

Inflammatory markers in assessing bacterial infections
and aiding prescribing decisions
Prof. Stephan Harbarth Geneva (Switzerland)
BSAC Spring Meeting 2014 [email protected]

• Several research projects presented in this talk received funding by BRAHMS (Germany)
• Advisory board: BioMerieux
Disclosures
RApid Point-of-Care test Platforms for Infectious Diseases

Widely used diagnostic tests to assess inflammation vs. infection
• Erythrocyte sedimentation rate – Earliest indirect method to assess
inflammation • Differential WBC • C-reactive protein (CRP) • Procalcitonin (PCT) • [IL-6, TNF ….]
Gabay C, Kushner I N Engl J Med 1999, 340:448-54
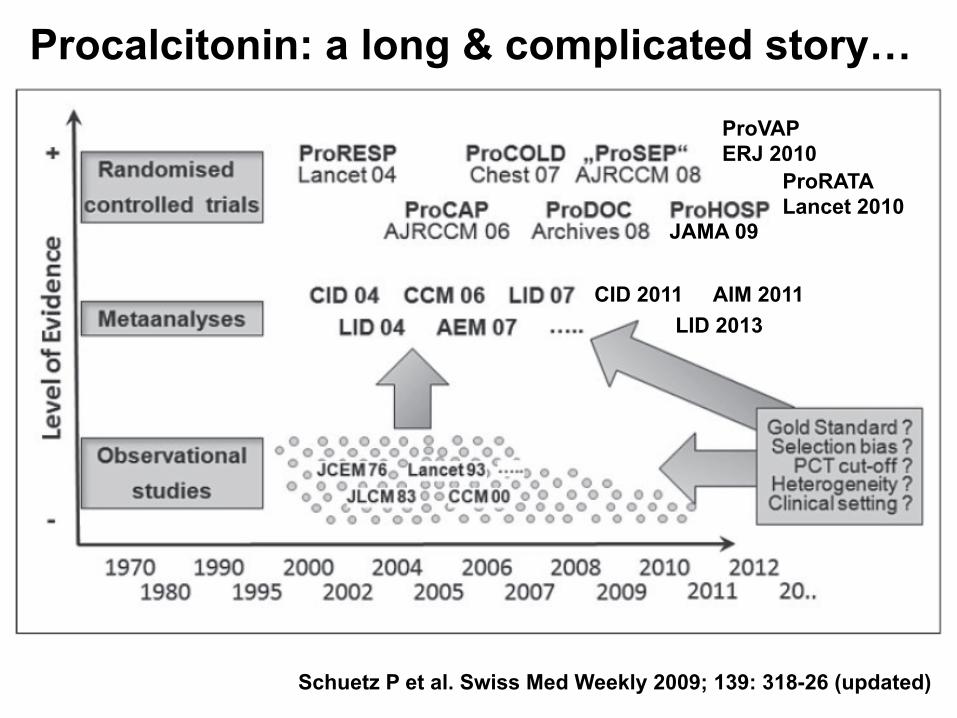
Schuetz P et al. Swiss Med Weekly 2009; 139: 318-26 (updated)
JAMA 09
ProRATA Lancet 2010
Procalcitonin: a long & complicated story…
ProVAP ERJ 2010
CID 2011 LID 2013
AIM 2011

Ongoing controversy about PCT


Reasons for discrepant conclusions on PCT as a marker of bacterial infection
• Different assays • Cut-off range depends on:
– Clinical setting and type of infection – Pretest probabilities
• Poor study design of many observational studies • Single PCT measurement of limited value • False positives & negatives (≈10%)
Christ-Crain M & Muller B, Swiss Med Wkly 2005; 135: 451-60

ANTIBIOTIC DURATION
Individualized treatment guidance
Procalcitonin and CRP
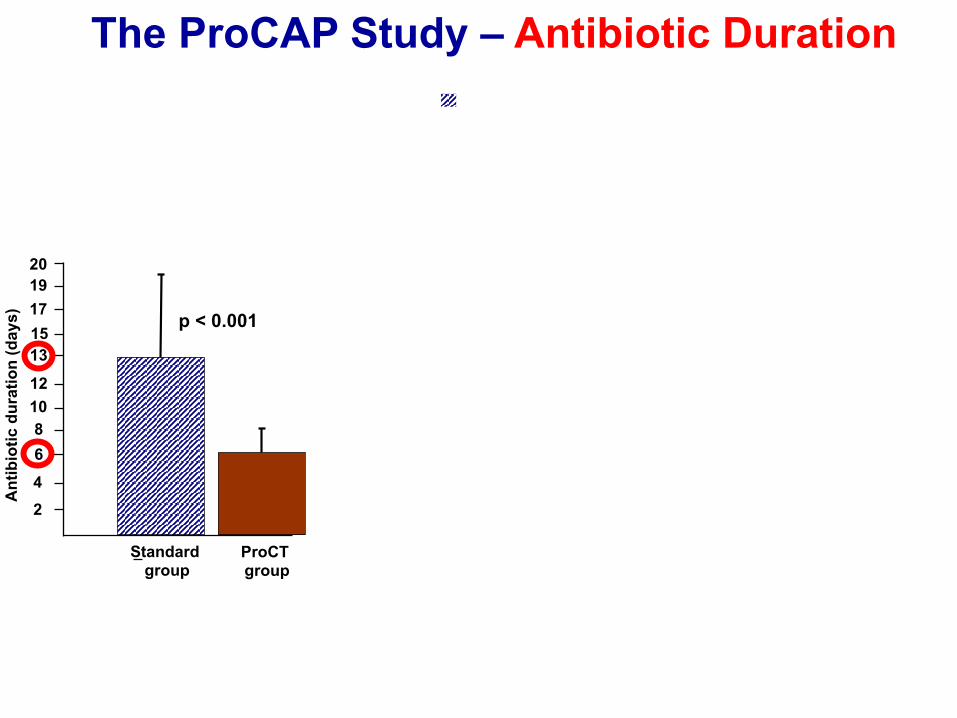
The ProCAP Study – Antibiotic Duration
p < 0.001
Standard group ProCT
group
2 4 6 8
10 12 13
20
Ant
ibio
tic d
urat
ion
(day
s)
15 17 19
Standard group ProCT group
0
10
20
30
40
50
60
70
80
90
100
AB started > 4d > 6d > 8d > 10d > 14d > 21d
Ant
ibio
tic P
resc
ripto
in (%
)
Christ-Crain M et al, Am J Respir Crit Care Med 2006

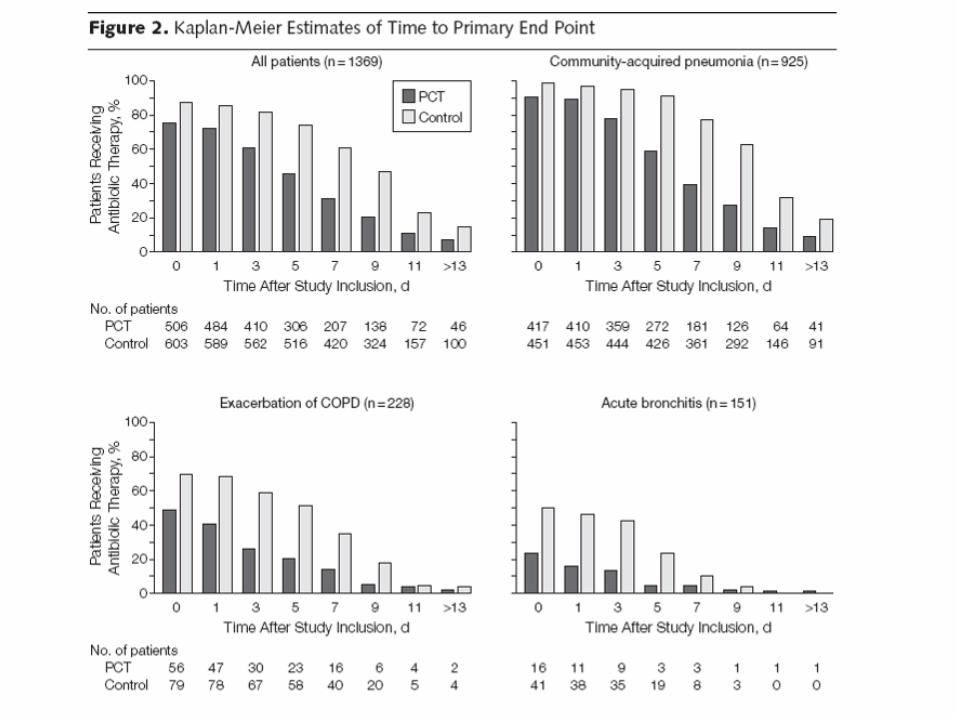
JAMA 2009; 302: 1059-66
Main results
• In the PCT group, antibiotic exposure significantly lower as compared to controls (35% reduction, p<0.001)
• Rate of adverse outcomes similar in PCT and control group (15.4% vs. 18.9%)
• Antibiotic-associated side effects less frequent in the PCT group (19.8% vs. 28.1%; p<0.001)
Schuetz P et al. JAMA 2009; 302: 1059-66
BICAP study, CH
• Pa#ents were treated with an#bio#cs for a median of 10.0 days (IQR 8.0-‐12.0) in the monotherapy vs. 10.0 days (IQR 7.0-‐11.0) in the combina#on arm
N. Garin, unpublished data (March 2014)

Procalcitonin (PCT) guidance allows shortening antibiotic therapy duration in patients with severe
sepsis and septic shock. A randomized clinical trial
Nobre V, Harbarth S, Graf J-D, Rohner P, and Pugin J University Hospitals of Geneva, Switzerland
Am J Respir Crit Care Med 2008; 177: 498–505

To test if a PCT-guided strategy allows
reducing the use of antibiotics in patients
with severe sepsis and septic shock.
Objective
Nobre V et al. Am J Respir Crit Care Med 2008; 177: 498–505
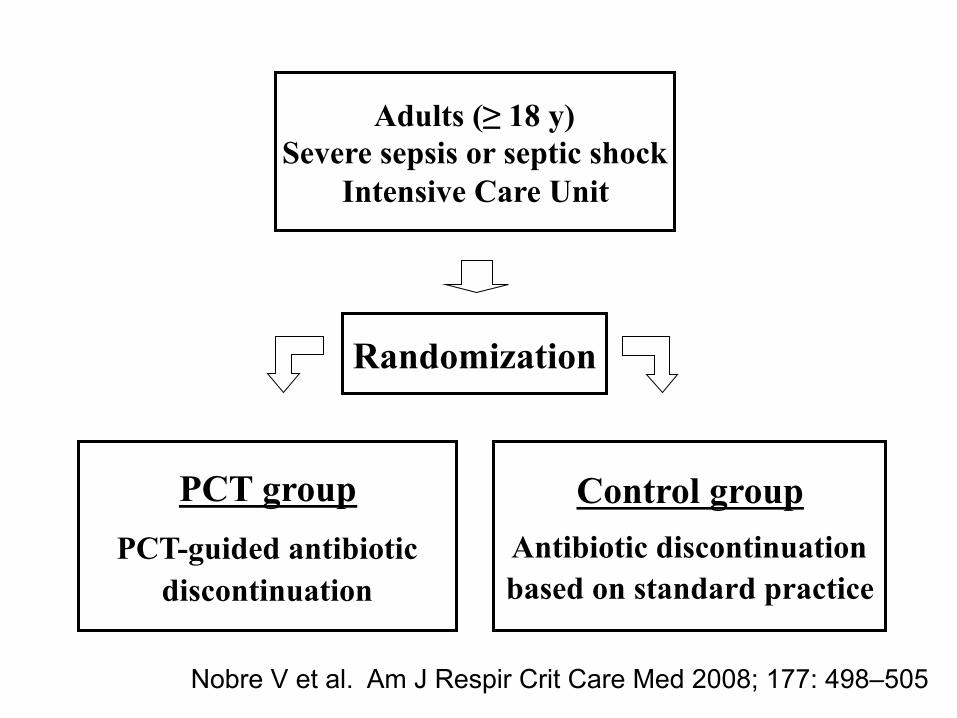
Adults (≥ 18 y) Severe sepsis or septic shock
Intensive Care Unit
PCT group PCT-guided antibiotic
discontinuation
Randomization
Control group Antibiotic discontinuation based on standard practice
Nobre V et al. Am J Respir Crit Care Med 2008; 177: 498–505

Baseline characteristics of patients – Per protocol (n=68 )
Characteristics PCT group (n=31)
Control group (n=37) p value
Nobre V et al. Am J Respir Crit Care Med 2008; 177: 498–505

Primary endpoints
Per protocol analysis
Control group (n=37)
PCT group (n=31)
p value / IRR
Days of AB therapy
10 (3-33) 6 (4-16) 0.003
AB exposure-days
655 504 0.0002 IRR=1.3 (95% CI: 1.1-1.5)
Nobre V et al. Am J Respir Crit Care Med 2008; 177: 498–505
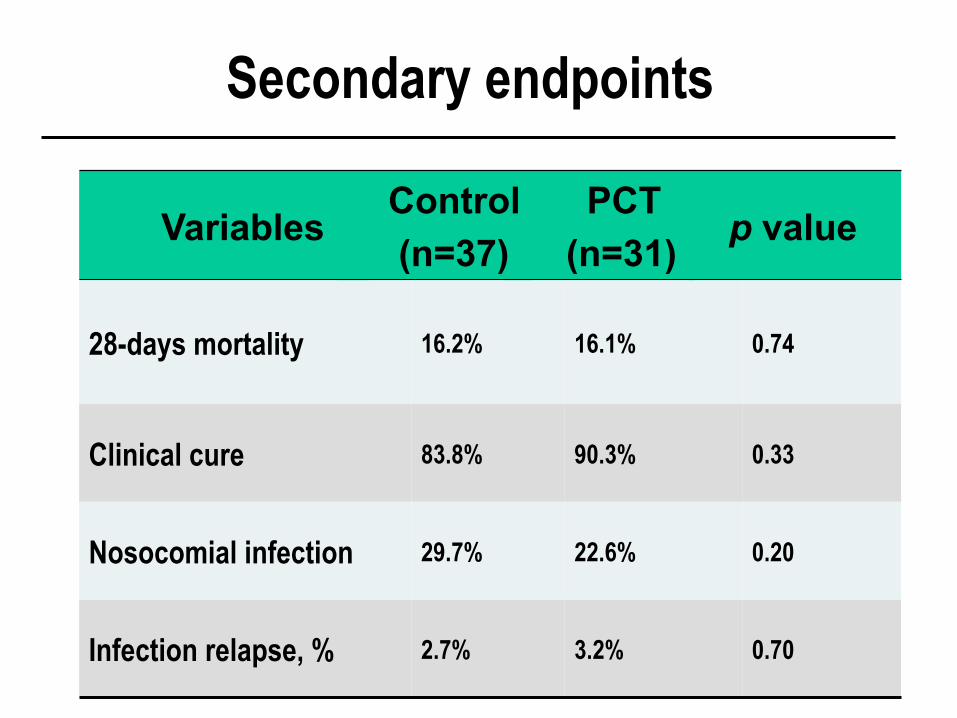
0.70 3.2% 2.7% Infection relapse, %
0.20 22.6% 29.7% Nosocomial infection
0.33 90.3% 83.8% Clinical cure
0.74 16.1% 16.2% 28-days mortality
p value PCT (n=31)
Control (n=37)
Variables
Secondary endpoints

Procalcitonin use at HUG N
umbe
r of P
CT
test
s

PCT value
(N=2015)
AnBbioBcs prescribed
within 24 hrs
(N=659)
No anBbioBcs prescribed
within 24 hrs
(N=1356)
<0.25 ug/L
Inappropriate prescrip#on
277 /659= 42.0%
Appropriate withholding
779/1356= 57.4 %
>= 0.25 ug /L, < 2 ug/L
Indeterminate
243 / 659=36.9 %
Indeterminate
397 / 1356= 29.3 %
>2 ug/L
Appropriate prescrip#on
139 / 659 = 21.1 %
Inappropriate withholding
180/1356= 13.3 %
UBlisaBon de la PCT au Département de Médecine Interne, 2009-‐2010
N.Garin, V.Poffet, S.Harbarth, A.Perrier (unpublished data)

Early antibiotic withdrawal.....
47-y drug abuser, CAP & BSI due to E. coli, stop AB at D13 Lung abscess, requiring prolonged treatment

1315 Patients Assessed for Eligibility 685 Ineligible 158 had expected ICU stay <3 days 138 had SAPS II >65 104 had received AB for >24 hours 99 required prolonged therapy 63 not enrolled for logistic reasons 46 had do-not-resuscitate orders 31 were neutropenic 15 had no medical insurance 12 had been enrolled in other studies 10 refused consent 9 excluded for other reasons
630 Randomized
311 Assigned to the Procalcitonin Group
319 Assigned to the Control Group
307 Included in Analysis
(1 lost to follow-up on day 15)
314 Included in Analysis
(1 lost to follow-up on day 22)
4 withdrew consent 1 randomized twice
The ProRata Trial
4 withdrew consent
Courtesy: Jean Chastre, Paris (Bouadma, Lancet 2010)

PCT group: algorithme
Stopping antibiotics
strongly encouraged
[PCT]<0.25 µg/l Ø[PCT]≥80%/[PCT] max
or0.25≤[PCT]<0.5 µg/l
Stopping antibiotics encouraged
Ö[PCT]/[PCT] previousand
[PCT]≥0.5 µg/l
Changing antibiotics
strongly encouraged
Ø[PCT]<80%/[PCT] maxand
[PCT]≥0.5 µg/l
Continuing antibiotics encouraged
Guidelines for stopping, continuing, or changing antibiotics according to daily measured PCT value
Guidelines for initiating antibiotics according to PCT value Except any situation requiring immediate antibiotic therapy (septic shock, purulent meningitis, etc.)
Obtain second PCT determination 6–12 hours laterif value had been obtained early after the start of the episode
[PCT]< 0.25 µg/l
Antibiotics strongly discouraged Antibiotics discouraged
0.25≤[PCT]<0.5 µg/l [PCT]≥1 µg/l
Antibiotics strongly encouragedAntibiotics encouraged
0.5≤[PCT]<1 µg/l
Stopping antibiotics
strongly encouraged
[PCT]<0.25 µg/l Ø[PCT]≥80%/[PCT] max
or0.25≤[PCT]<0.5 µg/l
Stopping antibiotics encouraged
Ö[PCT]/[PCT] previousand
[PCT]≥0.5 µg/l
Changing antibiotics
strongly encouraged
Ø[PCT]<80%/[PCT] maxand
[PCT]≥0.5 µg/l
Continuing antibiotics encouraged
Guidelines for stopping, continuing, or changing antibiotics according to daily measured PCT value
Guidelines for initiating antibiotics according to PCT value Except any situation requiring immediate antibiotic therapy (septic shock, purulent meningitis, etc.)
Guidelines for initiating antibiotics according to PCT value Except any situation requiring immediate antibiotic therapy (septic shock, purulent meningitis, etc.)
Guidelines for initiating antibiotics according to PCT value Except any situation requiring immediate antibiotic therapy (septic shock, purulent meningitis, etc.)
Obtain second PCT determination 6–12 hours laterif value had been obtained early after the start of the episode
Obtain second PCT determination 6–12 hours laterif value had been obtained early after the start of the episode
[PCT]< 0.25 µg/l
Antibiotics strongly discouraged
[PCT]< 0.25 µg/l
Antibiotics strongly discouraged Antibiotics discouraged
0.25≤[PCT]<0.5 µg/l
Antibiotics discouraged
0.25≤[PCT]<0.5 µg/l [PCT]≥1 µg/l
Antibiotics strongly encouraged
[PCT]≥1 µg/l
Antibiotics strongly encouragedAntibiotics encouraged
0.5≤[PCT]<1 µg/l
Antibiotics encouraged
0.5≤[PCT]<1 µg/l
Courtesy: Jean Chastre, Paris (Bouadma, Lancet 2010)
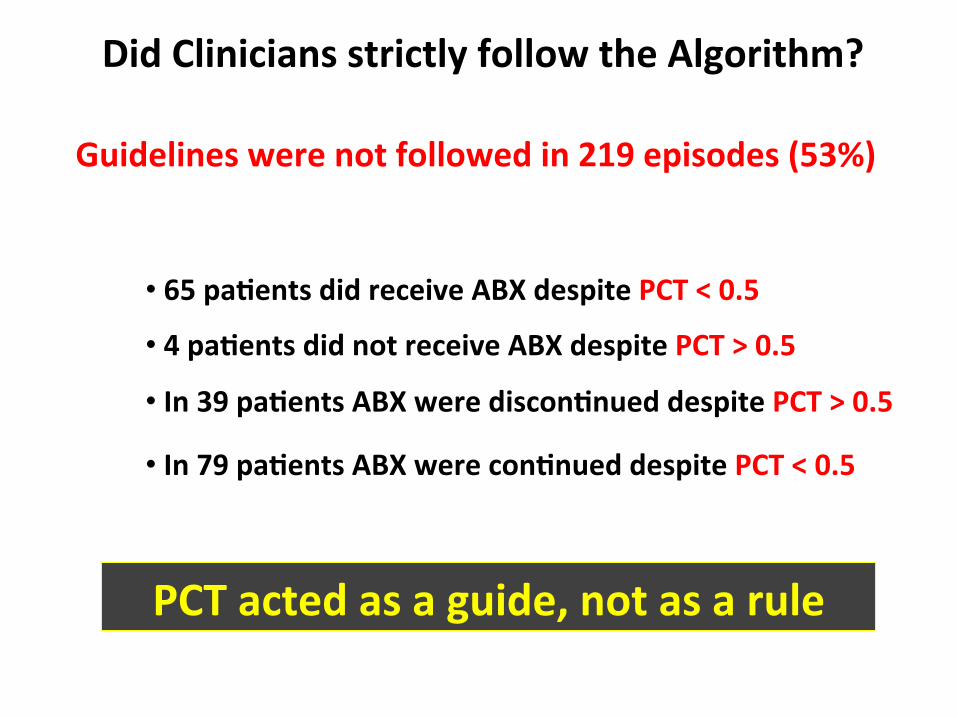
Did Clinicians strictly follow the Algorithm?
Guidelines were not followed in 219 episodes (53%)
• 65 paBents did receive ABX despite PCT < 0.5 • 4 paBents did not receive ABX despite PCT > 0.5 • In 39 paBents ABX were disconBnued despite PCT > 0.5
• In 79 paBents ABX were conBnued despite PCT < 0.5
PCT acted as a guide, not as a rule

Characteristic
PCT Group
(n = 307)
Control Group
(n = 314)
Age, mean (SD), y 61.0 (15.2) 62.1 (15.0)
SAPS II, mean (SD)
SOFA score, mean (SD)
43.8 (16.1)
7.5 (4.4)
43.4 (15.4)
7.2 (4.4)
Mechanical ventilation, No. (%) 211 (68.7) 208 (66.2)
Type of infection, No. (%)
Community-acquired
Hospital-acquired
153 (49.8)
154 (50.2)
173 (55.1)
141 (44.9)
Septic shock, No. (%) 131(42.7) 123 (39.2)
Positive blood cultures, No. (%) 55 (17.9) 53 (16.9)
Procalcitonin, mean (SD), µg/L 12.0 (30.9) 12.0 (32.6)
Courtesy: Jean Chastre, Paris (Bouadma, Lancet 2010)

Use of Procalcitonin to Shorten Antibiotic Exposure in ICU Patients : The ProRata Trial
Bouadma et al. Lancet 2010
All patients VAP Intraabdominal infection
UTI Positive blood cultures
N
CAP
20 14
9.9
6.1
10.6
5.6
9.4
7.3
10.8
8.1
14.5
7.4
12.8
9.8
0
2
4
6
8
10
12
14
16
Dur
atio
n of
trea
tmen
t (da
ys)
314 307 101 79 66 75 18 24 53 55
PCT
Control

Use of Procalcitonin to Shorten Antibiotic Exposure in ICU Patients : The ProRata Trial Bouadma et al. Lancet 2010 P
roba
bilit
y of
Sur
viva
l, %
Days after Inclusion
Procalcitonin Control group
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60
OR at D28; 0.81, 90% CI 0.63-1.29 OR at D60; 1.09, 90% CI 0.79-1.51

PCT arm (secondary outcomes): - ICU LoS increased by one day (p < .004) - Rate of mechanical ventilation per day increased by 5% - More broad-spectrum drug escalation - Shorter time to administration of appropriate antimicrobials
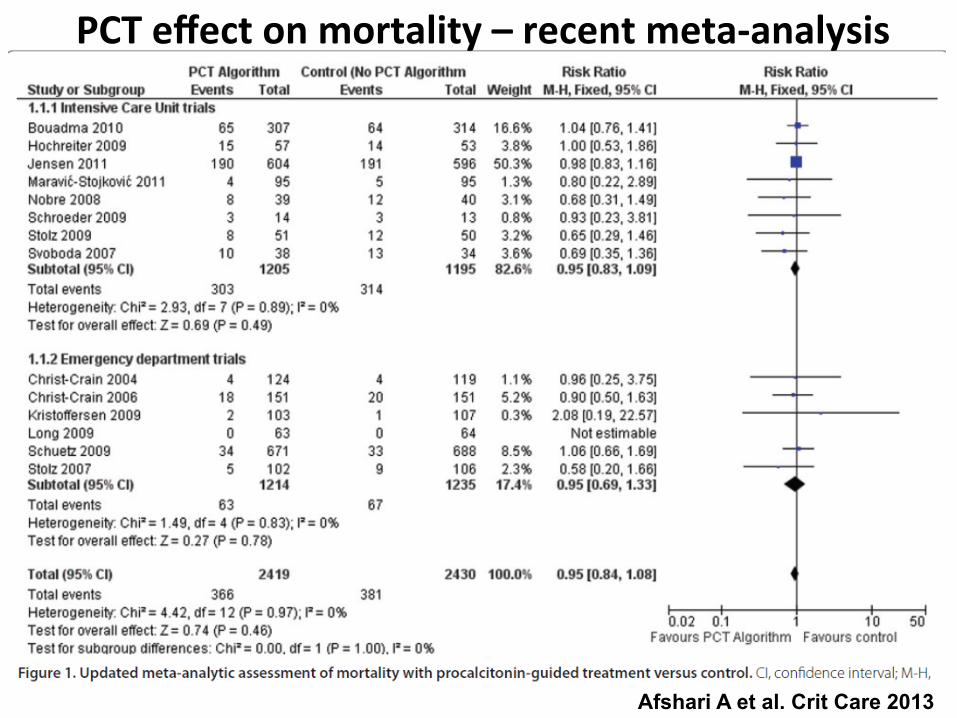
Afshari A et al. Crit Care 2013
PCT effect on mortality – recent meta-‐analysis

• Limited role for the starBng of ABX -‐ 28% of proven infecBons had PCT < 0.25 -‐ 29% of non-‐infected paBents with PCT >1
Corona A et al. J Antimicrob Chemother 2004;54:809-17.

Corona A et al. J Antimicrob Chemother 2004;54:809-17.

And what about CRP ?

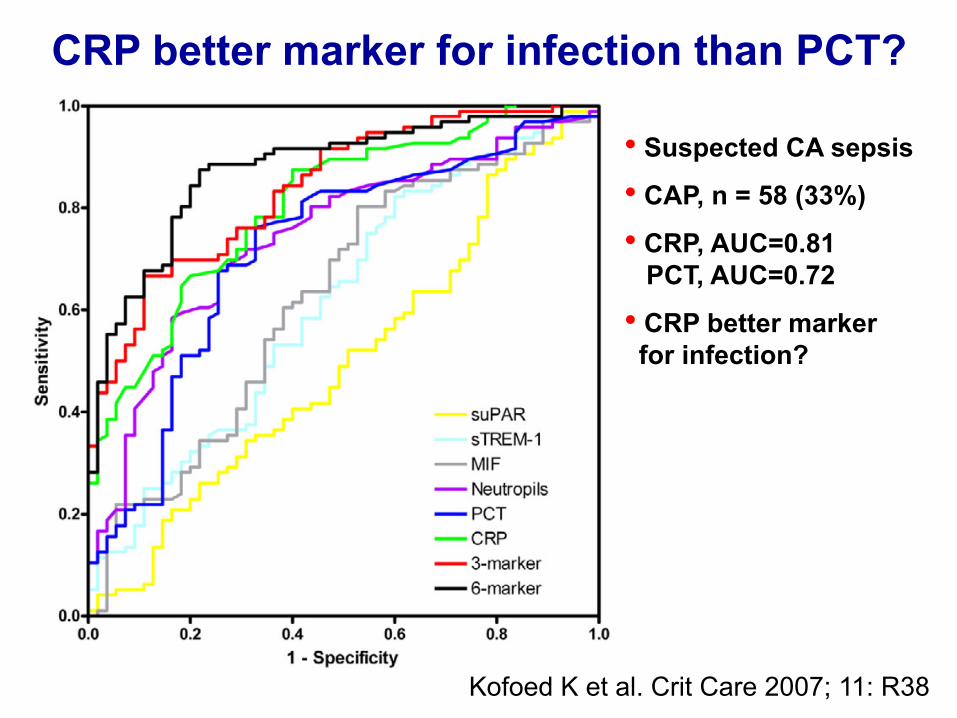
CRP better marker for infection than PCT?
• Suspected CA sepsis
• CAP, n = 58 (33%)
• CRP, AUC=0.81 PCT, AUC=0.72
• CRP better marker for infection?
Kofoed K et al. Crit Care 2007; 11: R38

0 0.
25
0.50
0.
75
1.00
S
ensi
tivity
0.25 0.50 0.75 1.00 1-Specificity
PCT (0.88; 0.84-0.93) CRP (0.76; 0.69-0.83) Leukocytes (0.69; 0.62-0.77) Temperature (0.55; 0.46-0.63)
0
Müller B et al. BMC Infect Dis 2007
Diagnostic accuracy to predict radiographically suspected CAP

Meisner M et al, Crit Care 2006

BMJ review
• Testing for CRP neither sufficiently sensitive to rule out nor sufficiently specific to rule in bacterial LRTI
• Poor methodological quality of studies • Not sufficient evidence to support a wide
introduction of CRP as a rapid test to guide antibiotic prescription
BMJ 2005; 331: 26-29

CRP for monitoring CAP
• CRP useful for monitoring individual clinical course
• Marker of delayed resolution of chest infiltrates and complications
• BUT: No RCT available that investigated specifically the role of CRP for guiding AB treatment duration in CAP
Bruns AH et al. Clin Infect Dis 2007; 45: 983-91 Coelho L et al. Crit Care 2007; 11: R92

Pediatrics 2004;114:1– 8

Conclusions

Take home messages • PCT: not a perfect biomarker of sepsis,
but currently the most effective tool to: – Individualize antibiotic use in LRTIs – Reduce AB treatment duration
• CRP: urgent need for well-designed RCTs • But:
– any infection is far too complex to be reduced to a single cutoff of any biomarker
– PCT still not cost-beneficial in most countries

Surgeon General‘s Warning
Procalcitonin without Doctors
can do harm!
Doctors without Procalcitonin even more!
Medicine
IS THERE AN INFECTION? IS THERE AN INFECTION?
Medicine
Courtesy: Beat Müller







