
RHEUMATIC
VALVULAR HEART
DISEASE

LEARNING OBJECTIVES :-
I. To know the incidence of RVHD.
II. The pathophysiology, clinical features, diagnostic
modalities & treatment options of commonly
occurring valvular lesions.
III. Why to Emphasis prevention.
INTRODUCTION
Rheumatic Heart Disease causes the permanent
heart valve damage resulting from one or more
attacks of Acute Rheumatic Fever.
It is thought that 40-60% of patients with ARF will
go on to developing RHD without proper secondary
prophylaxis*.
The commonest valves affecting are the mitral and
aortic, in that order. However all four valves can be
affected*.
*AHA guidelines 2006


-: MITRAL REGURGITATION :-

MITRAL REGURGITATION :-
Pathophysiology :-
Structural changes include loss
of valvular substance with
shortening & thickening of
cordae tendineae.
With increasing severity of MR,
dilation of Left atrium &
ventricle result in dilation of
mitral valve ring.
Pulmonary hypertension may
eventually develops.
Small
vegetations
are
formed at
injured parts

MITRAL REGURGITATION
Clinical Manifestations :-
History –
i. Usually asymptomatic with mild MR
ii. Rarely, fatigue & palpitations
Physical Examination –
i. JVP normal.
ii. Heaving, hyperdynamic apex beat in severe MR

MITRAL
REGURGITATION
Clinical Manifestations :-
S1 normal or diminished.
S2 widely split.
S3 commonly present.
Regurgitant systolic murmur
starting with s1, Grade 2 to
4/6 at apex with good
transmission to left axilla.
MITRAL REGURGITATION
Electrocardiography :-
Normal in mild cases.
Left ventricular hypertrophy Or LV dominance with or
without Left atrial hypertrophy is usually present.
Atrial fibrillation is rare in pediatric age.
X ray studies :-
LA & LV enlarged.
Pulmonary venous congestion if CHF.
Echocardiography :-
2D echo shows dilated LA & LV.
Color flow mapping & Doppler studies

MITRAL REGURGITATION
Management :-
Medical-
i. Preventive measures against SBE & prophylaxis
against recurrence of rheumatic fever.
ii. No activity restriction for mild cases.
iii. Afterload-reducing agents
iv. Anticongestive therapy if CHF.
v. For atrial fibrillation digoxin indicated.

MITRAL REGURGITATION
Management :-
Surgical* –
i. Severe MR
ii. Progressive cardiomegaly with symptoms.
iii. Pulmonary hypertension.
iv. Valve repair preferred over valve replacement.
v. Valve function checked by 2D echo every 6 to 12
months.
vi. Valve replacement warrants anticoagulation for
life time.
*AHA guidelines 2006

-: MITRAL STENOSIS :-

MITRAL STENOSIS :-
Pathophysiology :-
Fibrosis of mitral ring, commissural adhesions,
contractures of valve leaflets, cordae & papillary
muscles
Takes 10 years or more to fully established lesion.
Usually recognized in adult life.
Significant MS causes left atrial enlargement,
pulmonary venous hypertension, leading to right
ventricular & atrial dilatation.

MITRAL STENOSIS
Clinical Manifestations :-
History –
i. Usually asymptomatic with mild MS.
ii. Breathlessness with or without exertion is commonest
symptom, orthopnea, nocturnal dyspnea, palpitations
in more severe cases.
Physical Examination –
i. Increased right ventricular impulse.
ii. Distended Neck veins.
MITRAL STENOSIS
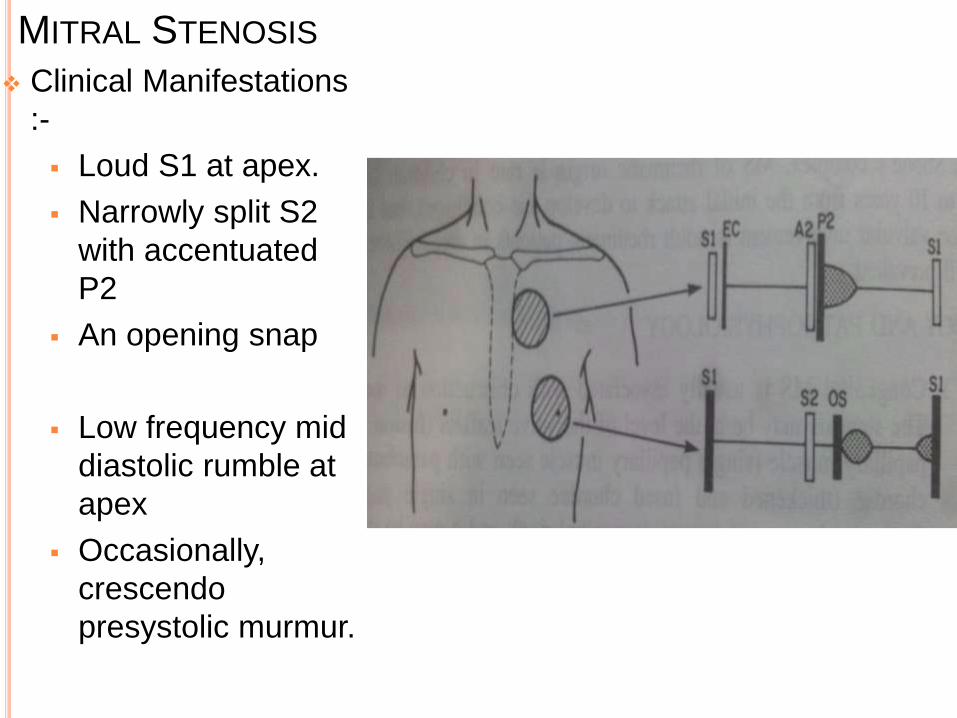
Clinical Manifestations
:-
Loud S1 at apex.
Narrowly split S2
with accentuated
P2
An opening snap
Low frequency mid
diastolic rumble at
apex
Occasionally,
crescendo
presystolic murmur.

MITRAL STENOSIS
Electrocardiography :-
Right axis deviation, Left atrial hypertrophy & Right
ventricular hypertrophy
Atrial fibrillation is rare.
X ray studies :-
LA & RV enlarged & main PA segment prominent.
Pulmonary venous congestion, interstitial edema
shown as Kerley’s B lines
Redistribution of pulmonary blood flow with increased
pulmonary vascularity to upper lobes.
Echocardiography :-
2D echo shows dilated LA & LV.
Color flow mapping & Doppler studies

MITRAL STENOSIS
Echocardiography :-
Most accurate noninvasive tool.
2D echo defines structural abnormality.
Doppler estimates pressure gradient.
o Less than 5 mmHg mild
o 6 to 12 mm Hg moderate
o More than 12 severe
Natural History :-
Asymptomatic mild MS become symptomatic with
exertion.
Recurrence of rheumatic fever worsens the stenosis.
SABE is rare.
Hemoptysis common.

MITRAL STENOSIS
Management :-
Medical-
i. Mild to moderate MS managed with
anticongestive measures.
ii. Good dental hygiene & antibiotics prophylaxis
against SBE
iii. Varying degrees of restriction of activity.
iv. Recurrence of rheumatic fever should be
prevented

MITRAL STENOSIS
Management :-
Surgical* –
i. MS with symptoms
ii. Significant MS with failure to thrive warrants
balloon or surgical intervention.
iii. Failed balloon dilatation.
iv. Mitral commissurotomy for pliable valve without
calcification.
*AHA guidelines 2006
-: AORTIC REGURGITATION :-

AORTIC REGURGITATION
Pathophysiology :-
Almost always associated with mitral valve disease.*
In chronic aortic rheumatic aortic regurgitation,
sclerosis of aortic valves results in distortion &
retraction of the cups.
Regurgitation of blood leads to volume overload with
dilatation & hypertrophy of left ventricle.
*M.Park pediatric cardiology 5th edition

AORTIC REGURGITATION
Clinical Manifestations :-
History –
i. Usually asymptomatic with mild AR.
ii. Exercise tolerance is reduced with moderate to
severe AR.
Physical Examination –
i. Hyperdynamic precordium with moderate or severe
AR with laterally displaced apical impulse.
ii. Diastolic thrill at left third intercostals space
iii. Wide pulse pressure with bounding water hammer
pulse with severe AR

AORTIC REGURGITATION
Clinical Manifestations :-
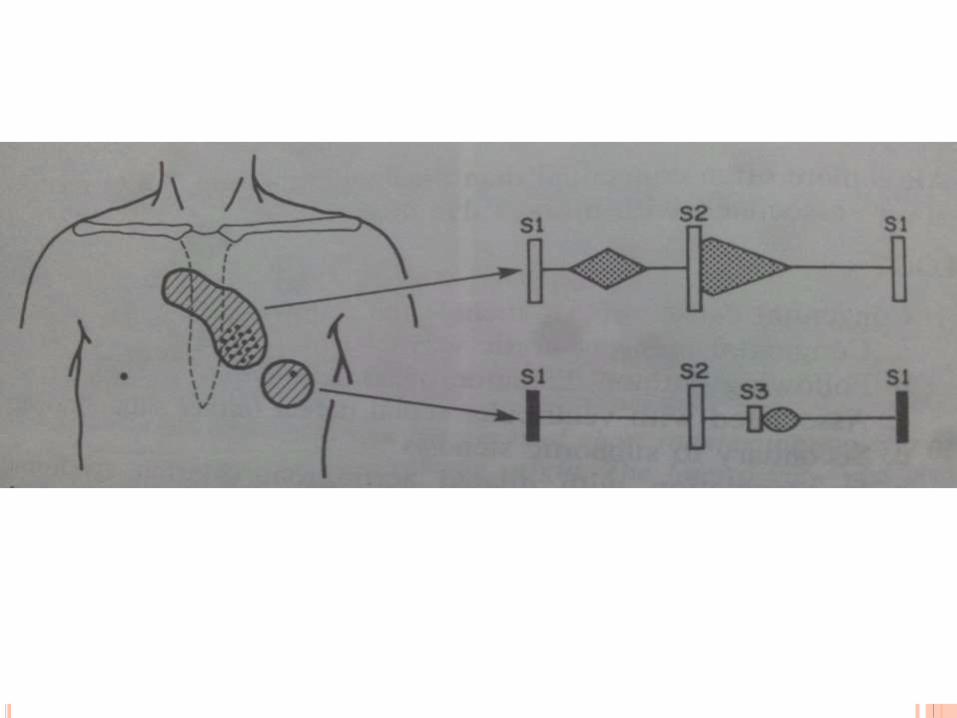
S1 is decreased in intensity.
S2 may be normal or single.
High pitched diastolic decrescendo murmur is the
hallmark of AR.
Longer the murmur more severe the regurgitation.
Systolic murmur at right second intercostal space may
be present.
Severe AR presents with to & fro murmur*
A mid diastolic mitral rumble (Austin flint murmur) at
apex. *M.Park pediatric cardiology 5th edition

AORTIC REGURGITATION
Electrocardiography :-
Left ventricular hypertrophy in severe AR.
X ray studies :-
Cardiomegaly involving Left ventricle.
Dilated ascending aorta & prominent aortic knob.
Echocardiography :-
Left ventricular dimensions are increased.
Left ventricular dimensions are proportional to severity
of AR.

AORTIC REGURGITATION
Natural History :-
Mild to moderate AR remains Asymptomatic for long
time but when symptoms begin to appear patient
deteriorate rapidly.
Anginal pain, CHF, Multiple premature ventricular
contractions are unfourable signs occurring with severe
AR.
Infective endocarditis is rare

AORTIC REGURGITATION
Management :-
Medical-
i. If CHF develop digoxin, diuretics may be
beneficial but the benefits are rarely maintained.
ii. When used on long term basis ACE inhibitors
reduce the dilatation & hypertrophy of LV
iii. Activity restriction not needed in mild AR.

AORTIC REGURGITATION
Management :-
Surgical* –
i. AR with symptoms
ii. Asymptomatic AR with Left ventricular systolic
dysfunction
iii. Asymptomatic AR with progressive Left
ventricular enlargement
iv. Repair is favored over replacement.
*AHA guidelines 2006

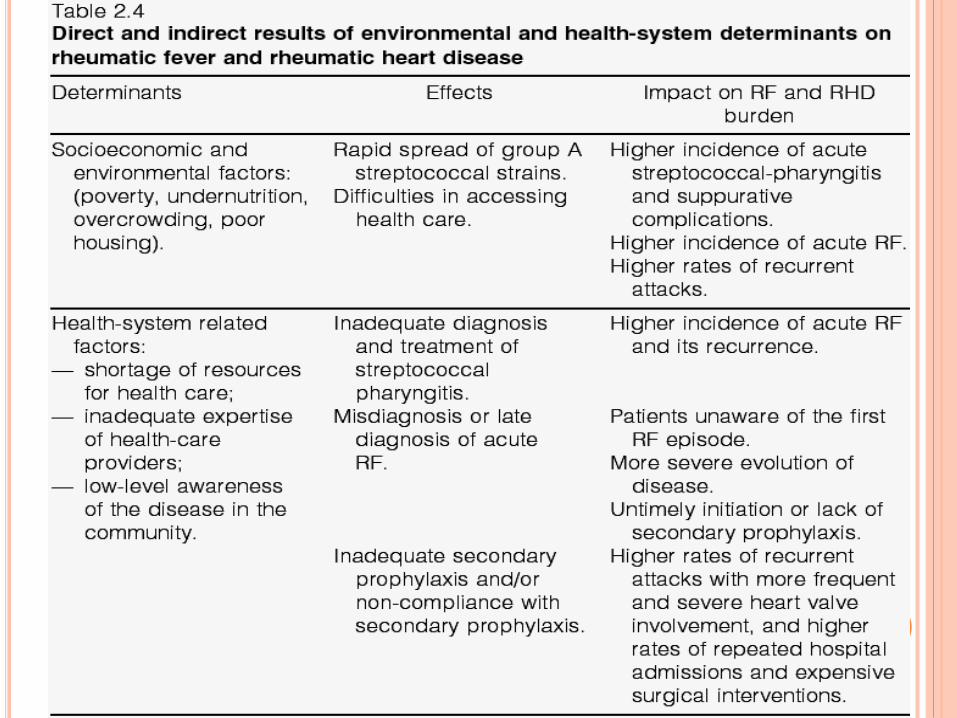
EFFECT OF ENVIRONMENTAL
FACTORS ON RHEUMATIC HEART
DISEASE

WHY SECONDARY PREVENTION ?
Sadly, RHD can go undetected with the result
that patients present with debilitating heart
failure.
At this stage surgery is the only possible
treatment option.
Patients living in poor countries have limited or
no access to expensive heart surgery.

THIS IS TOO
LATE
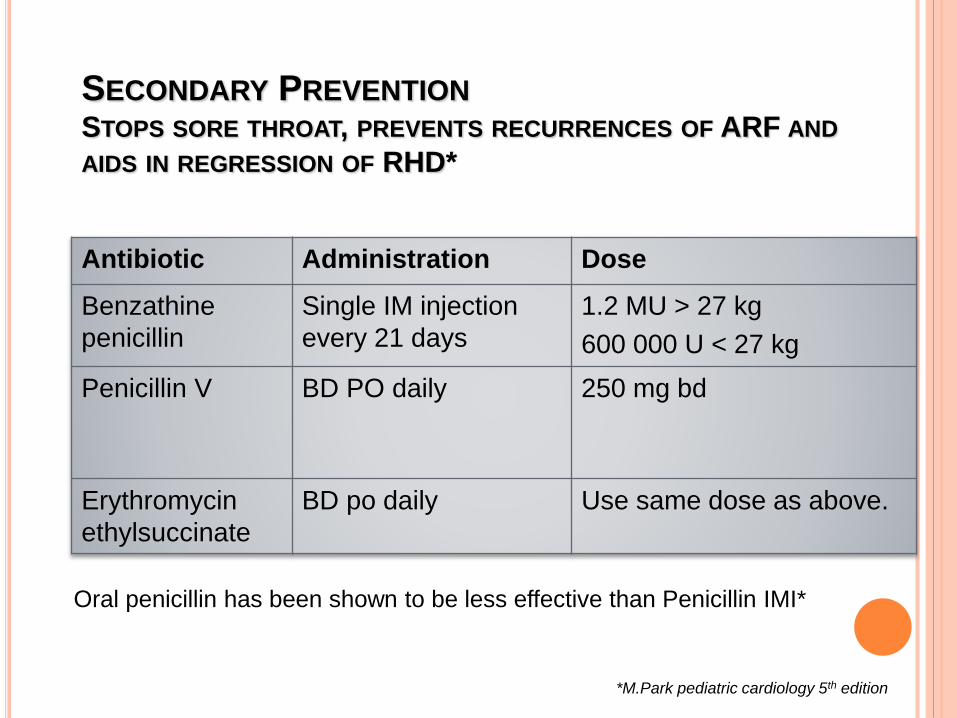
Antibiotic Administration Dose
Benzathine
penicillin
Single IM injection
every 21 days
1.2 MU > 27 kg
600 000 U < 27 kg
Penicillin V BD PO daily 250 mg bd
Erythromycin
ethylsuccinate
BD po daily Use same dose as above.
SECONDARY PREVENTION
STOPS SORE THROAT, PREVENTS RECURRENCES OF ARF AND
AIDS IN REGRESSION OF RHD*
Oral penicillin has been shown to be less effective than Penicillin IMI*
*M.Park pediatric cardiology 5th edition

WHO SHOULD RECEIVE* ?
Patients with documented history of rheumatic fever.
Isolated rheumatic chorea
*M.Park pediatric cardiology 5th edition
Awareness ♦ Surveillance ♦ Advocacy ♦ Prevention
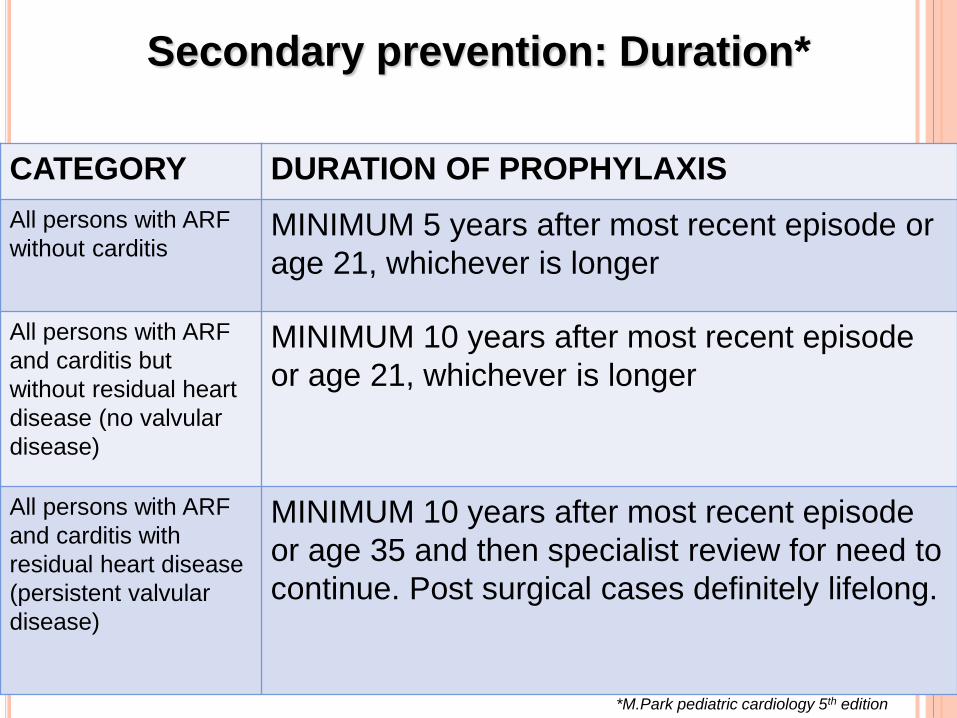
Secondary prevention: Duration*
CATEGORY DURATION OF PROPHYLAXIS
All persons with ARF
without carditisMINIMUM 5 years after most recent episode or
age 21, whichever is longer
All persons with ARF
and carditis but
without residual heart
disease (no valvular
disease)
MINIMUM 10 years after most recent episode
or age 21, whichever is longer
All persons with ARF
and carditis with
residual heart disease
(persistent valvular
disease)
MINIMUM 10 years after most recent episode
or age 35 and then specialist review for need to
continue. Post surgical cases definitely lifelong.
*M.Park pediatric cardiology 5th edition
Secondary prevention: specifics
PENCILLIN
Secondary prophylaxis also reduces the severity of
RHD.
It is associated with regression of heart disease in
approximately 50-70% of those with good
adherence over a decade and reduces mortality.
Route:
BPG is most effective when given as a deep
intramuscular injection.

Secondary prevention: Adherence
• Use a 23-gauge needle- deeper is better
• Local pressure to area for 10 seconds
• Warm syringe to room temperature
• First allow alcohol to dry.
How can we reduce the pain associated with
IM Penicillin?
• Deliver injection very slowly(over 2-3mins)
• Distraction techniques
• Good rapport with the case, is a significant aid to
injection comfort, compliance and understanding.
• Can Use 0.5-1ml of 1% lignocaine. Reduces
pain significantly and excellent for younger
patients.
Secondary prevention: Adherence

Ensuring that patients understand their disease, are informed regarding their future and receive secondary prophylaxis
EDUCATIONHealth education is critical at all levels
Lack of parental awareness of the causes and consequences of
ARF/RHD is a key contributor to poor adherence amongst children on
long-term prophylaxis.

!!! THANK YOU !!!







