

Principles of Cardiac Pacing Principles of Cardiac Pacing
Miguel Leal, MDMiguel Leal, MD
Assistant Professor of Medicine, University of WisconsinAssistant Professor of Medicine, University of Wisconsin
Director, Cardiac Electrophysiology, VA Hospital Director, Cardiac Electrophysiology, VA Hospital -- MadisonMadison
PacemakersPacemakers

Implantable CardioverterImplantable Cardioverter--DefibrillatorsDefibrillators

Advances in Device (ICD) Implantation
Implanting physicianImplanting physician Cardiac surgeonCardiac surgeon EP or surgeonEP or surgeon
Device size (volume)Device size (volume) 120 120 -- 140 mL140 mL << 40 mL40 mL
Implant site Implant site AbdominalAbdominal PectoralPectoral
ProcedureProcedure Median sternotomyMedian sternotomy Skin incisionSkin incisionLateral thoracotomyLateral thoracotomy
Procedure timeProcedure time 2 2 -- 4 hours4 hours 1 hour1 hour
PerioperativePerioperative 2.5%2.5% < 0.5%< 0.5%mortalitymortality
PostPost--implant implant 3 3 -- 5 days5 days 1 day1 dayhospitalization hospitalization
Battery longevityBattery longevity 18 months18 months Up to 9 yearsUp to 9 years
# Implants# Implants 00--2,000/yr2,000/yr 80,000 / year80,000 / year
1980 - 1999 2000 - date
Morgan Stanley Dean Witter. Investors Guide to ICDs. 2000.

Number of Worldwide ICD Implants Per Year
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
100,000
1980 1985 1990 1995 2000 E
Evolution of ICD Therapy
19801980•• First HumanFirst Human
ImplantImplant
19851985•• FDA ApprovalFDA Approval
of ICDsof ICDs
19991999•• MUSTTMUSTT
19931993•• SmallerSmaller
DevicesDevices
19961996•• SteroidSteroid
LeadsLeads
•• MADITMADIT
19891989•• TransvenousTransvenous
LeadsLeads
•• BiphasicBiphasic
WaveformWaveform
1997/981997/98•• DC ICDsDC ICDs
•• AT TherapiesAT Therapies
•• AVIDAVID
•• CASHCASH
•• CIDSCIDS
19881988•• TieredTiered
TherapyTherapy
20002000•• CRTCRT--DD

External Defibrillator



Pacemaker ECG StripsPacemaker ECG Strips
•• Assessing Paced ECG StripsAssessing Paced ECG Strips
–– Identify intrinsic rhythm and clinical conditionIdentify intrinsic rhythm and clinical condition
–– Identify pacer spikesIdentify pacer spikes
–– Identify activity following pacer spikesIdentify activity following pacer spikes
–– Failure to captureFailure to capture
–– Failure to senseFailure to sense
•• EVERY PACER SPIKE SHOULD HAVE A EVERY PACER SPIKE SHOULD HAVE A
PP--WAVE OR A QRSWAVE OR A QRS--COMPLEX COMPLEX
FOLLOWING IT.FOLLOWING IT.

Pacemaker CodesPacemaker Codes
PositionPosition
FunctionFunction
11
Chambers Chambers
PacedPaced
22
Chambers Chambers
SensedSensed
33
Response to Response to
Sensed Sensed
StimulusStimulus
44
Rate Rate
Modulation?Modulation?
O (none)O (none) OO OO O (nonO (non--rate rate
responsive)responsive)
A (atrium)A (atrium) AA T (triggered)T (triggered) R (rate R (rate
responsive)responsive)
V (ventricle)V (ventricle) VV I (inhibited)I (inhibited)
D (both atrium & D (both atrium &
ventricle)ventricle)

Principles of PacingPrinciples of Pacing
•• Commonly used modes:Commonly used modes:
–– AAI AAI –– atrial demand pacingatrial demand pacing
–– VVI VVI –– ventricular demand pacingventricular demand pacing
–– DDD DDD –– atrial/ventricular demand pacing, atrial/ventricular demand pacing,
senses & paces both chambers; trigger senses & paces both chambers; trigger
or inhibitor inhibit
–– AOO AOO –– atrial asynchronous pacingatrial asynchronous pacing
–– VOO VOO –– ventricular asynchronous pacingventricular asynchronous pacing

Normal PacingNormal Pacing
•• Atrial pacingAtrial pacing
–– Atrial pacing spikes followed by PAtrial pacing spikes followed by P--waveswaves

Normal PacingNormal Pacing
•• Ventricular pacingVentricular pacing
–– Ventricular pacing spikes followed by wide, Ventricular pacing spikes followed by wide,
bizarre QRSbizarre QRS--complexescomplexes

Normal PacingNormal Pacing
•• Sequential AV pacingSequential AV pacing
–– Atrial & ventricular pacing spikes followed by Atrial & ventricular pacing spikes followed by
atrial & ventricular complexesatrial & ventricular complexes

Normal PacingNormal Pacing
•• PP--wave synchronous mode of pacingwave synchronous mode of pacing
–– Ventricle paced at sensed atrial rateVentricle paced at sensed atrial rate
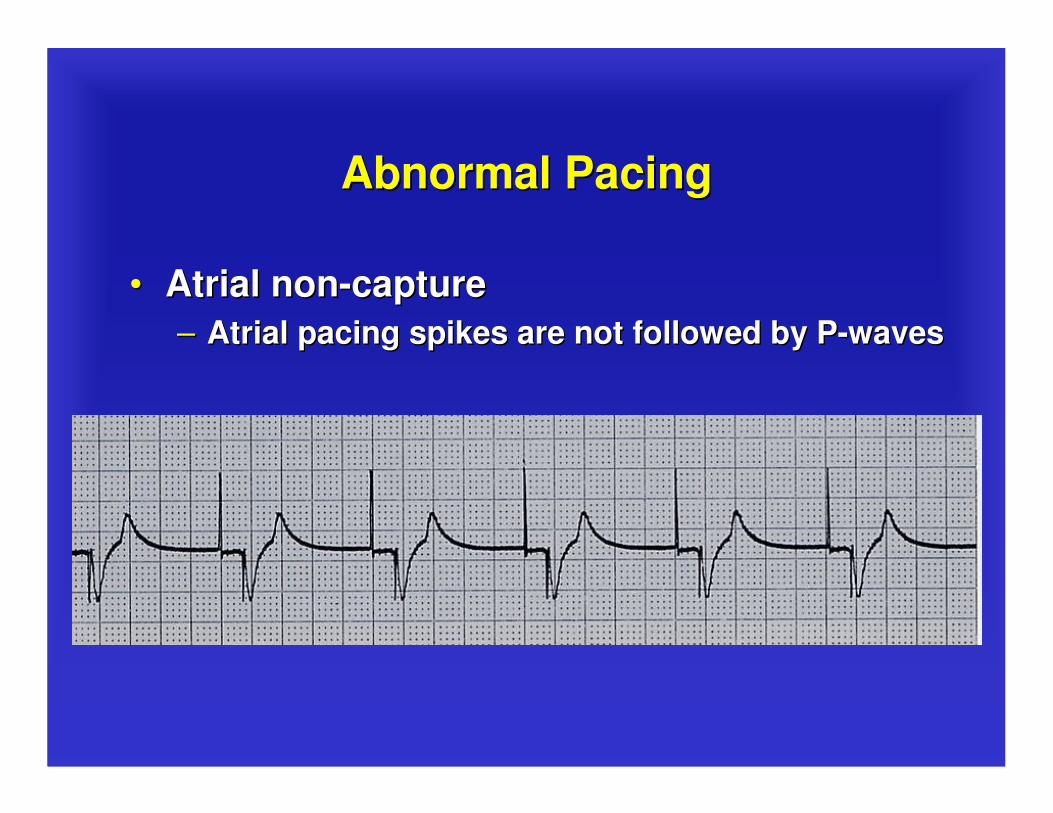
Abnormal PacingAbnormal Pacing
•• Atrial nonAtrial non--capturecapture
–– Atrial pacing spikes are not followed by PAtrial pacing spikes are not followed by P--waveswaves

Abnormal PacingAbnormal Pacing
•• Ventricular nonVentricular non--capturecapture
–– Ventricular pacing spikes are not followed by Ventricular pacing spikes are not followed by
QRSQRS--complexescomplexes

Failure to CaptureFailure to Capture
•• CausesCauses
–– Insufficient energy delivered by pacerInsufficient energy delivered by pacer
–– Low battery voltageLow battery voltage
–– Dislodged, loose, fibrotic, or fractured Dislodged, loose, fibrotic, or fractured
electrodeelectrode
–– Electrolyte abnormalitiesElectrolyte abnormalities
•• AcidosisAcidosis
•• HypoxemiaHypoxemia
•• HyperkalemiaHyperkalemia

Failure to CaptureFailure to Capture
•• SolutionsSolutions
–– View rhythm in different leadsView rhythm in different leads
–– Change electrodesChange electrodes
–– Check connectionsCheck connections
–– Increase pacer outputIncrease pacer output
–– Change battery, cables, pacer Change battery, cables, pacer
–– Reverse polarityReverse polarity

Abnormal PacingAbnormal Pacing
•• Atrial undersensingAtrial undersensing
–– Atrial pacing spikes occur irregardless of PAtrial pacing spikes occur irregardless of P--
waveswaves
–– Pacemaker is not Pacemaker is not ““seeingseeing”” the intrinsic activitythe intrinsic activity

Abnormal PacingAbnormal Pacing
•• Ventricular undersensingVentricular undersensing–– Ventricular pacing spikes occur regardless of Ventricular pacing spikes occur regardless of
QRSQRS--complexescomplexes
–– Pacemaker is not Pacemaker is not ““seeingseeing”” the intrinsic activitythe intrinsic activity

Failure to SenseFailure to Sense
•• CausesCauses
–– Pacemaker not sensitive enough to detect Pacemaker not sensitive enough to detect the patientthe patient’’s intrinsic electrical activity s intrinsic electrical activity (mV)(mV)
–– Insufficient myocardial voltageInsufficient myocardial voltage
–– Dislodged, loose, fibrotic, or fractured Dislodged, loose, fibrotic, or fractured electrodeelectrode
–– Electrolyte abnormalitiesElectrolyte abnormalities
–– Low battery voltageLow battery voltage

Failure to SenseFailure to Sense
•• Danger Danger –– potential (low) for paced potential (low) for paced
ventricular beat to land on T wave ventricular beat to land on T wave
(R(R--onon--T phenomenon)T phenomenon)

Failure to SenseFailure to Sense
•• SolutionsSolutions
–– View rhythm in different leadsView rhythm in different leads
–– Change electrodesChange electrodes
–– Check connectionsCheck connections
–– Increase pacemakerIncrease pacemaker’’s sensitivitys sensitivity
–– Replace cables and/or batteryReplace cables and/or battery
–– Reverse polarityReverse polarity
–– Check electrolytesCheck electrolytes
–– Unipolar settingUnipolar setting

OversensingOversensing
•• Pacing does not occur when intrinsic Pacing does not occur when intrinsic
rhythm is inadequaterhythm is inadequate

OversensingOversensing
•• CausesCauses
–– Pacemaker inhibited due to sensing of Pacemaker inhibited due to sensing of
““PP”” waves & waves & ““QRSQRS”” complexes that do complexes that do
not existnot exist
–– Pacemaker too sensitivePacemaker too sensitive
–– Possible wire fracture, loose contactPossible wire fracture, loose contact
–– Pacemaker failurePacemaker failure
•• Risks: heart block, asystoleRisks: heart block, asystole

OversensingOversensing
•• SolutionsSolutions
–– View rhythm in different leadsView rhythm in different leads
–– Change electrodesChange electrodes
–– Check connections Check connections
–– Decrease pacemaker sensitivityDecrease pacemaker sensitivity
–– Change cables and/or batteryChange cables and/or battery
–– Reverse polarityReverse polarity
–– Check electrolytesCheck electrolytes
–– Unipolar pacing with subcutaneous Unipolar pacing with subcutaneous ““ground ground wirewire””
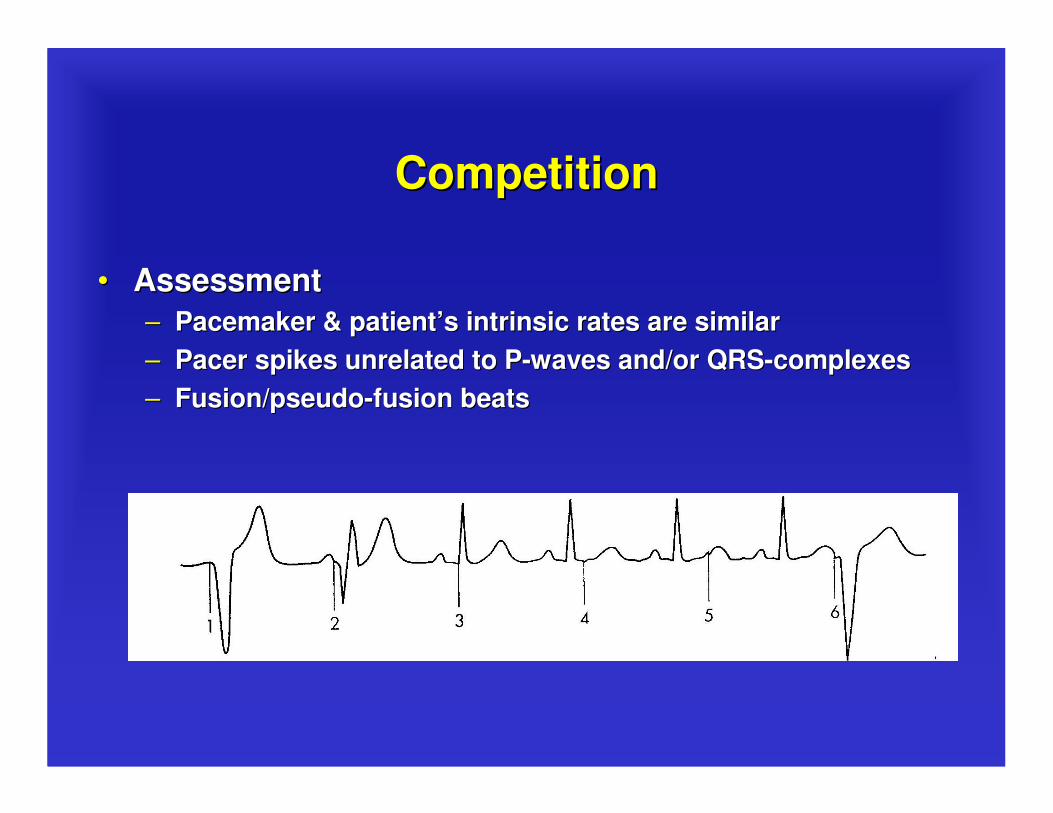
CompetitionCompetition
•• AssessmentAssessment
–– Pacemaker & patientPacemaker & patient’’s intrinsic rates are similars intrinsic rates are similar
–– Pacer spikes unrelated to PPacer spikes unrelated to P--waves and/or QRSwaves and/or QRS--complexescomplexes
–– Fusion/pseudoFusion/pseudo--fusion beatsfusion beats

Magnet modeMagnet mode
•• Pacemakers: asynchronous pacingPacemakers: asynchronous pacing
•• Defibrillators: suspended detection of Defibrillators: suspended detection of
arrhythmiasarrhythmias

Assessing Underlying RhythmAssessing Underlying Rhythm
•• Carefully assess underlying rhythmCarefully assess underlying rhythm
–– Right way: slowly decrease pacemaker rateRight way: slowly decrease pacemaker rate

Assessing Underlying RhythmAssessing Underlying Rhythm
•• Assessing Underlying RhythmAssessing Underlying Rhythm
–– Wrong way: pause pacer or unplug cablesWrong way: pause pacer or unplug cables

Pacemaker WenckebachPacemaker Wenckebach
•• AssessmentAssessment
–– Appears similar to 2Appears similar to 2ndnd degree heart blockdegree heart block
–– Occurs with intrinsic tachycardiaOccurs with intrinsic tachycardia
•• CausesCauses
–– DDD mode safety featureDDD mode safety feature
–– Prevents rapid ventricular pacing Prevents rapid ventricular pacing
impulse in response to rapid atrial rateimpulse in response to rapid atrial rate
•• Sinus tachycardiaSinus tachycardia
•• Atrial fibrillation, flutterAtrial fibrillation, flutter
•• Prevents pacemakerPrevents pacemaker--mediated tachycardiamediated tachycardia
•• Upper rate limit may be inappropriateUpper rate limit may be inappropriate
Pacemaker WenckebachPacemaker Wenckebach

•• SolutionSolution
–– Treat cause of tachycardiaTreat cause of tachycardia
•• Fever: CoolingFever: Cooling
•• Atrial tachycardia: AntiAtrial tachycardia: Anti--arrhythmicarrhythmic
•• Pain: AnalgesicPain: Analgesic
•• Hypovolemia: Fluid bolusHypovolemia: Fluid bolus
–– Adjust pacemaker upper rate limit as appropriateAdjust pacemaker upper rate limit as appropriate
Pacemaker WenckebachPacemaker Wenckebach

Special scenarios Special scenarios –– MVPMVP
(Managed Ventricular Pacing)(Managed Ventricular Pacing)

Practice Strip #1Practice Strip #1
AAI: normal atrial pacing

Practice Strip #2Practice Strip #2
Sinus rhythm: no pacing;
possible back-up settings are AAI, VVI or DDD

Practice Strip #3Practice Strip #3
DDD: failure to sense ventricle; increase ventricular sensitivity

Practice Strip #4Practice Strip #4
VVI: ventricular pacing

Practice Strip #5Practice Strip #5
DDD: failure to capture atria or ventricle;
increase atrial & ventricular output

Practice Strip #6Practice Strip #6
DDD: normal atrial & ventricular pacing
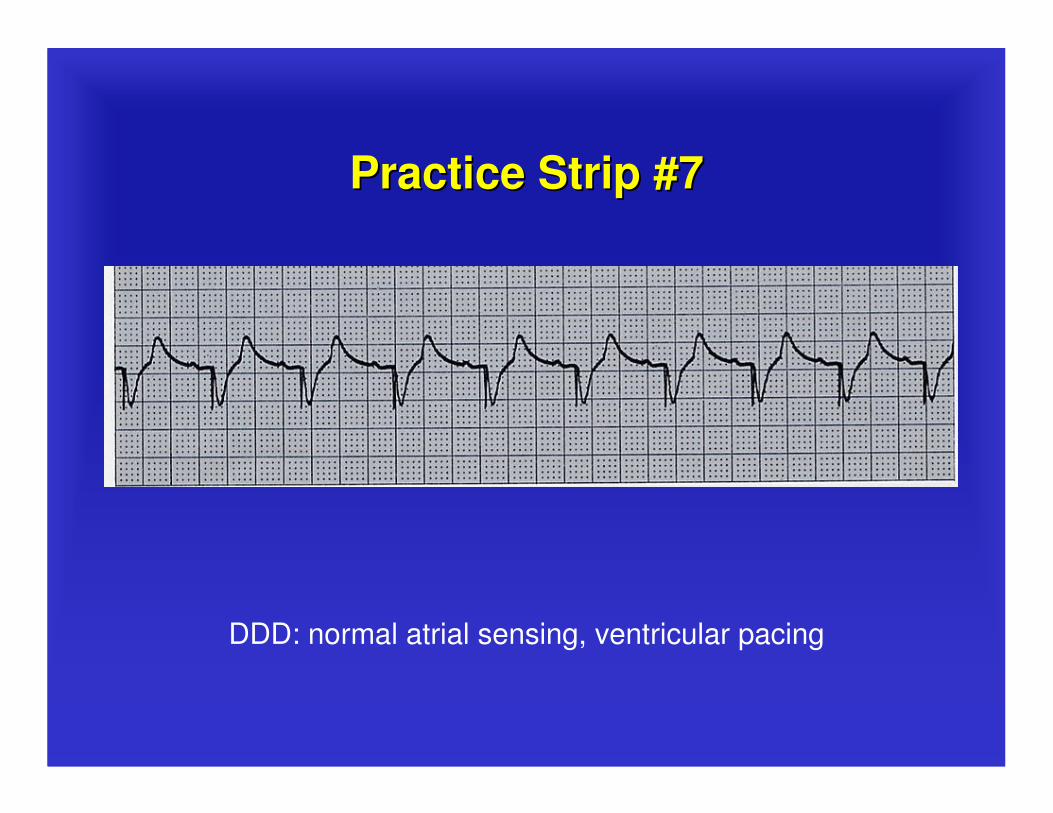
Practice Strip #7Practice Strip #7
DDD: normal atrial sensing, ventricular pacing

Practice Strip #8Practice Strip #8
DDD: failure to sense P-waves; increase atrial sensitivity

Practice Strip #9Practice Strip #9
DDD: ventricular oversensing; decrease ventricular sensitivity

Thank you!Thank you!
Questions?Questions?







