

Respiratory Distress in New born
Presented by Dr. Ankit AgarwalGuided by: Dr. J.P. Jain
Dept. of PediatricsNIMS, Jaipur

Overview• General Considerations
– Epidemiology– Definition and Clinical Features– Assessment of severity– Causes– Approach to a New born with
resp. distress
• Meconium Aspiration Syndrome– Epidemiology– Etiopathogenesis– Clinical Features– Diagnosis – Management
• Respiratory Distress Syndrome– Epidemiology– Etiopathogenesis– Clinical Features– Diagnosis – Management– Surfactant Therapy– Complication
• Transient Tachypnea of Newborn– Epidemiology– Etiopathogenesis– Clinical Features– Diagnosis – Management
Epidemiology
• Commonest problem encountered within the first few hours of life.
• It occurs in approximately 1%-6% of live births
• Responsible for about 20% of neonatal mortality
Gen
eral
Con
side
ratio
ns

Definition and Clinical Features
Tachypnea
AND
Expiratory Grunt OR Inspiratory Retraction
Only Tachypnea is NOT Respiratory Distress
• Cyanosis• Nasal Flaring• Desaturation• Lethargy/Poor feeding
• Pallor• Decreased Breath Sounds
+\- Rales or Ronchi
Other Features
Gen
eral
Con
side
ratio
ns

Gen
eral
Con
side
ratio
ns
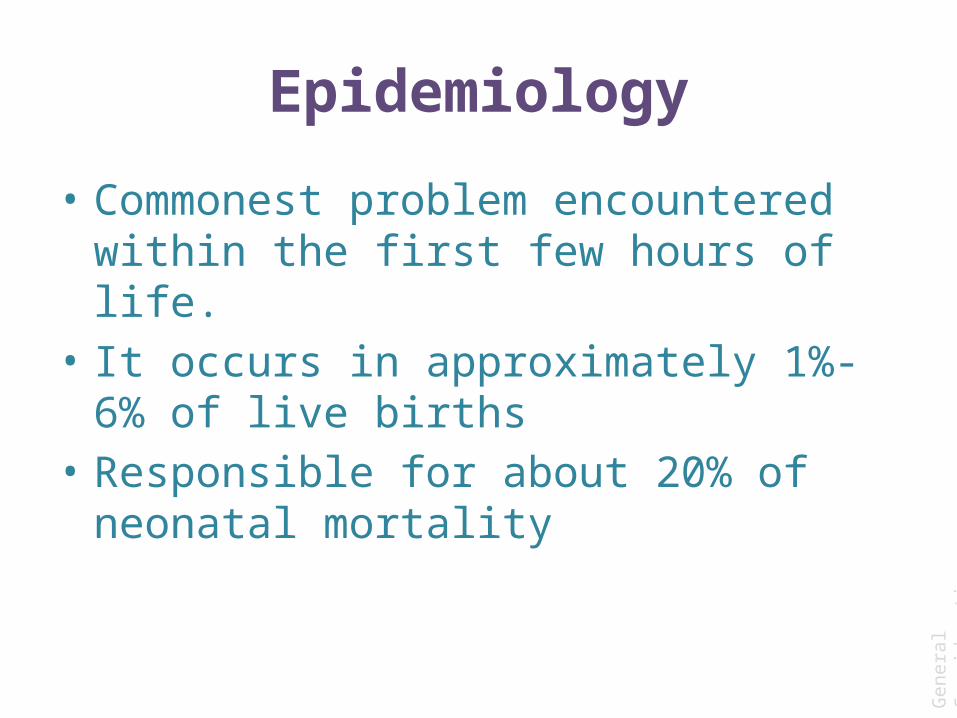
Assessment of SeverityDowne’s Scoring System
Score 0 1 2
Respiratory Rate (rate/min)
<60 60-80 >80
Cyanosis None in room air No cyanosis in 40% oxygen
Requiring more than 40% ambient oxygen
Retractions None Mild Moderate to Severe
Grunting None Audible with Stethoscope
Audible without Stethoscope
Air Entry Good Decreased Barely Audible
Gen
eral
Con
side
ratio
ns
Modified Downe’s Scoring System
No cyanosis with oxygen support
Cyanosis in spite oxygen support

Interpretation:
<4: No Respiratory Distress
4-7: Clinical Distress
>7: Impeding Respiratory Failure
Downe’s Score should be noted every 30mins-1 hour to monitor progression of respiratory
distress.
Gen
eral
Con
side
ratio
ns
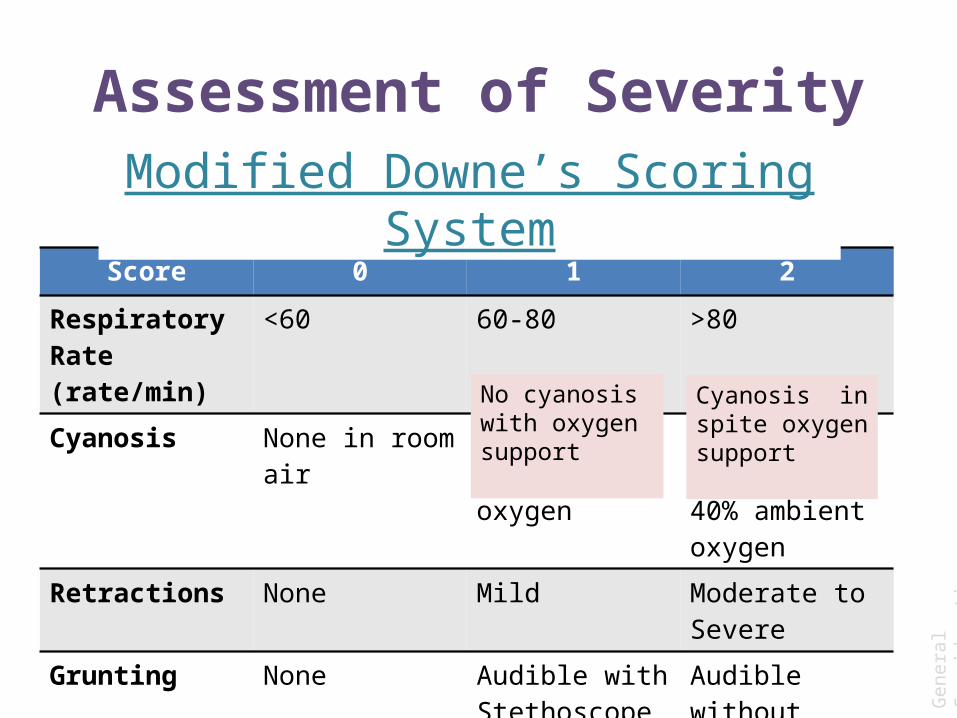
Silverman-Andersen Retraction Scoring
InterpretationScore 0-3 = Mild respiratory distress Score 4-6 = Moderate respiratory distress Score > 6 = Impending respiratory failure Score 10 = Severe Respiratory distress
Gen
eral
Con
side
ratio
ns
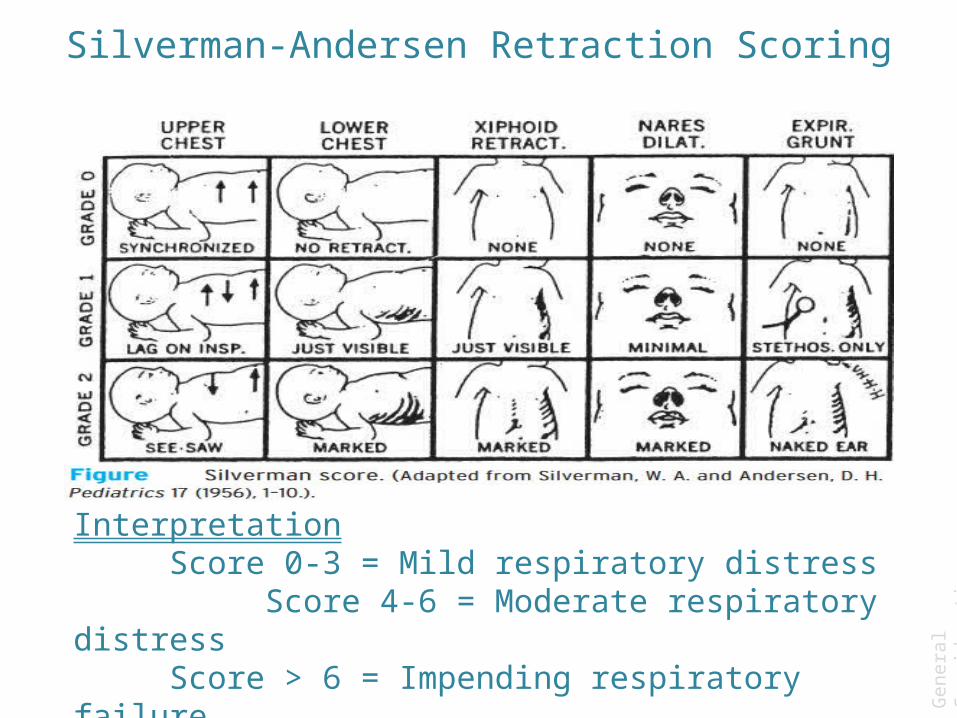
A progressively increasing O2 requirement to maintain saturation is also a sensitive indicator of the severity and progress of distress
>95% Term baby, pulmonary hypertension (PPHN) 88-94% 28-34 weeks preterm85-92% Below 28 weeks gestational age
Guidelines for monitoring oxygen saturation levels by pulse oximetry
MJAFI, Vol. 63, No. 3, 2007
Gen
eral
Con
side
ratio
ns

Causes
• Pulmonary• Extra-pulmonary
Gen
eral
Con
side
ratio
ns
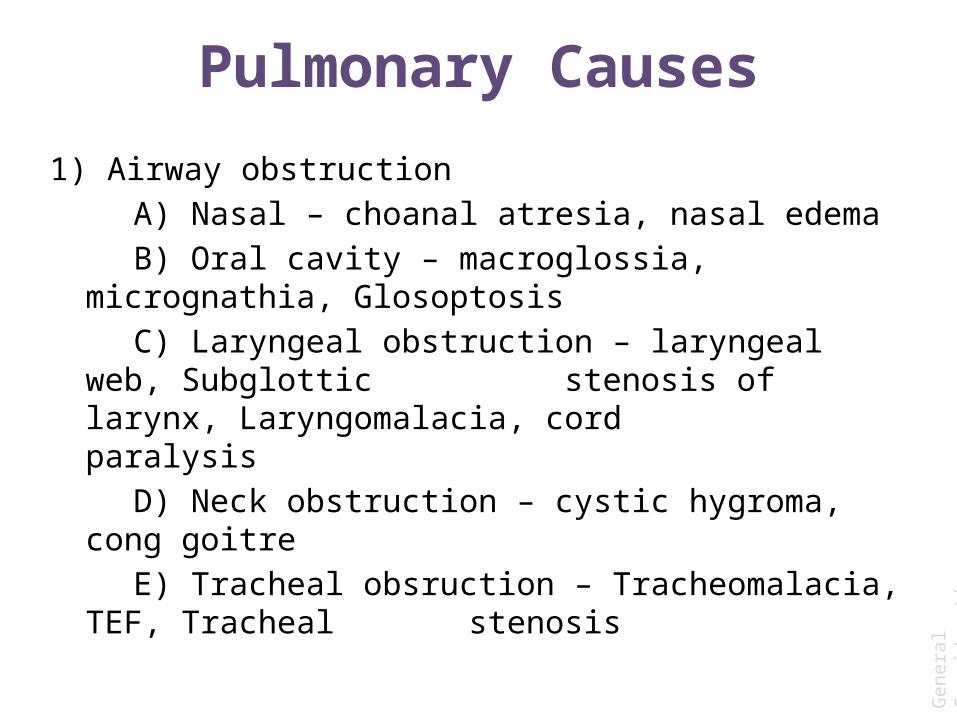
Pulmonary Causes
1) Airway obstruction A) Nasal – choanal atresia, nasal edemaB) Oral cavity – macroglossia, micrognathia, GlosoptosisC) Laryngeal obstruction – laryngeal web, Subglottic
stenosis of larynx, Laryngomalacia, cord paralysis
D) Neck obstruction – cystic hygroma, cong goitreE) Tracheal obsruction – Tracheomalacia, TEF, Tracheal
stenosis
Gen
eral
Con
side
ratio
ns
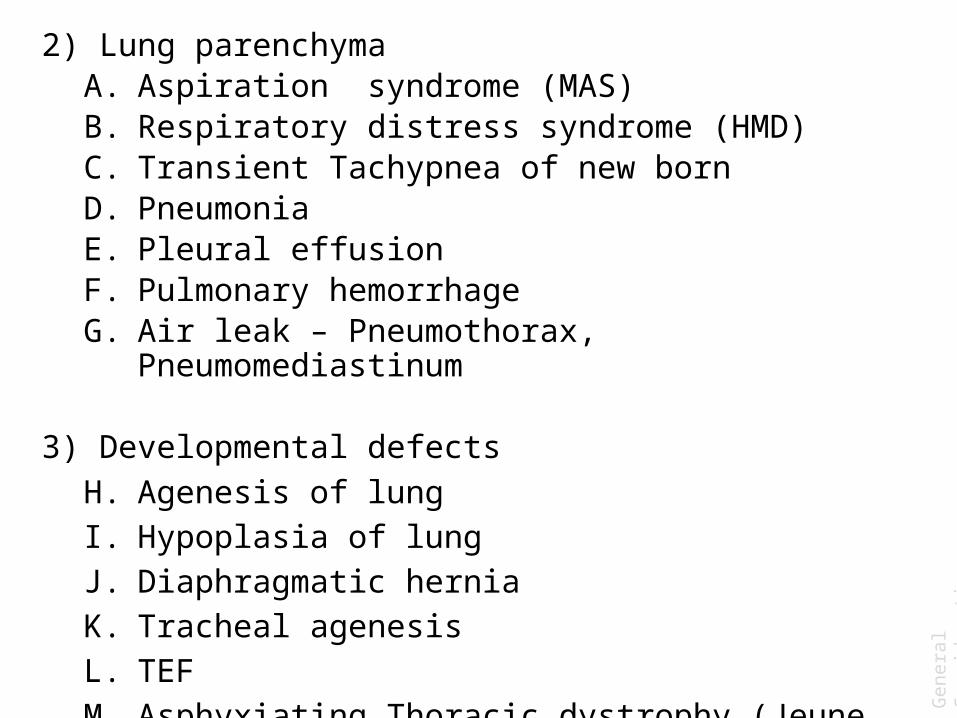
2) Lung parenchymaA. Aspiration syndrome (MAS)B. Respiratory distress syndrome (HMD)C. Transient Tachypnea of new bornD. Pneumonia E. Pleural effusionF. Pulmonary hemorrhageG. Air leak – Pneumothorax, Pneumomediastinum
3) Developmental defects H. Agenesis of lungI. Hypoplasia of lungJ. Diaphragmatic herniaK. Tracheal agenesisL. TEF M. Asphyxiating Thoracic dystrophy (Jeune Syndrome)
Gen
eral
Con
side
ratio
ns

Extrapulmonary Causes
• CNS Trauma or Birth Asphyxia• Cardiac Failure• Metabolic acidosis• Persistent pulmonary hypertension• Diaphragmatic Hernia• Intercostal muscle Paralysis• Others: Hypothermia/Hyperthermia,
Hypoglycemia, Anemia/Polycythemia,
Gen
eral
Con
side
ratio
ns
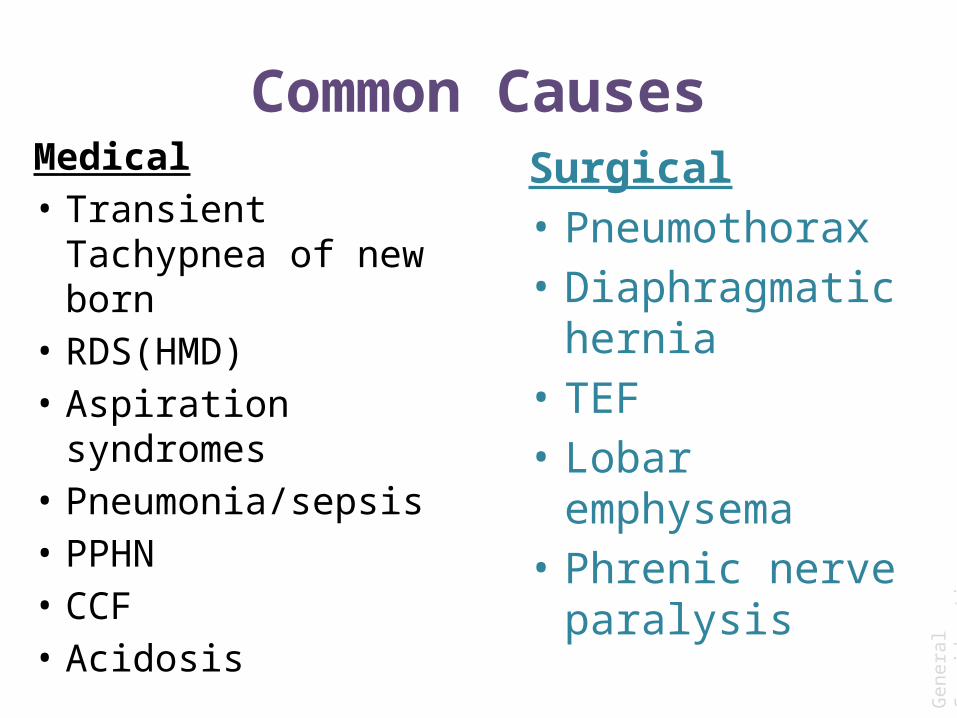
Common CausesMedical• Transient Tachypnea
of new born• RDS(HMD)• Aspiration
syndromes• Pneumonia/sepsis• PPHN• CCF• Acidosis
Surgical• Pneumothorax• Diaphragmatic
hernia• TEF• Lobar emphysema• Phrenic nerve
paralysis
Gen
eral
Con
side
ratio
ns

New Born with Respiratory DistressWhat to do???
Gen
eral
Con
side
ratio
ns

HistoryWhat we need to know Why we need to knowWere there any risk factors in the antepartum period or evidence of fetal distress prior to delivery?
Birth asphyxia or PPHN
Did the mother receive antenatal steroids if it was a preterm delivery?
Antenatal steroids decrease the incidence of HMD by 50%
Was there a history of premature rupture of membranes and fever?
Congenital pneumonia orsepsis
Was there meconium stained amniotic fluid?
MAS is a possibility
Gen
eral
Con
side
ratio
ns
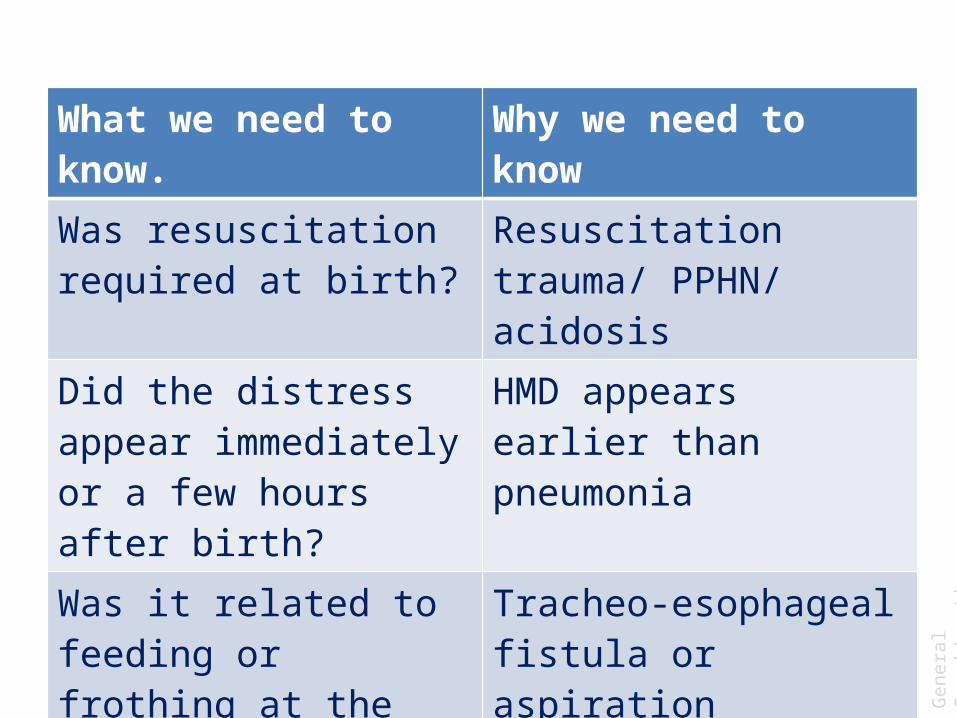
What we need to know. Why we need to knowWas resuscitation required at birth?
Resuscitation trauma/ PPHN/ acidosis
Did the distress appear immediately or a few hours after birth?
HMD appears earlier than pneumonia
Was it related to feeding or frothing at the mouth?
Tracheo-esophageal fistula or aspiration
Does the distress decrease with crying
Choanal atresia
Gen
eral
Con
side
ratio
ns

Signs-Will depend on causeWhat we need to look for Why we need to look forA preterm baby weighing <1500 gms with retractionsand grunt
Likely to have HMD.
Meconium stainedamniotic fluid with an increase in the anterio-posterior diameter of the chest (full chest)
Likely to be suffering from MAS
A depressed baby with poor circulation
Neonatal sepsis with or without congenitalpneumonia.
Gen
eral
Con
side
ratio
ns
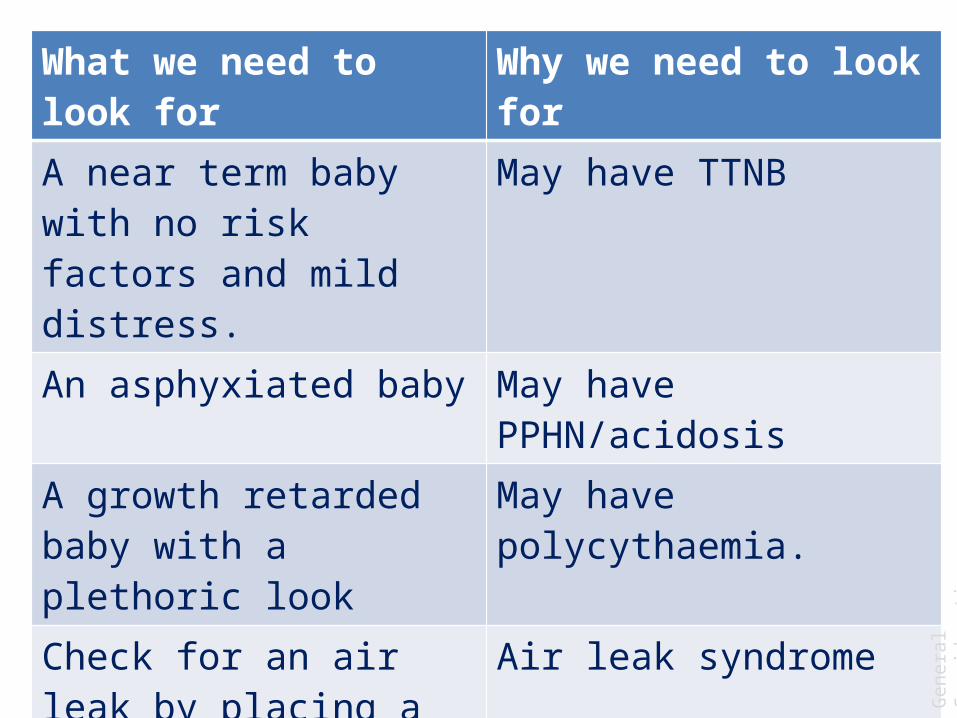
What we need to look for Why we need to look forA near term baby with no risk factors and mild distress.
May have TTNB
An asphyxiated baby May have PPHN/acidosisA growth retarded baby with a plethoric look
May have polycythaemia.
Check for an air leak by placing a light source overthe chest wall in a darkened room.
Air leak syndrome
Inability to pass an 5F catheter through the nostrilof a term baby
Suggestive of choanal atresia.
Gen
eral
Con
side
ratio
ns
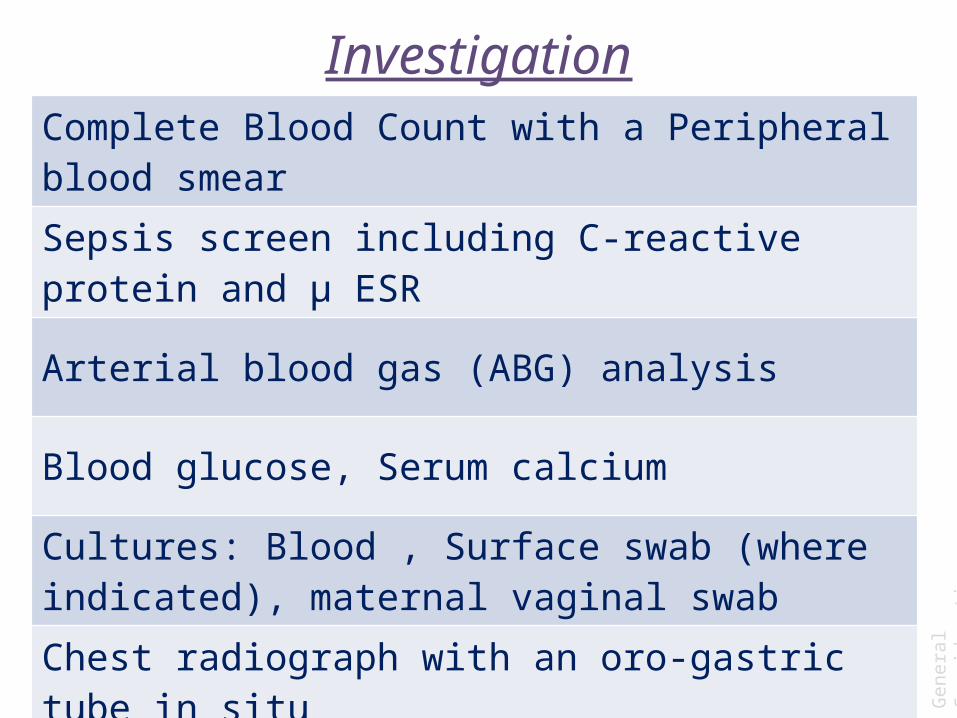
Investigation
Complete Blood Count with a Peripheral blood smear
Sepsis screen including C-reactive protein and μ ESR
Arterial blood gas (ABG) analysis
Blood glucose, Serum calcium
Cultures: Blood , Surface swab (where indicated), maternal vaginal swab
Chest radiograph with an oro-gastric tube in situ
Gen
eral
Con
side
ratio
ns

Management• Clear the airway, ensuring adequate breathing and circulation. • Continuous pulse oximeter monitoring.• Warm, humidified oxygen is given with a head box.• Maintenance of correct temperature is essential. • Fluid and electrolyte management: Electrolyte balance, fluids,
calcium and glucose homeostasis are all equally important.• Maintenance of adequate hemoglobin: Any neonate with
respiratory distress should have a packed cell volume (PCV) above 40% (but less than 75%).
• All preterm babies with respiratory distress should be started on broad spectrum antibiotics. In term babies, decision to start antibiotics would depend on the clinical situation, but the threshold should be low.
Gen
eral
Con
side
ratio
ns

Respiratory SupportRespiratory support is given in the form of continuous positive airway pressure (CPAP) or intermittent mandatory ventilation (IMV). Depends upon condition and severity of distress.
0 1 2 3PaO2
mmHg>60 50-60 <50 <50
PaCO2
mmHg<50 50-60 61-70 >70
pH >7.3 7.20-7.29 7.1-7.19 <7.1
ABG Scoring System
A score of >3 suggests ventilator/respiratory requirement Gen
eral
Con
side
ratio
ns

Indications for starting CPAP are • Downes’ or Silvermann score of >6 at birth • FiO2 requirement of >0.4 to maintain an acceptable
saturation on pulse oximeter. • ABG score of more than 3.
CPAP is said to have failed when the FiO2 requirement is >0.6 or the pressure required to maintain oxygenation exceeds 7-8 cm of H2O.
Mechanical Ventilation: Time cycled pressure limited ventilation is the modality of choice for ventilation. If patient triggered ventilation is used it is given as synchronized intermittent mandatory ventilation (SIMV).
Best outcome are seen in babies with impending respiratory failure or failed CPAP rather than in complete respiratory failure.
Gen
eral
Con
side
ratio
ns

Specific Management depends on the CAUSE of distress
Gen
eral
Con
side
ratio
ns
Meconium Aspiration Syndrome
Definition
MAS is defined as respiratory distress in an infant born through meconium-stained amniotic fluid (MSAF) whose symptoms
cannot be otherwise explained
J Perinatol. 2008 Dec
Mec
. Asp
. Syn
d
Epidemiology
• Most common cause of respiratory distress in term and post-term infants.
• MSAF observed in 5-25% of all births out of which 10% develop MAS.
• One third require ventilator support• 10% develop air leaks • 5-10% of them have a fatal outcome
Mec
. Asp
. Syn
d

What is meconium?
• The term was coined by Aristotle from the Greek word “meconium arion” meaning “opium like”
• Consists of gastrointestinal, hepatic and pancreatic secretions, cellular debris, swallowed amniotic fluid, lanugo, vernix caseosa and blood
• Appear in the fetal intestines by the 10th week of life gradually increasing in amount to reach 200gms at birth
Mec
. Asp
. Syn
d

Cause of MSAF• The passage of meconium from the fetus into
amnion is prevented by lack of peristalsis(low motilin level) , tonic contraction of the anal sphincter, terminal cap of viscous meconium.
• Vagal Stimulation due to in utero hypoxia, acidosis, cord or head compression cause increased peristalsis and a relaxed anal sphincter.
• Fetal maturation (post term) causes high motilin level increased peristalsis
Mec
. Asp
. Syn
d

Risk factors for MAS
• Post term pregnancy• Primigravida• Maternal Anemia• Chorioamnionitis• Prolonged Labour• Fetal Distress• IUGR• Maternal Age >30yrs• Maternal DM
• Maternal heavy cigarette smoking
• Pre-eclampsia / eclampsia
• Oligohydramnios• Antepartum
Hemorrhage
Mec
. Asp
. Syn
d
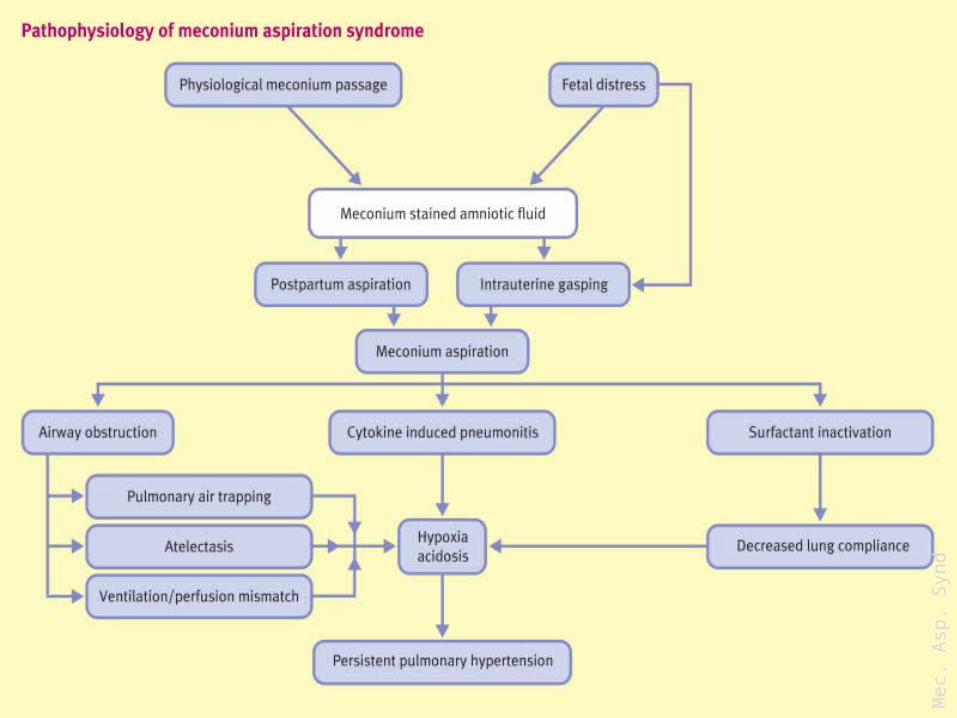
Pathophysiology
1. Mechanical obstruction of airways 2. Chemical Pneumonitis3. Surfactant Inactivation
Mec
. Asp
. Syn
d

Mechanical obstruction of airways
• With onset of respiration – meconium migrates from central to peripheral airways.
• Thick particulate and viscous meconium lead to complete or partial airway obstruction.
• Complete obstruction Atelectasis Ventilation-Perfusion (V-Q) mismatch
• Partial obstruction Ball-valve – air trapping Obstructive Emphysema Risk of pneumothorax (15 – 33%)
Mec
. Asp
. Syn
d

Chemical pneumonitis
• Meconium in the airways initiates an inflammatory reaction
• Meconium inhibits oxidative burst and phagocytosis by neutrophil increased risk of infection
• Meconium induces production of inflammatory cytokines Injury of parenchyma and vascular leakage injury similar to ARDS
Mec
. Asp
. Syn
d
Surfactant inactivation
• Bilirubin, fatty acid, triglycerides, cholesterol and proteins present in meconium alter phospholipid structure of surfactant reduced surfactant function
• Bile has cytotoxic effect on Type II Pneumocytes Reduced surfactant production.
Mec
. Asp
. Syn
d
Mec
. Asp
. Syn
d

Clinical Features
History
• Maternal risk factors present• Term or Post term Infants• Meconium Stained Amniotic fluid (Thick pea
soup/Thin)• IUGR. • Many babies are depressed at birth.(in utero
aspiration)
Mec
. Asp
. Syn
d

Physical examination
• Evidence of postmaturity: peeling skin, long fingernails, and decreased vernix.
• The vernix, umbilical cord, and nails may be meconium-stained, depending upon how long the infant has been exposed in utero.
• In general, nails will become stained after 6 hours and vernix after 12 to 14 hours of exposure .
• umbilical cord staining (thick-15min, thin-1hour)
Mec
. Asp
. Syn
d

Meconium stained umbilical cord
Mec
. Asp
. Syn
d

Meconium stained nails
Mec
. Asp
. Syn
d

• Features of respiratory distress within first few hours of birth
• The chest typically appears barrel-shaped, with an increased anterior-posterior diameter caused by over inflation.
• Auscultation reveals rales and rhonchi -immediately after birth.
• Some patients are asymptomatic at birth and develop worsening signs of respiratory distress as the meconium moves from the large airways into the lower tracheobronchial tree.
• In case of massive meconium aspiration, meconium pigments may be absorbed from lungs excreted in urine. Urine may appear dark brown in colour.
Mec
. Asp
. Syn
d
Diagnosis
MAS must be considered in any infant born through MSAF who develops
symptoms of Respiratory Distress with typical chest x ray findings
Mec
. Asp
. Syn
d
Diagnosis
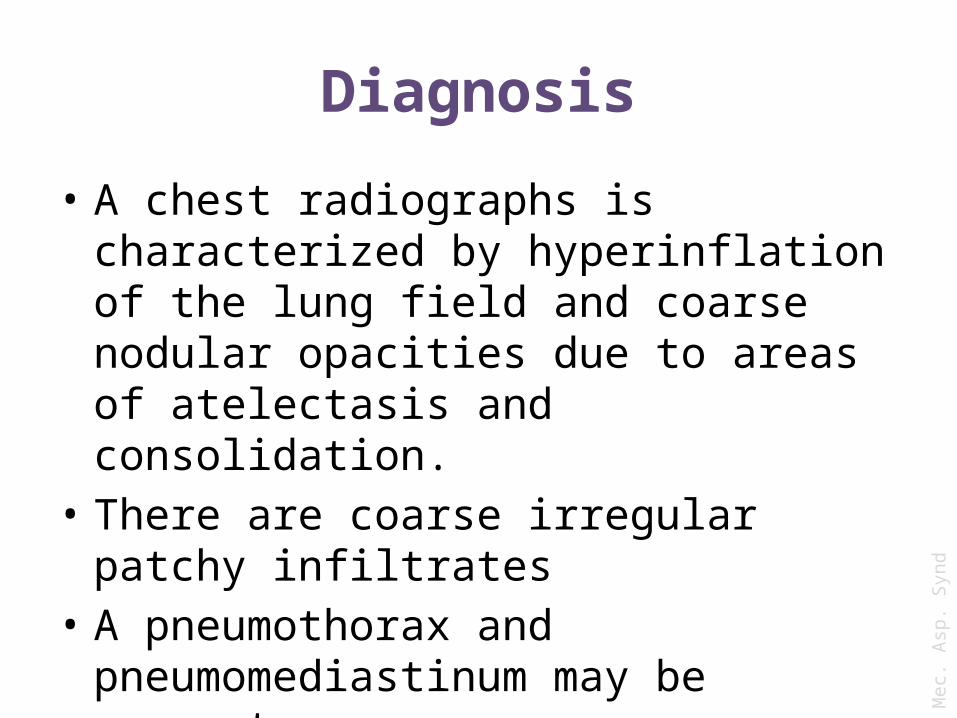
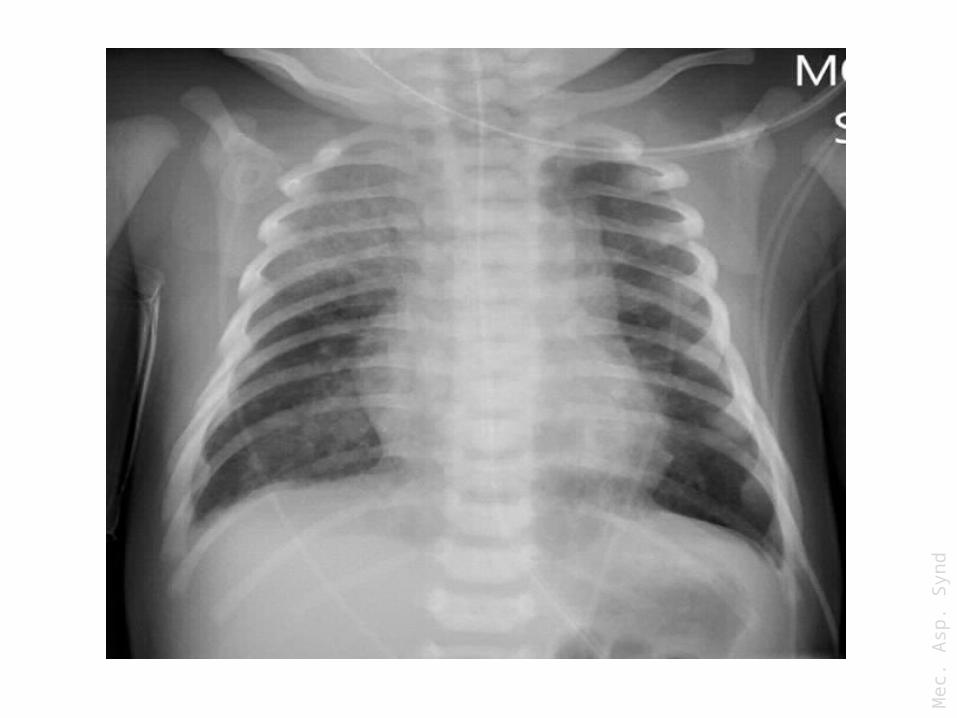
• A chest radiographs is characterized by hyperinflation of the lung field and coarse nodular opacities due to areas of atelectasis and consolidation.
• There are coarse irregular patchy infiltrates • A pneumothorax and pneumomediastinum
may be present .
Mec
. Asp
. Syn
d
Mec
. Asp
. Syn
d
Mec
. Asp
. Syn
d

Mec
. Asp
. Syn
d

Mec
. Asp
. Syn
d
Diagnosis
• Arterial blood gas measurements typically show hypoxemia and hypercarbia.
• Infants with pulmonary hypertension and right-to-left shunting may have a gradient in oxygenation between preductal and postductal samples.
• Echocardiogram for evaluation of Persistent Pulmonary Hypertension.
Mec
. Asp
. Syn
d
Management
• Prenatal management: Key management lies in prevention during prenatal period.
• Identification of high risk pregnancies and close monitoring. Pregnancy that continue past due date, induction as early as 41 weeks may help prevent meconium aspiration.
• If there is sign of fetal distress corrective measure should be undertaken or infant should be delivered in timely manner.
• Amnioinfusion has no role.
Mec
. Asp
. Syn
d
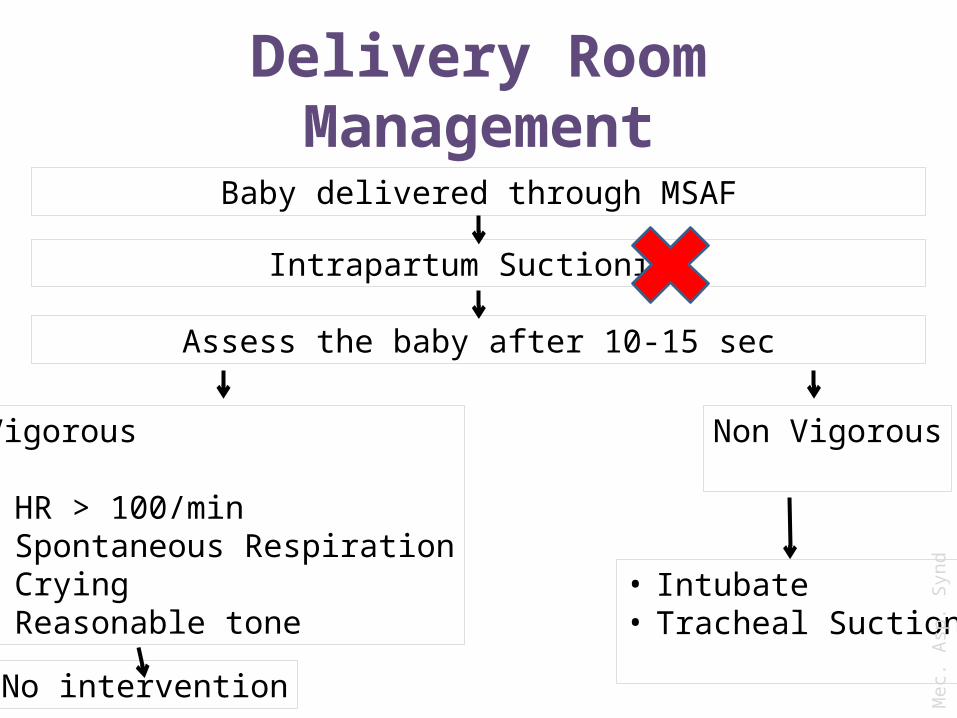
Delivery Room Management
Baby delivered through MSAF
Intrapartum Suctioning
Assess the baby after 10-15 sec
Vigorous
• HR > 100/min• Spontaneous Respiration• Crying• Reasonable tone
No intervention
Non Vigorous
• Intubate• Tracheal Suction
Mec
. Asp
. Syn
d
• When the infant is not vigorous:1. Place under radiant warmer but delay
stimulation.2. Clear airways as quickly as possible. 3. Intubation and then suction directly to the ET
tube. repeat until either ‘‘little meconium is recovered, or until the baby’s heart rate indicates that resuscitation must proceed without delay’’.
4. May also require saline lavage to remove thick particles.
5. After all meconium is sucked out, ventilate the baby with bag and mask.
Mec
. Asp
. Syn
d
Postnatal Management
• Shift to NICU setup with respiratory support facilities available
• Gastric wash with normal saline to reduce gastritis and aspiration of meconium stained products.
• Close monitoring for Respiratory distress. • Most infants who develop symptoms will do
so in the first 12 hours of life.
Mec
. Asp
. Syn
d
Postnatal Management Approach to the ill newborns:1. Maintain temperature2. O2 support by hood
3. 2/3rd restricted IV fluids4. Look for and manage hypoglycemia/ hypocalcemia/
hypotension 5. ??? Antibiotics6. Initiate CPAP/ventilation if indicated7. ??? Surfactant therapy (Bolus/Trachebroncial Lavage) - should
be used in setups where ECMO facility is unavailable8. iNO(Inhaled Nitric Oxide) – when PPHN complicates MAS9. ECMO (Extra Corporeal Membrane Oxygenation)10. Keep high suspicion for Air Leaks and PPHN
Mec
. Asp
. Syn
d

Respiratory Distress Syndrome (RDS)
• Also known as Hyaline Membrane Disease (HMD)• Commonest cause of preterm neonatal mortality• RDS occurs primarily in premature infants; its
incidence is inversely related to gestational age and birth weight
Nelson Textbook of Pediatrics, 18th Ed.
Gestational age Percentages
Less than 28 wks 60-80%
32-36 wks 15-30%
37-39 wk 5%
Term Rare
Resp
. Dis
. Syn
.

Risk Factors
Increased Risk Decreased Risk• Maternal diabetes• multiple births• cesarean section
delivery• perinatal asphyxia• cold stress• history of previously
affected infants
• Chronic or pregnancy-associated hypertension
• maternal heroin use• prolonged rupture of
membranes• antenatal
corticosteroid prophylaxis
Resp
. Dis
. Syn
.
Etiology & Pathophysiology• Lack of surfactant due to immaturity of lungs
is the basic abnormality.• Surface-Active-Agent (Surfactant) which is
produced by type II alveolar cells, reduces surface tension and maintains alveolar stability at low pressure so that end-expiratory alveolar atelectasis does not occur.
• Surfactant production is also compromised in birth asphyxia, acidosis, hypothermia, Rh incompatibility, antepartum hemorrhage and shock
Resp
. Dis
. Syn
.

Resp
. Dis
. Syn
.

Resp
. Dis
. Syn
.
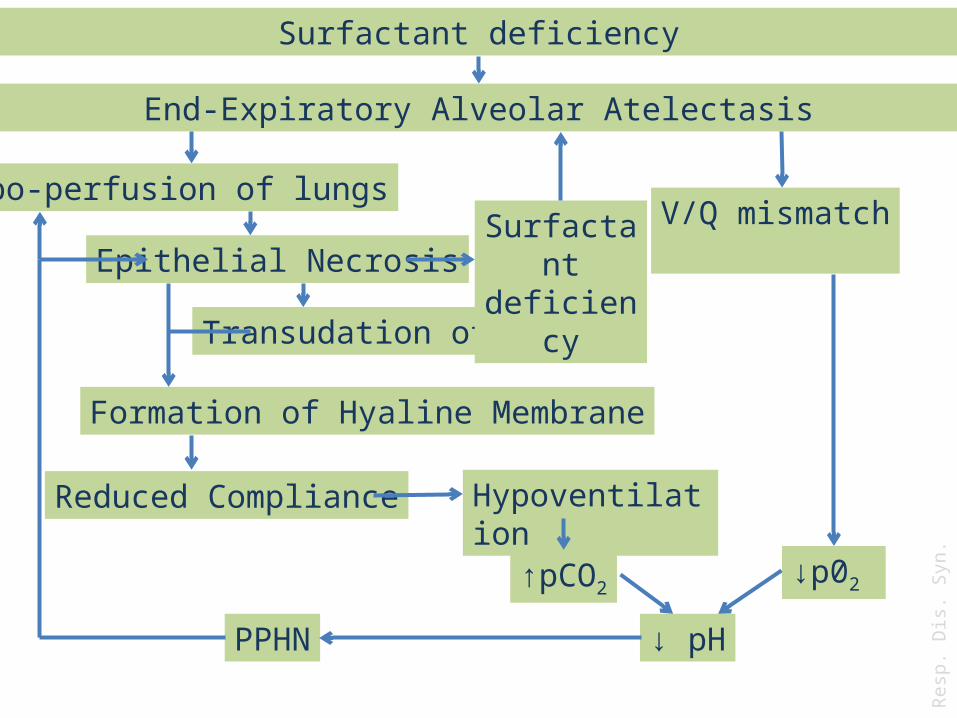
Surfactant deficiency
End-Expiratory Alveolar Atelectasis
Hypoventilation
Hypo-perfusion of lungs
Epithelial Necrosis
Transudation of Plasma
Formation of Hyaline Membrane
V/Q mismatch
Reduced Compliance
↓p02↑pCO2
↓ pHPPHN
Surfactant deficiency
Resp
. Dis
. Syn
.

Clinical Features• Maternal Risk factors present in history• Preterm Infant• Features of respiratory distress usually appear within
few minutes of birth to upto 6 hours of birth• Breath sounds may be normal or diminished with a
harsh tubular quality• Fine rales may be heard, especially posteriorly over
the lung bases• Apnea and irregular respirations occur as infants
tire and are ominous signs requiring immediate intervention
• Respiratory failure may occur in patients with rapid progression of the condition
Resp
. Dis
. Syn
.
• Patient may have a mixed respiratory-metabolic acidosis, edema, ileus and oliguria.
• In most cases, the symptoms and signs reach a peak within 3 days, after which improvement is gradual
• Death is rare on the 1st day of illness, usually occurs between days 2 and 7– associated with alveolar air leaks (interstitial
emphysema, pneumothorax), pulmonary hemorrhage, or IVH.
Resp
. Dis
. Syn
.

Diagnosis
• Amniotic Fluid Lecithin/Sphingomyelin Ratio– ≥2 suggests lung maturity. – ≤1.5 associated with HMD
• Phosphatidyl Glycerol estimation– More specific than L/S ratio– Absence is invariably associated with HMD
• Gastric Aspirate Shake Test– Unreliable if gastric aspirate is contaminated with blood
or meconium– Serial tests can be done to assess maturity of lungs during
course of disease
Resp
. Dis
. Syn
.

• ABG initially shows hypoxemia and later worsening of hypoxemia, hypercapnia and metabolic acidosis
• On X-Ray Chest– Initial X-ray may be normal– Typical pattern develop at 6-12 hours
– Grade 1 (mild cases): symmetrical reticulogranular pattern due to scattered atelectasis
– Grade 2: widespread air bronchogram become visible– Grade 3: reticulogranular pattern becomes
increasingly confluent leading to formation of ground glass opacity due to marked underaeration
– Grade 4: complete white lung fields with obscuring of the cardiac shadow due to global atelectasis Re
sp. D
is. S
yn.

Resp
. Dis
. Syn
.
Prevention
• Suppress Premature labor to gain gestational maturity
• Delay induction of labour till pulmonary maturity is assured by L/S ratio
• Antenatal Steroids to mother– Betamethasone (12mg IM every 24 hr for 2 doses)– Dexamethasone(6mg IM every 12 hr for 4 doses)
Resp
. Dis
. Syn
.
Management1. Shift to NICU setup with respiratory support facilities
available
2. Close monitoring for Respiratory distress.
3. Maintain temperature
4. O2 support by hood
5. 2/3rd restricted IV fluids
6. Look for and manage hypoglycemia/ hypocalcemia/ hypotension
7. ???Antibiotics
8. Initiate CPAP/ventilation if indicated
9. Surfactant therapy if indicated
10.Vitamin E
11. ???Post natal steroids Resp
. Dis
. Syn
.

Surfactant• Surfactant reduces surface tension, improves lung compliance, and
stabilizes lung volumes at a lower transpulmonary pressure
• Surfactant’s secondary function is to enhance macrophage activity and mucociliary clearance, and to reduce inflammation.
• Types of Surfactant– Natural or Synthetic
• Indications– Prophylactic
• Premature infants at high risk of developing RDS secondary to surfactant deficiency (eg 32 weeks or low birth weight 1, 300 g)
• Infants in whom there is laboratory evidence of surfactant deficiency such as lecithin/sphingomyelin ratio 2:1 or the absence of phosphatidylglycerol
Resp
. Dis
. Syn
.\su
rf
• Indication– Rescue or therapeutic administration is indicated in
preterm or full-term infants who are suspected of having surfactant deficiency by inactivation and• who require endotracheal intubation and mechanical
ventilation secondary to respiratory failure
OR
• who require an FiO2 ≥ 40% or a PEEP of ≥7 to maintain adequate PaO2 and SpO2 and have Clinical and radiographic evidence of neonatal RDS or MAS.
– Surfactants may be used as a vehicle to deliver other drugs such as antibiotics, anti-inflammatory agents, and bronchodilators.
Resp
. Dis
. Syn
.\su
rf
• Indication– Postoperative development of ARDS following cardiac
surgery. Reduces time on ventilation and ICU and hospital stay.
– Porcine surfactant in RSV induced respiratory failure may improve gas exchange and respiratory mechanics and shorten the duration of ventilation and hospital stay.
• Contraindication– Presence of congenital anomalies incompatible with life
beyond the neonatal period– Respiratory distress in infants with laboratory evidence of
lung maturity– Diagnosis of congenital diaphragmatic hernia. Studies have
shown that early use of surfactant increases mortality.– Patient hemodynamically unstable– Active pulmonary hemorrhage Re
sp. D
is. S
yn.\
surf
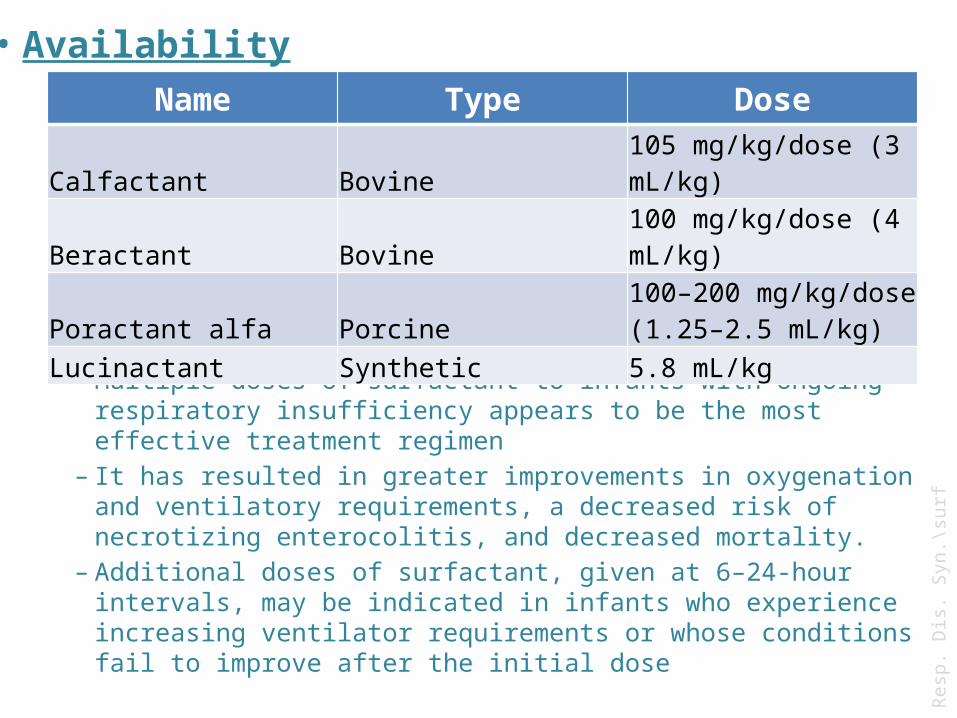
• Frequency– Multiple doses of surfactant to infants with ongoing respiratory
insufficiency appears to be the most effective treatment regimen– It has resulted in greater improvements in oxygenation and
ventilatory requirements, a decreased risk of necrotizing enterocolitis, and decreased mortality.
– Additional doses of surfactant, given at 6–24-hour intervals, may be indicated in infants who experience increasing ventilator requirements or whose conditions fail to improve after the initial dose
Name Type Dose
Calfactant Bovine 105 mg/kg/dose (3 mL/kg)
Beractant Bovine 100 mg/kg/dose (4 mL/kg)
Poractant alfa Porcine 100–200 mg/kg/dose (1.25–2.5 mL/kg)
Lucinactant Synthetic 5.8 mL/kg
• Availability
Resp
. Dis
. Syn
.\su
rf
• DELIVERY TECHNIQUES– INSURE (Intubation, Surfactant, Extubation)• This technique features early surfactant replacement therapy
with prompt extubation to nasal CPAP. The technique is associated with less need for mechanical ventilation, lower incidence of BPD, and fewer air leak syndromes.
– Selective surfactant replacement therapy with mechanical ventilation followed by extubation from lower ventilator settings• This technique is initiated upon clinical evidence of RDS,
such as radiological findings, increased FIO2 requirement, and/or increased work of breathing.
– Pharyngeal instillation before first breath• There have been no randomized controlled trials in humans
to validate this technique. Animal studies have confirmed improvement of lung expansion and better survival rates.
Resp
. Dis
. Syn
.\su
rf

– Laryngeal mask airway (LMA) administration• In an animal studies on surfactant delivery, it was reported
that surfactant delivery could be accomplished sooner in the LMA group than ETT with equivalent efficacy. While far from conclusive, this method holds hope for areas in which ETT intubation skills are lacking.
– Bronchoalveolar lavage• Bronchoalveolar lavage has shown promise in the treatment of
MAS. Studies have demonstrated that surfactant lavage is a safe and effective alternative treatment for MAS.
• In animal studies, it is shown that distribution of intratracheally instilled surfactant has been largely determined by gravity, and unaffected by the position of the chest. Therefore, leaving the chest in a horizontal position may result in the most even distribution of surfactant to the lungs.
Resp
. Dis
. Syn
.\su
rf
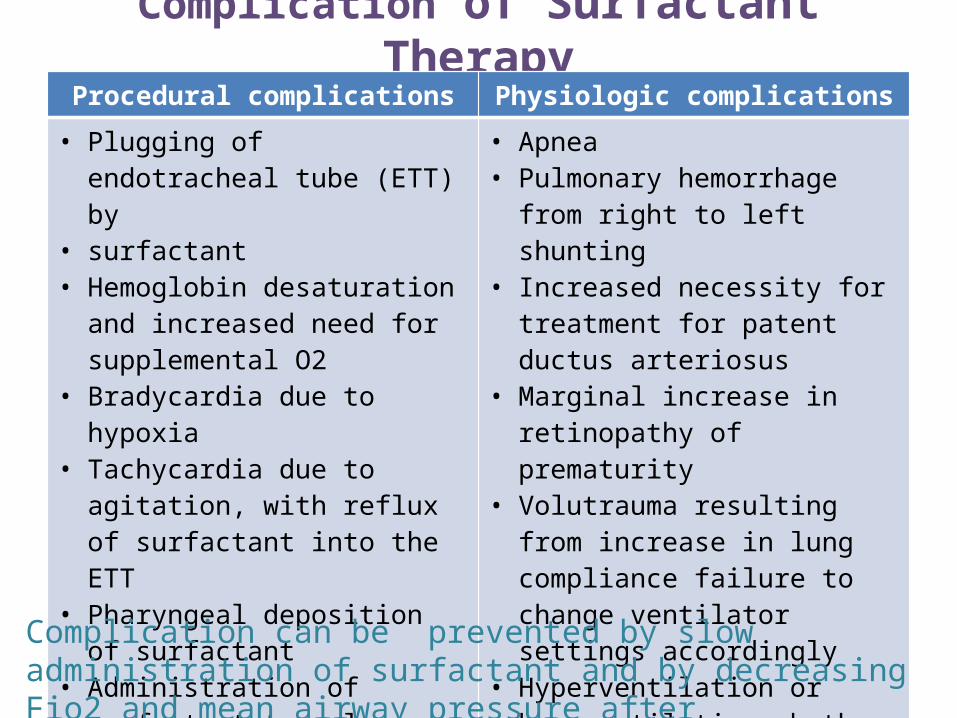
Complication of Surfactant TherapyProcedural complications Physiologic complications
• Plugging of endotracheal tube (ETT) by
• surfactant• Hemoglobin desaturation and
increased need for supplemental O2
• Bradycardia due to hypoxia• Tachycardia due to agitation, with
reflux of surfactant into the ETT• Pharyngeal deposition of
surfactant• Administration of surfactant to
only one lung (ie, right mainstem intubation)
• Administration of suboptimal dose
• Apnea• Pulmonary hemorrhage from right
to left shunting• Increased necessity for treatment
for patent ductus arteriosus• Marginal increase in retinopathy of
prematurity• Volutrauma resulting from increase
in lung compliance failure to change ventilator settings accordingly
• Hyperventilation or hypoventilation, both of which can alter blood flow to the brain, leading to further complications
Complication can be prevented by slow administration of surfactant and by decreasing Fio2 and mean airway pressure after administration

Complication of RDS
• Intraventricular Hemorrhage• Air Leaks• Pulmonary Infection• Pulmonary Hemorrage• Hypoglycemia• DIC• Cardiac Failure• Metabolic alterations
Resp
. Dis
. Syn
.
Transient Tachypnea of Newborn
• Also called Wet Lung Syndrome or Type II Respiratory Distress Syndrome
• The most common cause of neonatal respiratory distress constituting more than 40 percent of cases
• 11 per 1,000 live births..
• Represents a milder form of HMD or due to failure of drainage of alveolar fluids resulting in pulmonary edema decreased compliance and increased airway resistance Respiratory Distress
Tran
. Tac
hy. N
ewbo
rn

Risk Factors
• Term or Near Term Babies• Male Child• Cesarean Section• Delayed cord clamping or cord milking• Macrosomia• Maternal Sedation• Large amount of IV Fluids to mother during
labor• Maternal Asthma• Maternal Diabetes Tr
an. T
achy
. New
born
Clinical Features
• Tachypnea immediately after birth or within 6hrs after delivery with mild to moderate respiratory distress.
• These manifestations usually persist for 12-24hrs, but can last up to 72hrs
• Auscultation usually reveals good air entry with or without crackles
• Usually maintain good color and are alert.
Tran
. Tac
hy. N
ewbo
rn

• X-Ray Chest– Hyperinflation of the lungs– Linear streaking at hila due to dilated lymphatics– Interlobar Fluid–Mild Cardiomegaly
• Chest x-ray usually shows evidence of clearing by 12-18 hrs with complete resolution by 48-72 hrs
Tran
. Tac
hy. N
ewbo
rn

Tran
. Tac
hy. N
ewbo
rn

Fluid in the inter lobar fissure
Tran
. Tac
hy. N
ewbo
rn

TTN is a clinical diagnosis of exclusion
Tran
. Tac
hy. N
ewbo
rn
Management
• Continuous Monitoring of distress.• Supportive Management
• O2 by hood if required
• Provide adequate nutrition• ???Furosemide• ???Antibiotics
Usually a self limited condition and no active management is required
Tran
. Tac
hy. N
ewbo
rn

Bibliography1. Alok Kumar, B. Vishnu Bhat Epidemiology of respiratory distress of newborns The
Indian Journal of Pediatrics January–February 1996, Volume 63, Issue 1, pp 93-98
2. Antonowiez I, Schwachman H. Meconium in health and disease. Adv Paediatr 1979; 26:275-92.
3. Basu S, Kumar A, Bhatia BD. Role of antibiotics in meconium aspiration syndrome. Ann Trop Paediatr. 2007 Jun;27(2):107-13.
4. Brian K Walsh, Brandon Daigle, Robert M DiBlasi, and Ruben D Restrepo AARC Clinical Practice Guideline. Surfactant Replacement Therapy: 2013Respir Care, February 2013 58:2 367-375
5. Canadian Pediatric Society, “Recommendation for neonatal surfactant therapy,” Paediatrics and Child Health, vol. 2, no. 10, pp. 109–116, 2004.
6. Carbine DN. Meconium aspiration. Paediatr Rev 2008; 29: 212-3
7. Clark P, Doff P. Inhibition of neutrophil oxidative burst and phagocytosis by meconium.Am J Obstet Gynecol 1995; 173:1301-5.
8. Fanaroff AA. Meconium aspiration syndrome: historical aspects. J Perinatol. 2008 Dec;28 Suppl 3:S3-7
9. I. El Shahed, P. Dargaville, A. Ohlsson, and R. F. Soll, “Surfactant for meconium aspiration syndrome in full term/near term infants,” Cochrane Database of Systematic Reviews, no. 3, Article ID CD002054, 2007.

10. Jones CA. Early production of pro inflamatory cytokines in the pathogenesis of neonatal ARDS associated with meconium aspiration.Pediatr Res 1994; 35:339.
11. Kamala Swarnam, Amuchou S. Soraisham, and Sindhu Sivanandan, “Advances in the Management of Meconium Aspiration Syndrome,” International Journal of Pediatrics, vol. 2012, Article ID 359571, 7 pages, 2012. doi:10.1155/2012/359571
12. Mechanical Ventilation in Neonatal Medicine zuhair aldajani
13. National Neonatal-Perinatal Database Report 2002-2003
14. Nelson Textbook of pediatrics 18th edition SAUNDERS
15. Nelson Textbook of pediatrics 19th edition SAUNDERS
16. Neonatal morbidity and mortality. Report of the national neonatal perinatal database. Indian Pediatrics 1997; 34: 1039-42
17. Neonatal resuscitation: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Kattwinkel J, Perlman JM, Aziz K, Colby C, Fairchild K, GallagherJ, Hazinski MF, Halamek LP, Kumar P, Little G, McGowan JE, Nightengale B, Ramirez MM, Ringer S, Simon WM, Weiner GM, Wyckoff M, ZaichkinJ. Circulation. 2010;122:S909 –S919.
18. Sankhyan Naveen, Sharma Vijay Kumar, Sarin Ritu, Pathania Kushla. Predictors of meconium stained amniotic fluid : a possible strategy to reduce neonatal morbidity and mortality J Obstet Gynecol India Vol. 56, No. 6 :November/December 2006

19. Soll RF, Blanco F. Natural surfactant extract versus synthetic surfactant for neonatal respiratory distress syndrome. Cochrane Database Syst Rev 2001(2):CD000144.
20. Surg Cdr SS Mathai , Col U Raju , Col M Kanitkar. Management of Respiratory Distress in the Newborn Medical Journal Armed Forces India 2007; 63 : 269-272
21. Text book on Care of Newborn 8th edition,Meharban Singh, CPS publication
22. U Raju, Maj V Sondhi, Maj SK Patnaik. Meconium Aspiration Syndrome : An Insight Medical Journal Armed Forces India, Vol. 66, No. 2, 2010
23. Vain NE, Szyld EG, Prudent LM, Wiswell TE, Aguilar AM, Vivas NI. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomised controlled trial. Lancet. 2004;364:597– 602.
24. W. P. Kanto Jr.v, “A decade of experience with neonatal extracorporeal membrane oxygenation,”Journal of Pediatrics, vol. 124, no. 3, pp. 335–347, 1994
25. Wiswell TE, Gannon CM, Jacob J, Goldsmith L, Szyld E, Weiss K, Schutzman D, Cleary GM, Filipov P, Kurlat I, Caballero CL, Abassi S, Sprague D, Oltorf C, Padula M. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 Pt 1)

THANK YOU







