levels(Reproduced from “Physical Activity for People with Heart Disease”14, page 24 with permissionfrom the National Heart Foundation)
Category Self-care Occupational Recreational Physicalconditioning
Very light Washing, shaving, Sitting (clerical, Indoor bowls, Walking (level at 3dressing, desk work, assembling), billiards, archery#, kph),writing, standing (shop golf (with buggy), stationary bicyclewashing dishes, assistant, (very low resistance),driving care bar tender), very light
driving truck*, callisthenicscrane operator#
Light cleaning windows, stock shelves, Dancing (social and Walking (3-5kph),3-5 mets raking leaves, (light objects)#, square), level bicycling
weeding, light welding, golf (walking), (10-13 kph),power lawn mowing, light carpentry#, sailing , light callisthenicswaxing floors (slowly), machine assembly, horseback riding,painting carrying care repair, volleyball (6 man),objects (8-14kg) paper hanging# tennis (doubles),
bowls,
Moderate Easy digging in Carpentry (exterior Badminton Walking (5-7 kph),5-7 mets garden, home building)#,, (competitive), bicycling,25-33 Kj Level hand lawn Shovelling earth, tennis (singles), swimming (breast
mowing, Pneumatic tools# snow skiing stroke)Climbing stairs (downhill),(slowly), light backpacking,Carrying objects basketball,(14-27 kg) football, skating
(ice and roller)
Heavy Sawing wood#, Tending furnace#, Canoeing#, Jog (8kph),7-9 mets heavy shovelling#, digging ditches#, mountain climbing#, swim (crawl stroke),33-42Kj climbing stairs pick and shovel#, fencing rowing machine,
(moderate speed), heavy callisthenics,carrying objects bicycling (19kph)(27-41 kg)
Very heavy Carrying loads Logging, Handball, squash, Running (10 kph),upstairs#, heavy labouring, ski touring over bicycle (21 kphcarrying objects hills#, or up steep hill),(41kg)#, vigorous basketball skippingclimbing stairs(quickly),shovelling 10mins(7kg)
# may produce disproportionate myocardial demands because of arm or isometric exercise * may cause added pyschological stress that will increase workload on the heart
health professionals OUTPATIENT CARDIAC REHABILITATION
36
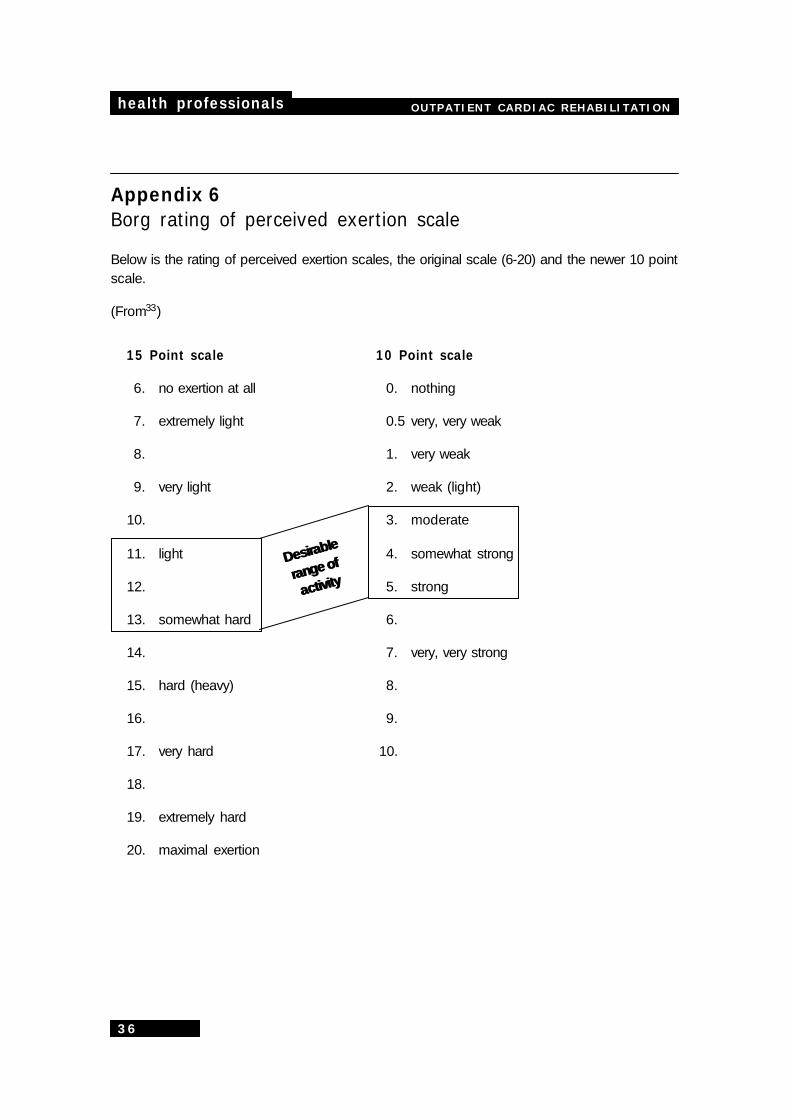
Appendix 6Borg rating of perceived exertion scale
Below is the rating of perceived exertion scales, the original scale (6-20) and the newer 10 pointscale.
(From33)
DesirableDesirable
range ofrange of
activityactivity
15 Point scale 10 Point scale
6. no exertion at all 0. nothing
7. extremely light 0.5 very, very weak
8. 1. very weak
9. very light 2. weak (light)
10. 3. moderate
11. light 4. somewhat strong
12. 5. strong
13. somewhat hard 6.
14. 7. very, very strong
15. hard (heavy) 8.
16. 9.
17. very hard 10.
18.
19. extremely hard
20. maximal exertion
OUTPATIENT CARDIAC REHABILITATION health professionals
37
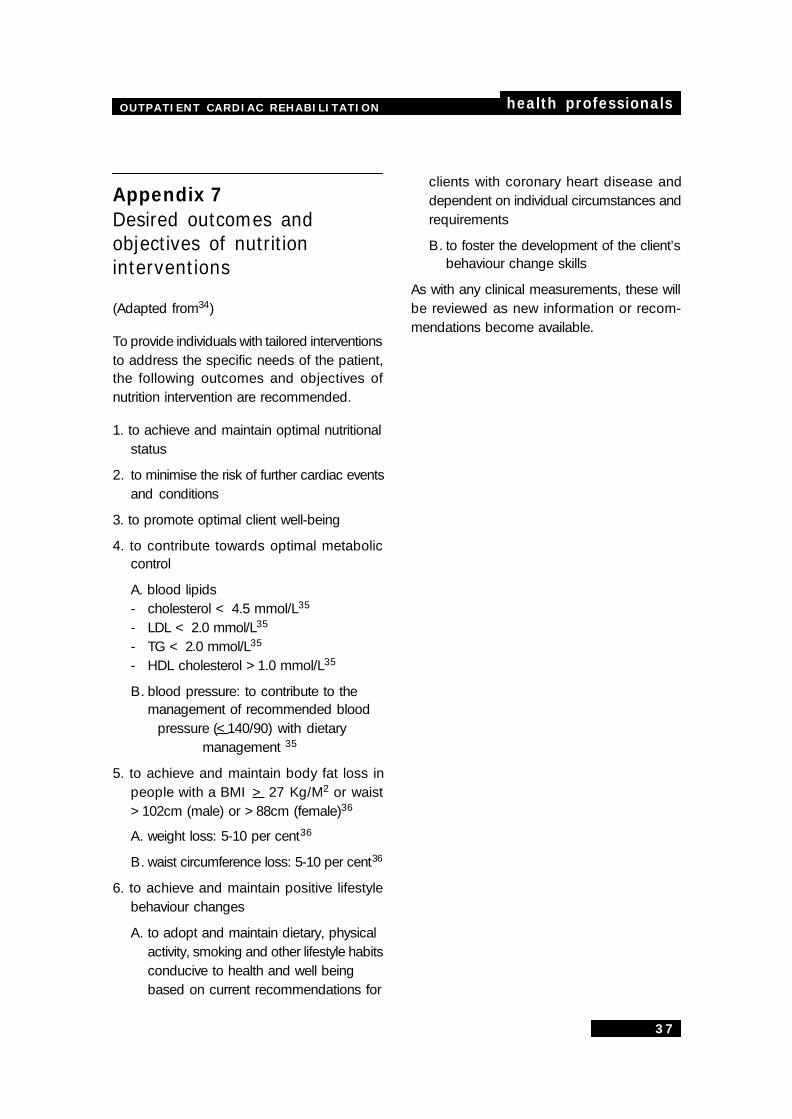
Appendix 7Desired outcomes andobjectives of nutritioninterventions
(Adapted from34)
To provide individuals with tailored interventionsto address the specific needs of the patient,the following outcomes and objectives ofnutrition intervention are recommended.
1. to achieve and maintain optimal nutritionalstatus
2. to minimise the risk of further cardiac eventsand conditions
3. to promote optimal client well-being
4. to contribute towards optimal metaboliccontrol
A. blood lipids- cholesterol < 4.5 mmol/L35
- LDL < 2.0 mmol/L35
- TG < 2.0 mmol/L35
- HDL cholesterol >1.0 mmol/L35
B. blood pressure: to contribute to themanagement of recommended blood
pressure (<140/90) with dietarymanagement 35
5. to achieve and maintain body fat loss inpeople with a BMI > 27 Kg/M2 or waist>102cm (male) or >88cm (female)36
A. weight loss: 5-10 per cent36
B. waist circumference loss: 5-10 per cent36
6. to achieve and maintain positive lifestylebehaviour changes
A. to adopt and maintain dietary, physicalactivity, smoking and other lifestyle habitsconducive to health and well beingbased on current recommendations for
clients with coronary heart disease anddependent on individual circumstances andrequirements
B. to foster the development of the client’sbehaviour change skills
As with any clinical measurements, these willbe reviewed as new information or recom-mendations become available.