

Selecting sperm for ICSI - IMSI
Allan PaceyUniversity of Sheffield
Sheffield Teaching Hospitals

[email protected]://www.twitter.com/allanpacey
Intra Cytoplasmic Sperm Injection
Palermo et al., (1992) Lancet 340: 17-18

What does ICSI bypass?
Suarez and Pacey (2006) Human Reprod Update 12: 23-37

Sperm Transport
Suarez and Pacey (2006) Human Reprod Update 12: 23-37
Cervix
Utero-tubal junction
Sperm-epithelial interactions
Sperm-oocyte interaction

Summary of sperm functionsin relation to mode of conception
Mode of fertilisation / conception
coitus IC IUI GIFT IVF ICSI
Passage through cervical mucus Y N N N N N
Transport through the uterus Y Y N N N N
Passage through the UTJ Y Y Y N N N
Sperm-epithelial interaction Y Y Y ? N N
Capacitation Y Y Y Y Y N
Sperm Egg Binding Y Y Y Y Y N
Passage through zona pellucida Y Y Y Y Y N
Decondensation of sperm DNA Y Y Y Y Y Y
Pacey (2005) What Makes ‘Good Sperm’? In Implantation and Early Development. RCOG Press. pp. 119 - 128.

Pacey (2005) What Makes ‘Good Sperm’? In Implantation and Early Development. RCOG Press. pp. 119 - 128.
Summary of sperm functionsin relation to mode of conception
Mode of fertilisation / conception
coitus IC IUI GIFT IVF ICSI
Passage through cervical mucus Y N N N N N
Transport through the uterus Y Y N N N N
Passage through the UTJ Y Y Y N N N
Sperm-epithelial interaction Y Y Y ? N N
Capacitation Y Y Y Y Y N
Sperm Egg Binding Y Y Y Y Y N
Passage through zona pellucida Y Y Y Y Y N
Decondensation of sperm DNA Y Y Y Y Y Y

DNA Quality
% FAS positive cells
Lewis & Simon (2010) Human Fertility 13: 201-217

Nagy et al., (1995) Human Reproduction 10: 1123-1129
ICSI and semen parameters

Motile Sperm Organelle Morphology Examination (MSOME)
Bartoov et al., (2002) Journal of Andrology 23: 1-8

Motile Sperm Organelle Morphology Examination (MSOME)
Bartoov et al., (2002) Journal of Andrology 23: 1-8

Motile Sperm Organelle Morphology Examination (MSOME)
Bartoov et al., (2003) Fertility and Sterility 80: 1413-1419

Antinori et al., (2008) RBM Online 16: 835-841
Prospective RCT (IMSI)
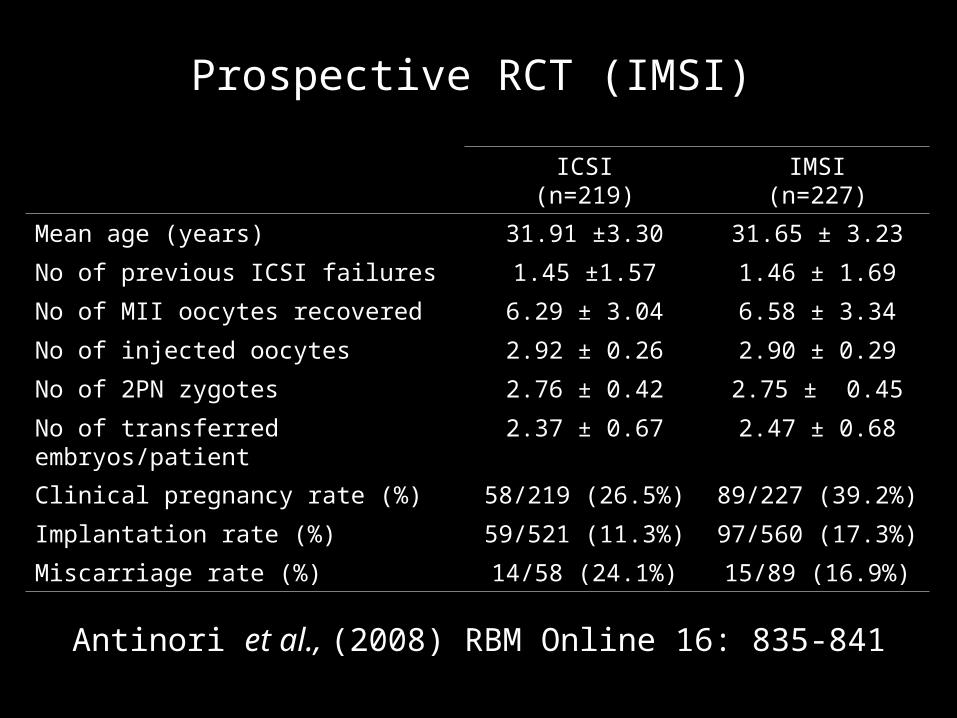
Antinori et al., (2008) RBM Online 16: 835-841
ICSI(n=219)
IMSI(n=227)
Mean age (years) 31.91 ±3.30 31.65 ± 3.23
No of previous ICSI failures 1.45 ±1.57 1.46 ± 1.69
No of MII oocytes recovered 6.29 ± 3.04 6.58 ± 3.34
No of injected oocytes 2.92 ± 0.26 2.90 ± 0.29
No of 2PN zygotes 2.76 ± 0.42 2.75 ± 0.45
No of transferred embryos/patient 2.37 ± 0.67 2.47 ± 0.68
Clinical pregnancy rate (%) 58/219 (26.5%) 89/227 (39.2%)
Implantation rate (%) 59/521 (11.3%) 97/560 (17.3%)
Miscarriage rate (%) 14/58 (24.1%) 15/89 (16.9%)
Prospective RCT (IMSI)

Antinori et al., (2008) RBM Online 16: 835-841
Prospective RCT (IMSI)
ICSI(n=219)
IMSI(n=227)
Mean age (years) 31.91 ±3.30 31.65 ± 3.23
No of previous ICSI failures 1.45 ±1.57 1.46 ± 1.69
No of MII oocytes recovered 6.29 ± 3.04 6.58 ± 3.34
No of injected oocytes 2.92 ± 0.26 2.90 ± 0.29
No of 2PN zygotes 2.76 ± 0.42 2.75 ± 0.45
No of transferred embryos/patient 2.37 ± 0.67 2.47 ± 0.68
Clinical pregnancy rate (%) 58/219 (26.5%) 89/227 (39.2%)
Implantation rate (%) 59/521 (11.3%) 97/560 (17.3%)
Miscarriage rate (%) 14/58 (24.1%) 15/89 (16.9%)

How is IMSI done?• Sperm obtained and
prepared
• Observed using Nomarski differential interference contrast optics
• Images captures on a video camera and projected on a monitor
• Total magnification = x6,600
• Each cell observed individually by a second embryologist
Antinori et al., (2008) RBM Online 16: 835-841

What do sperm vacuoles represent ?
Sperm from infertile men have a higher incidence of:
•DNA Fragmentation
•Errors of chromatin packaging
•Aneuploidy
Therefore, does the appearance of sperm vacuoles represent a non-invasive way of detecting one or more of these.

Sperm DNA fragmentation (TUNEL) #1
Oliveria et al., (2010) Fertility and Sterility 94: 1937-1940

Watanabe et al., (2011) Human Reproduction (in press)
Sperm DNA fragmentation (TUNEL) #2

Franco et al., (2011) Int Journal of Andrology (in press)
Sperm chromatin packaging
Normal Sperm Sperm with vacuoles
Positive staining 337 719
Negative Staining 498 632

Cássia et al., (2011) Fertility and Sterility 95: 990-993
Sperm and embryo aneuploidy
Characteristic ICSI(n=60)
IMSI(n=60)
P value
Female age (years) 38.1 ± 5.4 37.3 ± 3.2 0.5866
Male age (years) 42.6 ± 8.0 43.6 ± 8.9 0.7330
Total gonadotrophin dose (IU) 2,601 ± 676 2,697 ± 659
0.6592
Total aspirated follicles 13.2 ± 8.2 17.3 ± 10.7
0.0976
Total retrieved oocytes 8.6 ± 5.2 12.9 ± 9.7 0.1705
Sperm concentration (x106/ml) 22.2 ± 5.3 21.8 ± 6.7 0.7954
Sperm progressive motility (%)
35.6 34.8 0.6823
Fertilisation rate (%) 84.3 76.7 0.0638
Embryos 1.1 ± 1.0 1.7 ± 1.0 0.1705

• IMSI was associated with lower risk of:
Sex chromosome abnormality (OR 0.57; CI 0.37-0.90) Chaotic embryo development (OR 0.64; CI 0.43-0.96)
• Sex chromosome aneuploidy was higher in ICSI embryos compared to IMSI embryos (23.5% vs 15.0%; P=0.920)
• Unexpected higher incidence of euploid XX embryos derived from IMSI cycles compared to ICSI (30.0% vs 21.6%; P=0.0326)
Sperm and embryo aneuploidy
Cássia et al., (2011) Fertility and Sterility 95: 990-993
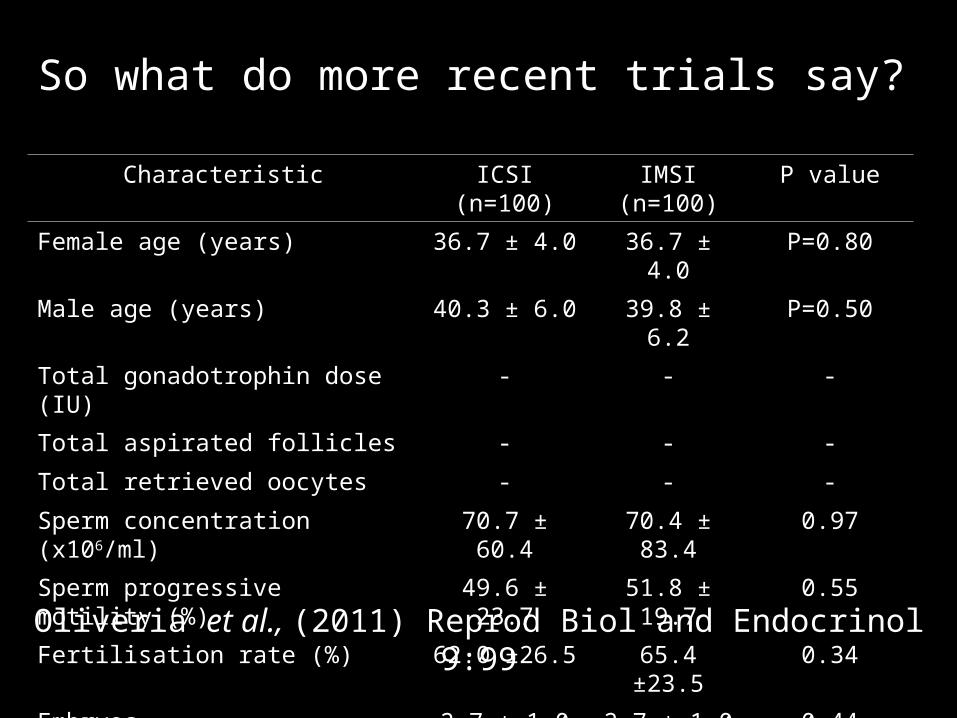
So what do more recent trials say?
Oliveria et al., (2011) Reprod Biol and Endocrinol 9:99
Characteristic ICSI(n=100)
IMSI(n=100)
P value
Female age (years) 36.7 ± 4.0 36.7 ± 4.0 P=0.80
Male age (years) 40.3 ± 6.0 39.8 ± 6.2 P=0.50
Total gonadotrophin dose (IU) - - -
Total aspirated follicles - - -
Total retrieved oocytes - - -
Sperm concentration (x106/ml) 70.7 ± 60.4 70.4 ± 83.4
0.97
Sperm progressive motility (%)
49.6 ± 23.7 51.8 ± 19.7
0.55
Fertilisation rate (%) 62.0 ±26.5 65.4 ±23.5 0.34
Embryos 2.7 ± 1.0 2.7 ± 1.0 0.44
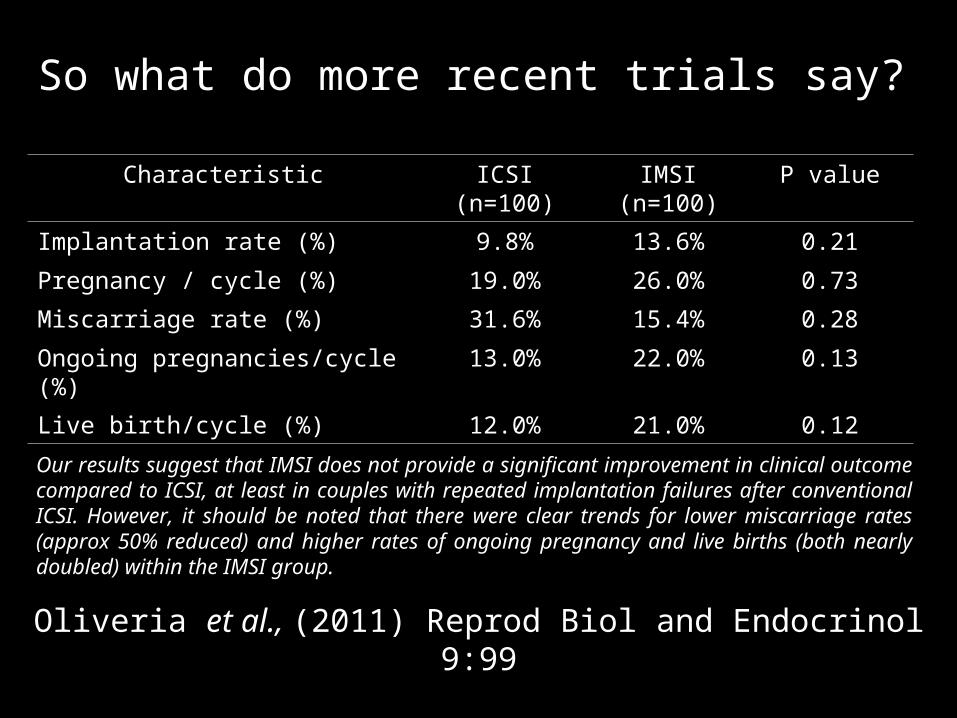
So what do more recent trials say?
Oliveria et al., (2011) Reprod Biol and Endocrinol 9:99
Characteristic ICSI(n=100)
IMSI(n=100)
P value
Implantation rate (%) 9.8% 13.6% 0.21
Pregnancy / cycle (%) 19.0% 26.0% 0.73
Miscarriage rate (%) 31.6% 15.4% 0.28
Ongoing pregnancies/cycle (%)
13.0% 22.0% 0.13
Live birth/cycle (%) 12.0% 21.0% 0.12
Our results suggest that IMSI does not provide a significant improvement in clinical outcome compared to ICSI, at least in couples with repeated implantation failures after conventional ICSI. However, it should be noted that there were clear trends for lower miscarriage rates (approx 50% reduced) and higher rates of ongoing pregnancy and live births (both nearly doubled) within the IMSI group.

Meta Analysis
Souza et al., (2010) RBM Online 21: 450-455
• The meta-analysis results demonstrated no significant difference in fertilization rate between ICSI and IMSI groups.
• However, a significantly improved implantation (OR: 2.72; 95% CI: 1.50-4.95) and pregnancy rate (OR 3.12; 95% CI 1.55-6.26) was observed in IMSI cycles.
• The results showed a significantly decreased miscarriage rate (OR 0.42; 95% CI 0.23-0.78) in IMSI cycles as compared with ICSI cycles.
• However, more randomized controlled trials are needed to confirm these results.
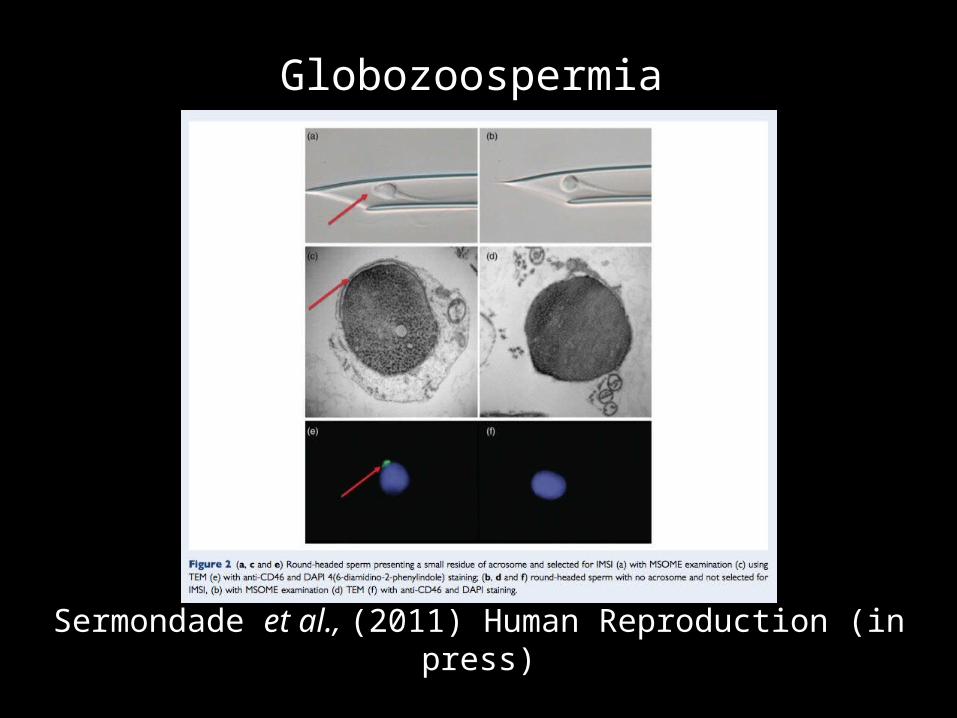
Globozoospermia
Sermondade et al., (2011) Human Reproduction (in press)

• In theory IMSI offers some advantage to sperm selection because of the high magnifications involved (x6,000).
• A single meta-analysis shows that IMSI improves pregnancy rates and decreases miscarriage rates – we need more studies!
• The science is unclear with many unsubstantiated claims made about what ‘qualities of sperm’ are being selected for.
• A Health Economic Analysis is needed given the additional staff time involved in performing IMSI (e.g. two embryologists).
• Should only be offered to patients in the context of an appropriately controlled clinical trial.
Conclusions








