

TUBO TUBAL ANASTOMOSIS VS IVF IN THIS ERA
DR SANJAY MAKWANA
MSFICOGFIAGES
Vasundhara Hospital Ltd Jodhpur
wwwvasundharafertilitycom
bull Tubal damage ndash 25-35 cases of infertility
bull Fallopian tube interruption is a common form
of contraception worldwide For a variety of
reasons (eg change in marital status wish
for additional children psychological factors)
many of these women seek restoration of
fertility
bull (Fertil-steril 20002008 Obst Gynecol survey 94)
Point to checkhellip
bull Age ovarian reserve prior fertility no of
children desired site amp extent of tubal damage
presence of other infertility factors
bull Experience of the surgeon
bull Success rates of the IVF program
bull Patient preference religious beliefs cost and
insurance reimbursement
PATIENT SCREENING AND SELECTION
Basic infetility work up
Exclude other factors
Semen analysis
IVF better choice with other co- existing factors
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
bull Tubal damage ndash 25-35 cases of infertility
bull Fallopian tube interruption is a common form
of contraception worldwide For a variety of
reasons (eg change in marital status wish
for additional children psychological factors)
many of these women seek restoration of
fertility
bull (Fertil-steril 20002008 Obst Gynecol survey 94)
Point to checkhellip
bull Age ovarian reserve prior fertility no of
children desired site amp extent of tubal damage
presence of other infertility factors
bull Experience of the surgeon
bull Success rates of the IVF program
bull Patient preference religious beliefs cost and
insurance reimbursement
PATIENT SCREENING AND SELECTION
Basic infetility work up
Exclude other factors
Semen analysis
IVF better choice with other co- existing factors
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

bull Fallopian tube interruption is a common form
of contraception worldwide For a variety of
reasons (eg change in marital status wish
for additional children psychological factors)
many of these women seek restoration of
fertility
bull (Fertil-steril 20002008 Obst Gynecol survey 94)
Point to checkhellip
bull Age ovarian reserve prior fertility no of
children desired site amp extent of tubal damage
presence of other infertility factors
bull Experience of the surgeon
bull Success rates of the IVF program
bull Patient preference religious beliefs cost and
insurance reimbursement
PATIENT SCREENING AND SELECTION
Basic infetility work up
Exclude other factors
Semen analysis
IVF better choice with other co- existing factors
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Point to checkhellip
bull Age ovarian reserve prior fertility no of
children desired site amp extent of tubal damage
presence of other infertility factors
bull Experience of the surgeon
bull Success rates of the IVF program
bull Patient preference religious beliefs cost and
insurance reimbursement
PATIENT SCREENING AND SELECTION
Basic infetility work up
Exclude other factors
Semen analysis
IVF better choice with other co- existing factors
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

PATIENT SCREENING AND SELECTION
Basic infetility work up
Exclude other factors
Semen analysis
IVF better choice with other co- existing factors
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Treatment of Tubal Factor Infertility
1 Surgical Approach
Laparotomy Microsurgical technique
Laparoscopy Pelviscopy
Transcervical Tubal recanalization
2 Assisted Reproductive Technology (ART)
IVF - ET
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Tubal Surgery Tuboplasty
1 Adhesiolysis
Salpingoovariolysis2 Proximal Tubal Occlusion
Tubocornual reanastomosisFluoroscopic recanalizationTranscervical balloon tuboplasty
3 Distal Tubal OcclusionFimbrioplastyNeosalpingostomy
4 Tubal sterilization (TL)Tubal reanastomosis (TR)
Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Tubal Reanastomosis
Prognosis of TR depends on
Method of ligation
Repair site of tube
Residual tubal length
Other causes of infertility
Bipolar coagulation PR 49
Ring clip PR 67
Pomeroy TL PR 75
(S Gordts Fertil steril 2009 Kim jd 1997)
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Tubal Reanastomosis
bull Better prognosis with small difference in diameter
of reconstructed tubal locations
Isthmus ndash isthmus
Ampulla ndash isthmus
Ampulla - Ampulla
( Laparoscopic micro surgery - Koh and Janik 1996)
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Tubal ReanastomosisMethod and location of ligation
The time interval between tubal ligation and its reversalPotential postop tubal lengthCoexistent pelvic disease
bull Gomel amp Swolin 1980
Low PR lt 4 cm of postop tubal length Inverse correlation between postop tubal lengthand interval to pregnancy
bull In older women gt 40 yrs
TR (Trimpos amp Kemper 1980)PR 45 Interval to pregnancy 55 months
IVF-ET (Tan 1992)CPR 10 TR indicated after 3 cycles of IVF-ET
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
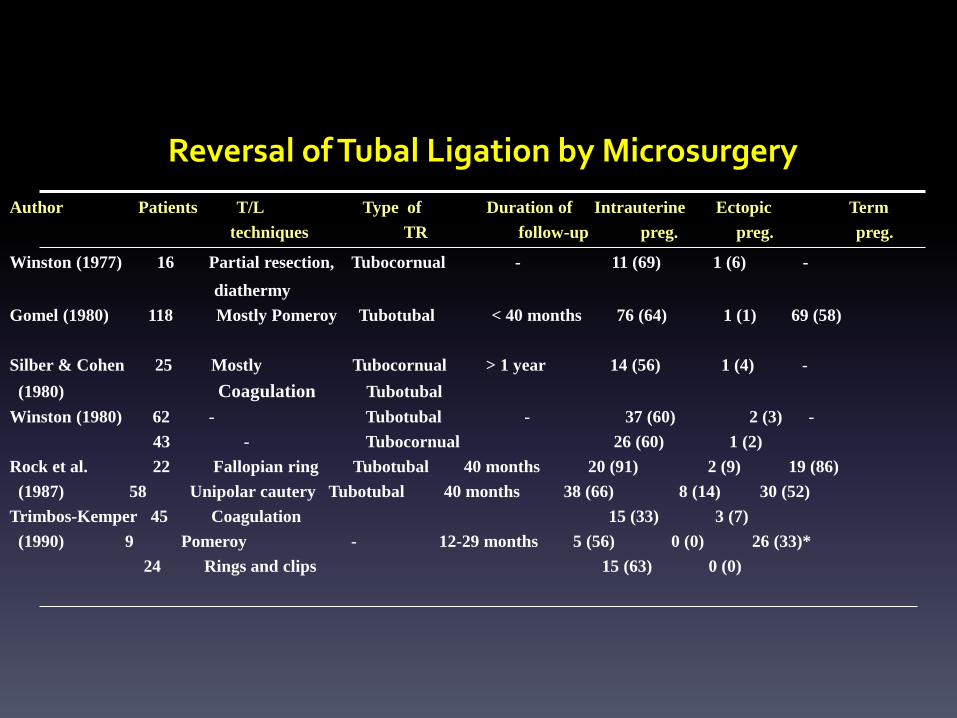
Reversal of Tubal Ligation by Microsurgery
Author Patients TL Type of Duration of Intrauterine Ectopic Term
techniques TR follow-up preg preg preg
Winston (1977) 16 Partial resection Tubocornual - 11 (69) 1 (6) -
diathermy
Gomel (1980) 118 Mostly Pomeroy Tubotubal lt 40 months 76 (64) 1 (1) 69 (58)
Silber amp Cohen 25 Mostly Tubocornual gt 1 year 14 (56) 1 (4) -
(1980) Coagulation Tubotubal
Winston (1980) 62 - Tubotubal - 37 (60) 2 (3) -
43 - Tubocornual 26 (60) 1 (2)
Rock et al 22 Fallopian ring Tubotubal 40 months 20 (91) 2 (9) 19 (86)
(1987) 58 Unipolar cautery Tubotubal 40 months 38 (66) 8 (14) 30 (52)
Trimbos-Kemper 45 Coagulation 15 (33) 3 (7)
(1990) 9 Pomeroy - 12-29 months 5 (56) 0 (0) 26 (33)
24 Rings and clips 15 (63) 0 (0)
Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Tubal Reanastomosis
bull Gomel 1980
PR 64 Ectopic PR 1 Interval to pregnancy 102 months
bull Kim et al 1997 (n=1118)
Anatomic patency rate 882PR 548 DR 725
bull Kjayakrishnan 2011 journal of HuReprod sc The pregnancy rate was better for laparoscopic sterilization by Falope ring (857) as compared with those with Pomeroys procedure (40)
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
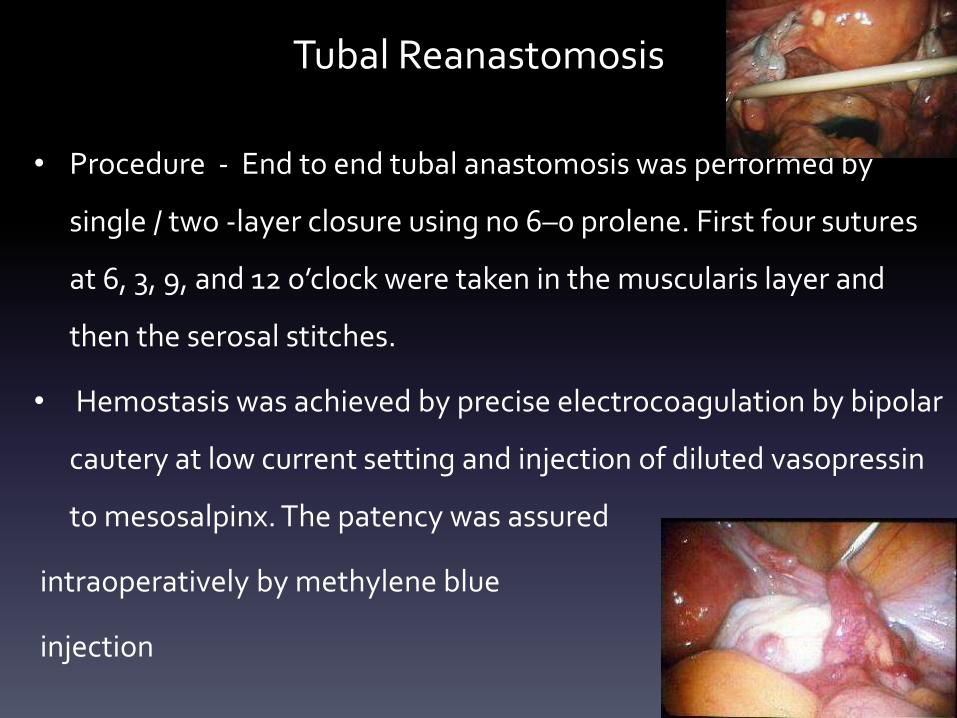
Tubal Reanastomosis
bull Procedure - End to end tubal anastomosis was performed by
single two -layer closure using no 6ndash0 prolene First four sutures
at 6 3 9 and 12 orsquoclock were taken in the muscularis layer and
then the serosal stitches
bull Hemostasis was achieved by precise electrocoagulation by bipolar
cautery at low current setting and injection of diluted vasopressin
to mesosalpinx The patency was assured
intraoperatively by methylene blue
injection
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
IVF - ET
Alternative of choice to surgical approach
Dominant role in treatment of tubal factor infertility
Growing number of qualified IVF centers
Nearly equal to availability of tubal surgery
Requirement of expertise and credentialing
Tubal surgery can be performed although perhaps less
successfully by those without speciality training
Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Benadiva 1995
Is pelvic reconstructive surgery obsolete
Penzias 1996
Is there ever a role for tubal surgery
Dubuisson 1998
Are there still indications for tubal surgery in infertility
Status of ART
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
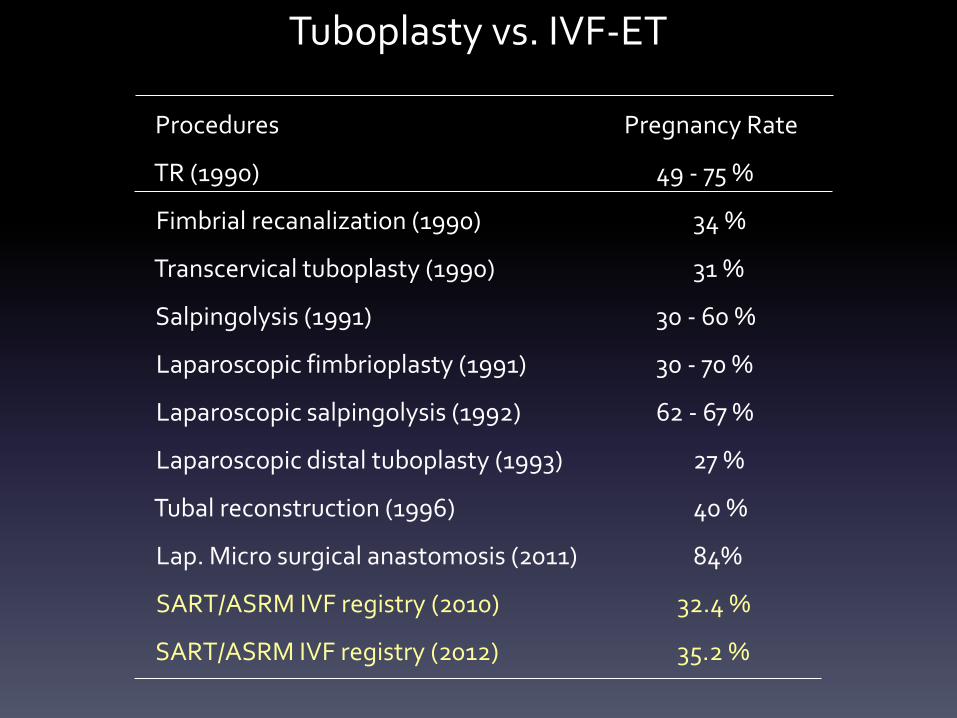
Tuboplasty vs IVF-ET
Procedures
TR (1990)
Fimbrial recanalization (1990)
Transcervical tuboplasty (1990)
Salpingolysis (1991)
Laparoscopic fimbrioplasty (1991)
Laparoscopic salpingolysis (1992)
Laparoscopic distal tuboplasty (1993)
Tubal reconstruction (1996)
Lap Micro surgical anastomosis (2011)
SARTASRM IVF registry (2010)
SARTASRM IVF registry (2012)
Pregnancy Rate
49 - 75
34
31
30 - 60
30 - 70
62 - 67
27
40
84
324
352
Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Standard IVF-ET by Maternal Age
SART amp ASRM 2010
lt 35 yrs male factor (-)
35 - 37 yrs male factor (-)
38 - 40 yrs male factor (-)
gt 40 yrs male factor (-)
Cancellation
rate ()
102
148
193
244
Delivery
retrieval ()
339
294
212
94
Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Tuboplasty or IVF
bull TuboplastyMild or moderate tubal diseaseYoung female
bull IVF-ETExtensive pelvic adhesionOld age Impossible tubal reconstruction due to absenceof tubes or history of tuberculous salpingitis
Failed tubal surgeryExistence of other infertility factors
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Considerations for Tuboplasty or IVF
bull Technical view Invasiveness
Infertility factors involved
bull Nontechnical view Cost
Wishes of patients
bull Surgery Specialty training
bull (surgeon considering laparoscopic tubal microsurgery
should be competent with both the traditional techniques
of microsurgery and intra corporeal micro suturing )
bull IVF-ET Expertise and credentialing of the program
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Advantages and Disadvantages IVF bull per-cycle success rates and the fact that it is less surgically invasive
bull Its disadvantages are generalizable to surgeons with less skill and
experience and include cost (especially if more than one cycle is
required)
bull the frequent injections monitoring most significantly risks of
multiple pregnancy and OHSS
bull IVF alone has been associated with a higher incidence of adverse
perinatal outcomes in singleton infants such as perinatal mortality
preterm delivery low and very low birth weights intrauterine
growth retardation and congenital malformations
bull (Human Reproduction 05 Fertil Steril 2009 2010)
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
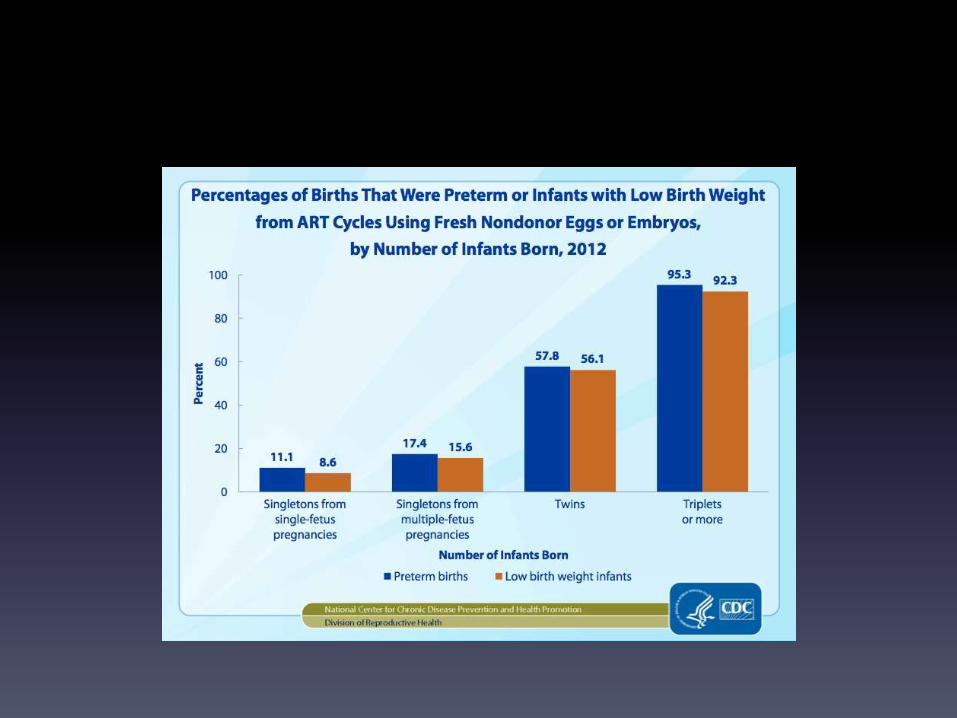
bull The advantages of Lap tubal surgery are that it is a
one-time usually minimally invasive outpatient
procedure and patients may attempt conception
every month without further intervention and may
conceive more than once
bull They also avoid the risks associated with IVF
bull The disadvantages are the risks for surgical
complications While the risk of ectopic pregnancy is
increased in patients having IVF for tubal disease it is
higher after tubal surgery
bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

bull Tubal anastomosis had a higher cumulative
pregnancy rate for women less than 37 years
of age no significant difference above 37
years of age
bull Human reproduction 2007 P Devroey
Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal

Comparison of Cost per Delivery
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Patient Counselling
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
bull The most recent national assisted reproductive
technology (ART) registry data from 2012 noted a
324 live-birth rate per cycle initiated in patients with
tubal infertility similar to the 341 rate overall(SART)
bull Meaningful success rates with the various tubal
surgical procedures are largely lacking Most of the
published literature is from surgeons with the greatest
expertise Their results may not be generalizable to less
skilled or experienced surgeons
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
bull The results of tubal surgery and IVF are not directly
comparable because surgical success is reported as
pregnancy rate per patient whereas IVF success
rates are per cycle As a result there are no
adequate trials comparing pregnancy rates with tubal
surgery versus IVF
bull ( Cochrane Database syst rev 2008 )
However IVF has a higher per cycle pregnancy rate
whereas tubal anastomoses has higher cumulative
pregnancy rate and is more cost effective
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
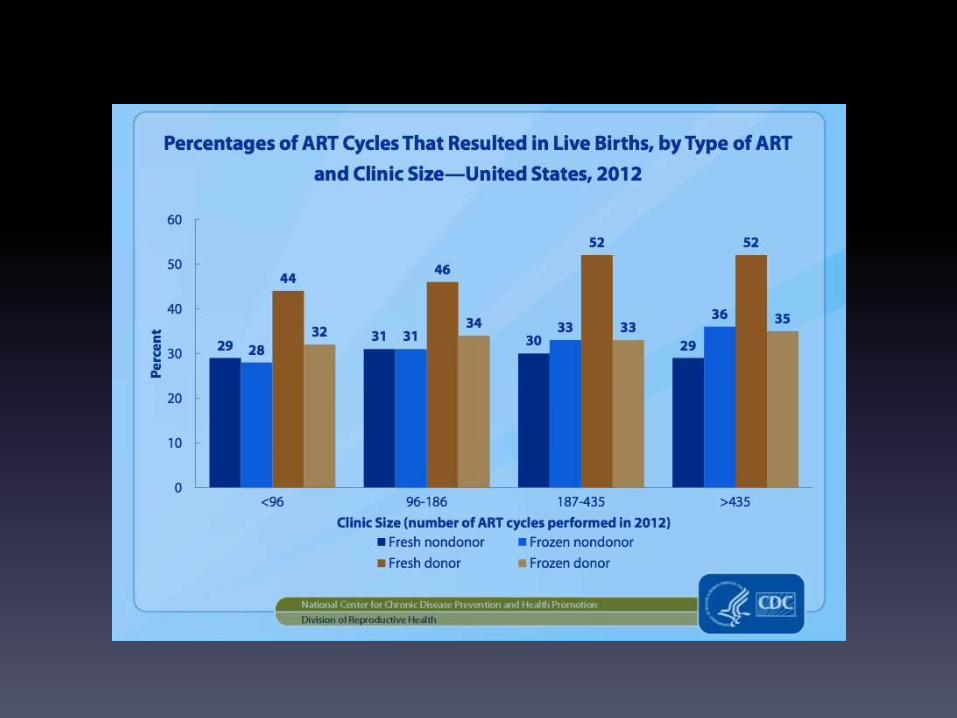
Ann Acad Med Singapore 2010 Jan39(1)22-6Microsurgical reversal of sterilisation - is this still clinically relevant
todayTan HHLoh SF
bull Pregnancy (778 vs 700) and live birth rates (667 vs 600)
were similar between laparoscopy and open surgery The mean
interval to pregnancy was marginally lower via laparoscopy (113 vs
136 months) Hospitalisation stay was significantly halved (143 vs
300 days) but ectopic pregnancies were increased 3-fold (3 vs 1) with
laparoscopy Compared with IVF the estimated average cost per
delivery for laparoscopic reversal was reduced for laparoscopic
reversal with no multiple pregnancies
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Hum Reprod 2012 Jun27(6)1657-62 doi 101093humrepdes078 Epub 2012 Mar 27
High pregnancy rate after microsurgical tubal reanastomosis bytemporary loose parallel 4-quadrant sutures technique a long
long-term follow-up report on 961 casesMoon HS1 Joo BS Park GS Moon SE Kim SG Koo JS
bull The overall pregnancy rate was 851 826 being
intrauterine and 25 ectopic
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal
Tuboplasty vs IVF-ET
Conclusions
1 The goal for infertile couples should be live birth or
at least the ability to feel that they did their best
2 These options should be carefully considered and
individualized regarded as complementary
not competitive to achieve the desired goal







