

DOI: 10.1542/peds.2010-0941; originally published online February 15, 2010; 2010;125;e651PediatricsMarjolein Y. Berger
Leo A. A. Spee, Marieke B. Madderom, Maaike Pijpers, Yvonne van Leeuwen andChildren
and Gastrointestinal Symptoms inHelicobacter pyloriAssociation Between
http://pediatrics.aappublications.org/content/125/3/e651.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Association Between Helicobacter pylori andGastrointestinal Symptoms in Children
abstractOBJECTIVE: Recurrent abdominal pain (RAP) and other gastrointesti-nal (GI) symptoms are common complaints among children. The role ofHelicobacter pylori in the cause of these complaints remains contro-versial. Nevertheless, there is an increasing pressure on primary careclinicians to screen for H pylori infection in symptomatic children. Wesystematically reviewed the published evidence for an association be-tween H pylori infection and GI symptoms in children.
METHODS: Medline and Embase databases up to July 2009 weresearched to identify studies that evaluated the association betweenH pylori and GI symptoms in children aged up to 18 years. When studiesreported on abdominal pain without additional definition, thus notfulfilling Apley’s criteria, we grouped these outcomes as unspecifiedabdominal pain (UAP). Methodologic quality was scored by using astandardized list of criteria, and crude odds ratios (ORs) with 95%confidence intervals (CIs) were calculated and pooled.
RESULTS: Thirty-eight studies met our inclusion criteria: 23 case-control studies, 14 cross-sectional studies, and 1 prospective cohortstudy. The overall methodologic quality was low. Pooled ORs for theassociation between RAP and H pylori infection in children were 1.21(95% CI: 0.82–1.78) in 12 case-control studies and 1.00 (95% CI: 0.76–1.31) in 7 cross-sectional studies. Meta-analysis of the association be-tween UAP and H pylori infection in 6 hospital-based studies resulted ina pooled OR of 2.87 (95% CI: 1.62–5.09) compared with 0.99 (95% CI:0.46–2.11) in 5 population-based studies. Two of 3 studies concerningepigastric pain reported a statistically significant positive associationwith H pylori infection.
CONCLUSIONS: We found no association between RAP and H pyloriinfection in children and conflicting evidence for an association be-tween epigastric pain and H pylori infection. We found evidence for anassociation between UAP but could not confirm this finding in childrenseen in primary care. Pediatrics 2010;125:e651–e669
AUTHORS: Leo A. A. Spee, MD, Marieke B. Madderom,MSc, Maaike Pijpers, MD, Yvonne van Leeuwen, PhD, andMarjolein Y. Berger, MD, PhD
Department of General Practice, Erasmus MedicalCenter–University Medical Center, Rotterdam, Netherlands
KEY WORDSHelicobacter pylori, signs and symptoms, digestive, meta-analysis, review
ABBREVIATIONSGI—gastrointestinalRAP—recurrent abdominal painOR—odds ratioCI—confidence intervalUAP—unspecified abdominal painSRAP—short-term recurrent abdominal painGP—general practitioner
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0941
doi:10.1542/peds.2010-0941
Accepted for publication Oct 21, 2009
Address correspondence to Marjolein Y. Berger, MD, PhD,Erasmus MC, Department of General Practice, PO Box 2040, 3000CA Rotterdam, Netherlands. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e651 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Helicobacter pylori is 1 of the mostcommon bacterial pathogens in hu-mans and affects�50% of the world’spopulation.1 The prevalence of H pyloriinfection varies greatly between devel-oping countries and developed coun-tries (respectively, 90% vs 40% at theage of 40),1 and infection is mainly ac-quired in early childhood.2 In adults,H pylori infection is associated withconditions such as chronic active gas-tritis and peptic ulcer disease,1 andH pylori has been confirmed as themost important risk factor for non-cardia gastric adenocarcinomas andgastric mucosa-associated lymphoidtissue lymphomas.3 Despite this knowl-edge, the natural history of H pyloriinfection in children, such as the modeof acquisition and signs of infection, ispoorly understood.
Guidelines on screening for H pyloriin children contradict. Recommenda-tions vary from no need to screen chil-dren with gastrointestinal (GI) symp-toms4 and no need to screen childrenwith recurrent abdominal pain (RAP)5
to all children with upper GI symptomsshould be tested for H pylori infection(Maastricht III).6 These recommenda-tions are based on the lack of proofthat infection with H pylori is a signifi-cant cause of GI symptoms.
In addition, nowadays, a lot of diagnos-tic tests for H pylori are available.Some of them, such as the 13C-ureabreath test, detection of H pylori anti-gen in stool, and detection of specificantibodies in serum,7 are suitable foruse in primary care. Thus, this in-creased availability is likely to result inincreased number of children to betested. This emphasizes the need forup-to-date guidelines with indicationsfor investigating and treating childrenfor H pylori infection.
Good-quality studies, preferably sum-marized in a systematic review, formthe basis for evidence-based screen-ing guidelines. Previous reviews8,9 re-
garding this topic were limited to theassociation between H pylori and spe-cific symptoms, such as RAP. Becauseof the limitations of previous system-atic reviews and the several studiespublished after the publication of theseanalyses, we performed a new system-atic literature review to review sys-tematically the extent and the qualityof the current published evidence for arelationship between GI symptoms andH pylori infection in children.
METHODS
To identify relevant publications, weperformed a Medline database searchfrom 1966 to July 27, 2009, by using thefollowing key words: “Helicobacter py-lori,” “Campylobacter pylori,” “abdo-minal pain,” and “dyspepsia.” A searchstrategy for follow-up studies recom-mended by Altman10 was added. TheEmbase database was searched from1980 to July 27, 2009; the search strat-egy for Medline was adapted for Em-base with the assistance of a librarian(Appendix 1). To identify additionalpotentially relevant publications, wehand searched the reference lists ofincluded studies, of published reviewarticles, and of articles written by ex-perts in the field. No language restric-tion was used.
Study Selection
We limited our search to studies thatcompared children who did havesymptoms with children who did nothave symptoms. All abstracts ofidentified articles were screened foreligibility, and decisions regarding in-clusion of studies were made indepen-dently by 2 reviewers (L.A.A.S. andM.B.M. or Y.vL.). We used 4 criteria toselect relevant studies: (1) the studyhad a case-control, cross-sectional, orprospective cohort design; (2) 1 of itsaims was to evaluate the associationbetweenH pylori infection and GI symp-toms; (3) the study group included chil-dren aged 0 to 18 years; and (4) at least
30 children were included and sepa-rately analyzed. Because of an in-creased risk for acquiring an H pyloriinfection, studies concerning exclu-sively childrenwith relevant comorbid-ity such as mental disabilities, immu-nodeficient disorders, and diabeteswere excluded.
Interobserver reliability of the eligibil-ity screening was calculated with Co-hen’s �.11 Any disagreements betweenboth reviewers were resolved throughconsensus or by arbitration of a thirdperson (M.B.M. or Y.vL.). Full-text arti-cles of all selected titles were re-trieved or in case the abstract gave in-sufficient information on the inclusioncriteria. When an included study or thedata of a study were not available, firstauthors were contacted.
Quality Assessment
To rate the risk for bias of the includedstudies, we scored 9 identical method-ologic criteria with 1 additional crite-rion for case-control/cross-sectionalstudies and 2 additional criteria forprospective cohort studies (Appendix2). The criteria were adapted from Alt-man,10 Lievense et al,12 Hayden et al,13
and the STROBE Statement14 and weremodified to cover the topic of this re-view. Criteria could be answered with“yes (�),” “no (�).” or “don’t know(?).” One point was given to a criterionanswered with “yes,” and no pointswere given when answered with “no”or “don’t know.” Equal weights wereapplied to all items, resulting in a max-imum score of 10 points for case-control/cross-sectional studies and 11points for prospective cohort studies.Low risk for bias was defined as ascore of �7 points. Two reviewersscored all included articles indepen-dently (L.A.A.S. and M.B.M.). Interob-server variability was calculated withCohen’s �. In case of disagreement be-tween both reviewers, a third reviewer(Y.vL.) made the final decision.
e652 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Data Extraction and Analysis
Two reviewers performed data extrac-tion on a structured list independently.Extracted data included demograph-ics, description of the study popula-tion, inclusion and exclusion criteria,baseline characteristics, type of symp-toms analyzed, diagnostic tests used,and outcome data. As a measure forthe association between GI symptomsand H pylori, odds ratios (ORs) with95% confidence intervals (CIs) werecalculated for each symptom on thebasis of unadjusted data presented inindividual studies.
Data analysis was performed by usingReview Manager 5.0 (RevMan). Theweight given to each study was basedon the inverse of the variance. Hetero-geneity was quantified by Z2 and I2,which can be interpreted as the per-centage of the total variation betweenstudies that is attributable to hetero-geneity rather than to chance. A valueof 0% indicates no heterogeneity.When statistically significant heteroge-neity (P � .05) was observed, the re-sults of the random-effects model arepresented. When there was statisti-cally significant heterogeneity in out-comes across studies, subgroup anal-yses according to the level of risk forbias and different geographic loca-tions (ie, low-prevalence areas [West-ern countries, United States, Canada]versus high-prevalence areas [Medi-terranean, African, and Asian coun-tries]) were performed. In addition,the effect of outliers on the results wasevaluated.
When in studies the term RAP wasused, we considered it conform Apley’scriteria,15 when there was a referenceto Apley or the definition used by theauthors was almost similar in timespectrum to the definition proposed byApley (ie, at least 3 discrete episodesof abdominal pain of sufficient severityto interrupt normal daily activities orperformance over a period of not
less than 3 months). When studies re-ported on “unspecified abdominalpain,” “abdominal pain,” “symptomaticpatients,” or “GI-referral patients” inrelation to H pylori infection andthus not fulfilling Apley’s criteria, wegrouped these outcomes as unspeci-fied abdominal pain (UAP).
RESULTS
In total, 1120 potentially relevant ab-stracts were identified. After removingduplicates, we were left with 880unique abstracts. After screening allabstracts, 39 publications met our in-clusion criteria and none of the exclu-sion criteria.16–54 By searching the ref-erence lists of previous review articlesand included studies, we identified 1additional study.55 The interobserveragreement of the overall eligibility was� � 0.826.
One study could not be retrieved andthus could not be included in our anal-ysis.49 After reading full-text articles,we excluded another article becausethe study population did not includechildrenwhowere aged 0 to 18 years.50
Finally, 38 articles were reviewed: 23case-control studies,16–35,53,54 14 cross-sectional studies,36–47,51,52 and 1 pro-spective cohort study.48 Of 23 in-cluded case-control studies, 19 werehospital based16,17,19–21,23–35,55, 3 werepopulation-based,18,53,54 and 1 wasprimary care based.22 All cross-sectional studies were populationbased,36–42,44–47,51,55 except for 1 that in-cluded children in whom infection wassuccessfully eradicated previously.43
The only included prospective cohortstudy was population based.48
Results of the MethodologicQuality Assessment
The 2 reviewers (L.A.A.S. and M.B.M.)initially agreed on 89.5% of all qualityitems scored. The interobserveragreement of the assessment of riskfor bias was high (� � 0.789).
Mean score of risk for bias of all 38included studies was 6.03, rangingfrom 3.00 to 10.00. The mean qualityscore of case-control studies andcross-sectional studies separatelywas 5.35 (range: 3.00–10.00) vs 6.93(range: 5.00–9.00), respectively. Thisdifference was mainly caused by thelack of equal assessment of GI symp-toms for both case patients and con-trol subjects in 19 of 23 case-controlstudies, whereas all 14 cross-sectionalstudies used equal symptom assess-ment. Furthermore, 12 case-controlstudies did not draw case patients andcontrol subjects from a population atthe same risk for exposure, whereasthe studied populations of all cross-sectional studies did. The only prospec-tive cohort study scored 9 of 11 points.
In total 8 case-control stud-ies,17–19,22,28,29,30,53 7 cross-sectionalstudies,36,37,39,41,45,46,52 and the prospec-tive cohort study48 were categorized ashaving low risk for bias. Themost prev-alent shortcomings of case-controland cross-sectional studies were alack of blinded assessment of GI symp-toms and H pylori infection (n � 31),no use of multivariate analysis (n �27), and that prognostic factors werenot comparable at baseline and nocorrection for these factors was ap-plied in the analysis (n� 29).
Prevalence of H pylori
The prevalence of H pylori in population-based cross-sectional studies rangedfrom 9.4% to 56.6% with a mean prev-alence of 28.0% (SD: 16.2%). The prev-alence in high-prevalence areas (n �8) ranged from 15.8%47 to 56.6%36 witha mean prevalence of 37.0%. The prev-alence in low-prevalence areas (n� 6)ranged from 9.4%41 to 28.9%,42 with amean prevalence of 16.1%. The effectof different tests on the prevalence ofH pylori could not be evaluated be-cause a large diversity of (combina-tions of) diagnostic tests for H pylori
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e653 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

with different cutoff points were used,although the vast majority of studiesincluded serology testing.
RAP and H pylori
Fourteen case-control studies, involv-ing 3253 participants, reported on therelationship between RAP and H pyloriinfection in children.* Six had low riskfor bias17,18,22,26,30,53 and 8 had high riskfor bias.23,25,31–34,54,55 Figure 1 presentsthe meta-analysis of the OR of an H py-lori infection given the presence ofRAP. Because of statistically significantheterogeneity (P � .00001), therandom-effects model is presented.The pooled OR for all case-control stud-ies was 1.69 (95% CI: 0.99–2.86).
When we excluded the 2 outlier stud-ies of Mendez Nieto et al32 andMukherjee et al.34 the pooled OR be-came 1.21 (95% CI: 0.82–1.78), butstatistical heterogeneity remainedsignificant. In all additional analyses, theaforementioned outliers remained ex-cluded. Evaluation of heterogeneity ex-plained some of it but did not alter theestimated effect size.
Ten cross-sectional studies, involving3980 participants, reported on the re-lation between RAP and H pylori. Four
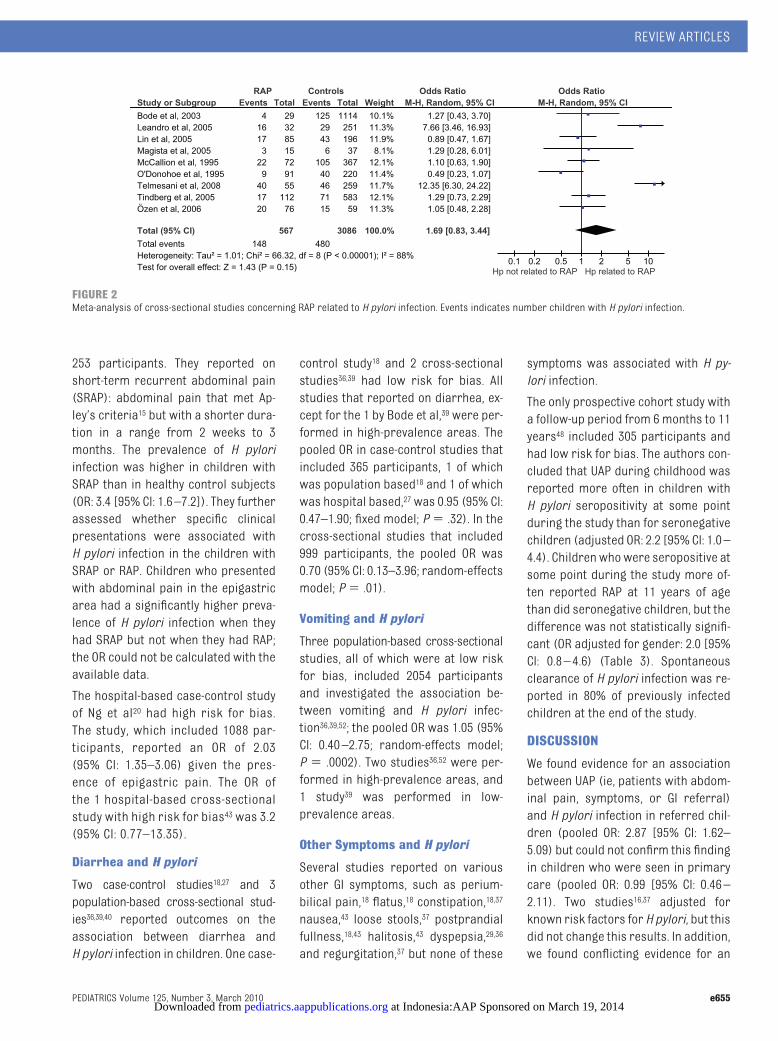
had low risk for bias36,37,39,45 and 6 highrisk.38,42–44,47,51 However, the study ofErtem et al,44 reporting an OR of 1.33,could not be pooled due to missing thepooled OR for the remaining studieswas 1.69 (95% CI: 0.83–3.44; randomeffects-model; P � .00001; Fig 2). Thestudies of Leandro Liberato et al47 andTelmesani51 explained statistical heter-ogeneity; excluding these outliers re-sulted in a pooled OR of 1.00 (95% CI:0.76–1.31; fixed model; P� .60). In ad-ditional analyses, these outliers re-mained excluded.
The pooled OR for the 4 studies withlow risk for bias was 0.95 (95% CI:0.66–1.37; fixed model; P � .24). Therelationship between RAP and H pyloriinfection was not influenced by risk forbias, setting, or geographic location.Two case-control studies22,30 and 2cross-sectional studies37,46 concerningRAP reported ORs adjusted for con-founders (Tables 1 and 2) ; however, alladjusted ORs are comparable to thepooled unadjusted ORs presented andremained nonsignificant.
UAP and H pylori
Six hospital-based case-control stud-ies16,19,21,24,28,35 that included 3142 partici-pants reported on the association be-
tween UAP and H pylori infection. Twostudies with low risk for bias19,28 and 4with high risk16,21,24,35 had a pooled OR of2.87 (95% CI: 1.62–5.09; random-effectsmodel; P � .0001; Fig 3). In the studieswith low risk for bias only, the pooled ORwas 1.66 (95% CI: 1.21–2.28; fixed model;P � .23). Pooling the 4 studies with highrisk for bias resulted in apooledORof 4.69(95%CI: 3.35–6.57; fixedmodel; P� .36).
Five population-based cross-sectionalstudies36,37,39,41,52 that included 3251participants and reported on UAP inchildren who were seen in primarycare all had low risk for bias. Thepooled OR was 0.99 (95% CI: 0.46–2.11;random-effectsmodel; P� .00001; Fig 4).
Three studies, 1 hospital-based case-control study16 and 2 population-basedcross-sectional studies,37,52 adjustedfor confounders (Tables 1 and 2). Theadjusted ORs were comparable to thepooled ORs presented.
Epigastric Pain and H pylori
Epigastric pain was evaluated in 2case-control studies18,20 and 1 cross-sectional study.43 Because of the diver-sity of outcome definitions, we werenot able to pool data. The population-based case-control study of Yang etal18 had low risk for bias and included*Refs 17, 18, 22, 23, 25, 26, 30–34, and 53–55.
FIGURE 1Meta-analysis of case-control studies concerning RAP related to H pylori infection. Events indicates number children with H pylori infection.
e654 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from
253 participants. They reported onshort-term recurrent abdominal pain(SRAP): abdominal pain that met Ap-ley’s criteria15 but with a shorter dura-tion in a range from 2 weeks to 3months. The prevalence of H pyloriinfection was higher in children withSRAP than in healthy control subjects(OR: 3.4 [95% CI: 1.6–7.2]). They furtherassessed whether specific clinicalpresentations were associated withH pylori infection in the children withSRAP or RAP. Children who presentedwith abdominal pain in the epigastricarea had a significantly higher preva-lence of H pylori infection when theyhad SRAP but not when they had RAP;the OR could not be calculated with theavailable data.
The hospital-based case-control studyof Ng et al20 had high risk for bias.The study, which included 1088 par-ticipants, reported an OR of 2.03(95% CI: 1.35–3.06) given the pres-ence of epigastric pain. The OR ofthe 1 hospital-based cross-sectionalstudy with high risk for bias43 was 3.2(95% CI: 0.77–13.35).
Diarrhea and H pylori
Two case-control studies18,27 and 3population-based cross-sectional stud-ies36,39,40 reported outcomes on theassociation between diarrhea andH pylori infection in children. One case-
control study18 and 2 cross-sectionalstudies36,39 had low risk for bias. Allstudies that reported on diarrhea, ex-cept for the 1 by Bode et al,39 were per-formed in high-prevalence areas. Thepooled OR in case-control studies thatincluded 365 participants, 1 of whichwas population based18 and 1 of whichwas hospital based,27 was 0.95 (95% CI:0.47–1.90; fixed model; P� .32). In thecross-sectional studies that included999 participants, the pooled OR was0.70 (95% CI: 0.13–3.96; random-effectsmodel; P� .01).
Vomiting and H pylori
Three population-based cross-sectionalstudies, all of which were at low riskfor bias, included 2054 participantsand investigated the association be-tween vomiting and H pylori infec-tion36,39,52; the pooled OR was 1.05 (95%CI: 0.40–2.75; random-effects model;P � .0002). Two studies36,52 were per-formed in high-prevalence areas, and1 study39 was performed in low-prevalence areas.
Other Symptoms and H pylori
Several studies reported on variousother GI symptoms, such as perium-bilical pain,18 flatus,18 constipation,18,37
nausea,43 loose stools,37 postprandialfullness,18,43 halitosis,43 dyspepsia,29,36
and regurgitation,37 but none of these
symptoms was associated with H py-lori infection.
The only prospective cohort study witha follow-up period from 6months to 11years48 included 305 participants andhad low risk for bias. The authors con-cluded that UAP during childhood wasreported more often in children withH pylori seropositivity at some pointduring the study than for seronegativechildren (adjusted OR: 2.2 [95% CI: 1.0–4.4). Childrenwhowere seropositive atsome point during the study more of-ten reported RAP at 11 years of agethan did seronegative children, but thedifference was not statistically signifi-cant (OR adjusted for gender: 2.0 [95%CI: 0.8–4.6) (Table 3). Spontaneousclearance of H pylori infection was re-ported in 80% of previously infectedchildren at the end of the study.
DISCUSSION
We found evidence for an associationbetween UAP (ie, patients with abdom-inal pain, symptoms, or GI referral)and H pylori infection in referred chil-dren (pooled OR: 2.87 [95% CI: 1.62–5.09) but could not confirm this findingin children who were seen in primarycare (pooled OR: 0.99 [95% CI: 0.46–2.11). Two studies16,37 adjusted forknown risk factors for H pylori, but thisdid not change this results. In addition,we found conflicting evidence for an
FIGURE 2Meta-analysis of cross-sectional studies concerning RAP related to H pylori infection. Events indicates number children with H pylori infection.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e655 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

TABLE1StudyCharacteristicsofIncludedCase-ControlStudies
Source
Setting,Place,Country,Period
CasePatients
ControlSubjects
DiagnosticTestUsed
forDeterminationof
HpyloriInfection
(CutoffPoint)
OR(95%CI)
Quality
Score
Daugule
etal,162007DiagnosticCentreofRiga,Latvia,
1998–2000
40consecutivechildrenwithindicationforupper
GIendoscopy,agerange8–12y,39%male
55asymptomaticchildrenwhovisitedtheirdoctor
forgeneralcheckuporminorhealthproblems,
aged7–12,55%male
Cases:RUTand/or
culturepositive
Controls:13C-UBT
UAP:1.80(0.62–5.14)
(adjustedforage)
4
Malatyetal,17
2006
PediatricGastroenterologyClinic
TexasChildren’sHospitaland
6primarycarepediatric
clinics,Houston,TX,Jun
2001–Dec2002
243consecutivechildrenreferredwith
abdominalpain,agerange3–18y,40%male;
excluded:childrenwithchronicillness/other
medicalconditions
330asymptomaticchildrenattending13licensed
childcarecentersinHouston,TX,aged3–18y,
45%male
Cases:13C-UBT
Controls:13C-UBT
(increaseof13C
abundanceof10
�g
ofureahydrolyzed
permin)
RAP:0.61(9.37–1.00)
7
Yangetal,18
2005
Elementaryschooland
associatedpreschool
kindergarten,Tainan,Taiwan
178childrenwhofulfilledthecriteriaofRAPor
SRAP(RAPduring2wk–3mo);agerange4–12
y,mean:9.2y,52%male
212age-andgender-matched,asymptomatic
childrenfromthesameschool
Cases:ELISA
Controls:ELISA
(absorbanceindexof
�0.14)
RAP:0.54(0.21–1.40)
SRAP:3.39(1.60–
7.17)
7
Chongetal,19
2003
12children’shospitalsor
medicalcentersthroughout
theUnitedStates,Jun
1996–Dec1997
373symptomaticGIreferralchildrenevaluated
inaGIclinicforabdominalpainandvomiting,
agerange:1–18y,mean:10.1y,48%male;
excluded:childrenwithintakeofantibiotics,
histamine-2blockers,orprotonpump
inhibitors1mobeforeenteringthestudy
618childrenseeninaclinicalsetting,who
requiredblooddrawingaspartofstandard
clinicalmanagement,withoutGIcomplaintsage
range:2mo–18y,meanage:7.7y,56%male
Cases:EIA
Controls:EIA
Referred
(symptomatic):
1.77(1.27–2.47)
8
Ngetal,20
2003
NationalUniversityHospital,
Singapore,Republicof
Singapore
489consecutivepatientswithepigastricpain;
outpatientreferralstopediatricGIclinic,
meanage:8.5
�3.3y,46%male;excluded:
childrenwhousedantibioticswithin4wkof
thestudy
599schoolchildrenparticipatingina
seroepidemiologicsurveyofDengueinthe
easternpartofSingapore,meanage:9.0
�0.5
y
Cases:ELISA
Controls:ELISA(2SD
abovevaluefor
histology-confirmed
negativesera)
Epigastricpain
(spiral):2.03
(1.35–3.06)
5
Plebanietal,21
1999
PediatricDepartment,Padua
UniversityHospital,Italy
183consecutivesymptomaticchildrenwho
underwentupperGIendoscopy,agerange:
1–16y,43%male
921randomlyselectedfromthosepresentatthe
second-degreeschoolsofPadua,agerange:
11–14y,53%male
Cases:atleast
histologypositive
Controls:anti–Hp-IgG
UAP:4.98(3.03–8.16)
3
MacArthur
etal,2219996primarycarepediatricians,
Toronto,Canada
100childrenpresentingwithRAP,agerange:
5–15y,mean:9.0
�2.7y,37%male;excluded:
childrenwithconcurrentdisease,suspected
organicdisease,aged
�5y,orhadused
bismuthinthepreviousmonth
100healthychildrenundergoingaroutine
checkuporvaccination,meanage:10.0
�3.2y,
57%male
Cases:serologyand/or
13C-UBT
Controls:serology
and/or13C-UBT
RAP:0.65(0.08–2.56)
(adjustmentnot
mentioned)
10
Guneletal,23
1998
DepartmentsofPediatric
SurgeryandPediatrics,Konya,
Turkey,during12-moperiod
42childrenwithRAP,agerange9–15y,mean:
9.4
�3.2y;excluded:iforganiccauseforRAP
(eg,pepticdisease,IBD,enzymedeficiencies)
wasfound
50healthychildrenattendingroutinedaysurgery,
meanage:9.65
�3.15y
Cases:IgGantibodytest
Controls:IgG
antibodytest
RAP:1.41(0.58–3.40)
3
Blumeletal,24
1998
KinderspitalderStadtWien,
Austria
31childrenpresentingwithchronicabdominal
pain
�4wkwithnegativestoolculture,
normalbloodcounts,andnormalabdominal
echo,agerange:6–14y,mean:10.51y,52%
male
31age-andnationality-matchedasymptomatic
childrenwhowereundergoingelective/acute
surgeryoroutpatientchildrenwhoreceived
treatmentfornoninfectiousdiseases,mean
age:10.5y
Cases:HpIgG-AK(�3
SDabovethemean
ofallnegativetests)
Controls:HpIgG-AK
UAP:2.52(0.90–7.02)
5
e656 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

TABLE1Continued
Source
Setting,Place,Country,Period
CasePatients
ControlSubjects
DiagnosticTestUsed
forDeterminationof
HpyloriInfection
(CutoffPoint)
OR(95%CI)
Quality
Score
Bansaletal,25
1998
KalawatiChildrenHospital,
DivisionofPediatric
Gastroenterologyand
Nutrition,NewDelhi,India
72childrenreferredwithcomplaintsofRAP;no
organiccausewasfoundafterstoolandurine
examinationsandapsychologicalevaluation;
agerange:3–12y,55%male
26age-andgender-matchedchildrenwith
complaintsotherthanthoserelatedtotheGI
tract,agerange:3–14y
Cases:RUTand/or
histologypositive
Controls:serology
(Hp-IgG
�20U/mL)
RAP:1.23(0.34–4.44)
3
Weweretal,26
1998
HvidovreHospital,Universityof
Copenhagen,Denmark
450childrenwithRAPwithnootherobvious
causesofRAP,agerange3.1–17.0y,mean:
9.0y,40%male
93childrenadmittedforminorelectivesurgery,
otherwiseingoodhealthanddidnotsuffer
fromGIcomplaints,agerange:3–15y,mean
age:6.3y,82%male
Cases:ELISA(�200EU)
andWesternblot
positive
Controls:ELISAand
Westernblotpositive
RAP(Westernblot):
2.36(1.14–4.87)
RAP(ELISA):2.09
(1.16–3.78)
7
Kehrtetal,27
1997
HealthCenter,Tipitapa,
Nicaragua,Sep1993–Dec199359childrenwithpersistentdiarrhearecruited
fromtheUROofthehealthcenterwithno
historyofantibioticuseinthepreviousmonth,
agerange:2–56mo,53%male
64randomlyselectedage-matchedasymptomatic
childrenreferredfrompediatriciansofthe
center,agerange:1–65mo,41%male
Cases:13C-UBT(13C/
12Cratioat60min
�3‰overbaseline)
Controls:13C-UBT
Persistentdiarrhea:
0.75(0.32–1.74)
6
Ozturketal,28
1996
DaySurgeryClinic,Hacettepe
UniversityChildren’sHospital,
Ankara,Turkey,Mar1993–Jun
1993
29childrenwhohadGIsymptomsandreported
tothedaysurgeryclinic,thelatterforminor
outpatientsurgicalproceduresofnon-GI
origin,agerange:1–17,59%male;excluded:
childrenwhousedantibiotics,Bismuth-
containingcompounds,NSAIDs,orantacids
duringpreceding2mo
32childrenwithoutGIsymptomswhoreportedto
thedaysurgeryclinic,thelatterforminor
outpatientsurgicalofnon-GIorigin,agerange:
1–17y,81%male
Cases:atleast2of4
followingtests
positive:serology,
RUT,histology,
bacterialculture
Controls:atleast2of
4followingtests
positive:serology,
RUT,histology,
bacterialculture
UAP:0.93(0.34–2.55)
7
Gurakan
etal,291996PediatricGastroenterologyUnit,
Ankara,Turkey,Nov1993–May
1994
59childrenreferredforevaluationofepigastric
orperiumbilicalpainand/ornausea,vomiting,
orregurgitationforatleast1mo,agerange:
5–17y,mean:11.1
�3.4,53%male;excluded:
useofantibiotics,H2-antagonists,Bismuth-salt
1mobeforeserologicexamination
48childrenwhowereseenintheoutpatient
clinicsfornon-GIcomplaints,agerange:5–17y,
meanage:10.73
�3.63,50%male
Cases:serology(IgG
�2SDabovethe
meanofallnegative
titers:ODunitsat
450nm)
Controls:serology
Dyspepsia:1.55
(0.72–3.34)
6
Hardikar
etal,301996RAPClinicatRoyalChildren’s
Hospital,Melbourne,
Australia,Feb1990–Feb1991
111childrenbetween5and12ywhohadRAP
andhadnotbeenseenpreviouslybya
pediatricianorsubspecialist,meanage:
8.5
�2.1y,33%male
103consecutivechildrenbetween5and12y
attendingdaysurgeryunitforcommonsurgical
disorders,otherwiseingoodhealthand
withoutGIsymptoms,meanage:7.7
�2.1y,
74%male
Cases:IgGantibodytest
(8Uofanti-HpIgG/
mL)Controls:IgG
antibodytest
RAP:0.21(0.05–0.85)
(adjustedfor
gender,age,and
parentalethnicity
andoccupation)
7
Chongetal,31
1995
GIDiseaseOutpatientClinic,J
Whitcomb,RileyHospitalfor
Children,IndianaUniversity,
IN,Jan1991–Dec1993
218childrenwhofulfilledcriteriaofRAPand
wereseenintheGIdiseaseoutpatientclinic
(RAPgroup),agerange:3–18y,meanage:
9.5y,49%male
238children,notfulfillingcriteriaofRAP,who
wereseenintheGIdiseaseoutpatientclinic
(non-RAPgroup)agerange:3–18y,meanage:
9.8y,55%male
Cases:serology
Controls:serology
RAP:1.80(1.05–3.10)
5
MendezNieto
etal,321994GastroenterologyDepartment,
NationalPediatricInstituteof
Mexico,Jan–Jun1993
40childrenreferredforrecurrentabdominal
pain,agerange5–18y,meanage:10.3y
40healthychildrenwithoutGIcomplaints
Cases:histologyand
rapidureasetest
Controls:ELISA(OD
of2SDofthemean
ofhealthychildren)
RAP:21.00
(4.45–99.08)
3
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e657 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

TABLE1Continued
Source
Setting,Place,Country,Period
CasePatients
ControlSubjects
DiagnosticTestUsed
forDeterminationof
HpyloriInfection
(CutoffPoint)
OR(95%CI)
Quality
Score
vanderMeer
etal,331992AcademicHospitalMaastricht,
Netherlands,during6-mo
period
82childrenbetween5.5and12.0y,withatleast
a6-moperiodofRAPofunknownorigin,
attacksofpainvaryinginseverity,duration,
andfrequency,sometimesaccompaniedby
vegetativesymptomssuchaspaleness,
nausea,orvomiting,meanage:10.8y,34%
male
39preoperativechildrenorchildrenattendingthe
outpatientclinicsforotherthanGIdiseases,
meanage:6.6y,64%male
Cases:ELISA(1.40OD
units)Controls:
ELISA
RAP:1.70(0.34–8.73)
4
Mukherjee
etal,342005OutpatientDepartmentofa
teachinghospital,Punjab,
India
68children
�3yofageattendingtheoutpatient
departmentofateachinghospitalbecauseof
RAPwithnoobviouscauseofpain,agerange:
3–12y,52%male
90normalcontrolsubjects,agerange:3–12y,
74%male
Cases:IgGantibodytest
Controls:IgG
antibodytest
RAP:13.67(5.88–
31.70)
5
Sedlackova
etal,352003HospitalinMorvia,Czech
Republic,1994–1999
829childrenbetween2and18y,whowere
referredforGIendoscopybecauseofRAPand/
ordyspepsia
205Age-,gender-,andSES-matchedchildren
attendingthehospitalinMorviaforother
reasonsthanGIcomplaints
Cases:serology
Controls:serology
Unspecified
(symptomatic):
6.20
4
Camorlinga
etal,551998NationalMedicalCenterofthe
InstitutoMexicanodelSeguro
Royal,MexicoCity,Mexico,Jan
1995–Sep1996
82consecutivechildrenseekingmedical
attentionbecauseofRAP,agerange:1–17y,
meanageinfectedcases:9.1
�3.9y,42%
male;excluded:childrenwhoreceived
antibiotics,H2blockers,orprotonpump
inhibitorsduringtheprevious30d
246age-andgender-matched,asymptomatic
patientsselectedusingamastersampling
framebasedongeneralpopulationcensus
data,agerange:2–17y,meanageinfected
controls:10.6
�3.7y,35%male
Cases:ELISA(mean
value
�3SDofthe
ODof30uninfected
patients)Controls:
ELISA
RAP:2.02(1.20–3.38)
3
Masoodpoor
etal,532008GuidanceschoolsinRafsanjan
City,Iran,Jan2006–Jan2007
40childrenfulfillingcriteriaofRAP,attendingthe
guidanceschool,meanage:12.7
�1.0y,50%
male;excluded:childrenwhoreceived
antibiotictreatment,H2blockers,orproton
pumpinhibitorsbeforeenteringstudy
60randomlyselected,age-,school-,andgender-
matchedhealthychildrenwhohadnoclinical
manifestationsofRAPandwerenormalon
physicalexamination,meanage:12.9
�1.1y,
50%male
Cases:HpSAELISAstool
antigentest(an
absorbanceat450/
630of
�0.120)
Controls:HpSAELISA
stoolantigentest
RAP:2.00(0.85–4.73)
7
Devanarayana
etal,542007SchoolinGampahaDistrictofSri
Lanka
55childrenidentifiedasfulfillingcriteriaofRAP
wererecruitedduringaschoolsurvey,mean
age:7.9
�3y,agerange:5–15y,41%male;
excluded:childrenwhoreceivedantibiotics,
acidsuppression,oranti–Hpyloritherapy
within3mobeforeinclusion
20healthychildrenrecruitedfromthesamearea,
meanage:9.0
�2.7y,agerange:5–15y,50%
male
Cases:Microwell-based
EIAthatdetectedH
pyloriantigensin
stool(absorbance
value
�190)Controls:
antigensinstool
RAP:1.03
(0.09–12.00)
4
RUTindicatesrapidureasetest;13C-UBT,13C-ureabreathtest;EIA,enzymeimmunoassay;ELISA,enzyme-linkedimmunosorbentassay;SES,socioeconomicstatus;IBD,irritablebowelsyndrome;URO,oralrehydrationunit;NSAID,nonsteroidal
anti-inflammatorydrug;OD,opticdensity.
e658 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

TABLE2StudyCharacteristicsofIncludedCross-SectionalStudies
Source
Setting,Place,Country,
Period
StudyPopulation
DiagnosticTestUsedfor
DeterminationofHpyloriInfection
(CutoffPoint)
N(Prevalence)
OR(95%CI)
Quality
Score
Ozenetal,36
2006
Preschoolsandschools,
Turkey,2004
136childrenwhoparticipatedinaprevious
study(Ertemetal),meanage:
13.45
�1.90y,range:8–17y,47%male
13C-UBT(achangeinthe13Cvalue
overbaselineof
�5‰)
136(56.6%)
RAP:1.05(0.48–2.28)
UAP:0.49(0.17–1.38)
Vomiting/diarrhea:1.80(0.68–4.74)
Dyspepsia:1.06(0.44–2.51)
9
Tindbergetal,37
2005
11localpublicschoolsin
Stockholm,Sweden,
Jan1998
695children,between10and12y,
attending1oftheparticipatinglocal
publicschools,meanage:11.2
�1.0y,
range:9–13y,48%male
PositiveifELISA(�0.22ODvalue)
positiveandatleast1of2ofthe
followingtestswaspositive:
immunoblot(CagA
�116kDa,
VacA
�89kDa),13C-UBT
695(16.1%)
RAP:1.00(0.50–2.10)
UAP:0.50(0.30–0.80)
Regurgitation:0.50(0.30–0.90)
Constipation:0.70(0.40–1.50)
WeeklyAP:1.50(0.70–3.30)
Loosestools:0.90(0.50–1.60)
(adjustedforage,gender,SES,
familysize,andimmigrant
background)
8
Linetal,382005
1primaryschool,
Danshuei,Taipei,
Taiwan,2003
289randomlyselectedgrades1to6
primaryschoolstudentswho
volunteeredforblood-testsforHpylori
IgGandanti–hepatitisAantibody,mean
age:9.21,51%male
ELISA
289(21.5%)
RAP:0.89(0.47–1.67)
6
Bodeetal,39
1998
SchoolsinUlm,Southern
Germany,1996
945preschoolchildren,aged5–8,who
wereexaminedforschoolfitnessbythe
PublicHealthService,meanage:5.84y,
range:5–8y,50%male;excluded:
childrenwhoreceivedantibiotic
treatmentwithinthelast4wk
13C-UBT(differencebetween
baseline13CO2/12CO2ratioand
30minratio
�5‰)
945(13.7%)
UAP:0.48(0.33–0.72)
Vomiting:0.45(0.29–0.72)
Diarrhea:0.31(0.20–0.48)
8
Rahmanetal,40
1998
Periurbancommunity
adjacenttothecapital
cityofBangladesh,
Jan–Oct1993
151childrenwhowerefreefromsystemic
infectioncausingdiarrhea,respiratory
infection,andotherinfectionsattimeof
enrollment,meanageHppos:8.9
�7.0
mo,Hpneg:9.9
�6.7,range:1–23mo,
50%male
13C-UBT(theexcessoverbaseline
valueof13CO2wasexpressed
aspartsperthousand(�%);a
cutoffpointof5intheratiowas
regardedaspositive)
151(45.0%)
Diarrhea:(after1mo):0.91(0.20–4.22)
Diarrhea(after6mo):1.08
(0.56–2.09)
6
Grimmetal,41
2003
SchoolsinAschaffenburg
andsurroundings,
Germany,schoolyear
1997/1998
540schoolchildren,aged7–9,11–15,and
16–20,whovoluntarilytookpart,age
range:7–20y,46%male
13C-UBT(theDOBvalueswere
elevatedabove3.5‰)
540Prevalence
�9.4
UAP:5.43(2.64–11.13)
7
McCallion
etal,421995
RoyalBelfastHospitalfor
SickChildren,Ireland,
during6-moperiod
439childrenattendingforroutineday
surgery,meanage:7.3y,range:4–13y
ELISA
439(28.9%)
RAP:1.10(0.63–1.90)
6
Magistaetal,43
2005
DepartmentofPediatric
Gastroenterology,
UniversityofBari,
Italy,1998–2000
52childreninwhominfectionwas
successfullyeradicatedpreviously,mean
age:12y,range:4.9–19.0y,52%male
Positivewhenall3testswere
positive:13C-UBT(changeof3.5
perthousandormorerelated
tobaselinesignal),RUT,and
histology
52(28.8%)
Epigastricpain:3.20(0.77–13.35)
Nausea:4.38(0.65–29.40)
RAP:1.29(0.28–6.01)
Halitosis:(4.28(0.65–29.40)
Postprandialfullness:1.27
(0.21–7.79)
6
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e659 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

TABLE2Continued
Source
Setting,Place,Country,
Period
StudyPopulation
DiagnosticTestUsedfor
DeterminationofHpyloriInfection
(CutoffPoint)
N(Prevalence)
OR(95%CI)
Quality
Score
Ertemetal,44
2003
Preschoolsandschools,
Turkey
327preschoolandschool-agedhealthy
children,meanage:8.2
�2.1y,range:
3–12y,52%male;excluded:children
whoreceivedoralorparenteral
antibioticswithin4wkbeforethe
investigation
13C-UBT(achangeinthe13Cvalue
overbaselineof
�5‰)
327(49.5%)
RAP:1.33(95%CIcouldnotbe
calculated)
5
O’Donohoe
etal,451995
7schoolsin1central
LondonDistrict,
England
640stateschoolandprivateschool
childrenwhovoluntarilyparticipated,
meanage:9.15y,range:4–13y,60%
male
IgGELISA(10U/mL)
640(16.7%)
RAP:0.49(0.23–1.07)
7
Bodeetal,46
2003
SchoolsinUlm,Erbach,
andEhingen,south
Germany,Jan–Jul
1997
1143preschoolchildrenaged5–8ywho
weretoattendfirstgradeand
underwentanschoolfitnessexamination
bythePublicHealthService,meanage:
5.88y,range:5–8y,49%male;excluded:
childrenwhousedantibioticswithinthe
past4wk
13C-UBT(achangeofthe13Cvalue
overbaselineof
�5‰)
1143(11.3%)
RAP:1.60(0.50–5.55)(adjustedfor
nationality,single-parenthousehold,
historyofpepticulcersofparents,
andhistoryofGIdisordersof
parents)
8
Leandroetal,47
2005
Healthcarecenter,Foral
deNavarra,Spain,Jan
2003–Mar2004
Randomsampleofchildrenaged1–14y,
visitingaregularhealthcareprogram,
meanage:6.89
�4.25y,50.7%male;
excluded:antibioticsinpastmonth,
previouseradicationtherapyforH
pylori,chronicdisease
EIAforfecalHpyloriantigen;at
450nmpositiveatDO
�0.160,
negativeatDO
�0.140
284(15.8%overall)
1–3y:8.4%
4–9y:13.9%
10–14y:24%
(P�.05)
RAP:7.66(3.46–16.93)
6
Telmesani,51
2008
Boys’schoolinMakkah
City,MakkahRegion,
WesternSaudiArabia
314boys,103ofwhominintermediatelevel
and211ofwhominsecondarylevel,age
range:12–18y,100%male;excluded:
recentuseofantibioticsorallergy
towardthetestmaterial
14C-UBT(resultscalculatedusing
grades0,notinfected;1,
borderline;2,infected;
borderlineresultsrequireda
repeattest)
314(27.4%)
RAP:12.35(6.30–24.22)
6
Siaietal,52
2008
SchoolsintheCap-Bon
region,Nabeul
Governorship,Tunesia
1055randomlyselected(1st,10th,20th,
etc)first-gradeprimaryschoolchildren
belongingtotherecruitmentpopulations
of13healthcarecenters’databases,813
childrenof6y,242childrenof7y,49.9%
male
IgGELISA
1055(51.4%)
UAP:1.45(1.01–2.50)(adjustedfor
householdmembers
�5,bottle
weaning
�18moplate/bed-sharing,
SES,abdominalpain,vomiting)
Vomiting:1.63(1.04–2.54)
9
ELISAindicatesenzyme-linkedimmunosorbentassay;OD,opticdensity;DOB,deltaoverbaseline.
e660 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

association between epigastric painand H pylori infection. In total, 2 of 3studies showed a statistically signifi-cant association between epigastricpain and H pylori infection. This findingwas independent of setting. Further-more, there is strong evidence thatRAP is not related to H pylori.
The European Pediatric Task Force4
concluded in their guidelines on man-agement of H pylori infection that, inchildren, H pylori infection is not re-lated to GI symptoms. Our findings con-tradict this assumption but are in
agreement with findings in adults, forwhom dyspepsia is thought to becaused by H pylori. Our findings par-tially support the Consensus Reportof The European Helicobacter StudyGroup; they reported that RAP is not anindication for a test-and-treat strategyfor H pylori infection in children; how-ever, children with upper GI symptomsshould be tested after exclusion ofother causes of the symptoms.6
The finding for an association betweenUAP and H pylori infection in referredchildren but not in children who were
seen in primary care is in agreementwith our finding of evidence that RAPandH pylori are not related. Abdominalpain in a child who sees a generalpractitioner (GP) has a different differ-ential diagnosis than abdominal painin a child who is seen in secondarycare. Abdominal pain in primary caremore often will be functional. In a set-ting where a symptom is dominantlyrelated to functional disease, an asso-ciation between the symptom and alow-prevalent disorder might be tooweak to detect. In addition, a GP will
FIGURE 3Meta-analysis of case-control studies concerning UAP related to H pylori infection. Events indicates number children with H pylori infection.
FIGURE 4Meta-analysis of cross-sectional studies concerning UAP related to H pylori infection. Events indicates number children with H pylori infection.
TABLE 3 Study Characteristics of Included Prospective Cohort Study
Source Setting, Place, Country,Period
Study Population Diagnostic Test Used forDetermination ofH pylori Infection(Cutoff Point)
Patients Lost to Follow-up,%
OR (95% CI) QualityScore
Tindberg et al,48
1999Vaccine trial, Southernpart of Sweden,Stockholm,1984–1995
305 children, born in 1984,who participated in apertussis vaccine trial,starting at 6 mo to 11 y;mean age at end offollow-up: 10.9 y (range:10.5–12.3 y)
ELISA (0.360 A405 nm),measured at 6 mo, 8mo, 10 mo, 18 mo, 2 y,4 y, and 11 y
Blood samples from 6 to 18mo of age and at least 1additional serum sampledrawn at 2, 4, or 11 y ofage were available from294 children; lost tofollow-up: 11 (3.6%)
RAP (during last 6 mo):2.0 (0.8–4.6) UAP(during childhood):1.4 (0.7–2.9) UAP(last 6 mo):2.2 (1.2–4.7)
9
ELISA indicates enzyme-linked immunosorbent assay.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e661 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

refer only children in whom he sus-pects underlying disease; therefore, inreferred children, the same symptomis more likely to be related to a poten-tial pathogen such as H pylori.
RAP as defined by Apley and Naish15 isthought to be related to functionaldisease and should therefore theo-retically preclude H pylori. We foundno evidence for any relation betweenRAP by Apley and Naish and H pyloriinfection in children in both case-control studies (OR: 1.21 [95% CI:0.82–1.78) and cross-sectional stud-ies (OR: 1.00 [95% CI: 0.76 –1.31). Sub-group analyses of RAP in differentsettings, high-quality studies, anddifferent geographic locations didnot alter this finding. In low-qualitycase-control studies, the associationbetween RAP and H pylori was clini-cally and statistically significant (OR:2.68 [95% CI: 1.47– 4.89); however, webelieve that this OR is overestimatedbecause of a biased selection of con-trol subjects. Whereas in 4 of 5 high-quality studies case patients andcontrol subjects were drawn from apopulation at a comparable risk forexposure (ie, H pylori infection), thiswas not the case in all of the low-quality studies. The ORs suggest a se-lection of control subjects in whomnot only GI symptoms but also H py-lori infection was precluded. Thismight have seriously biased theseoutcomes.
After excluding the outlier studies ofLeandro Liberato et al47 and Telme-sani,51 the pooled OR of cross-sectionalstudies that evaluated the relation be-tween RAP and H pylori was 1.00 (95%CI: 0.76–1.31). This finding underlinesthe absence of a relation between RAPand H pylori infection in children asfound in the case-control studies. Onthe basis of the data presented, wecould not explain the outlying resultsof the study of Leandro Liberato et al47
and Telmesani.51
RAP is mainly defined by the durationof abdominal pain. We assume that se-lecting children with RAP is more thana selection that is based on duration ofabdominal pain alone. Selection ofchildren with RAP will implicitly com-prise the belief of the primary care cli-nician that RAP in the long-term doesnot affect growth and that develop-ment of the child will be functional andthat in referred children it will com-prise the (negative) results of previousinvestigations. Because of these im-plicit selection criteria, we assumethat the included childrenwith RAPwillbe at high risk for functional disease.None of these selection mechanisms,however, was described in the studieson RAP that were included in this re-view. That duration of pain may pre-clude underlying disorders as a resultof the aforementioned mechanisms isaffirmed by the findings of Yang et al.18
That population-based study reporteda statistically significant associationbetween SRAP (ie, abdominal pain thatmet the criteria of Apley and Naish15
but with a shorter duration in rangefrom 2 weeks to 3 months) in the epi-gastric region and H pylori infection.
To our knowledge, this is the first pub-lished review to investigate the associ-ation between GI symptoms in generaland H pylori infection in children. Theresults of our review concerning RAPare consistent with 2 previous system-atic reviews that reported no obviousassociation between RAP and H pyloriinfection in children.8,9
Although our literature search wascomprehensive, some published andunpublished studies may have beenmissed. Also, some information perti-nent to the review and collected by thereviewers may not have been providedin the journal article, although we con-tacted first authors to request missingdata with variable success.
Cautious interpretation of pooled ORsis necessary because we found a large
statistical and clinical heterogeneitybetween studies and an overall poormethodologic quality. Using a best evi-dence synthesis to summarize the datacould overcome these problems, butlimited data exist on best evidence syn-theses for observational studies, andthe possibility of misclassifying the re-sults of studies with a small samplesize is large.
We found that children who are re-ferred to a gastroenterologist withUAP or pain in the epigastric region ingeneral are at two- to threefold higherrisk for H pylori infection than childrenwithout these symptoms. Because weare not aware of the criteria on whicha GP decides to refer a child with ab-dominal pain to a pediatric gastroen-terologist, a more specific clinical pic-ture has yet to be established. Whetherto screen systematically referred chil-dren with abdominal (epigastric) paindepends on effectiveness and adverseeffects of eradication therapy. No opti-mal treatment has yet been defined.
To confirm, disclaim, or specify ourfindings on UAP and epigastric pain,additional research is necessary. Ifthere is an association between thesesymptoms and H pylori infection, thentreating and thus eradicating H pylorimust lead to improvement or disap-pearance of symptoms. Randomized,placebo-controlled, double-blind trialswith minimal loss to follow-up andstandardized and validated outcomemeasures are needed. To our knowl-edge, no such trial has been published.
CONCLUSIONS
There is no association betweenRAPandH pylori infection in children; therefore,screening children with this classicalsymptom is not warranted, regardlessof setting and geographic location. Fur-thermore, all other GI symptoms in-vestigated in primary care–based orpopulation-based studies, except for epi-gastric pain, were not associated with H
e662 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

pylori infection in children; therefore, wepostulate that as long as no typical clini-cal picture of a child with H pylori infec-tion has been established and treatmenteffectiveness is not known, referral to a
subspecialist for this matter is notrecommended.
Furthermore we postulate that UAPin a hospital-based setting and epi-gastric pain in general might be as-
sociated with an (acute) H pylori in-fection. Data reporting on epigastricpain, however, were limited, so addi-tional research to investigate this as-sociation is needed.
APPENDIX 1: SEARCH STRATEGIES
Medline search, 27th of July 2009 608 results
(epidemiologic-studies OR case-control OR cohort OR follow-up OR longitudinal OR prospective OR retrospective OR cross-sectional) AND (helicobacter pylori OR campylobacter) AND (“Signs and Symptoms, Digestive”[mesh] OR abdominal pain ORdyspepsia) AND (infant OR infant* OR child OR child* OR adolescent OR adolescen*)
Embase search, 27th of July 2009 512 results
((‘epidemiologic studies’/exp OR ‘epidemiologic studies’) OR ‘cross-sectional study’ OR ‘case control study’ OR ‘cohort analysis’OR (‘follow up’/exp OR ‘follow up’) OR longitudinal OR prospective OR retrospective) AND ((‘helicobacter pylori’/exp OR ‘heli-cobacter pylori’) OR (‘campylobacter’/exp OR ‘campylobacter’)) AND ((‘gastrointestinal symptom’/exp OR ‘signs and symp-toms, digestive’) OR (‘abdominal pain’/exp OR ‘abdominal pain’) OR (‘dyspepsia’/exp OR ‘dyspepsia’)) AND ((‘infant’/exp OR‘infant’) OR infant* OR (‘child’/exp OR ‘child’) OR child* OR (‘adolescent’/exp OR ‘adolescent’) OR adolescen*)
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e663 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

APPENDIX 2: EXPLANATION OF CRITERIA
MB / YvL / LS / MM
General
Case control study / Cross-sectional study
Criteria Score
1.
2.
3.
4.
5.
6.
7.*
8.
9.
10.
Total Score (10 points maximum)
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
……*
e664 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Explanation of criteria: Case control study/Cross-sectional study
Study population1.
2.
3.
Helicobacter pylori4.
5.
6.
Study design7.
Analysis and data presentation8.
9.
10.
OR
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e665 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

MB / YvL / LS / MM
General
Prospective cohort study
Criteria Score
1.
2.
3.
4.
5.
6.
7. *
8.
9.
10.
11.
Total Score (11 points maximum)
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
…….*
e666 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Explanation of criteria: Prospective cohort study
Study population1.
2.
3.
Helicobacter pylori4.
5.
Gastrointestinal symptoms6.
Study design7.
8.
Analysis and data presentation9.
10.
11
OR
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e667 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

REFERENCES1. Logan RP, Walker MM. ABC of the upper gas-trointestinal tract: epidemiology and diag-nosis of Helicobacter pylori infection. BMJ.2001;323(7318):920–922
2. Malaty HM, El-Kasabany A, Graham DY, et al.Age at acquisition of Helicobacter pyloriinfection: a follow-up study from infancy toadulthood. Lancet. 2002;359(9310):931–935
3. Moss SF, Malfertheiner P. Helicobacter andgastric malignancies. Helicobacter. 2007;12(suppl 1):23–30
4. Drumm B, Koletzko S, Oderda G. Helicobac-ter pylori infection in children: a consensusstatement. European Paediatric Task Forceon Helicobacter pylori. J Pediatr Gastroen-terol Nutr. 2000;30(2):207–213
5. Gold BD, Colletti RB, Abbott M, et al. Helico-bacter pylori infection in children: recom-mendations for diagnosis and treatment.J Pediatr Gastroenterol Nutr. 2000;31(5):490–497
6. Malfertheiner P, Megraud F, O’Morain C, etal. Current concepts in the management ofHelicobacter pylori infection: the Maas-tricht III Consensus Report. Gut. 2007;56(6):772–781
7. Koletzko S. Noninvasive diagnostic tests forHelicobacter pylori infection in children.Can J Gastroenterol. 2005;19(7):433–439
8. Macarthur C, Saunders N, Feldman W. Heli-cobacter pylori, gastroduodenal disease,and recurrent abdominal pain in children.JAMA. 1995;273(9):729–734
9. Macarthur C. Helicobacter pylori infectionand childhood recurrent abdominal pain:lack of evidence for a cause and effect rela-tionship. Can J Gastroenterol. 1999;13(7):607–610
10. Altman DG. Systematic reviews of evalua-tions of prognostic variables. BMJ. 2001;323(7306):224–228
11. Landis JR, Koch GG. An application of hierar-chical kappa-type statistics in the assess-ment of majority agreement among multi-ple observers. Biometrics. 1977;33(2):363–374
12. Lievense AM, Bierma-Zeinstra SM, VerhagenAP, Verhaar JA, Koes BW. Prognostic factorsof progress of hip osteoarthritis: a system-atic review. Arthritis Rheum. 2002;47(5):556–562
13. Hayden JA, Cote P, Bombardier C. Evaluationof the quality of prognosis studies in sys-tematic reviews. Ann Intern Med. 2006;144(6):427–437
14. von Elm E, Altman DG, Egger M, et al. TheStrengthening the Reporting of Observa-tional Studies in Epidemiology (STROBE)statement: guidelines for reporting obser-
vational studies. Lancet. 2007;370(9596):1453–1457
15. Apley J, Naish N. Recurrent abdominalpains: a field survey of 1,000 school chil-dren. Arch Dis Child. 1958;33(168):165–170
16. Daugule I, Rumba I, Alksnis J, Ejderhamn J.Helicobacter pylori infection among chil-dren with gastrointestinal symptoms: ahigh prevalence of infection among patientswith reflux oesophagitis. Acta Paediatr.2007;96(7):1047–1049
17. Malaty HM, Abudayyeh S, Graham DY, GilgerMA, Rabeneck L, O’Malley K. A prospectivestudy for the association of Helicobacter py-lori infection to a multidimensional mea-sure for recurrent abdominal pain in chil-dren. Helicobacter. 2006;11(4):250–257
18. Yang YJ, Sheu BS, Lee SC, Wu JJ. Short-termrecurrent abdominal pain related to Helico-bacter pylori infection in children. J Gastro-enterol Hepatol. 2005;20(3):395–400
19. Chong SK, Lou Q, Zollinger TW, et al. The se-roprevalence of Helicobacter pylori in a re-ferral population of children in the UnitedStates. Am J Gastroenterol. 2003;98(10):2162–2168
20. Ng BL, Quak SH, Aw M, Goh KT, Ho B. Immuneresponses to differentiated forms of Helico-bacter pylori in children with epigastricpain. Clin Diagn Lab Immunol. 2003;10(5):866–869
21. Plebani M, Guariso G, Fogar P, et al. Effect ofcagA status on the sensitivity of enzyme im-munoassay in diagnosing Helicobacterpylori-infected children. Helicobacter. 1999;4(4):226–232
22. Macarthur C, Saunders N, Feldman W, et al.Helicobacter pylori and childhood recur-rent abdominal pain: community basedcase-control study. BMJ. 1999;319(7213):822–823
23. Gunel E, Findik D, Caglayan O, Caglayan F,Topgac Z. Helicobacter pylori and hypergas-trinemia in children with recurrent abdom-inal pain. Pediatr Surg Int. 1998;14(1–2):40–42
24. Blumel P, David M, Hirschl AM, Konig H. Inci-dence of increased serum Helicobacter py-lori IgG antibodies in childrenwith andwith-out chronic abdominal pain [in German].Klin Padiatr. 1998;210(5):366–369
25. Bansal D, Patwari AK, Malhotra VL, MalhotraV, Anand VK. Helicobacter pylori infection inrecurrent abdominal pain. Indian Pediatr.1998;35(4):329–335
26. Wewer V, Andersen LP, Paerregaard A, et al.The prevalence and related symptomatol-ogy of Helicobacter pylori in children withrecurrent abdominal pain. Acta Paediatr.1998;87(8):830–835
27. Kehrt R, Becker M, Brosicke H, Kruger N,Helge H. Prevalence of Helicobacter pyloriinfection in Nicaraguan children with per-sistent diarrhea, diagnosed by the 13C-ureabreath test. J Pediatr Gastroenterol Nutr.1997;25(1):84–88
28. Ozturk H, Senocak ME, Uzunalimoglu B, Has-celik G, Buyukpamukcu N, Hicsonmez A. Hel-icobacter pylori infection in symptomaticand asymptomatic children: a prospectiveclinical study. Eur J Pediatr Surg. 1996;6(5):265–269
29. Gurakan F, Kocak N, Yuce A. Helicobacterpylori serology in childhood. Turk J Pediatr.1996;38(3):329–334
30. Hardikar W, Feekery C, Smith A, Oberklaid F,Grimwood K. Helicobacter pylori and recur-rent abdominal pain in children. J PediatrGastroenterol Nutr. 1996;22(2):148–152
31. Chong SK, Lou Q, Asnicar MA, et al. Helico-bacter pylori infection in recurrent abdom-inal pain in childhood: comparison of diag-nostic tests and therapy. Pediatrics. 1995;96(2 pt 1):211–215
32. Mendez Nieto CM, Ramirez Mayans J, Cer-vantes Bustamente R, et al. Helicobacter py-lori diagnosis in children with recurrentabdominal pain [in Spanish]. Acta Gastro-enterol Latinoam. 1994;24(3):169–174
33. van der Meer SB, Forget PP, Loffeld RJ, Stob-beringh E, Kuijten RH, Arends JW. The prev-alence of Helicobacter pylori serumantibodies in children with recurrent ab-dominal pain. Eur J Pediatr. 1992;151(11):799–801
34. Mukherjee P, Chacko B, Singh T, Pawar G,Kaur H. Prevalence of Helicobacter pylori in-fection in children with recurrent abdomi-nal pain. Trop Gastroenterol. 2005;26(2):102–104
35. Sedlackova M, Malaty H, Volf V, et al. Helico-bacter pylori infection in a group of symp-tomatic and asymptomatic children and ad-olescents in the Czech Republic [in Czech].Cas Lek Cesk. 2003;142(2):102–105
36. Ozen A, Ertem D, Pehlivanoglu E. Natural his-tory and symptomatology of Helicobacterpylori in childhood and factors determiningthe epidemiology of infection. J Pediatr Gas-troenterol Nutr. 2006;42(4):398–404
37. Tindberg Y, Nyren O, Blennow M, GranstromM. Helicobacter pylori infection and abdom-inal symptoms among Swedish school chil-dren. J Pediatr Gastroenterol Nutr. 2005;41(1):33–38
38. Lin HY, Chuang CK, Lee HC, Chiu NC, Lin SP,Yeung CY. A seroepidemiologic study of Hel-icobacter pylori and hepatitis A virus infec-tion in primary school students in Taipei. J
e668 SPEE et al at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

Microbiol Immunol Infect. 2005;38(3):176–182
39. Bode G, Rothenbacher D, Brenner H, AdlerG. Helicobacter pylori and abdominalsymptoms: a population-based studyamong preschool children in southern Ger-many. Pediatrics. 1998;101(4 pt 1):634–637
40. Rahman MM, Mahalanabis D, Sarker SA, etal. Helicobacter pylori colonization in in-fants and young children is not necessarilyassociated with diarrhoea. J Trop Pediatr.1998;44(5):283–287
41. Grimm W, Fischbach W. Helicobacter pyloriinfection in children and juveniles: an epide-miological study on prevalence, socio-economic factors and symptoms [in Ger-man]. Dtsch Med Wochenschr. 2003;128(37):1878–1883
42. McCallion WA, Bailie AG, Ardill JE, BamfordKB, Potts SR, Boston VE. Helicobacter pylori,hypergastrinaemia, and recurrent abdomi-nal pain in children. J Pediatr Surg. 1995;30(3):427–429
43. Magista AM, Ierardi E, Castellaneta S, et al.Helicobacter pylori status and symptom as-sessment two years after eradication in pe-diatric patients from a high prevalencearea. J Pediatr Gastroenterol Nutr. 2005;40(3):312–318
44. ErtemD, Harmanci H, Pehlivanoglu E. Helico-
bacter pylori infection in Turkish preschooland school children: role of socioeconomicfactors and breast feeding. Turk J Pediatr.2003;45(2):114–122
45. O’Donohoe JM, Sullivan PB, Scott R, RogersT, Brueton MJ, Barltrop D. Recurrent ab-dominal pain and Helicobacter pylori in acommunity-based sample of London chil-dren. Acta Paediatr. 1996;85(8):961–964
46. Bode G, Brenner H, Adler G, Rothenbacher D.Recurrent abdominal pain in children: evi-dence from a population-based study thatsocial and familial factors play a major rolebut not Helicobacter pylori infection. J Psy-chosom Res. 2003;54(5):417–421
47. Leandro Liberato SV, Hernandez Galindo M,Torroba Alvarez L, et al. Helicobacter pyloriinfection in the child population in Spain:prevalence, related factors and influenceon growth [in Spanish]. An Pediatr (Barc).2005;63(6):489–494
48. Tindberg Y, Blennow M, Granstrom M. Clini-cal symptoms and social factors in a cohortof children spontaneously clearing Helico-bacter pylori infection. Acta Paediatr. 1999;88(6):631–635
49. Kasirga E, Ertan P, Tosun S, Sanhdag T, Tan-sug N, Onag A. Children with recurrent ab-dominal pain in Manisa Region, WesternTurkey: an evaluation of serological preva-
lence of Helicobacter pylori. Int J Med. 2003;5(1):32–35
50. Reshetnikov OV, Haiva VM, Granberg C,Kurilovich SA, Babin VP. Seroprevalence ofHelicobacter pylori infection in Siberia. Hel-icobacter. 2001;6(4):331–336
51. Telmesani AM. Helicobacter pylori: preva-lence and relationship with abdominal painin school children in Makkah City, westernSaudi Arabia. Saudi J Gastroenterol. 2009;15(2):100–103
52. Siai K, Ghozzi M, Ezzine H, et al. Prevalenceand risk factors of Helicobacter pylori infec-tion in Tunesian children: 1055 children inCap-Bon (northeastern Tunisia). Gastroen-terol Clin Biol. 2008;32(11):881–886
53. Masoodpoor N, Darakhshan, SheikhvatanM. Helicobacter pylori infection in Iranianchildren with recurrent abdominal pain.Trop Gastroenterol. 2008;29(4):221–223
54. Devanarayana NM, de Silva DG, de Silva HJ.Aetiology of recurrent abdominal pain in acohort of Sri Lankan children. J PaediatrChild Health. 2008;44(4):195–200
55. Camorlinga-Ponce M, Torres J, Perez-PerezG, et al. Validation of a serologic test for thediagnosis of Helicobacter pylori infectionand the immune response to urease andCagA in children. Am J Gastroenterol. 1998;93(8):1264–1270
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e669 at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2010-0941; originally published online February 15, 2010; 2010;125;e651PediatricsMarjolein Y. Berger
Leo A. A. Spee, Marieke B. Madderom, Maaike Pijpers, Yvonne van Leeuwen andChildren
and Gastrointestinal Symptoms inHelicobacter pyloriAssociation Between
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/125/3/e651.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/125/3/e651.full.hat:This article cites 55 articles, 8 of which can be accessed free
Citations
tml#related-urlshttp://pediatrics.aappublications.org/content/125/3/e651.full.hThis article has been cited by 7 HighWire-hosted articles:
Subspecialty Collections
ology_subhttp://pediatrics.aappublications.org/cgi/collection/gastroenterGastroenterologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 19, 2014pediatrics.aappublications.orgDownloaded from







