

PTC
Primary Trauma
Care

PTC
PTC System
Prevention
Triage
Primary survey
Secondary survey
Stabilisation
Transfer
Definitive care
PTC
What is PTC
Primary Trauma Care
is a 2 day course followed by a one
day instructors’ course,
training doctors and nurses in the
acute management of the severely
injured patient

PTC
PTC Mission Statement
• To train doctors & nurses to treat
severely injured patients quickly &
systematically
• To use what equipment is available, to
prioritise and treat patients safely
• To train clinicians to teach PTC
principles in their hospitals

PTC
Objectives of a PTC
2 day course
- demonstrate the systematic assessment
& treatment of the severely injured
patient
- to train you in the knowledge, skills and
attitudes of the PTC principles
- To consider how these PTC principles
can be adapted to your hospital
PTC
PTC system
Prevention
PTC
PTC system
Triage
Sorting patients according to priority
Priority depends on
• experience
• resources
• severity of injury

PTC
PTC systemPrimary & Secondary Survey
History
Examination
• Look (Inspection)
• Feel (Palpation)
• Listen (Auscultation)
Special Investigations if available

PTC
PTC system
Stabilisation Includes
• Re-assessment
• Optimisation بهینه سازی
• Documentation
• Immunisation
When stable
Transfer for definitive care
PTC
PTC System

PTC
PTC SystemSummary
PTC offers
• a systematic approach
• rapid assessment and
treatment of the injured patient
• adaptability to all healthcare
environments

PTC
Primary Survey
Objectives
• To introduce the elements of
the Primary Survey
• To understand when to perform
the Primary Survey
PTC
Primary Survey
• Rapid sequential look
• 2 minutes
• Treat as you find
• Repeat if at any time unstable

PTC
Primary Survey
• Airway
• Breathing
• Circulation
• Disability
• Exposure
PTC
AirwayAssessment
• Look, listen, feel
• Colour
• Conscious state
• Accessory muscle use
PTC
AirwayBeware
• Airway obstruction
• Chest injuries with breathing difficulties
• Cervical spine injury
PTC
AirwayManagement
• Clear mouth
• Chin lift/jaw thrust
• Guedel / Nasopharyngeal airway
• Intubation
• Cervical spine care

PTC
BreathingAssessment
• Air movement
• Respiratory rate
PTC
Breathing
Beware
• Tension pneumothorax
• Massive haemothorax
• Open pneumothorax
• Flail chest
• Lung contusion

PTC
BreathingManagement
• Oxygen (if available)
• Artificial ventilation
• Decompress pneumothorax
• Drain haemothorax
PTC
CirculationAssessment
• Cardiac output
• Blood volume
• External haemorrhage
PTC
CirculationBeware
• Intra-abdominal injury
• Intra-thoracic injury
• Long bone fracture
• Pelvic fracture
• Penetrating injury
• Scalp wounds
PTC
CirculationManagement
• Stop bleeding
• Large bore intravenous access x 2
• Blood for crossmatch and Hb
• Administer IV fluid

PTC
Disability
• Pupils
• Check awareness
• A Awake
• V Responds to verbal command
• P Responds to pain
• U Unresponsive

PTC
Exposure
• Undress for thorough
assessment
• Prevent hypothermia

PTC
Primary SurveyX-Rays ( if available)
Cervical spine (lateral)
Chest
Pelvis

PTC
Reassessment of
ABCDE
If patient is, or becomes,
unstable

PTC
Primary Survey
PTC
Primary SurveySummary
• Rapid sequential look
• 2 minutes
• Treat as you find
• Repeat at any time if unstable
PTC
Airway and
Breathing
Objectives
• To understand the structured approach to airway and breathing
• To recognise and manage common airway and breathing problems
PTC
Airway Management
• First priority is a patent airway
• Talk to the patient
• Give oxygen (if available)
• Assess the airway
• Cervical spine
PTC
Airway Assessment
• Look
• Listen
• Feel
• Colour
• Respiratory
distress
• Conscious state
• Chest movement
• Breath sounds
• Respiratory
distress
PTC
Airway Assessment Signs Of Obstruction
• Snoring or gurgling
• Stridor
• Agitation (hypoxia)
• Use of accessory muscles
• Paradoxical chest movement
• Cyanosis
PTC
Airway ManagementBasic Techniques
• Chin lift
• Jaw thrust

PTC
Airway ManagementAdjuncts
• Oropharyngeal airway
• Nasopharyngeal airway
PTC
Airway ManagementAdvanced Techniques
• Endotracheal intubation
• Surgical Cricothyroidotomy

PTC
Endotracheal Intubation
if:
• Failure to maintain an airway by other means
• Failure of ventilation by other means
Consider:
Risk of aspiration
Control CO2 (eg head injury)
PTC
Remember
1. Cervical spine
2. Patients die from lack
of oxygen not lack of an
ETT
PTC
Surgical Cricothyroidotomy
Consider if:
• Intubation attempted and failed
and still needed
• Patient cannot be ventilated
PTC
Breathing
(Ventilation)
PTC
BreathingAssessment
• Inspection (LOOK)
• Palpation (FEEL)
• Auscultation (LISTEN)
• Resuscitate
PTC
Breathing Look
• Respiratory rate
• Accessory muscle use
• Cyanosis
• Penetrating injury
• Flail chest
• Sucking chest wound
PTC
Breathing Feel
• Tracheal shift
• Rib fractures
• Subcutaneous emphysema
• Percussion
PTC
BreathingListen
• Breath sounds
• Heart sounds
• Bowel sounds

PTC
Tension PneumothoraxSigns
• Respiratory distress
• Tachycardia
• Hypotension
• Distended neck veins
• Resonant percussion note
• Tracheal deviation
• Air entry

PTC
Tension Pneumothorax Management
• Immediate decompression
• Large bore needle
• Second intercostal space
• Mid clavicular line
• Formal chest drain must follow

PTC
Tension Pneumothorax
• Should be a clinical diagnosis
• Treat before X-ray
PTC
BreathingManagement
• High flow oxygen if available
• Assist ventilation if necessary
• Treat pneumothorax +
haemothorax
PTC
Airway and Breathing

PTC
Airway and Breathing
Summary
• Open the airway
• Consider intubation
• Do not forget cervical spine
• Oxygen if available
• Assist ventilation as required
PTC
Circulation
Objectives
• To understand the structured approach to circulation problems
• To recognise and manage shock

PTC
CirculationAssessment
• Blood pressure
• Heart rate
• Capillary refill
• Peripheral temperature
• Peripheral colour
• Urine output

PTC
Shock
• Inadequate organ perfusion and
tissue oxygenation
• Most often due to hypovolaemia
in trauma

PTC
Circulation Types of shock
Hypovolaemic
Cardiogenic
Neurogenic
Septic
Anaphylactic
PTC
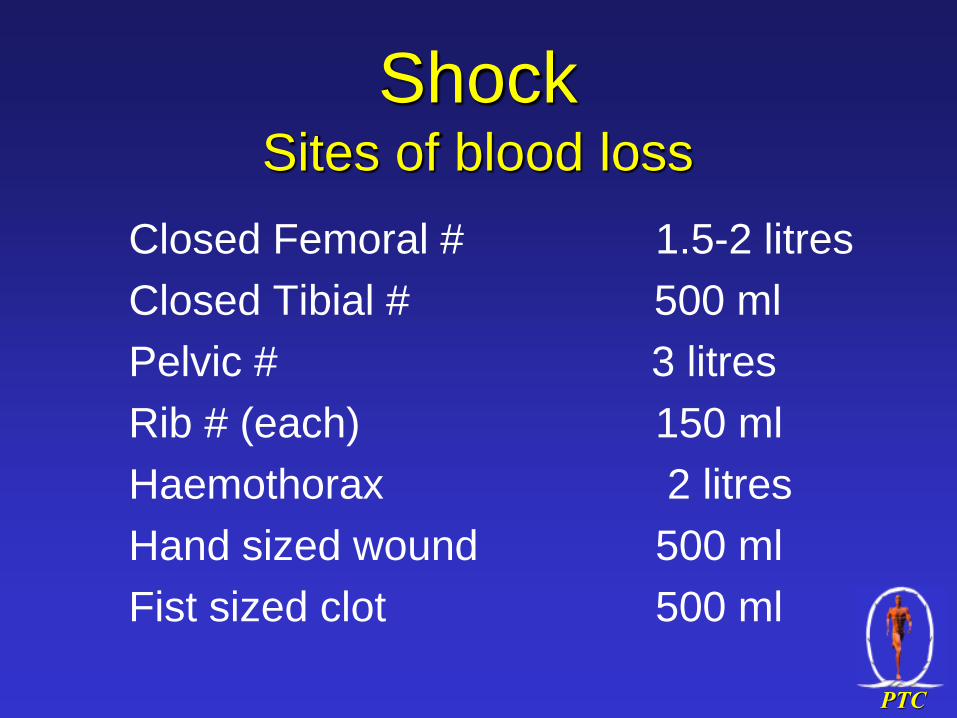
ShockSites of blood loss
Closed Femoral # 1.5-2 litres
Closed Tibial # 500 ml
Pelvic # 3 litres
Rib # (each) 150 ml
Haemothorax 2 litres
Hand sized wound 500 ml
Fist sized clot 500 ml

PTC
Shock
Concealed blood loss
• Abdominal Cavity
• Pleural Cavity
• Femoral Shaft
• Pelvic Fractures
• Scalp (children)

PTC
Types of Bleeding
• Compressible
- usually peripheral
• Non-compressible
- e.g. intra-abdominal
- Surgery required

PTC
ShockClinical Signs
• Altered mental state : anxiety to coma
• Pulse present ?
- radial systolic > 80 mmHg
- femoral systolic >70 mmHg
- carotid systolic > 60 mmHg
• Tachycardia
• Pulse pressure narrowed
PTC
ShockClinical Signs
• Skin - cold, pale, sweaty, cyanosed
• Capillary refill time > 2 seconds
• Blood pressure
• JVP
• Urine output < 0.5 ml/kg/hr
• Respiratory rate
PTC
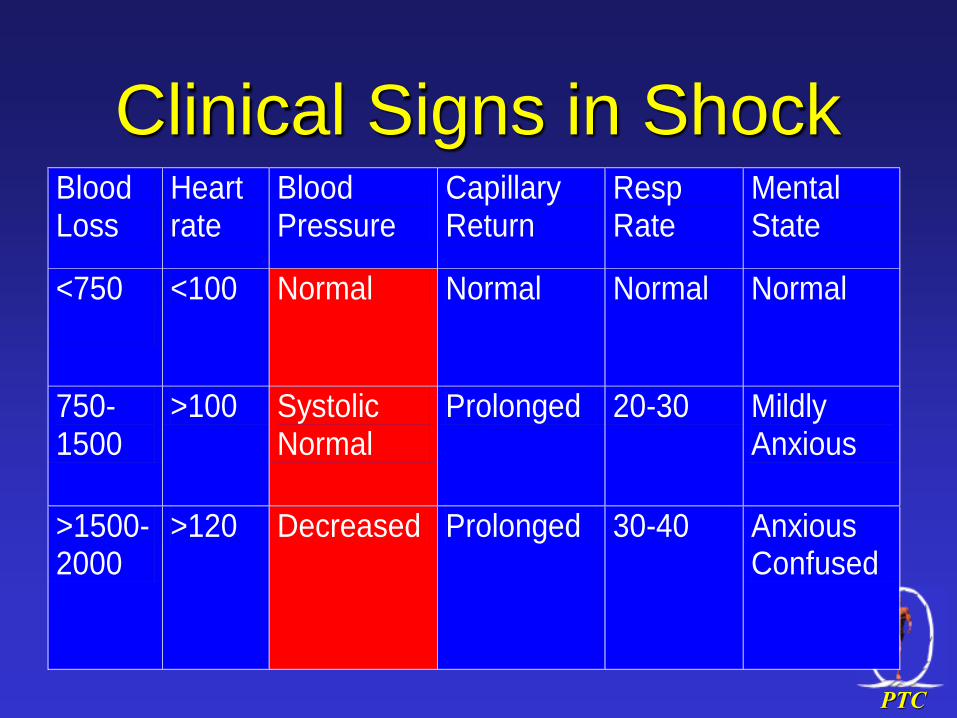
Clinical Signs in Shock Blood Loss
Heart rate
Blood Pressure
Capillary Return
Resp Rate
Mental State
<750
<100 Normal Normal Normal Normal
750-1500
>100 Systolic Normal
Prolonged 20-30 Mildly Anxious
>1500-2000
>120 Decreased Prolonged 30-40 Anxious Confused
PTC
Blood Loss < 750ml
Heart rate <100
Blood pressure normal
Capillary refill normal
Respiratory rate normal
Mental state normal

PTC
Blood loss 750-1500ml
Heart rate >100
Blood pressure systolic normal
Capillary refill prolonged
Respiratory rate 20-30
Mental state mild concern
PTC
Blood loss >1500ml
Heart rate >120
Blood pressure decreased
Capillary refill prolonged
Respiratory rate >30
Mental state axious/confused/coma

PTC
Cardiogenic Shock
• Myocardial contusion
• Cardiac tamponade
• Tension pneumothorax
• Penetrating wound of heart
• Myocardial infarction

PTC
Circulation Management
• A + B, oxygen (if available)
• Two large bore i/v cannulae
• Stop obvious bleeding
• Fluid replacement
• Maintain temperature
• Analgesia

PTC
CirculationStop bleeding
• Chest
• Drain tube and re-expand lung
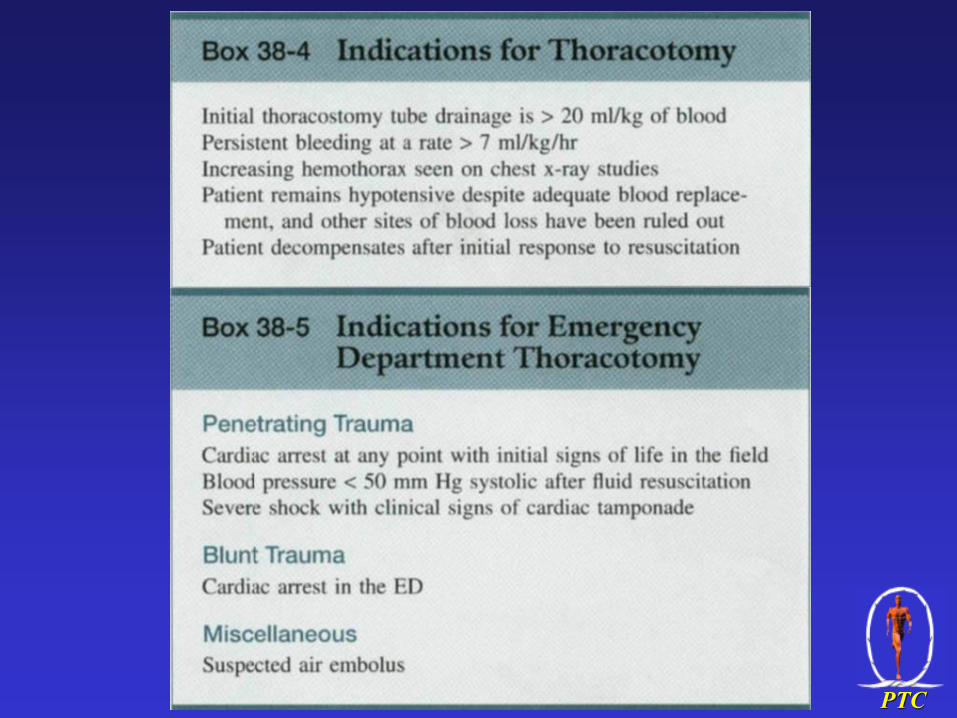
• Emergency thoracotomy rarely
• Abdomen
• Laparotomy if hypotensive after fluids
• Limbs
• Pressure dressing
• Tourniquet last resort

PTC
CirculationFluid replacement
• Warm fluids if possible
• Colloids or crystalloids?
• Consider hypotensive resuscitation if
haemostasis not secure
• Consider oral resuscitation

PTC
CirculationFluid replacement - How much?
1000-2000ml 0.9% Saline or Ringer’s
Reassess
1000-2000ml 0.9% Saline or Ringer’s
Reassess
Consider blood
Consider surgery
Aim for systolic BP>90 + HR <100
PTC
Circulation
Consider blood transfusion if:
• Haemodynamic instability in spite of
fluids
Haemoglobin <7g/dl and patient still
bleeding

PTC
Circulation

PTC
Circulation
Summary
• Careful assessment
• Stop the bleeding
• Replace volume

PTC
Secondary Survey
Objectives
• To understand how and when to
perform the secondary survey

PTC
Secondary Survey
• Thorough head to toe examination
• On completion of primary survey
• When ABC’s are stable
• Aim to find any injury that may threaten life or limb
• Return to primary survey if any deterioration

PTC
Secondary SurveyHead examination
• Scalp (bruising, lacerations)
• Skull (tenderness, depression)
• Eyes (pupils, fundi, lens, conjunctiva)
• CSF or blood from ear, nose, mouth
PTC
Secondary SurveyNeck
• Assume neck is injured
• Immobilise in neutral position
PTC
Secondary SurveyNeck
• Penetrating wounds
• Subcutaneous emphysema
• Tracheal deviation
• Neck veins
PTC
• Glasgow Coma Score
• Motor Function
• Sensation
• Reflexes
Secondary SurveyNeurological examination

PTC
Secondary SurveyChest
• Inspection
• Palpation
• Percussion
• Auscultation
• CXR (if not done, and if possible)
• ECG ( if available)

PTC
• Potentially Difficult
• Beware “hidden haemorrhage”
• Look, listen, feel
• Remember rectal examination
Secondary SurveyAbdomen

PTC
Secondary SurveyAbdomen
• Penetrating wound surgical
exploration
• Blunt trauma - naso/orogastric tube
• Urinary Catheter if no meatal blood
• Reassess frequently
PTC
Secondary SurveyExtremities
• Look : deformity, bruising, laceration
• Feel : tenderness, pulses
• Remember compartment syndrome

PTC
Secondary Survey
Don’t forget the back!
PTC
Secondary SurveyLog Roll
• 4 people
• Airway/neck controller in charge
• Clear timing and instructions
• Allows back examination

PTC
Secondary SurveyX-Rays
• In secondary survey if not already
done
• Chest
• Cervical spine - all 7 vertebrae + T1
• Pelvis
• Others as indicated by examination
PTC
Secondary Survey
PTC
Secondary Survey
Summary
• Thorough head to toe examination
• Return to primary survey if any
deterioration
• Don’t forget the back
PTC
Chest Injuries
Objectives
• Recognise common life threatening chest injuries
• Understand principles of management of chest injuries

PTC
Chest InjuriesInitial assessment
Airway
Breathing
Circulation

PTC
Chest Injuries
• Cause of ~25% of trauma deaths
• Immediate deaths due to major
disruption of heart and great
vessels
• Early deaths due to airway
obstruction, cardiac tamponade or
aspiration

PTC
Chest Injuries
• Pneumothorax (simple, tension, open)
• Haemothorax
• Pulmonary contusion
• Rib fractures
• Flail chest
• Pericardial tamponade
• Myocardial contusion

PTC
Chest InjuriesTension Pneumothorax
• Air enters the pleural space but cannot leave
• Intrathoracic pressure
• Mediastinal shift
• venous return + cardiac output
• Respiratory distress and hypoxia
PTC
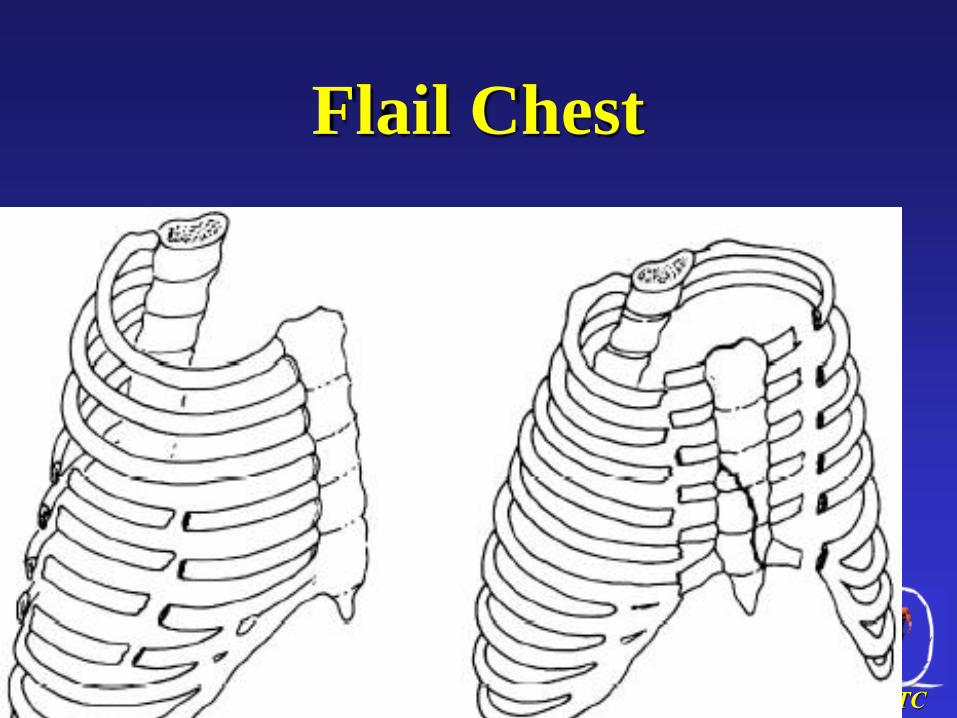
Flail Chest
PTC
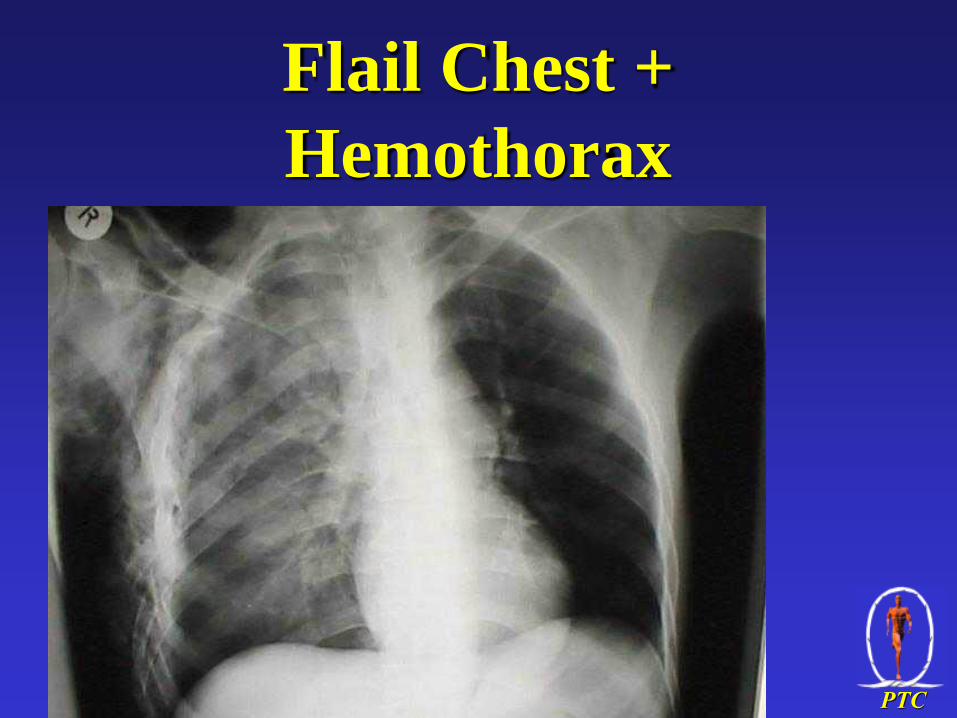
Flail Chest +
Hemothorax

PTC
• Chest InjuriesFlail Chest
• Unstable segment
• Paradoxical movement with ventilation
• May severe respiratory distress
Adequate analgesia vital
• Give oxygen (if available)
• Consider intubation and IPPV

PTC
Flail Chest• Free floating segment of ribs
• 3 or more rib fx.s broken in 2 places
• Look for paradoxical chest wall motion
• Inhaleinward
• Exhaleoutward
• Decreased air entry
PTC
Flail Chest• Stabilization of the flail segment by
positioning the person with the injured side down or placing a sand hag on the affected segments
• .

PTC
Flail Chest
• Oxygen
• Cardiac & oximetry monitors if available
• Analgesia & intercostal nerve block
• Restrict IV fluids.
• Observation for signs of an associated injury such as tension pneumothorax
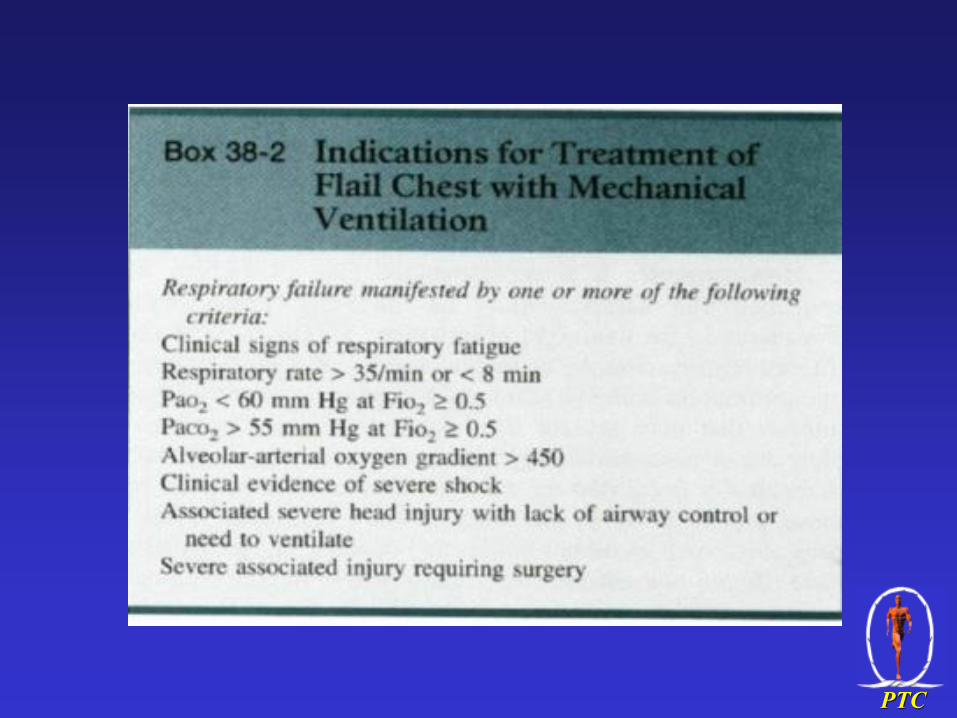
• Ventilatory support: shock, 3 or more injuries, head injury, pulmonary disease, 8 or more fx.’s, >65 yrs
PTC
PTC
Chest Injuries
Tension Pneumothorax
• Life threatening emergency
• Clinical diagnosis
• Urgent decompression
PTC
Tension PneumothoraxSigns
• Respiratory distress
• Tachycardia
• Hypotension
• Distended neck veins
• Resonant percussion note
• Tracheal deviation
• air entry

PTC
Tension PneumothoraxManagement
• Immediate decompression
• Large bore needle
• Second intercostal space
• Mid clavicular line
• Formal chest drain to follow
PTC
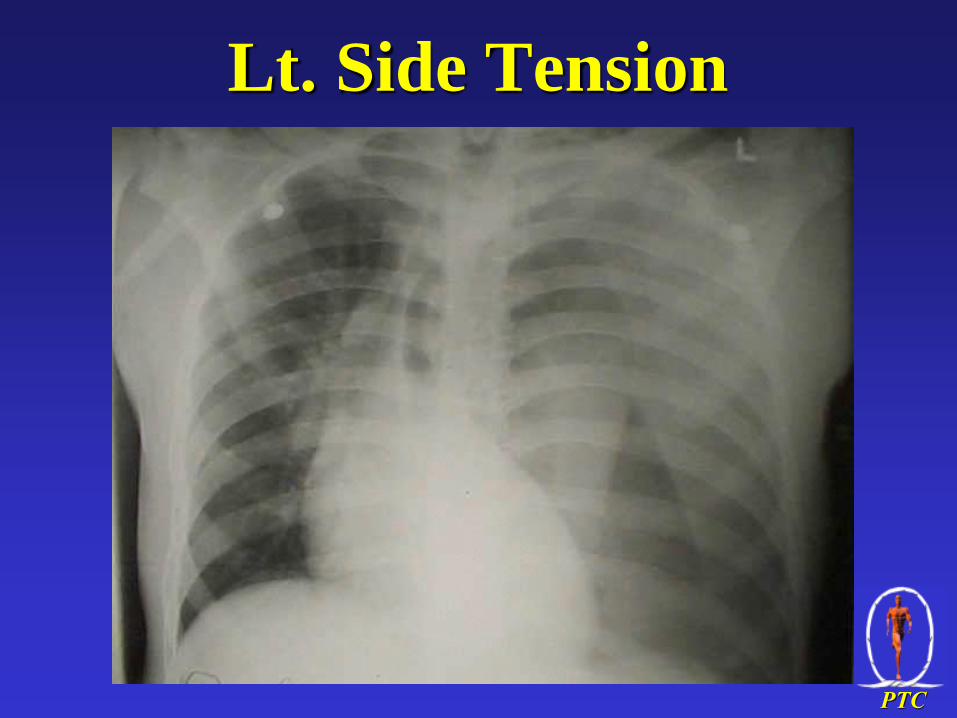
Lt. Side Tension
Pneumothorax
PTC
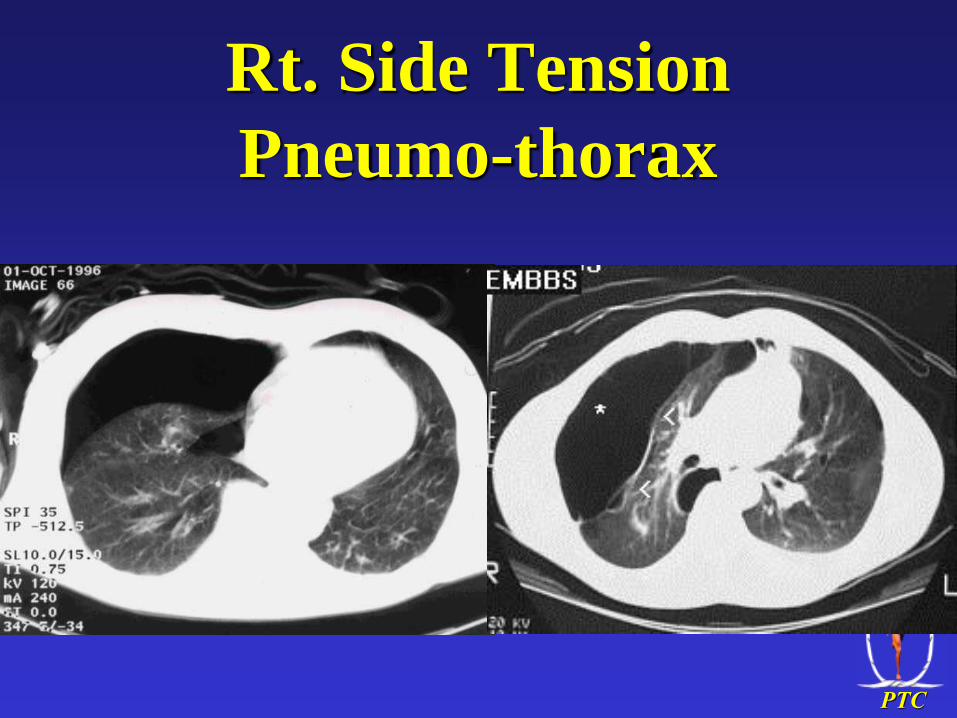
Rt. Side Tension
Pneumo-thorax
PTC
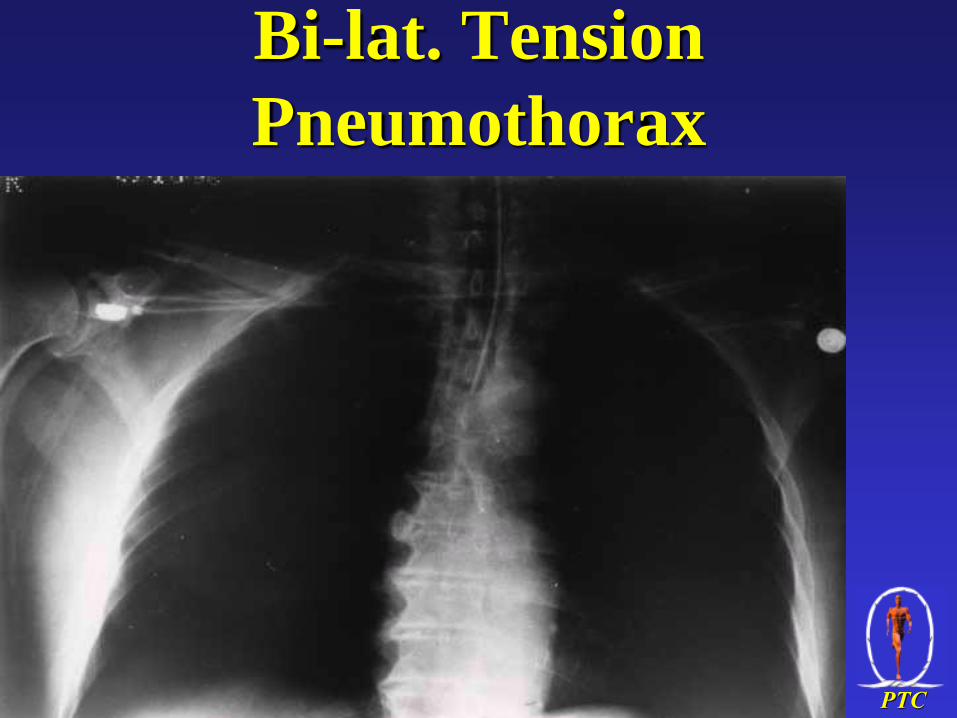
Bi-lat. Tension
Pneumothorax

PTC
Needle Decompression
PTC
Chest InjuriesSimple Pneumothorax
• X-Ray to confirm and size
• Chest drain
• Treat if considering IPPV

PTC

PTC

PTC
Open
(Communicating)
Pneumothorax
(Sucking Chest
Wound)

PTC
Chest InjuriesOpen Pneumothorax
• “Sucking” chest wound
• Other signs of pneumothorax
present
• Occlude wound (3 sides only)
• Air escapes on expiration
• Urgent insertion of chest drain

PTC
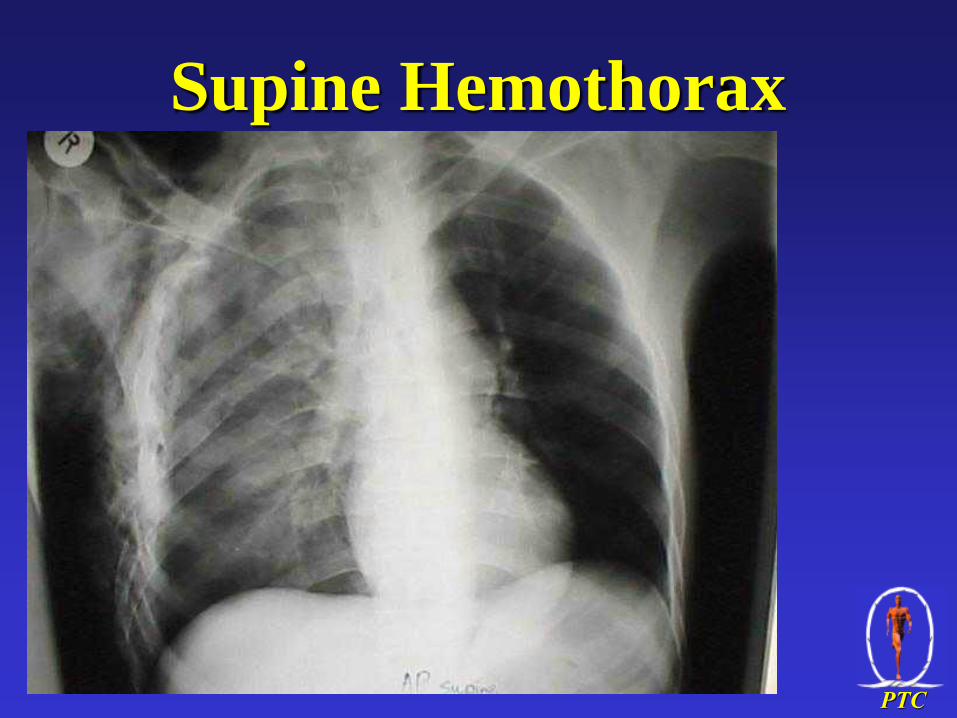
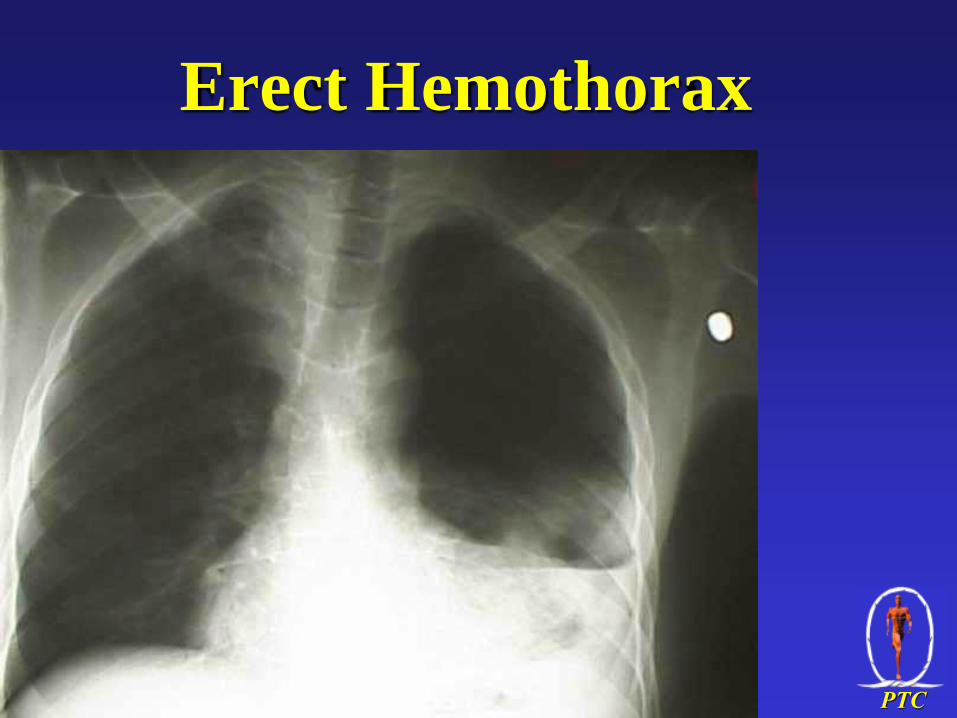
Chest InjuriesHaemothorax
• Commoner in penetrating than in blunt trauma
• May Hypovolaemic shock
• Large bore chest drain
• Lung re-expansion may stop bleeding
• Consider thoracotomy if bleeding continues > 200-300 ml/hr
PTC
Supine Hemothorax
PTC
Erect Hemothorax

PTC
Lt. subclavian Artery
Stab

PTC
Indications for Closed-tube
Thoracostomy
• Traumatic cause of the pneumothorax
• Moderate-to-large pneumothorax
• Respiratory symptoms regardless of the size of the pneumothorax
• Increasing size of the pneumothorax after initial conservative therapy
PTC
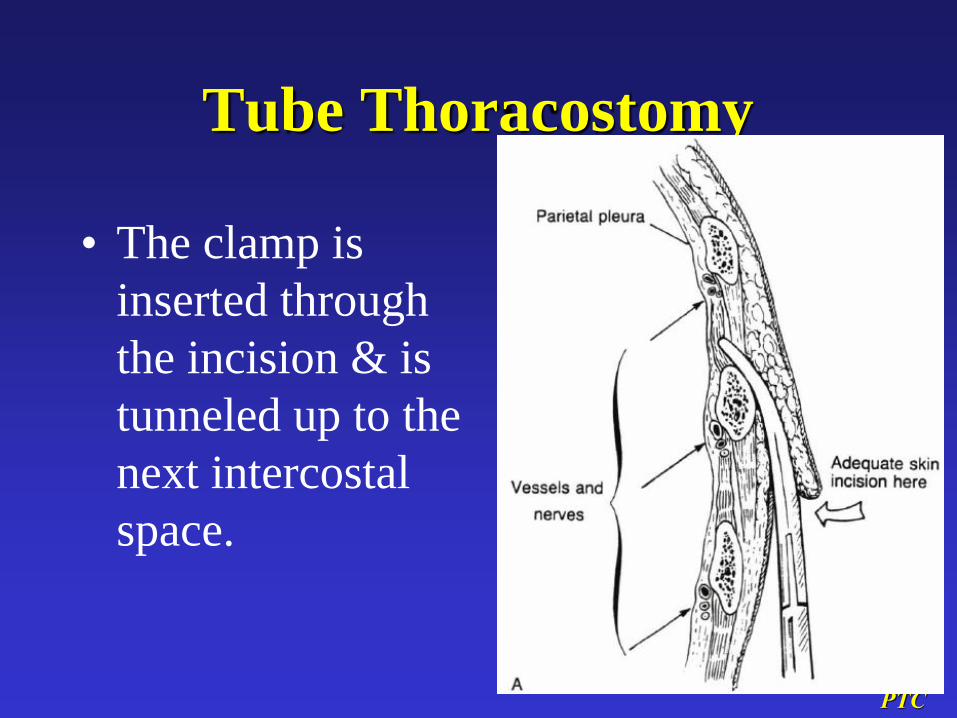
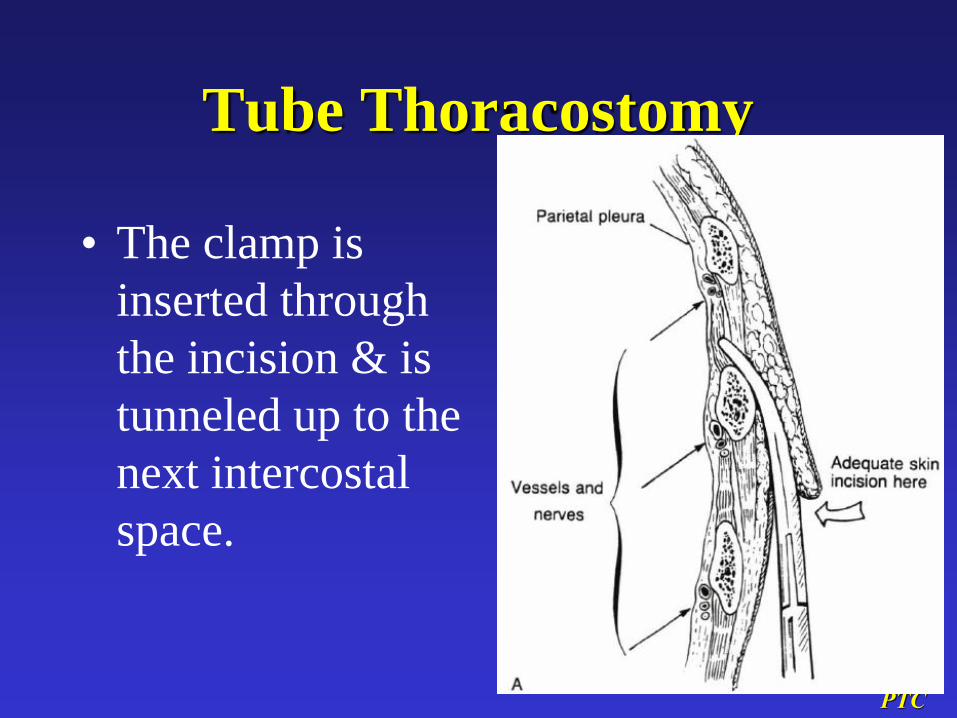
Tube Thoracostomy
• The clamp is
inserted through
the incision & is
tunneled up to the
next intercostal
space.
PTC
Tube Thoracostomy
• The clamp is
inserted through
the incision & is
tunneled up to the
next intercostal
space.

PTC
Most Frequent Reasons for Failure
to Evacuate a Pneumothorax
Rapidly & to Completely Expand the
Lungs
1) Improper connections or leaks in the external tubing or water-seal collection apparatus
2) Improper position of the chest tube(s)

PTC
Most Frequent Reasons for Failure to
Evacuate a Pneumothorax Rapidly & to
Completely Expand the Lungs
3) Occlusion of bronchial by secretions
or a foreign body
4) A tear of one of the large bronchi
5) A large tear of the lung parenchyma

PTC
Most Frequent Reasons for Failure to
Evacuate a Pneumothorax Rapidly & to
Completely Expand the Lungs
• If a pneumothorax persists in spite of 1 or 2 well-placed chest tubes & there is a large leak, emergency bronchoscopy should be performed to clear the bronchi & identify any damage to the tracheobronchial tree that may need repair.
PTC
Most Frequent Reasons for Failure to
Evacuate a Pneumothorax Rapidly & to
Completely Expand the Lungs
• High-frequency oscillation is indicated for bronchopleural fistula & may substantially slow the leak.
• Continued large air leakage & failure of the lung to expand adequately in spite of these measures is an indication for early thoracotomy to control the air leak.

PTC

PTC
Eosophage
al Rupture
&
Mediastina
l Air
PTC
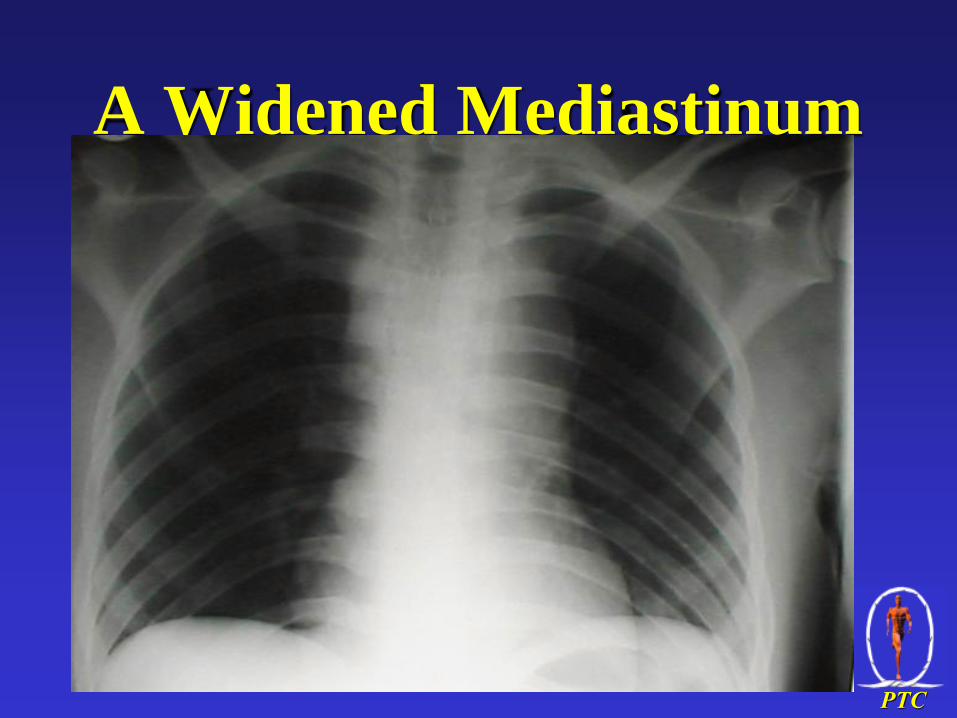
A Widened Mediastinum
PTC
Pulmonar
y
Contusio
n

PTC

PTC

PTC

PTC
Lt. Diaphragm Rupture +
stomach & Spleen Herniation +
Rib Fx.

PTC
Clues to Dx. of Blunt Cardiac
Injury
• Ph. Ex.
• Tachycardia out of proportion to other findings
• Hx.
• High-speed MVA
• Crush steering wheel
• Angina-like CP
• Any dysrhythmia
• Any part of Beck triad
• Evidence of severe ant chest injury
• Any evidence of HF
• Radiography
• Fractured sternum or first 2 ribs
• Widened pericardial silhouette

PTC
Clues to Dx. of Blunt Cardiac
Injury
• Lab• Elevated CPK-MB levels
• ECG• Dysrhythmias or conduction disturbance
• Elevated ST segments
• Other studies• Impaired motion of ant heart on 2-dimensional
echocardiogram or radionuclide angiography
• Pulmonary artery catheter monitoring showing elevated PAWP, low CO, &/or poor response to fluid

PTC
ARDS after Pulmonary
Contusion

PTC
Tension Viscerothorax After
Blunt Abd Trauma

PTC
PTC

PTC
Outcome of ED
Thoracotomy

PTC
Indications for Closed-tube
Thoracostomy
• Recurrence of the pneumothorax after removal of the initial chest tube
• Patient requires ventilator support
• Patient requires general anesthesia
• Associated hemothorax.
• Bilateral pneumothorax regardless of size
• Tension pneumothorax

PTC

PTC
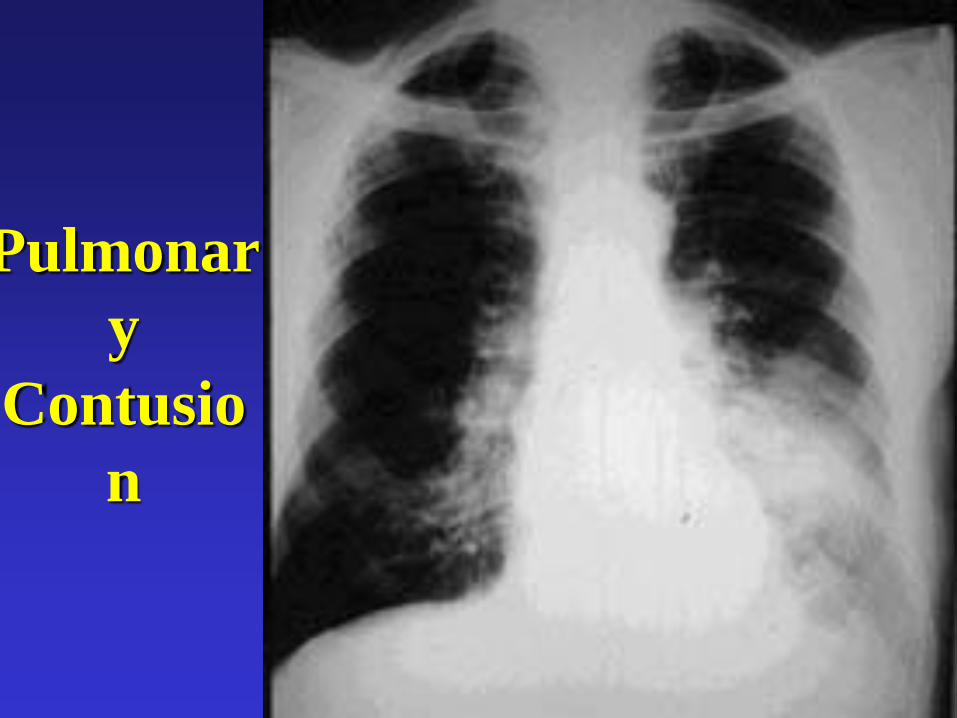
Chest InjuriesPulmonary Contusion
• Potentially life threatening
• Occurs with blunt and penetrating trauma
• Suspect if rib fractures
• Onset often slow and progressive over 24 hours

PTC
Chest InjuriesRib Fractures
• Associated with pulmonary
contusion
• Associated with pneumothorax
• May result from simple trauma
in the elderly
• Remember analgesia
PTC
Chest InjuriesMyocardial Contusion
• Common in blunt trauma
• May mimic myocardial infarction
• Can cause sudden death
• ECG monitoring (if available)

PTC
Chest InjuriesOther Injuries
• Pericardial tamponade
• Great vessel injury
• Airway rupture
• Oesophageal trauma
• Diaphragmatic injury

PTC
Chest Injuries
PTC
Chest Injuries
Summary
• Management is ABC
• Recognise life threatening
problems in primary survey
• Surgical intervention rarely needed

PTC
Abdominal Trauma
Objectives
• Recognise common life threatening
abdominal injuries
• Understand principles of
management of abdominal injuries

PTC
Abdominal TraumaInitial Assessment
Airway
Breathing
Circulation

PTC
Abdominal Trauma
• Common site of injury
• Assessment can be difficult
• Site of “hidden haemorrhage”
• Continual reassessment important
• Early surgical consultation if
possible

PTC
Blunt Abdominal
Trauma
Flank ecchymosis from internal
bleeding
PTC
Abdominal TraumaMechanism of injury
Penetrating (gunshot, stabbing)
-Entry/exit wounds may not be obvious
-Surgical opinion / laparotomy
Non-penetrating
-Good history important
-Compression, crush, seat belt,
acceleration, deceleration
PTC
Abdominal TraumaSite of injury
• Liver
• Spleen
• GIT
• Pancreas
• Kidney and urinary tract

PTC
Abdominal TraumaRemember
Intra-peritoneal cavity extends up
to 4th intercostal space in
thorax
PTC
Abdominal TraumaLook
• Lacerations
• Penetrating injury
• Distension
• Bruising may indicate significant
injury
• External urethral meatus

PTC
Abdominal TraumaFeel
• Be gentle (especially children)
• Tenderness
• Rigidity
• Rectal examination (blood, tone,
prostate)
PTC
Abdominal TraumaManagement
• Airway
• Breathing
• Circulation• IV access
• Fluid resuscitation
• ? Laparotomy
PTC
Abdominal TraumaManagement
• Gastric decompression and
aspiration
- Especially in children
- Look for blood
• Urinary catheterisation
- After exclusion of urethral trauma
PTC
Abdominal TraumaLaparotomy ?
• Penetrating trauma
• Haemodynamic instability with
- obvious intra-abdominal injury
- no other obvious cause
• Seek Early Surgical Advice

PTC
PTC
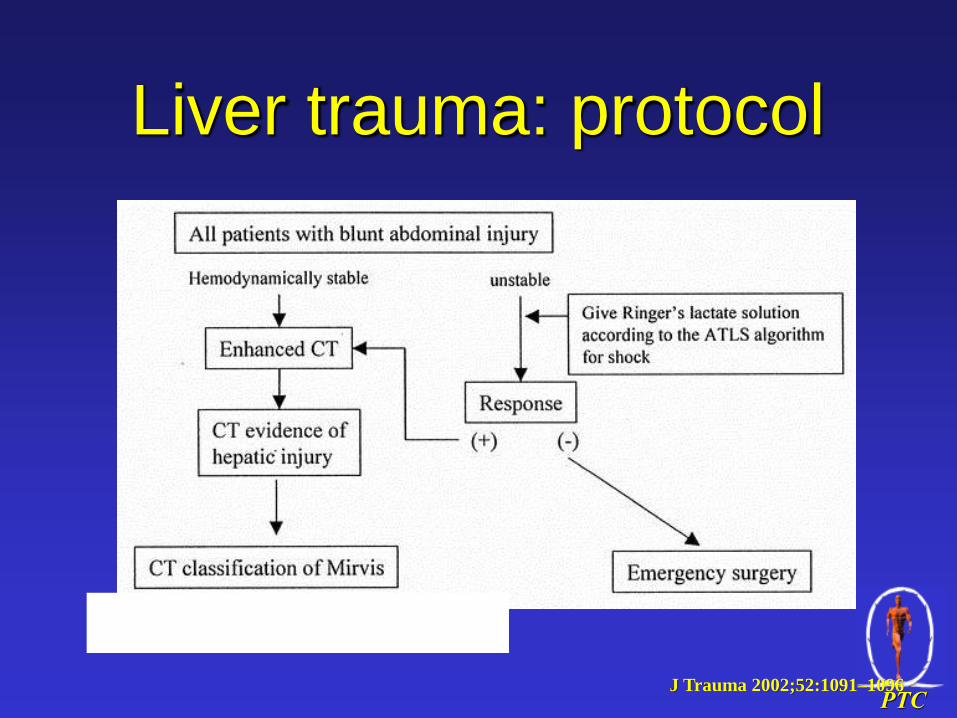
Liver trauma: protocol
J Trauma 2002;52:1091–1096

PTC
Liver trauma: protocol
J Trauma 2002;52:1091–1096
PTC
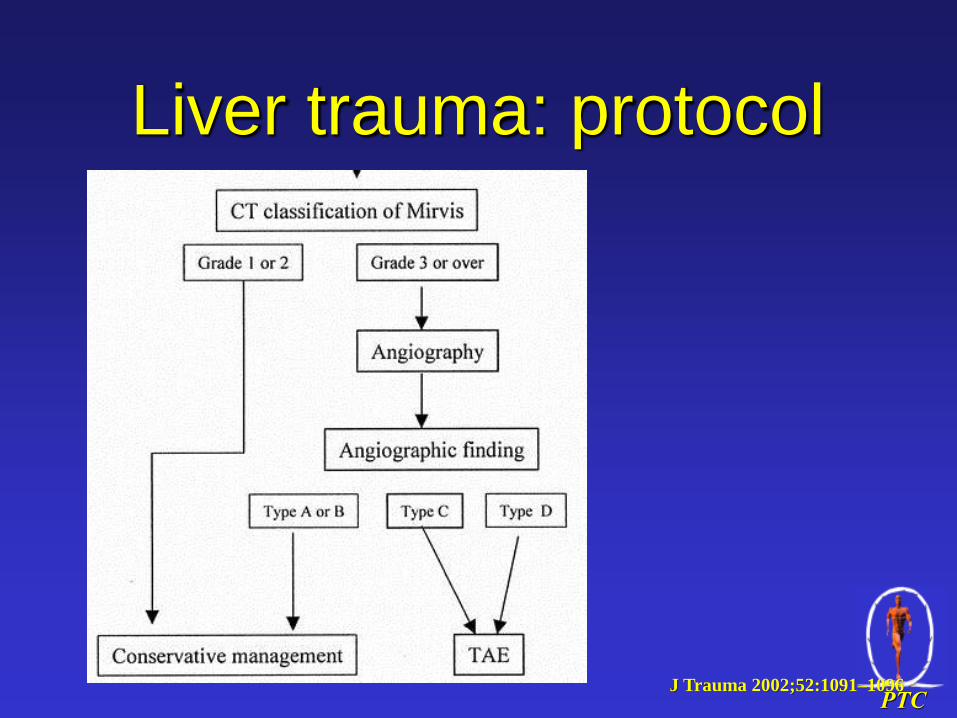
Liver trauma: protocol
J Trauma 2002;52:1091–1096







