
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Arkansas Trauma System Evidence-Based Guidelines for
Abdominal Trauma- Advanced Trauma Techniques-
Upper Abdomen
Section Editor: Charles D. Mabry MD FACS
Introduction-
Trauma to the abdomen remains one of the most common major injuries for humans. The first
evidence-based guideline regarding abdominal trauma covered the pre-hospital and emergency
department evaluation and treatment of abdominal trauma. This second guideline is aimed at the
patient with major injuries to the upper abdominal organs. The remaining two guidelines will cover
trauma to the lower abdominal / pelvic area and damage control / open abdomen surgery.
Upper Abdominal Trauma- Liver, Stomach, Duodenum, Pancreas, and Spleen,
Liver trauma:
Trauma to the liver is one of the more common major category of traumas of the abdomen, due in
part to the size of the liver, and to the ease that blunt trauma to the upper abdomen and lower
chest can injure the liver. Despite its size and frequency of injury, non-operative management of the
liver has become much more common and accepted, than operative repair of the liver. Even
isolated penetrating injuries to the dome of the liver can be managed without open exploration in
some instances. 1 Non-operative management does include the use of interventional radiology as a
method to control bleeding. 2,3
Diagnosis of liver trauma can be made with a FAST ultrasound exam, but abdominal CT scan with IV
contrast remains the primary method to gage the extent of overall liver injury as well as to detect
significant bleeding via a “blush” seen on the CT scan. Thus, it is important to promptly evaluate the
patient with abdominal injury with the proper CT scan in order to determine prognosis as well as
anticipated treatment. 4 If your trauma center doesn’t have interventional radiology capability and
the patient has a suspected major liver injury, then consideration of transferring the patient to a

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
center that does have this capability should be entertained. Liver injury can be graded, and
although the grade of liver injury may not always determine the need for open surgery, a grading
scale is useful for communication to other providers about the extent of injury and for a prognostic
indicator of likely later bleeding and mortality. Most surgeons use the AAST grading scale for liver
injury, which was updated in 1994 to include CT scan findings. 5 [Figure A] It is important to
consider including delayed phase imaging of the liver for the trauma CT scan protocol to visualize
the portal and hepatic veins to detect any major vascular injury.
Predictors of need for open surgery for the liver injury patient revolve around the key factors of: 1)
ongoing hemodynamic instability, including a shock index > 1, 2) ongoing hemorrhage, other
abdominal injury requiring surgery, presence of a blush on angiography, and 3) a low GCS. 6 , 7
Operative management involves several techniques including four quadrant packing to control
hemorrhage and compress the liver as a first step, portal clamping (the Pringle maneuver), and
balloon tamponade (Foley catheter or Fogarty balloon) and direct ligation of arterial bleeding. See
[Figure B] for a good algorithm for operative management of liver injury. 8 [Figure C] shows the
standard liver segments that are typically numbered. 9 As with all traumas, avoidance of
hypothermia, coagulopathy, and acidosis is critical, along with the use of component blood therapy
all-the-while avoiding excessive IV fluids.

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure A- AAST Liver Injury Grading Scale

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure B- Operative Management of Hepatic Injury

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure C- Hepatic Segment Anatomy

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Pancreatic and Duodenal Trauma:
While infrequent, injuries to the pancreas and duodenum are well known and respected for their
associated major complications. Detection of injury to the duodenum and pancreas remain difficult
in many cases, and delayed presentation of injury is not uncommon, despite good front-end
evaluation. Thus, a high index of suspicion is necessary to avoid a delay in diagnosis which almost
always increases morbidity and mortality.
MVA (steering wheel) injury is perhaps the most common mechanism for injury to this area, where
these organs are crushed against the spine. One marker for potential pancreas and duodenum (and
small bowel) injury is a compression fracture of the lower thoracic and upper lumbar spine (Chance
fracture). 10 Evaluation with CT scans with IV contrast is often necessary to detect bleeding or small
leaks from the pancreas or duodenum. For isolated blunt or penetrating injuries to upper abdominal
area (e.g. knife injury, handle-bar, or bull / horse stomping) oral contrast should also be considered
to rule out occult injuries to the duodenum. 11
The superior mesenteric artery and vein provides an anatomic marker that divides these injures into
two zones: 1) to the patient’s left are pancreatic tail injuries and 2) to the patient’s right are often
combined duodenal, pancreas, and common bile duct catastrophes. After the anatomic zone of
injury is determined, the next major question to answer is whether or not the pancreatic duct is
injured or if the duodenum is leaking. 12, 13
Injuries to the tail of the pancreas are perhaps the most straightforward of all of the possible
combinations of duodenal and pancreatic injuries. These often involve the spleen, but if minor and
there are no other injuries, and the pancreatic duct is intact, these can often be managed non-
operatively. More severe injuries in this area can be managed by a distal pancreatectomy and
splenectomy, with placement of drains. Injures to the patient’s right of the superior mesenteric
vessels are more problematic. If there is minor injury with no leakage, the nasogastric
decompression and total parenteral nutrition often will be all that is needed. More severe injury,
however, requires open surgery, debridement, drainage, and possible diversion. 12, 13 The algorithm
in [Figure D] is from Up to Date, and the reader is urged to read this entire document for
management options and techniques for these types of complex injuries. 10 These injuries are not
only complex but deadly, and early referral to a Level I trauma center is an excellent choice to
consider.
Both the pancreas and duodenum are largely retroperitoneal organs and they lie in Zone I of the
retroperitoneum, along with the aorta and inferior vena cava. [See Figure E]. As such, large
hematomas in Zone I are typically explored to rule out significant sources of hemorrhage from major
vessels.

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure D: Management of Pancreatic Injury

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure E: Zones of the Retroperitoneum in the Abdomen

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Splenic Trauma
Similar to the liver, trauma to the spleen is now being management more frequently non-
operatively, especially if there are no other reasons to explore the abdomen. For the
hemodynamically unstable patient, with a positive FAST scan of the abdomen, prompt transfer to
the operating room should be the first option considered. For trauma centers without general
surgery capability, stabilization and expeditious transfer to an appropriate trauma center should
occur. 14 For the stable patient, evaluation with a CT scan with IV contrast is the best tool to help
understand the extent and prognosis for splenic trauma.
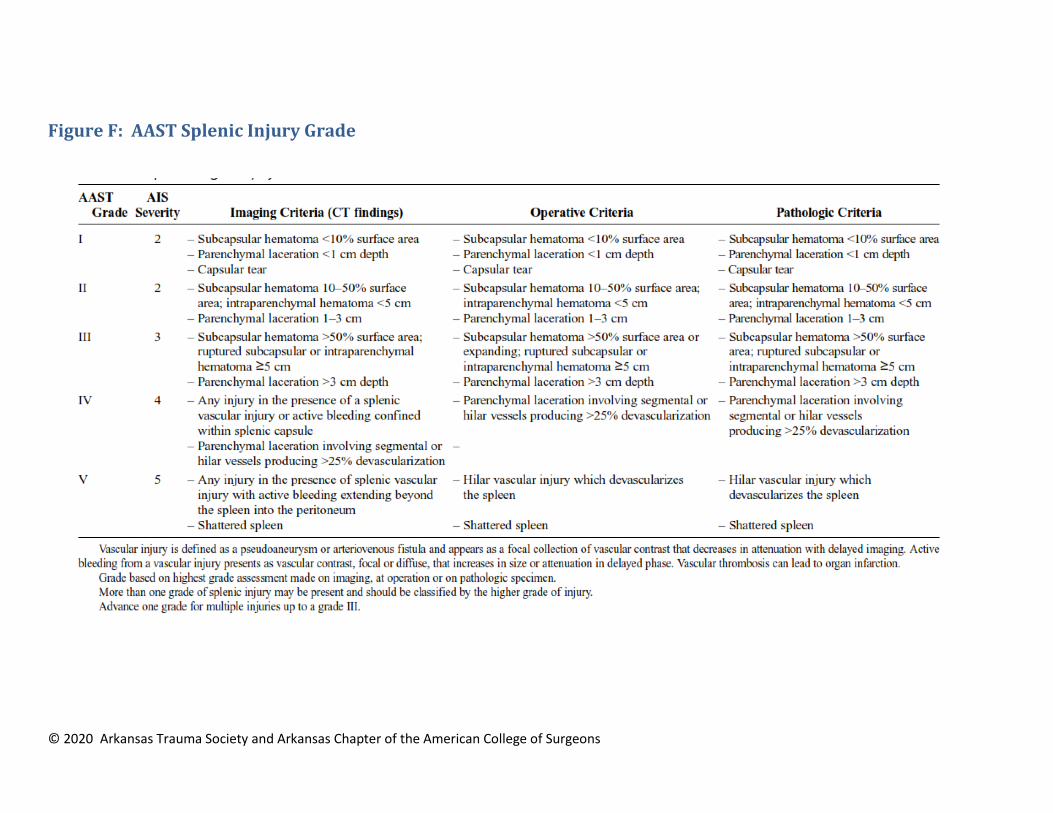
While the grade of splenic injury doesn’t always determine the need for open surgery, as a general
rule, non-operative management fails more frequently as the grade of injury increases, especially
for Grades III to V. The American Association for the Surgery of Trauma (AAST) published the most
widely used splenic injury grading scale in 1989, and this was updated in 2018 to incorporate CT
scan findings [Figure F]. 15 16 17 Active bleeding detected by an arterial blush on CT scan can often be
managed by interventional radiology and embolization of the bleeding artery. 18 Other markers for
failure of non-operative management are increasing age (more fragile splenic capsule and more
atherosclerotic arteries) and significant head injury (inability to tolerate hypotension). 19 Non-
operative management should not be attempted for significant splenic trauma (Grades III and
above) in a center without the capability of immediate open surgery &/or angiography.
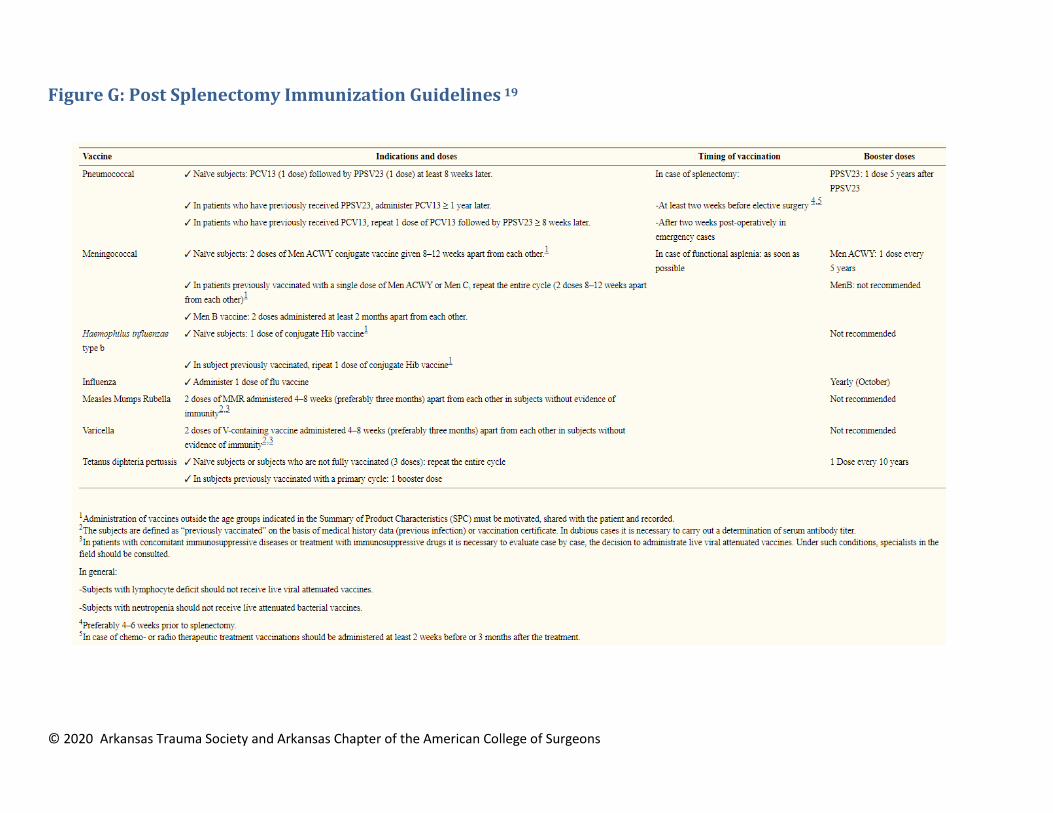
For patients who undergo splenectomy, especially for those younger than 16 years of age, the
standard recommendations are to immunize the patient after 14 days against pneumococcal
pneumonia, meningitis, and influenza, to avoid the 3-5% post-splenectomy sepsis syndrome. 20 21
[See Table G for details] 19
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure F: AAST Splenic Injury Grade
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
Figure G: Post Splenectomy Immunization Guidelines 19

© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
References 1 DuBose J, Inaba K, Teixeira PG, Pepe A, Dunham MB, McKenney M. Selective non-operative management of solid organ injury
following abdominal gunshot wounds. Injury. 2007;38(9):1084–90. 2 Stassen, Nicole A., Indermeet Bhullar, Julius D. Cheng, Marie L. Crandall, Randall S. Friese, Oscar D. Guillamondegui, Randeep S.
Jawa et al. "Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline." Journal of Trauma and Acute Care Surgery 73, no. 5 (2012): S294-S300. 3 Evans, Cory, and Martin A. Croce. "When Should You Operate on Major Hepatic Trauma?." In Difficult Decisions in Hepatobiliary
and Pancreatic Surgery, pp. 63-72. Springer, Cham, 2016. 4 Up to Date: Management of hepatic trauma in adults. https://www-uptodate-com.libproxy.uams.edu/contents/management-of-
hepatic-trauma-in adults?search=hepatic%20trauma&source=search_result&selectedTitle=1~102&usage_type=default&display_rank=1 5 Kozar RA, Crandall M, Shanmuganathan K, et al. Organ injury scaling 2018 update: Spleen, liver, and kidney. J Trauma Acute Care
Surg 2018; 85:1119 6 Tran, Alexandre, Maher Matar, Jacinthe Lampron, Ewout Steyerberg, Monica Taljaard, and Christian Vaillancourt. "Early
identification of patients requiring massive transfusion, embolization or hemostatic surgery for traumatic hemorrhage: A systematic review and meta-analysis." Journal of Trauma and Acute Care Surgery 84, no. 3 (2018): 505-516. 7 Up to Date: Surgical Techniques for Managing Hepatic Injury. https://www-uptodate-com.libproxy.uams.edu/contents/surgical-
techniques-for-managing-hepatic-injury/print?search=damage 8 Kozar RA, Felciano DV, Moore EE, et al. Western Trauma Association/Critical Decisions in Trauma: Operative management of adult
blunt hepatic trauma. J Trauma 2011; 71:1. 9 https://radiologyassistant.nl/abdomen/liver-segmental-anatomy
10 Management of duodenal and pancreatic trauma in adults. https://www-uptodate-
com.libproxy.uams.edu/contents/management-of-duodenal-and-pancreatic-trauma-in-adults?search=Management%20of%20duodenal%20and%20pancreatic%20trauma%20in%20adults&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 11
Up to Date: Traumatic gastrointestinal injury in the adult patient. https://www-uptodate-com.libproxy.uams.edu/contents/traumatic-gastrointestinal-injury-in-the-adult-patient?search=antibiotics%20in%20trauma&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=2 12
Ho, Vanessa Phillis, Nimitt J. Patel, Faran Bokhari, Firas G. Madbak, Jana E. Hambley, James R. Yon, Bryce RH Robinson et al. "Management of adult pancreatic injuries: a practice management guideline from the Eastern Association for the Surgery of Trauma." Journal of Trauma and Acute Care Surgery 82, no. 1 (2017): 185-199. 13
Western Trauma Association Critical Decisions in Trauma: Diagnosis and management of duodenal injuries. Malhotra A, Biffl WL, Moore EE, Schreiber M, Albrecht RA, Cohen M, Croce M, Karmy-Jones R, Namias N, Rowell S, Shatz DV, Brasel KJ J Trauma Acute Care Surg. 2015 Dec;79(6):1096 14
Rowell, Susan E., Walter L. Biffl, Karen Brasel, Ernest E. Moore, Roxie A. Albrecht, Marc DeMoya, Nicholas Namias et al. "Western Trauma Association Critical Decisions in Trauma: Management of adult blunt splenic trauma—2016 updates." Journal of Trauma and Acute Care Surgery 82, no. 4 (2017): 787-793. 15
Tinkoff G, Esposito TJ, Reed J, et al. American Association for the Surgery of Trauma Organ Injury Scale I: spleen, liver, and kidney, validation based on the National Trauma Data Bank. J Am Coll Surg 2008; 207:646. 16
Moore, E. E., S. R. Shackford, H. L. Pachter, J. W. McAninch, B. D. Browner, H. R. Champion, L. M. Flint, T. A. Gennarelli, M. A. Malangoni, and M. L. Ramenofsky. "Organ injury scaling: spleen, liver, and kidney." The Journal of trauma 29, no. 12 (1989): 1664-1666.Moore, E. E., S. R. Shackford, H. L. Pachter, J. W. McAninch, B. D. Browner, H. R. Champion, L. M. Flint, T. A. Gennarelli, M. A. Malangoni, and M. L. Ramenofsky. "Organ injury scaling: spleen, liver, and kidney." The Journal of trauma 29, no. 12 (1989): 1664-1666. 17
Kozar, Rosemary A., Marie Crandall, Kathirkamanthan Shanmuganathan, Ben L. Zarzaur, Mike Coburn, Chris Cribari, Krista Kaup, Kevin Schuster, Gail T. Tominaga, and AAST Patient Assessment Committee. "Organ injury scaling 2018 update: Spleen, liver, and kidney." Journal of Trauma and Acute Care Surgery 85, no. 6 (2018): 1119-1122. 18
Up to Date: Management of splenic injury in the adult trauma patient. https://www-uptodate-com.libproxy.uams.edu/contents/management-of-splenic-injury-in-the-adult-trauma-

Arkansas Trauma System Evidence-Based Guidelines for Upper Abdominal Trauma
© 2020 Arkansas Trauma Society and Arkansas Chapter of the American College of Surgeons
patient?search=Management%20of%20splenic%20trauma%20in%20adults&source=search_result&selectedTitle=1~97&usage_type=default&display_rank=1 19
Stassen, Nicole A., Indermeet Bhullar, Julius D. Cheng, Marie L. Crandall, Randall S. Friese, Oscar D. Guillamondegui, Randeep S. Jawa et al. "Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline." Journal of Trauma and Acute Care Surgery 73, no. 5 (2012): S294-S300. 20 Buzelé, R., L. Barbier, A. Sauvanet, and B. Fantin. "Medical complications following splenectomy." Journal of visceral surgery 153, no. 4 (2016): 277-286. 21 Bonanni P, Grazzini M, Niccolai G, et al. Recommended vaccinations for asplenic and hyposplenic adult patients. Hum Vaccin Immunother. 2017;13(2):359‐368. doi:10.1080/21645515.2017.1264797







