

ProvenCare®:Management of the Acute
COPD Exacerbation
Patricia Maani-Fogelman DNP
Ruby A Weller CRNP
Division of Pulmonary, Critical Care and Sleep Medicine
Geisinger Medical Center
Danville PA
PCNP Nov 2016

COPD
A preventable and treatable disease state characterized by
airflow limitation that is not fully reversible. The airflow
limitation is usually progressive and is associated with an
abnormal inflammatory response of the lungs to noxious
particles or gases, primarily caused by cigarette smoking.
Although COPD affects the lungs, it also produces significant
systemic consequences. (ATS/ERS Definition)

Fast Facts: The Cost of Healthcare
Today, 18% of the United States’ gross domestic product (GDP) is spent on healthcare:- $3 trillion is spent on healthcare annually in the US—twice the amount spent on food.- 33% is spent on hospitalization costs
By 2037, that percentage is expected to increase to 25%– Spending is unsustainable. – Despite these high expenditures, health outcomes in the U.S. are not
considerably better than other high-income countries.
Institute of Medicine (IOM). (2013a). Delivering affordable cancer care in the 21st century, workshop summary.http://www.nationalacademies.org/hmd/Reports/2013/Delivering-Affordable-Cancer-Care-in-the-21st-Century.aspxInstitute of Medicine (IOM) (2013b). Delivering high-quality cancer care: charting a new course for a system in crisis. http://www.nationalacademies.org/hmd/Reports/2013/Delivering-High-Quality-Cancer-Care-Charting-a-New-Course-for-a-System-in-Crisis.aspx
Martin, A.B., Hartman, M., Benson, J., Catlin, A., & the National Health Expenditure Accounts Team. (2016). National health spending in 2014: faster growth driven by coverage expansion and prescription drug spending. Health Affairs, 35(1), 1150-1160. doi: 10.1377/hlthaff.2015.1194.

COPD Is a Major Public Health Problem
On average, more people die every day from COPD than
diabetes or breast cancer:
– 377 per day from COPD
– 193 per day from diabetes
– 112 per day from breast cancer
Qaseem, Wilt, et al., for the American College of Physicians, the American College of Chest Physicians, the American Thoracic Society, and
the European Respiratory Society* Diagnosis and Management of Stable Chronic Obstructive Pulmonary Disease: A Clinical Practice
Guideline Update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and
European Respiratory Society . Ann Intern Med. 2011;155:179-191.

Age-adjusted prevalence (%) of self-reported physician diagnosedCOPD among adults aged >/= 25 years, by state/United States.Behavioral Risk Factor Surveillance System, 2011 .
|5
COPD Surveillance—United States,1999-2011.Ford et al., CHEST 2013; 144(1):284 –305.

|6

COPD Is a Major Public Health Problem: 2014 CDC
• Number of adults with diagnosed chronic bronchitis in the past year: 8.7 million
• Percent of adults with diagnosed chronic bronchitis in the past year: 3.6%
• Number of adults who have ever been diagnosed with emphysema: 3.4 million
• Number of visits to emergency departments with chronic and unspecified bronchitis as the primary hospital discharge diagnosis: 285,000
• Percent of SNF residents with COPD: 10.8%
• COPD is currently the 3rd-leading cause of death in the United States.
http://www.cdc.gov/nchs/fastats/copd.htm
American Lung Association. Trends in COPD (Chronic Bronchitis and Emphysema): Morbidity and Mortality. August 2011. www.lungusa.org.

Fast Facts: COPD
• COPD is an important cause of hospitalization in our aged population.
- Approximately 65% of discharges were in the 65 years and older population in 2010.
• In 2010, the cost to the nation for COPD was projected to be approximately $49.9 billion, including:
• $29.5 billion in direct health care expenditures,
• $8.0 billion in indirect morbidity costs and
• $12.4 billion in indirect mortality costs.
1. National Institutes of Health, National Heart, Lung & Blood Institute. Morbidity and Mortality: 2009 chart book on cardiovascular, lung and blood diseases. www.nhlbi.nih.gov/resources/docs/cht-book.htm.
2. American Thoracic Society/European Respiratory Society. Standards for the diagnosis and management of patients with COPD. Updated 2005. Version 1.2. www.thoracic.org/go/copd.

ATS Update on Dyspnea
Efforts to cure disease are the focus of much biomedical research and tend
to grab the public's attention.
However, the duty to alleviate suffering must remain a top priority.
It is our hope that this document summarizes the progress that has been
made and what remains to be done to allow our patients to enjoy one of
our most primal needs—breathing.

COPD: Multicomponent Disease with Complex Pathophysiology
►Loss of alveolar attachments
►Loss of elastic recoil
►Increased smooth muscle contraction
Airflowlimitation
Airwayinflammation
►Increased numbers ofinflammatory cells/activation:► CD8+ T-lymphocytes► Monocytes/
macrophages► Neutrophils► Mast cells
►Elevated inflammatorymediators: IL-8, TNF-,LTB-4, and oxidants
►Protease/anti-proteaseimbalance
Mucociliarydysfunction
►Mucus hypersecretion
►Reduced mucociliarytransport
►Mucosal damage
Structuralchanges
►Goblet cell hyperplasia/metaplasia
►Mucous gland hypertrophy
►Increased smooth muscle mass
►Airway fibrosis
►Alveolar destruction
Systemiccomponent
►Poor nutritional status
►Reduced BMI
►Impaired skeletal muscle
► Weakness
► Wasting
Adapted from Rodríguez-Roisin R. COPD: J COPD. 2005;2:253-262.

• As a result of their illness, these individuals suffer from:
• leading restricted lives
• experiencing social isolation
• being discredited
• burdening others

Consider COPD if:
• Smoking history
• Occupational/environmental exposure
• Breathlessness with exertion
• Chronic cough
• Regular sputum production
• Frequent winter bronchitis
• Wheeze

History
Past medical history– Pneumonia
– Other respiratory illnesses
Exposure– Environmental
– Agriculture
– Smoking
– Occupational
Family history
Weight loss or gain
Recent visits to ED/hospitalization
Smoking history– Pack years
– Max per day
– Passive exposure
Current functional status

History
• Dyspnea/breathlessness– Quantify if possible
– Severity
– What exacerbates SOB
– Wheezing
• Sleep limitation– Orthopnea
– PND
• Duration of symptoms– Age of onset
• Medications– Compliance
– Rescue med use
– Steroids – current and recent use
– Oxygen use
– Verify inhaler technique
• Cough– Sputum
• Color
• Consistency
• Amount
– Hemoptysis

Am J Respir Crit Care Med, http://www.atsjournals.org/doi/abs/10.1164/rccm.201204-0596PP
Published in: Jørgen Vestbo; Suzanne S. Hurd; Alvar G. Agustí; Paul W. Jones; Claus Vogelmeier; Antonio Anzueto; Peter J. Barnes; Leonardo M. Fabbri; Fernando J. Martinez; Masaharu Nishimura; Robert A. Stockley; Don D. Sin; Roberto Rodriguez-Roisin; Am J Respir Crit Care Med 2013, 187, 347-365. DOI: 10.1164/rccm.201204-0596PP Copyright © 2013 by the American Thoracic Society
Combined COPD Assessment:
When assessing risk, choose the highest risk according to GOLD spirometricgrade or exacerbation history.

ProvenCare®
• Geisinger’s team based intensive treatment program which assures that the best care is delivered to patients in our ProvenCare programs.
• ProvenCare portfolio includes: CABG, PCI, Bariatric Surgery, Thoracic Surgery and COPD.

• Multifaceted initiative that:
• Creates evidence-based "bundles" of discrete clinical care elements
• A fixed per-case rate for inpatient procedures and for pregnancy, that covers all aspects of preadmission, inpatient and follow-up care
• A "patient compact" that provides education and encouragement for patients to become more engaged in their own care.
ProvenCare®

ProvenCare®
• Reengineered care bundles based on guidelines: incorporate clinically relevant steps drawn from best practices and/or evidence-based care guidelines into the routine workflow.
• Care elements involve appropriate screenings, interventions, medications, and monitoring and are categorized according to preadmission, operative, postoperative, discharge, & post-discharge care.

ProvenCare®
• Electronic support: EPIC tools (e.g., checklists, default documentation templates, health maintenance gap reminders, and automated order sets) prompt clinicians to either adhere to the care elements or document justification for non-adherence.
• Gaps in care are highlighted so that they can be completed promptly.
• Bundled pricing: For inpatient services, ProvenCare® bundles all professional and technical fees for the episode of care into one fixed case rate.

COPD ProvenCare®
• All COPD ProvenCare® patients who come to the Pulmonary clinic on a post-discharge visit to receive assessments for Advance Care Planning, Caregiver Strain, and Mental Health.
• For Moderate to Very Severe COPD:
• Providers may place a referral to Pulmonary Palliative Shared Modality Clinic, otherwise patients followed by Pulmonary medicine
• Goal: ensure COPD patients are receiving care that is meeting best practice guidelines.

ProvenCare® COPD: System Wide EMR-based notification
A banner will appear in a patient’s chart once
enrolled.
Can be seen in the Patient Summary section of
a chart.

For Advanced COPD
• Patients enrolled in COPD ProvenCare® with advanced disease may be referred to the shared modality Pulmonary-Palliative Medicine Clinic at GMC.
• Patients with advanced illness are reviewed in CALD and referred for advanced therapy if indicated, e.g. transplant, LVRS.
• Referrals may come from our department or community providers caring for COPD patients.
• Advanced illness planning is initiated in clinic with patient/family/caregivers with ongoing management of pulmonary disease.

Dyspnea Exercise

ASSESSMENT and MANAGEMENTOF
COPD
|24

MMRC: Modified Medical Research Council
0: DOE with strenuous exercise
1: DOE walking up a steep hill
2: DOE walking on level ground, must stop occasionally due to dyspnea
3: Must stop due to dyspnea after walking 100 yards, or after a few minutes
4. Cannot leave house; dyspnea with dressing/undressing
MMRC score: *** points

CAT: COPD Assessment Tool
Cough (0-5): *** points
Sputum (0-5): *** points
Chest Tightness (0-5) : *** points
DOE, hill or stairs (0-5): *** points
Home Activity Limitation (0-5) *** points
Confidence leaving home (0-5) *** points
Sleep Quality (0-5) *** points
Energy Level (0-5) *** points
Total Points: ***
(CAT Score >= 10 is correlated with increased symptoms)(Trademark, GlaxoSmithKline, 2009)

GOLD Criteria: Global Strategy for Diagnosis, Management and Prevention of COPD
In patients with FEV1/FVC < 0.70:
• GOLD 1: Mild FEV1 > 80% predicted
• GOLD 2: Moderate 50% < FEV1 < 80% predicted
• GOLD 3: Severe 30% < FEV1 < 50% predicted
• GOLD 4: Very Severe FEV1 < 30% predicted
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease – Updated 2009. www.goldcopd.org. Accessed September 13, 2010. 2Based on Post-Bronchodilator FEV

Patient Characteristic SpirometricClassification
Exacerbations per year
CAT mMRC
ALow Risk
Less SymptomsGOLD 1-2 ≤ 1 < 10 0-1
BLow Risk
More SymptomsGOLD 1-2 ≤ 1 > 10 > 2
CHigh Risk
Less SymptomsGOLD 3-4 > 2 < 10 0-1
DHigh Risk
More SymptomsGOLD 3-4 > 2 > 10
> 2
Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD
When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.)
© 2015 Global Initiative for Chronic Obstructive Lung Disease

Severity of COPD at Initial Spirometry-Confirmed Diagnosis
Very Severe FEV1 <30%
Moderate FEV1 ≥50% to <80%
of patients already had moderate to very severe COPD at initial spirometry-confirmed diagnosis1
81%
.
Of patients with a COPD diagnosis in an ~250,000-member managed care population, 1520 patients were continuously enrolled for 12 years and had a pulmonary function test.
% o
f p
atie
nts
at
dia
gn
osi
s*
*Based on pulmonary function test results of 366 patients who had COPD confirmed at their initial pulmonary clinic spirometry assessment.
SevereFEV1 ≥30% to <50%
Primary Endpoint: COPD Severity at Diagnosis
n=180 n=96 n=19

Impact of Chronic Lung Disease
Complex coordination of care is required
Oxygen DME’s
Physical Therapy/Pulmonary Rehab
Symptom management
Palliative care
Surgeons
Radiation/medical oncology
PCP’s caring for other co-morbidities
Medication adherence concerns

COPD Comorbidities
• Over half of patients will have comorbidities– Hypertension
– Chronic renal failure
– Diabetes
– Arrhythmias, CAD, CHF
– Cerebrovascular disease
– Depression
• These do not trend as disease progresses with the exception of becoming underweight.
• Obesity paradox

• Relieve symptoms
• Prevent disease progression
• Improve exercise tolerance
• Improve health status
• Prevent and treat complications
• Prevent and treat exacerbations
• Reduce mortality
GOALS of COPD MANAGEMENT

Treatment
• Smoking cessation
• Inhaled bronchodilator therapy
• Short term corticosteroids for acute episodes
• Oxygen
• Non invasive ventilation
• Pulmonary rehabilitation
• Pneumococcal & influenza vaccines
• Treat anxiety & depression
• Nutrition
• Occupational therapy
• LVRS
• Transplant
• Bullectomy
• Palliative Care

More Frequent and More Severe Exacerbations as COPD Disease Severity Increases
GOLD Stage
% o
f P
atie
nts
Hurst, et al. New Engl J Med. 2010;363:1128-1138.
Data from the first year of follow-up
P<0.001 for both comparisons

COPD EXACERBATION
|35

|36
COPD Exacerbation: Definition
> 2 of 3 major criteria: worsened dyspnea increased sputum volume increased sputum color
OR
1 major criterion + 1 minor criterion: sore throat symptoms of a head cold (URI) fever without other explanation worsened coughing or wheezing
Ferguson GT, et al. Respir Med (2008) 102(8):1099-1108.

|37
COPD Exacerbation (cont.)
Symptoms present for > 2 consecutive days above the patient's normal day-to-day variation.
Severity:Mild: symptoms self-managed by the patientModerate: Systemic (oral) steroid with antibiotic use if infection suspected (PCT)Severe: moderate + hospitalization.
Reference: Ferguson GT, et al. Respir Med (2008) 102(8):1099-1108.

ProvenCare® COPD
• Nurse Specific BPE’s:
– Ensuring ordered labs are drawn
– Giving ordered medications
– Documenting oxygen saturations
• Standard SPO2 documentation
– Documenting education
• Standard documentation
– Giving ordered vaccines

• Treatment with corticosteroid reduces likelihood of treatment failure and relapse at 1 month
– Decreased LOS
– Improved lung function
– Improvement of breathlessness
• More side effects with IV steroids
• Less is more
– 5 days of 20 mg daily
COPD Exacerbation
ProvenCare® COPD Nursing BPE’s
• ABG within 24 hours of admission.
• Nasopharyngeal swab within 24 hours of admission.
• ECG upon admission.
• Pro-calcitonin level drawn within 48 hours of admission.
• Steroids initiated.
• Antibiotics initiated.
• Bronchodilator therapy initiated.
• Flu vaccine given if needed.
• Pneumonia vaccine given if needed.

ProvenCare® COPD Nursing BPE’s
Smoking cessation education documented
– Standard documentation
VTE prophylaxis (if appropriate)
– Standard documentation for stockings, SCDs, AV impulse boots.
– Medication if ordered and given.
Daily room air trial if patient is on less than 6L O2 via nasal cannula
– Nursing comm. order
– Standard documentation
COPD education sometime prior to discharge
– Core Measures Education Topics
• Standard documentation.

Characteristics of Patients Admitted for the First Time for COPD Exacerbation
Objective:
• To describe the characteristics of patients admitted for the first time for a COPD exacerbation, both at the time of admission and after reaching clinical stability
Study Design:
• Prospective, multicenter study in nine teaching hospitals in Spain
• All patients who were admitted for the first time for a COPD exacerbation episode January 2004 to March 2006
• 604 eligible patients; N=342 participated, mean age 67.5 years, 42% current smokers, mean post BD FEV1 47% of predicted during admission
Balcells E, et al. Respir Med. 2009;103:1293- 1302.

Exacerbations Occur at All Severity Levels
Balcells E, et al. Respir Med. 2009;103:1293- 1302.
Characteristics at time of first exacerbation Participants (n=342)
Length of hospital stay 7 days
Previous diagnosis of respiratory illness (self-reported) 64%
Any respiratory drug treatment 56%
Characteristics following first exacerbation* Participants (n=342)
COPD Severity
I: Mild (FEV1>80%) 6%
II: Moderate (FEV1>50% < 80%) 48%
III: Severe (FEV1>30, <50%) 39%
IV: Very Severe (FEV1<30%) 8%

Evaluation of Link Between Exacerbations and Decline in Lung Function
Objective:
• Evaluate the relationship between the frequency of exacerbations and the decline in lung function
Study Design:
• Included patients with COPD attending outpatient clinics (FEV1 <70% of predicted)
• In diaries, 109 patients recorded daily PEF, increase in symptoms (above normal)
Donaldson GC, et al. Thorax. 2002;57:847-852.

Frequency of Exacerbations Is Associated With a Decline in Lung Function
Results based on a secondary analysis of 32 patients who recorded daily FEV1. The median rate of exacerbations seen at clinic was 1.5 per patient per year.
Donaldson GC, et al. Thorax. 2002;57:847-852.
<1.5 >1.5
Exacerbations Per Year

Evaluation of the Relationship Between Exacerbations and Quality of Life
Objective:
• Evaluate the effect of the severity and frequency of exacerbations on quality of life
Study Design:
• Included 73 patients with COPD attending outpatient clinics (FEV1 <70% of predicted)
• Patients measured daily PEF and respiratory symptoms for 1 year
Seemungal T, et al. Am J Respir Crit Care Med. 1998;157:1418-1422.
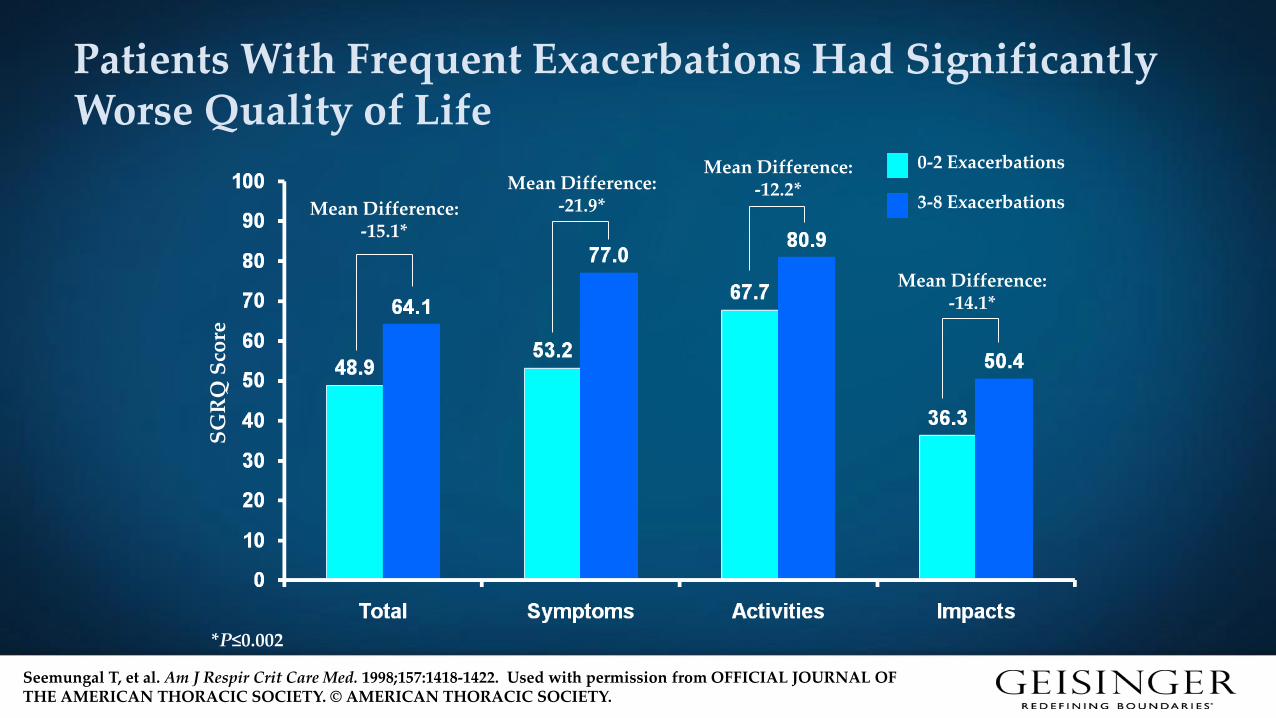
Patients With Frequent Exacerbations Had Significantly Worse Quality of Life
Seemungal T, et al. Am J Respir Crit Care Med. 1998;157:1418-1422. Used with permission from OFFICIAL JOURNAL OF THE AMERICAN THORACIC SOCIETY. © AMERICAN THORACIC SOCIETY.
SG
RQ
Sco
reMean Difference:
-15.1*
Mean Difference: -21.9*
Mean Difference: -12.2*
Mean Difference: -14.1*
*P≤0.002
0-2 Exacerbations
3-8 Exacerbations

Patients With More Frequent Exacerbations Had Significantly Worse Depression Scores
Quint JK, et al. Eur Respir J. 2008;32:53─60.
12.0
*≥3 COPD exacerbations in the preceding year Arbitrary cut-off based on the median exacerbation frequency in the cohort
Baseline Depression Scores by COPD Exacerbation Frequency
Med
ian
Dep
ress
ion
Sco
re
•35% of infrequent exacerbators had a CES-D score >16•54% of frequent exacerbators had a CES-D score >16
P=0.03

Evaluation of Recovery Time for Lung Function and Symptoms Following Exacerbations
Objective:
• To evaluate the recovery of lung function and symptoms following an exacerbation
Study Design:
• A cohort of 101 patients with COPD (FEV1 <70% of predicted) were followed over 2.5 years
• Patients recorded daily PEF and symptoms on diary cards
Seemungal T, et al. Am J Respir Crit Care Med. 2000;161:1608-1613.
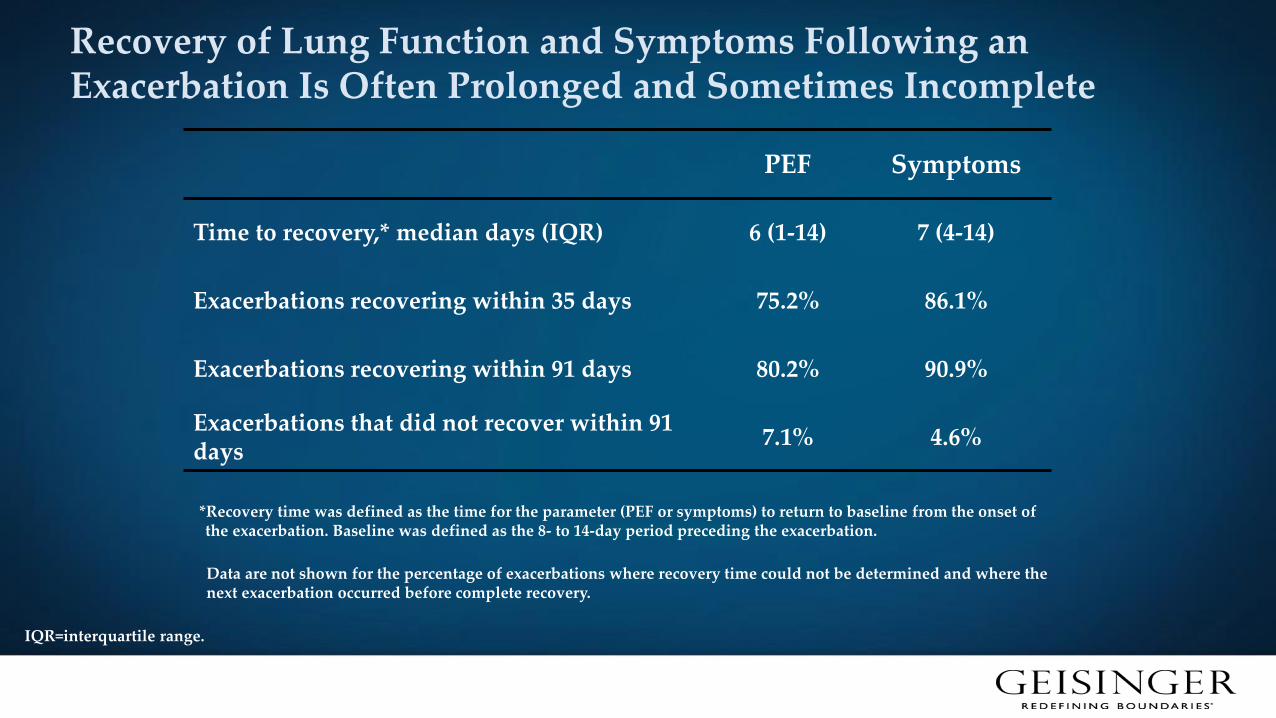
Recovery of Lung Function and Symptoms Following an Exacerbation Is Often Prolonged and Sometimes Incomplete
PEF Symptoms
Time to recovery,* median days (IQR) 6 (1-14) 7 (4-14)
Exacerbations recovering within 35 days 75.2% 86.1%
Exacerbations recovering within 91 days 80.2% 90.9%
Exacerbations that did not recover within 91 days
7.1% 4.6%
Seemungal T, et al. Am J Respir Crit Care Med. 2000;161:1608-1613.
*Recovery time was defined as the time for the parameter (PEF or symptoms) to return to baseline from the onset of the exacerbation. Baseline was defined as the 8- to 14-day period preceding the exacerbation.
IQR=interquartile range.
Data are not shown for the percentage of exacerbations where recovery time could not be determined and where the next exacerbation occurred before complete recovery.
Evaluation of the Relationship Between Exacerbations Requiring Hospitalization and Survival
Objective:
Evaluate whether severe exacerbations requiring hospital treatment have a direct effect on mortality
Study Design:
Prospective study of 304 male patients with stable COPD (no exacerbations in the previous month)
Patients were divided into 3 groups based on the number of severe exacerbations in the year of the study:
Group A (no exacerbations)
Group B (1-2 exacerbations)
Group C (≥3 exacerbations)
Soler-Cataluna JJ, et al. Thorax. 2005;60:925-931.

COPD Patients With a Greater Frequency of Severe Exacerbations* Per Year Have a Higher Risk of All-Cause Mortality
Soler-Cataluna JJ, et al. Thorax. 2005;60:925-931. Reproduced with permission from the BMJ Publishing Group.
1.0
0.8
0.6
0.4
0.2
0.00 10 20 30 40 50 60
Pro
bab
ilit
y o
f S
urv
ivin
g
Time (months)
P<0.0002
A
B
P=0.069
C
P<0.0001
No exacerbations
1-2 exacerbations
≥3 exacerbations
*Severe exacerbations = exacerbation required emergency visits or hospital admissions.

BODE Score
BODE Score:– FEV1 after BD >65 is 0, 50-64 is 1, 36-49 is 2, <35 is 3– 6MWT > 350m is 0, 250-349m is 1, 150-249 is 2, <149 is 3– Dyspnea w/strenuous is 0, w/slight hill is 0, w/level ground is 1, 100 yards is 2, cannot level
home is 3– BMI >21 is 0 and <21 is 1
Predicted Survival at 52 months: – 0-2 points: 80% – 3-4 points: 40% – 5-6 points: 30% – 7-10 points: 20%
Celli BR et al. The Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive
Pulmonary Disease. NEJM 2004;350:1005.

Kaplan–Meier survival curve.
Jacques Piquet et al. Eur Respir J 2013;42:946-955
©2013 by European Respiratory Society

Percentage of dead patients according to the number of hospital admissions for acute exacerbation of chronic obstructive pulmonary disease (COPD) within the previous year.
Jacques Piquet et al. Eur Respir J 2013;42:946-955
©2013 by European Respiratory Society

Final Thoughts
• High Quality includes medical therapy maximization with integration of the multidisciplinary group to promote best practice and assure best QOL for this challenging population with a chronic, progressive and ultimately fatal lung disease.
• Increased knowledge is essential: Outreach, education, didactics, joint conferences, interdisciplinary rounds.
• Importance of interdisciplinary approach to care.
|56

Questions?







