

Practical Internal Medicine
Megaesophagus
Wendy Blount, DVM
Nacogdoches, TX

Megaesophagus
The most common
esophageal disorder
in dogs and cats.

Cats Are Not Little Dogs
Speed of Esophageal Transit• Dog – 75-100 cm/sec• Cat – 1-2 cm/sec
Why??• Striated muscle is faster than smooth
So What??Eating fast causes more vomiting in cats – tube
feeding must be slow
Cats Are Not Little Dogs
Muscle Type• Dog – entirely striated• Cat – cranial 2/3 striated, caudal 1/3 smooth
So What??Cisapride works on smooth muscle
Will work better on cats with megaesophagus when compared to dogs

Megaesophagus - Definition
• Part or all of the esophagus is enlarged.• Food is not properly conducted from the
mouth to the stomach.• Affected pets may not get adequate
nutrition.• Affected pets are at risk for aspiration
pneumonia, which can be life threatening.• It can be part of a more widespread
disease or muscle weakness.
Megaesophagus - Etiology
Generalized Megaesophagus
Entire esophagus is affected
Localized megaesophagus
Usually proximal to obstruction
Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Esophageal Stricture
Causes• trauma• caustic substance swallowed• doxycycline
(Oreo)

Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Esophageal Stricture
Causes• trauma• caustic substance swallowed• doxycycline
(Oreo)

Megaesophagus - Etiology
Localized megaesophagusUsually proximal to obstruction
Foreign bodyWhere are they most common?• thoracic inlet• base of the heart
(Dr. Weatherly’s Case)

Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction

Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
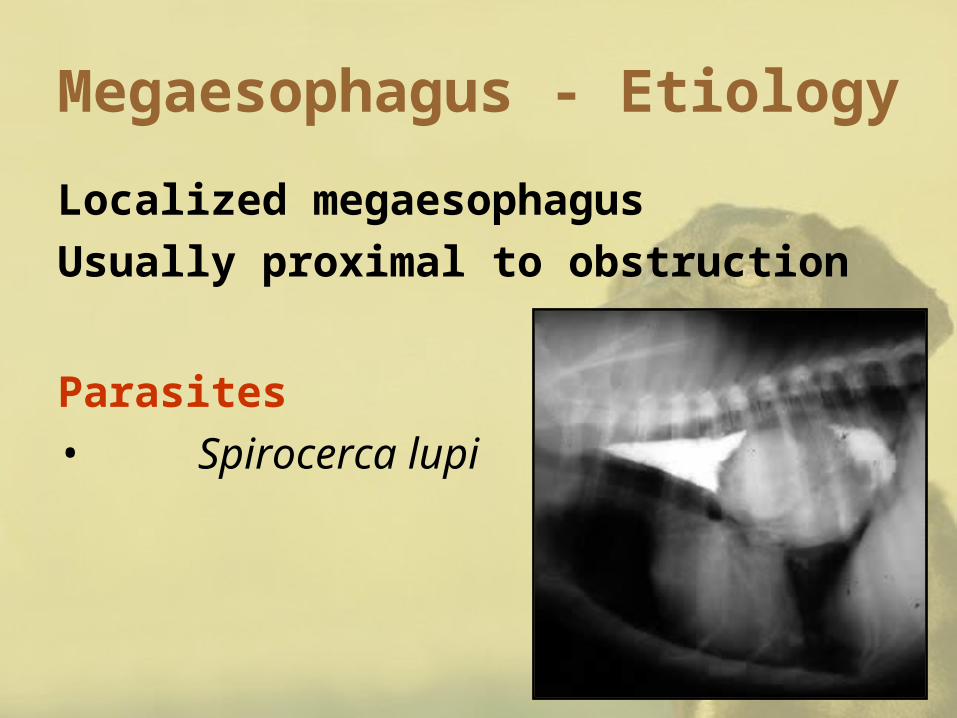
Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Parasites
• Spirocerca lupi

Spirocirca lupi
Localized megaesophagus
Usually proximal to obstruction

Spirocirca lupi
Localized megaesophagus
Usually proximal to obstruction
Spirocirca lupi
Localized megaesophagus
Usually proximal to obstruction

Spirocirca lupi
Who Gets It?
• Dogs
How Do They Get It?
• Eating a beetle
Where else can lesions be?
• Aorta
• Stomach

Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction

Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Vascular Ring Anomaly
• persistent right aortic arch (PRAA)
• ring by left subclavian artery and brachiocephalic trunk
Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
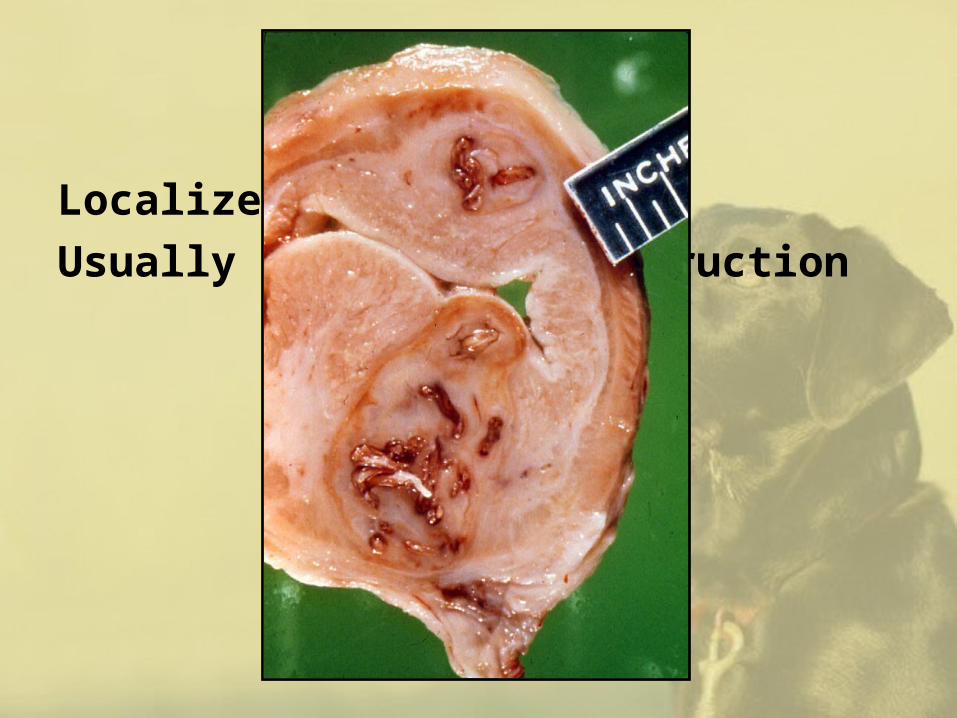
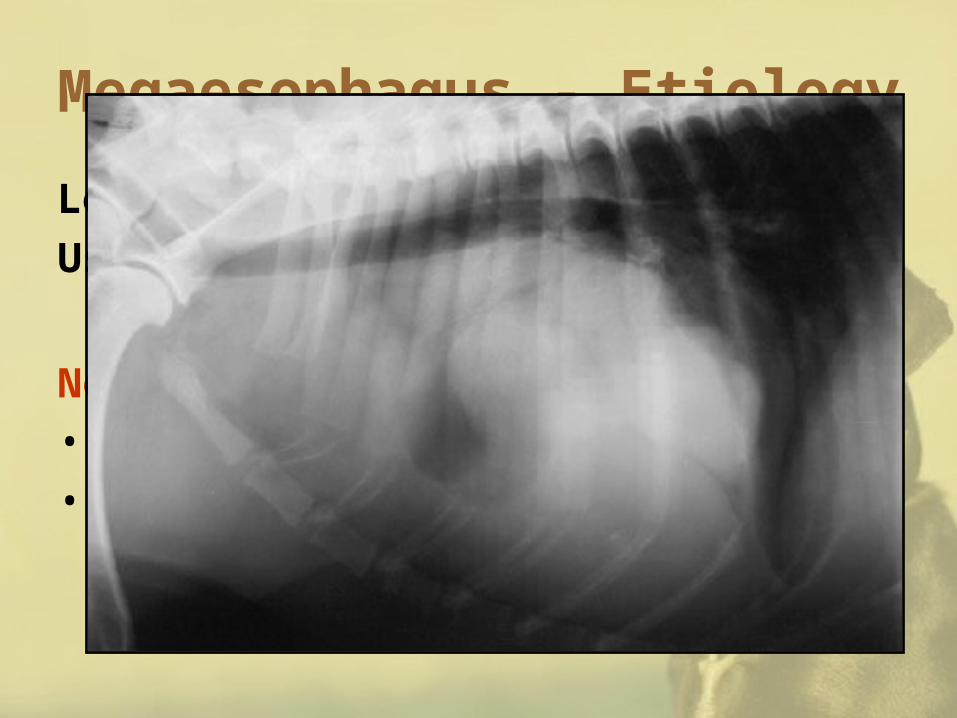
Neoplasia
• Esophageal neoplasia
• Mediastinal mass – which tumors?– Lymphosarcoma– Thymoma
Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Neoplasia
• Esophageal neoplasia
• Mediastinal mass – which tumors?– Lymphosarcoma– Thymoma
Megaesophagus - Etiology
Localized megaesophagus
Usually proximal to obstruction
Congenital
• Esophageal diverticulum – where?
• Base of the heart - breed?
• English Bulldog

Megaesophagus - Etiology
Generalized Megaesophagus
Localized megaesophagus
Usually proximal to obstruction
Generalized Megaesophagus
Generalized Megaesophagus
Two Onsets• Congenital• Acquired
What’s the Difference?
Prognosis• Congenital – guarded• Acquired – short term guarded; long term
potentially good, depending on the cause.
Generalized Megaesophagus
Two Types:
• Megaesophagus alone
• ME as part of a generalized myopathy, neuropathy or junctionopathy
Why Do We Care?
If the underlying cause of weakness is not addressed, the animal will not do well

Generalized Megaesophagus
What is Junctionopathy?
Disease of the myoneural junction
Most Common Junctionopathy
Myasthenia gravis
Who has diagnosed a case of myasthenia gravis?

Generalized Megaesophagus - Alone
The most common esophageal disease in dogs and cats is megaesophagus
Causes – two most common• Idiopathic• Myasthenia gravis
Other Causes• Esophagitis• Congenital
Esophagitis
Generalized Megaesophagus - Alone
Esophagitis
Chronic inflammation can result in ileus
Causes of esophagitis:
• Gastroesophageal reflux
• Hiatal hernia
• Chronic GDV
Generalized Megaesophagus
Myasthenia gravis• Auto-immune disorder• Autoantibodies against Ach receptors
There are four kinds of MG– Congenital– Acquired Focal
• Esophagus, pharynx/larynx, facial nerve
– Acquired Generalized– Acquired Acute Fulminant

Generalized Megaesophagus
There are four kinds of MGWhy do we care??Different Prognoses• Congenital – poor• Acquired Acute Fulminant – dismal• Acquired Focal and Generalized
– Long term potentially good– Most cases of acquired MG resolve within a year– Short term guarded– 50% die of aspiration pneumonia during therapy
Generalized Megaesophagus
ME as part of generalized weakness
Causes:• Congenital myopathy, neuropathy,
junctionopathy• Hypothyroidism• Hypoadrenocorticism• Muscular dystrophy• Dysautonomia – more common in cats
Generalized Megaesophagus
ME as part of generalized weakness
Causes:• Immune mediated disease
– Systemic Lupus Erythematosis– Dermatomyositis– Polymyositis
• Giant axonal neuropathy - GSD• Congenital myasthenia gravis
Generalized Megaesophagus
ME as part of generalized weakness
Causes:
• Hereditary myopathy of Labradors
• Lead toxicity
• Thallium toxicity
• Organophosphate toxicity
Vomiting, Regurgitation, Coughing
Time with respect to eating
Vomiting• Minutes to hours after eating
Regurgitation• Minutes to hours after eating
Coughing & gagging• Not related to eating• But can be precipitated by drinking water

Vomiting, Regurgitation, Coughing
Expulsion Process
Vomiting• Active – abdominal contractions
Regurgitation• More passive• Can be confusing – regurgitation can cause gagging and then
retching, and then vomiting
Coughing & gagging• After coughing• Can be confusing – productive cough can cause gagging and
then retching, and then vomiting

Vomiting, Regurgitation, Coughing
Premonitory signs
Vomiting• Salivation, pacing, licking lips, anxiety
Regurgitation• Salivation, exaggerated swallowing
Coughing & gagging• Elevated respiratory rate

Vomiting, Regurgitation, Coughing
Vomiting Regurgitation CoughingHardly digested to
liquidHardly digested to
liquidWhite and foamy
Smell variable May smell sour and fermented
Not usually foul smelling
Rarely has mucus Often is slimy with mucus
May contain mucus or pus
Digested blood suggests vomiting
Blood is rare May be blood tinged
May contain bile Never bile stained Never bile stained
Clues in the History - ME
Signs of Aspiration PneumoniaCoughingFeverDyspneaCyanosis
Can have coughing without regurgitationCoughing can be due to pressure of enlarged esophagus
on the trachea
SUSPECT MEGAESOPHAGUS IN AN OLDER DOG WHO IS BOTH “VOMITING” AND COUGHING

Clues in the History - ME
Weight lossCan be severe
Neurologic deficits – LMN SignsDepressed spinal and cranial nerve reflexesLarge, easily expressed bladderConstipation
Muscular abnormalitiesMuscle atrophy with generalized weaknessMuscle pain with polymyositis

Clues in the History - ME
Signs of myasthenia gravisWeakness worsens with exerciseChange in barkingDifficulty eating or swallowingWeak or absent palpebral reflex – fatigues
Signs of hypoadrenocorticismVomiting and diarrhea (especially with blood)Lethargy and weaknessShock if severe

Clues in the History - ME
Signs of hypothyroidismObesitySymmetrical alopeciaDry eyePyoderma
Signs of lead toxicityVomiting and diarrheaSeizures, dullness, behavior changes, apparent
blindness

Clues in the History - ME
Signs of immune mediated disease
Muscle pain - polymyositis
Joint pain or swelling - polyarthritis
Anemia - IMHA
Thrombocytopenia – ITP
Skin or mucous membrane lesions
Fever
Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs
• Survey rads may be normal
• Survey rads may show a gas filled esophagus
• You may need to do both right and left laterals to see air in the esophagus
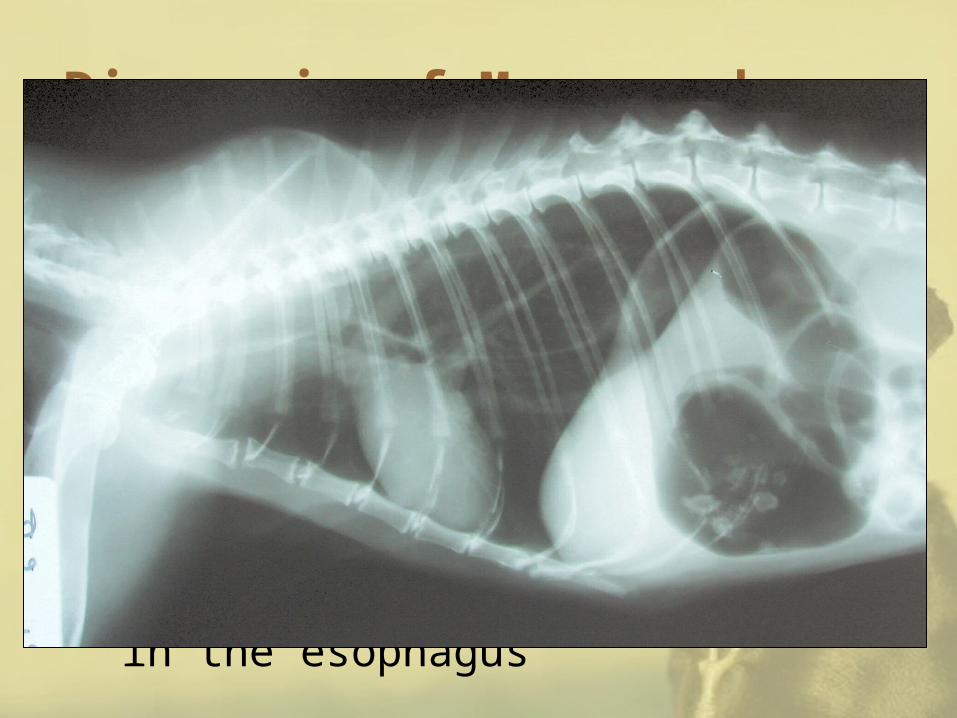
Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Barium Esophagram• Normal esophagram shows lines only

Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Barium Esophagram• Normal esophagram shows lines only

Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Barium Esophagram• Normal esophagram shows lines only• Barium will pool in the esophagus if ME

Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Barium Esophagram• Normal esophagram shows lines only• Barium will pool in the esophagus if ME

Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Barium Esophagram• Normal esophagram shows lines only• Barium will pool in the esophagus if ME• Can assess wall thickness• May see filling defect of radiolucent foreign
body, ulcer, or mass• Can sometimes see a herringbone pattern in
the distal feline esophagus, due to mucosal folds
Diagnosis of Megaesophagus
The test that most often diagnoses MERadiographs – Barium EsophagramProcedure:• Administer 5-20 ml barium paste, liquid or
barium coated food• Paste gives the best coating, but can be
dangerous if aspirated• If motility problem with good tone, it may take
barium coated food to see abnormalities***WARN OWNER OF DANGER OF THIS
PROCEDURE***
Diagnosis of Megaesophagus
The test that most often diagnoses ME
Radiographs – Survey Abdominal
• May see radiopaque foreign body if heavy metal poisoning
• May see a gas filled stomach if generalized GI motility disorder
• May see displaced pylorus of chronic gastric volvulus.
Diagnosis of Megaesophagus
The test that most often diagnoses ME
Fluoroscopy• The best way to evaluate mild to moderate
esophageal hypomotility• 5-20 cc liquid barium per bolus first• Then liquid barium mixed with canned food• Then liquid barium coated kibble• Strictures may show no abnormalities with
liquid barium bolus

Diagnosis of Megaesophagus
Minimum database for ME
CBC
General health profile
Electrolytes and venous blood gases
Urinalysis
Fecal flotation and direct wet mount
Thoracic and cervical radiographs

Diagnosis of Megaesophagus
Patterns in Minimum database
CBCAspiration pneumonia• Neutrophilia with left shift• Activated lymphocytes and monocytesImmune mediated disease (rare)• Absolute reticulocute count 300,000• HCT 16%• Spherocytes

Diagnosis of Megaesophagus
Patterns in Minimum Database
SerologyHypothyroidism• Elevated triglycerides• Elevated cholesterolHypoadrenocorticism• Azotemia (elevated BUN, creat, phos)• Hypercalcemia• Hyperkalemia

Diagnosis of Megaesophagus
Patterns in Minimum Database

Diagnosis of Megaesophagus
Patterns in Minimum Database
Fecal Examination
Standard sugar and salt flotation solutions will not give great yields of Spirocerca lupi larvated eggs
Sodium nitrate or direct wet mount is often more sensitive
Diagnosis of Megaesophagus
Tests indicated in every dog and cat with ME
Thyroid panel• Dog – TSH, T4, freeT4• freeT4ED is indicated if T4 is low, to rule out antithyroid
antibodiesACTH stimulation test• **Different protocols for dogs and cats**Myasthenia gravis titer• Comparative Neuromuscular Laboratory, UC-Davis
Getting a positive test result on one of the above should not preclude testing for the others.
A significant number of ME patients have 2 or even all 3 of these problems concurrently

Diagnosis of Megaesophagus
Ancillary tests for ME
Abdominal ultrasoundElectrodiagnostics – EMG, NCVMuscle and nerve biopsy **RISKY**Blood Lead levelOrganophosphate toxicology screenTensilon testANA (rarely helpful)
Treatment of Megaesophagus
Elevated Feedings
THE PRIMARY TREATMENT IF THE ANIMAL IS TO BE FED BY MOUTH
MAKE SURE YOU SPEND ENOUGH TIME WITH THE OWNER TO FULLY EXPLAIN THIS, AS THEIR PET’S LIFE CAN DEPEND ON IT

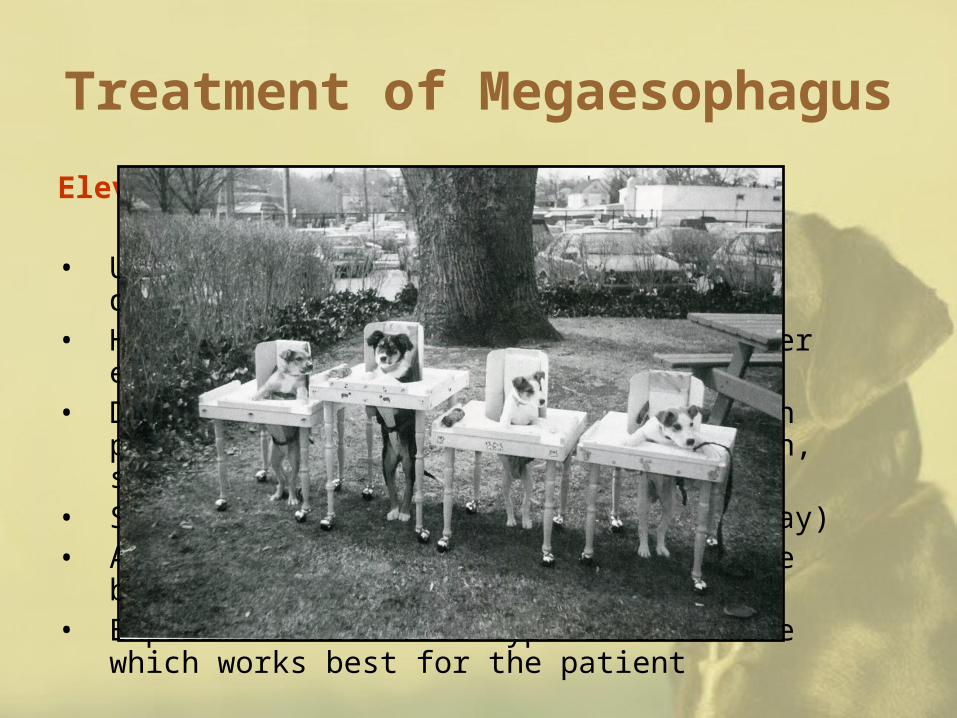
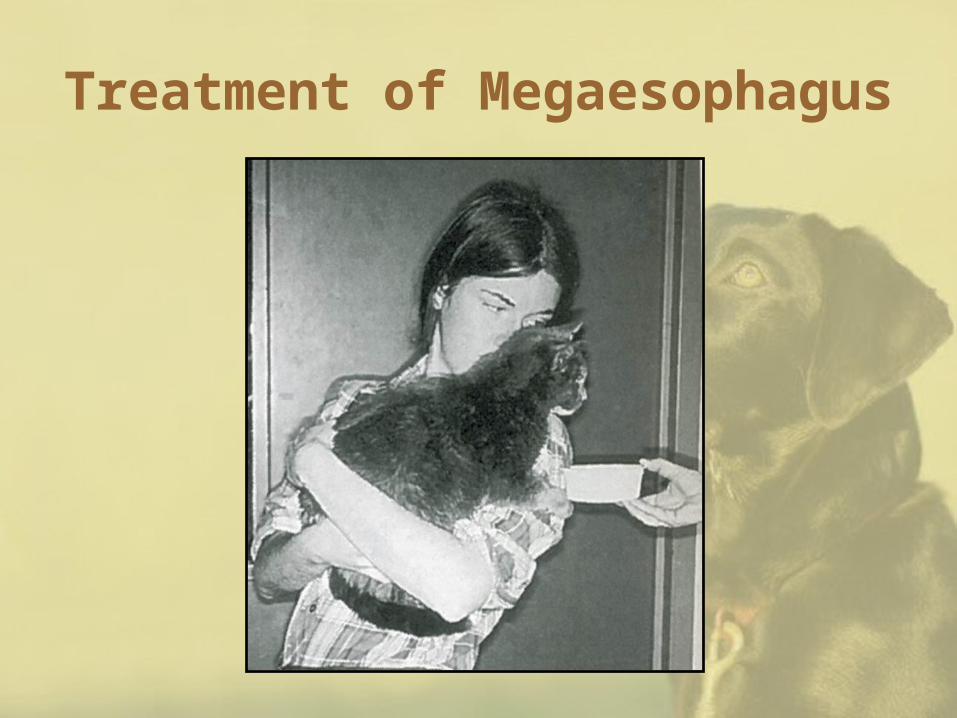
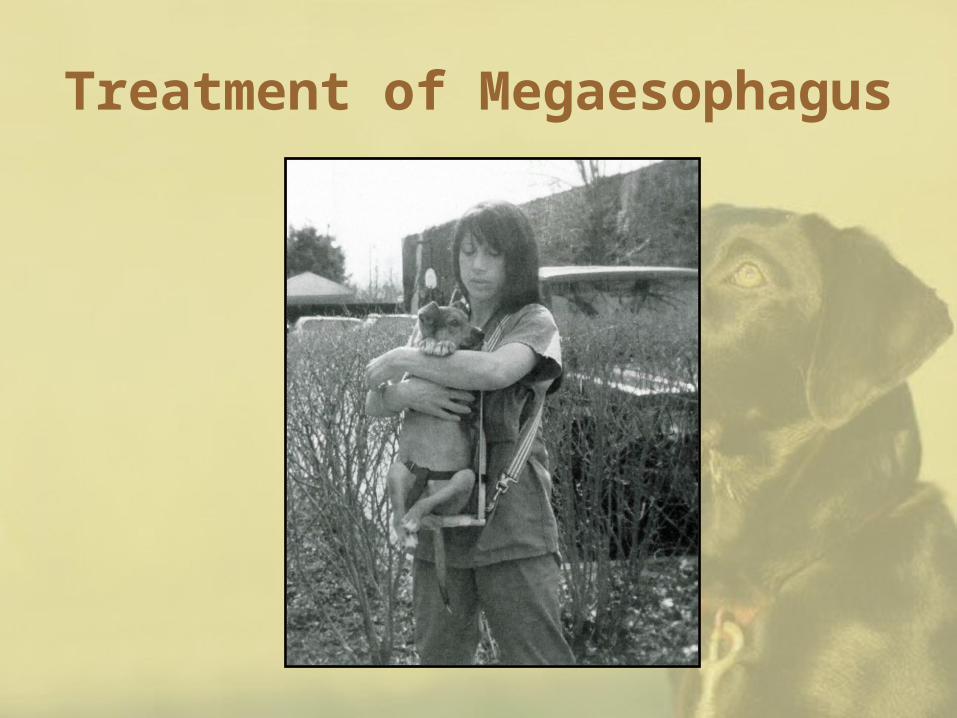
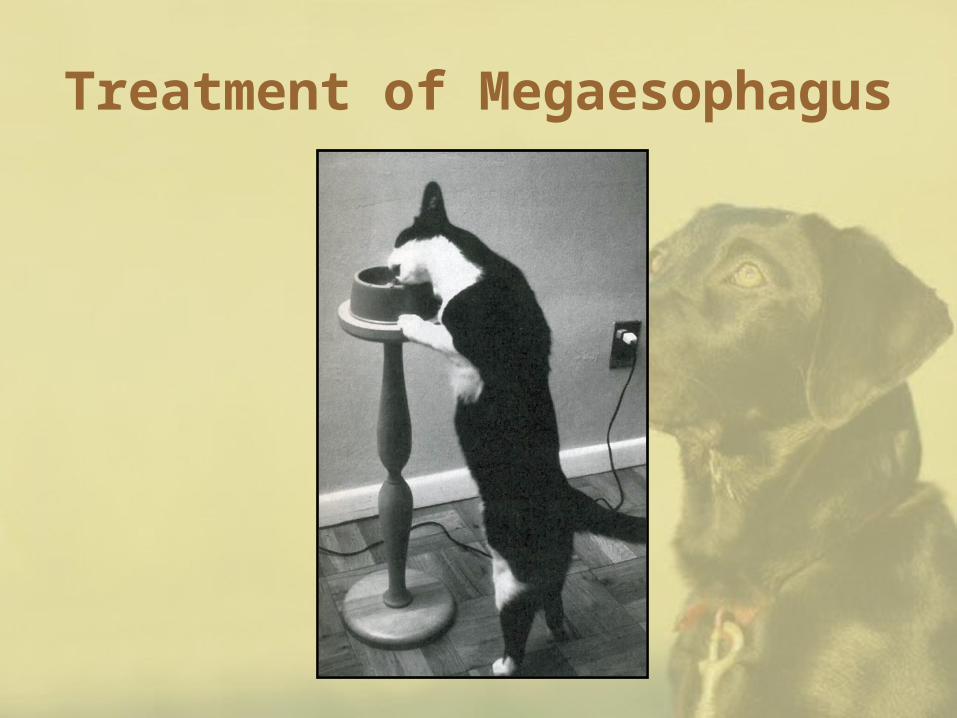
Treatment of MegaesophagusElevated Feedings• Upper body should be elevated 45-90 degrees.• Hold this position for 10 minutes after eating• Do this also prior to periods of known
prolonged lateral recumbency (sedation, sleeping)
• Small frequent meals (2-4 or more a day)• Avoid feeding for several hours before bedtime• Experiment with food type to determine which
works best for the patient• Lots of how to videos on www.youtube.com • “Bailey Chair”

Treatment of Megaesophagus
Elevated Feedings
• Upper body should be elevated 45-90 degrees.• Hold this position for 10 minutes after eating• Do this also prior to periods of known
prolonged lateral recumbency (sedation, sleeping)
• Small frequent meals (2-4 or more a day)• Avoid feeding for several hours before bedtime• Experiment with food type to determine which
works best for the patient

Treatment of Megaesophagus
Elevated Feedings
• Upper body should be elevated 45-90 degrees.• Hold this position for 10 minutes after eating• Do this also prior to periods of known
prolonged lateral recumbency (sedation, sleeping)
• Small frequent meals (2-4 or more a day)• Avoid feeding for several hours before bedtime• Experiment with food type to determine which
works best for the patient
Treatment of Megaesophagus
Elevated Feedings
• Upper body should be elevated 45-90 degrees.• Hold this position for 10 minutes after eating• Do this also prior to periods of known
prolonged lateral recumbency (sedation, sleeping)
• Small frequent meals (2-4 or more a day)• Avoid feeding for several hours before bedtime• Experiment with food type to determine which
works best for the patient

Treatment of Megaesophagus

Treatment of Megaesophagus

Treatment of Megaesophagus

Treatment of Megaesophagus

Treatment of Megaesophagus
Treatment of Megaesophagus
Treatment of Megaesophagus
Treatment of Megaesophagus
Treatment of Megaesophagus

Treatment of Megaesophagus

Treatment of Megaesophagus
Tube Feeding
Temporary gastrostomy • can help stabilize until megaesophagus can be
improved, it the cause is treatable• Often required for 1-3 months• Medications given by tube are more assured of
absorption• NEVER GIVE DOXYCYCLINE BY MOUTH TO
A PATIENT WITH ME• extremely helpful for aspiration pneumonia

Treatment of Megaesophagus
Tube Feeding
Permanent gastrostomy • Place a Pezzar tube first• When stoma is well healed, replace with low
profile gastrostomy tube• Medications given by tube long term• Owners have to be vigilant to keep their pets
from taking in food by mouth• If they do take food PO, they need to keep the
pet’s front end elevated for 10 minutes.
Treatment of Megaesophagus
Prokinetics
• Metoclopramide and cisapride - empty the stomach faster to minimize GER and regurgitation
• Cisapride – may actually improve esophageal function
– Seems to work more consistently in cats– Response in dogs varies from dramatically
positive to no response

Treatment of Megaesophagus
Treat aspiration pneumonia
• Broad spectrum antibiotics – gram negatives, positives and anaerobes
– Long term therapy might be needed for chronic recurring aspiration pneumonia
– Choose 3-4 that work and rotate q6-8 weeks
• IV fluid therapy – overhydration to keep respiratory secretions coming up
• Coupage• + Nebulization• Gastrostomy tube• NPO – including medications

Treatment of Megaesophagus
Treat esophagitis – 2 weeks after resolution of clinical signs
• Sucralfate - PO– Do not give within 2 hours of any other PO meds
• Prokinetics• H2 blockers• Proton pump blockers

Treatment of Megaesophagus
Immunosuppression – SKEERY!!
• Might be indicated for:– Myasthenia gravis– SLE– Polymyositis
• Only when IM disease has been confirmed, or as a last resort.
• Dangerous for those with aspiration pneumonia
• Some patients with MG can decompensate when immunosuppressed

Treatment of Megaesophagus
Immunosuppression – SKEERY!!
• Drugs:– Prednisone
• Start at 0.25 mg/lb/day and gradually increase to immunosuppression if tolerated
– Azathioprine• Start at 0.5 mg/kg PO SID, and then double if tolerated
• Eventually wean down to the lowest effective dose over 2-3 months
• Those who respond to immunosuppression may be able to be weaned off Mestinon
• Use MG titer to know how long to continue therapy– Begin the weaning process when titer negative– Check monthly to make sure not weaning too fast

Megaesophagus - Prognosis
Severe dilation often carries a poor prognosis, no matter the cause
Spirocerca – rarely can be effectively treatedAcquired idiopathic megaesophagus carry a variable
prognosis, depending on:• Use of permanent gastrostomy• Response to cisapride• Tendency to develop aspiration pneumoniaCongenital megaesophagus• Guarded in general• Occasionally a puppy will have resolution at 6-12
monthsAll patients with ME are at risk for sudden death due to
aspiration and respiratory obstruction

Handouts
• PowerPoint Presentation – behind the white tab• Instructions for Adrenal Testing in Dogs and
Cats• Lab Submission Forms
– TAMU GI Lab Endocrine Submission Form– Comparative Neuromuscular Laboratory Submission
Form and submission instructions• Client Drug Handouts
– Azathioprine– Prednisone– Pyridostigmine
• Client Information Handout– Hiatal Hernia– Megaesophagus







