
i
Shift Work: Health, safety and social effects
a case of rapidly rotating schedules
among male industrial workers
Dr. Anoop Velayudhan
Dissertation submitted in partial fulfillment of the requirements for
the award of the degree of
Master of Public Health
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology
Thiruvananthapuram, Kerala.
October 2011

ii
Acknowledgements
I extend my heartfelt gratitude to Dr.K.RThankappan , Dr.Sundari Ravindran,
Dr.V.Raman Kutty, Dr.Sankara Sarma , Dr.Mala Ramanathan , Dr. Kannan Srinivasan ,
Dr.Biju Soman, Dr.Manju Nair and Dr.Ravi Prasad Varma. I could see so far, only because I
stood on the shoulders of these giants.
I would like to thank my guide Dr.Ravi Prasad Varma, who put up with all my
idiosyncrasies and mistakes. In the language of this thesis‘s subject, he has always awakened
me when I was asleep, directed me whenever I was clueless, consoled me when I was
confused, and also asked me to rest and sleep when I was weary. He has never accepted
anything less than my best efforts.
This thesis owes its existence to Dr. Mohandas, Occupational Health specialist at
Travancore Titanium, who brought my attention to the problems of shift work, the need and
potential of research in it.
I would like to thank Dr.Ashalatha for giving me her time, technical help and
encouragement during this study. I thank Sunitha for teaching me the neuropsychology tests
and Dr.Ailey Alexander for discussing them with me.
I thank the management and staff of Kerala Minerals and Metals Ltd and also
Travancore Titanium for allowing me to conduct this study there. I am indebted to
Mrs.Bindu, administrator, Travancore Titanium, Dr.Bipin Pillai Medical Superintendent, and
Mrs.Jayanthi Bai, administrator, KMML.
I am indebted to Kerala State Council for Science Technology and Environment who
provided partial funding for this research and made my expenses, thus bearable.
I am grateful to all the workers who participated in this study and helped me during
the course of survey. They have taught me lessons about life in 3 months than I could have
learnt on my own in 3 years.
This thesis would not have been possible without the support of all my friends at
Achutha Menon Centre for Health sciences. Thanks to them, I found joy in every moment, in
the last two years. I am indebted to Dr. Ashish Anand, a dear friend and philosopher who
spared his time and best efforts to read and correct this work, while mending broken bones.
At last, I thank my family for their love, care and for simply being there for me, no
matter what. My parents and wife have been my ultimate strength and love. My Uncle
Mr.Aundeeshwaran, my brother and sister along with my friends helped me in various stages
of work and encouraged me to push myself further. I thank them too.

iii
Certificate
I hereby certify that the work embodied in this dissertation entitled ―Shift
Work: Health, safety and social effects-a case of rapidly rotating schedules
among male industrial workers‖ is a bona fide record of original research work
undertaken by Dr. Anoop Velayudhan, in partial fulfillment of the requirements
for the award of the degree of ‗Master of Public Health‘ under my guidance and
supervision.
Dr.Ravi Prasad Varma P
Assistant Professor
Achutha Menon Centre for Health Science Studies,
Sree Chitra Tirunal Institute for Medical Sciences and Technology,
Thiruvananthapuram, Kerala.
28th October, 2011.

iv
Declaration
I hereby declare that the work embodied in this dissertation entitled ―Shift
Work: Health, safety and social effects-a case of rapidly rotating schedules
among male industrial workers‖ is the result of original research and has not
been submitted for any other university or institution.
Dr. Anoop Velayudhan, MPH-2010,
Achutha Menon Centre for Health Science Studies,
Sree Chitra Tirunal Institute for Medical Sciences and Technology,
Thiruvananthapuram, Kerala.
28th
October, 2011.

v
TABLE OF CONTENTS
CHAPTERS
LIST OF TABLES
LIST OF FIGURES
ABSTRACT
CHAPTERS
Number Chapter Name Page No
1 Introduction 1
2 Literature review 2
2.1 Definition of shift work sleep disorder 2
2.1.1 Circadian rhythm disorders 2
2.1.2 Shift work 3
2.1.3 Shift work sleep disorder 3
2.2 Magnitude of problem 5
2.2.1 Public health importance 5
2.2.2 Reasons for shift work 6
2.2.3 Prevalence of shift work sleep disorder 6
2.3 Biomedical theory-Normal sleep and shift work sleep
disorder 10
2.3.1 The circadian system 11
2.3.2 Types of circadian rhythm disturbances 13
2.3.3 Shift work sleep disorder 14
2.4 Diagnostic and therapeutic features 15
2.4.1 Diagnosis 15

vi
2.4.2 Differential diagnosis 16
2.4.3 Treatment 16
2.5 Impact of shift work sleep disorder 17
2.5.1 How shift work affects health 17
2.5.2 Gastrointestinal disorders 18
2.5.3 Cardiovascular disorders 19
2.5.4 Mental health 20
2.5.5 Accidents 20
2.5.6 Social and domestic problems 20
2.5.7 Cognition and executive functions 21
2.6 Prognosis 21
2.7 Current recommendations 22
2.8 Rational of study 22
2.9 Research question 23
2.10 Objectives 23
3 Methodology 24
3.1 Study design 24
3.2 Cross sectional study 24
3.2.1 Study setting 24
3.2.2 Sampling unit 24
3.2.3 Sample size 24
3.2.4 Sample selection 24
3.2.5 Inclusion and exclusion criteria 25
3.2.6 Data collection 25
3.2.7 Data storage 27

vii
3.2.8 Data entry, analysis and statistical measures 27
3.2.9 Variables used in the study 27
3.2.9.1 Dependent variables 27
3.2.9.2 Independent variables 29
3.3 Ethical Considerations 29
3.3.1 Risk to participants 29
3.3.2 Privacy and confidentiality 30
3.3.3 Benefits 30
3.3.4 Informed consent process 30
3.3.5 Funding 31
4 Results
4.1 General description of survey outcome 32
4.2 Univariate analysis -Demographic description of study
subjects 32
4.3 Bivariate analyses 32
4.3.1 Types of shift cross tabulated against
morbidities and co-morbidities 35
4.3.1.1 Sleep disorders 35
4.3.1.2 Symptoms suggestive of Gastro
intestinal, cardiovascular and
mental health status of workers 37
4.3.1.3 Occupational health issues 38
4.3.2 Associations of insomnia or Excessive
sleepiness with various factors 41
4.4 Multivariate analysis 46
4.5 Clinical tests 48
viii
5 Discussion and conclusion 52
5.1 Discussion 52
5.1.1 Relation of work schedule with sleep-
Prevalence of insomnia or excessive
sleepiness 52
5.1.2 Shift work and its correlations 53
5.1.3 Insomnia or Excessive Sleepiness and its
correlations 54
5.1.4 Clinical tests 55
5.2 Strength and Limitations 57
5.3 Conclusions 58

ix
List of Tables
Table No. Title Page no
1 Mean age, BMI, years in service of workers 33
2 Age of workers segregated into five year age groups 34
3 Marital status and Habits of workers 35
4 Insomnia, Excessive Sleepiness and Insomnia or Excessive
sleepiness among workers
37
5 Symptoms suggestive of health problems among workers 38
6 Health problems(self reported) among workers 39
7 Accidents ,injuries and job satisfaction among workers 40
8 Social and domestic situation among workers 41
9 Bivariate analysis-Associations of Insomnia or Excessive
sleepiness
42
10 Bivariate analysis-Associations of Insomnia or Excessive
sleepiness
43
11 Bivariate analysis-Associations of Insomnia or Excessive
sleepiness
44
12 Bivariate analysis-Associations of Insomnia or Excessive
sleepiness
45
13 Multivariate analysis-factors associated with insomnia or
excessive sleepiness-Model 1
46
14 Multivariate analysis-factors associated with insomnia or
excessive sleepiness-Model 2
47
15 Multivariate analysis-factors associated with insomnia or
excessive sleepiness-Model 3
47
16 Clinical test scores among workers-RAVLT 49
17 Repeated Measures anova test of five rounds of RAVLT 50
18 Clinical test scores among workers-Trail A, Trail B and Digit
span
51
x
List of Figures
Figure no. Title Page
1 Entertainment of sleep wake cycle by light. 11
2 A The Normal sleep cycle 12
2 B Sleep cycle in a shift worker 13
3 Conceptual framework :Disease mechanisms in shift
work
18

xi
ABSTRACT
Background: This study was designed to examine the effects of shift work on the health and
lives of Industrial workers and to ascertain the prevalence of shift work sleep disorders and to
find its associations
Methods: It is a cross sectional study using self administered questionnaires.482 male
industrial workers of age > 18 years with mean age, participated in the study. Demographic
variables and work related factors were collected. General Job satisfaction, Insomnia scores,
Epworth Sleepiness score, and the Standard shift work Index were used to capture general
health, social and domestic situations. Clinical tests were done on a subset of the workers (30
regular and 30 shift worker) .Data was entered during Epidata ver 3.1 and analyzed using
spss ver.17
Results: Age adjusted prevalence of Insomnia or Excessive sleepiness among Shift workers
is 33.79% and Age adjusted prevalence of Insomnia or Excessive sleepiness among Regular
workers is 12.59%.Sleep disorder (insomnia or excessive sleepiness ) among workers. Work
schedule and Angina were found to be significantly associated with Sleep disorder (insomnia
or excessive sleepiness).Shift workers were found to be 2.71 times more likely to be
associated with sleep disorder, than their regular work counterparts (95% CI=1.58-4.66).Also
workers with Self reported Angina were 1.07 times more likely to be having Sleep disorder
(95% CI 1.08-6.13) than those without self reported angina.
Fewer shift workers reported that their work schedule interfered with domestic things
to do (45.7%) compared to regular workers (56%).Fewer shift workers (39%) than regular
work mates (60.1%) reported that their work interfered with non domestic things to do.
Contrary to expectation, accidents were lesser among shift worker (3.9%) than regular
workers (11.9%)
Shift work seems to affect memory (both immediate and delayed) among workers, as
suggested by Ray‘s Auditory Verbal Learning test, done among other neuro psychological
test
1
CHAPTER 1.INTRODUCTION
"And God divided the light from the darkness, and God called the light day, and the darkness
He called night. And the evening and the morning were the first day‖ (Genesis 1:4–5, King
James Version).
Under normal circumstances, the synchronization of our inherent time rhythms with
each other and with environmental rhythms (external time cues) maximizes our waking and
sleeping performance and promotes overall well-being. Unfortunately ‗Night work‘ or
working at night is opposed to the innate drive to sleep at night and work during the daytime.
Shift work in general and rotating work schedules commonly known as shift
schedules, causes disruption of biological rhythms, which is called circadian
desynchronization. The effects of such erratic work schedules are various. It has a negative
influence on performance efficiency, health and social well-being. It also makes
concentration difficult, which increases the possibility of errors or accidents-a risk both to the
worker and to the public. It causes disturbance of gastrointestinal systems and elevated risk of
cardiovascular disease. A shift work schedule affects not only the worker but also his family,
due to the different time table a shift worker follows, thus debilitating his personal life.
The importance of sleep can never be underscored and effects of its deprivation never
fully comprehendible. The problems of shift workers are the major focus here. Sans sleep,
sans health, sans safety shift workers are specifically denied of the tender loving care of the
universal physician as Sophocles described.
"Sleep, thou patron of mankind, Great physician of the mind who does nor pain nor sorrow
know, Sweetest balm of every woe."

2
CHAPTER 2. LITERATURE REVIEW
Literature regarding shift work and shift work sleep disorder was searched for in
books, journal articles and textbooks of sleep medicine and of neurology. The internet was
the predominant medium used. Journal publications, research papers, theses were referred to
understand and correlate available facts and nuances of the problem. Formatively, goggle
search yielded figures, report and other newspaper and grey literature on shift work and sleep
deprivations. For legitimate articles, PubMed repository was searched using MeSH term for
Shift work sleep disorder which was-―Sleep disorder, Circadian Rhythm‖.1048 article were
found on Pub Med (305 full free text,95 reviews).
The following themes were prepared to guide specific facets regarding the interest of
research and review shall also be written along the same lines.
A) Definition of Shift work Sleep Disorder
B) Magnitude of problem (Public Health importance, global and national
scene)
C) Biomedical theory-Normal sleep cycle and Shift work disorder
D) Current Diagnostic and Therapeutic techniques
E) Dynamics of Problem-determinants and associations
F) Impact of Shift work disorder-on Health, its Economical & Social consequences
G) Prognostic factors
H) Recommendations
2. 1. Definition of Shift work Sleep Disorder
2.1.1. Circadian rhythm disorders:
The twenty four hour intrinsic rhythm of the body is called circadian system. It exerts
a powerful influence, directly through its regulation of metabolism, and indirectly through its

3
interference or promotion of sleep. Disorders of sleep that arise as a result of disruption of
this rhythm are called circadian rhythm sleep disorders.1
Circadian rhythm sleep disorder can result from alterations in the endogenous
circadian clock (delayed sleep phase [DSP], advanced sleep phase [ASP], free running type,
and irregular sleep-wake cycle) or changes in the physical environment in relation to the
endogenous clock (shift work disorder and jet lag).2In most circadian disorders, the problem
is that the patient cannot sleep when sleep is desired, needed, or expected. As a result of sleep
episodes occurring irregularly, the corresponding wake periods may occur at undesired times.
Consequently, the patient complains of Insomnia or Excessive Sleepiness (ES).1 Today, large
proportions of the population in any nation have work schedules that interfere with night
sleep and therefore have people suffering from disturbed sleep and excessive sleepiness .3
However, sleep disorders connected with shift work have not received much clinical
attention despite the fact that the severity of the sleep impairment in shift and night work is as
high as that in traditional insomnia and seems to affect three fourths of those who work shifts
or at night.4
2.1 2. Shift work:
Shift work as per the standard definition, itself is defined as essentially involving
hours of employment during non-standard or alternative hours, i.e., work outside of the
typical day schedule of 8 a.m. to 5 p.m.5
2.1.3. Shift work sleep disorder:
Shift work sleep disorder or shift work disorder (SWSD or SWD) is defined by the
International Classification of Sleep Disorders as consisting of symptoms of insomnia or

4
excessive sleepiness that occur as transient phenomena in relation to work schedules (ICSD
category 307.45-1).1The work is usually scheduled during the habitual hours of sleep (i.e.,
shift work–rotating or permanent shifts), roster work, or irregular or undetermined hours of
work. The sleep complaint typically consists of an inability to maintain a normal sleep
duration when the major sleep episode is begun in the morning (6 a.m. to 8 a.m.) after a night
shift. The reduction in sleep length usually amounts to one to four hours. Subjectively, the
sleep period is perceived by the worker as unsatisfactory and not refreshing. The insomnia
appears despite the patient‘s attempts to optimize environmental conditions for sleep. The
condition usually persists for the duration of the work-shift period. Excessive sleepiness
usually occurs during shifts (mainly night) and is associated with the need to nap and is
associated with impaired mental ability because of the reduced alertness.
The Diagnostic and Statistical Manual of Mental Disorders-IV defines shift work
sleep disorder as ‗‗report of difficulty falling asleep, staying asleep, or non-restorative sleep
for at least one month‘‘ and it must be associated with ‗‗a work period that occurs during the
habitual sleep phase.‘‘ There are also required effects on impairment of wakefulness.
ICSD gives the Diagnostic Criteria for Shift Work Sleep Disorder (307.45-1) as
A. The patient has a primary complaint of insomnia or excessive sleepiness.
B. The primary complaint is temporally associated with a work period (usually night work)
that occurs during the habitual sleep phase.
C. Polysomnography and the MSLT demonstrate loss of a normal sleep-wake pattern (i.e.,
disturbed chronobiologic rhythmicity).
D. No medical or mental disorder accounts for the symptoms.
E. The symptoms do not meet criteria for any other sleep disorder producing
insomnia or excessive sleepiness (e.g., time-zone change [jet lag] syndrome).

5
Severity Criteria:
Mild: Mild insomnia or mild excessive sleepiness, the sleep deficit is often one to two hours.
Moderate: Moderate insomnia or moderate excessive sleepiness, the sleep deficit is often two
to three hours. Severe: Severe insomnia or severe excessive sleepiness, the sleep deficit is
greater than three hours.
Duration Criteria:
Acute: 7 days or less. Sub acute: More than 7 days but less than 3 months. Chronic: 3
months or longer
2.2. Magnitude of problem (Public Health Importance, Global and national scenario)
2.2.1. Public Health importance
Work patterns of a substantial proportion of the population now extend beyond
regular day-work hours; variable schedules (often including evening or night work) and
rotating shifts are both widespread and expanding.
In a 2005 European survey, 28% of the workforce had variable work patterns, 10%
had evening or night schedules, while 17% worked two-shift or three-shift rotating schedules
.7 Similarly, analyses of U.S. survey data showed that, in 1997, 27.6% of the workforce had
flexible work schedules, while 16.8% of full-time employees had ‗alternative‘ schedules
involving work outside normal day time hours (06.00-18.00 hrs), 6.4% of whom worked
night or rotating shifts.8These proportions varied by occupation; rotating shifts were
particularly common in security services (16.3%), mining (12.5%), and catering (8.7%), but
infrequent among professionals and managers (1.7%). Night work was prevalent in health
care, manufacturing, and manual occupations. Global trends towards a ‗24-hour society‘

6
suggest that these proportions are likely to rise; thus, the implications of shift work for
physical and mental health is not only a matter of current concern but also one that is likely to
become increasingly important in the future .9,10,11
Shift work poses a serious public health
risk, as it can impair an individual‘s ability to perform effectively and may lead to
occupational, traffic or even domestic accidents.
. 2.2.2. Reasons for shift work
Society and employer reasons for shift work are aplenty. A major reason is that
modern technology has made it possible to work day and night. This ―24-hour society‖ of
ours requires that key services be provided at all times. Critical services include public safety,
such as police and fire protection, military defense, health care, transportation and public
utilities, such as electrical power, water and telephone. Certain industries must operate 24
hours per day because the production process is much longer than 8 hour and must be
performed continuously.12
Chemicals and manufacturing industries need to be operated
continuously in order to be profitable.
2.2.3. Prevalence of shift work sleep disorder
Depending on the country, at least between five to eight percent of the population is
exposed to night work. Thus prevalence of SWD may be roughly estimated to be between
two to five percent of the total population.13
An authoritative and well defined study by Drake and colleagues report that the true
prevalence of SWSD is 10.0% among shift workers, and gives an overall prevalence of 1%
.14
The study was done In the general population of Detroit in USA.2036 day-shift, 360
rotating-shift, and 174 night-shift workers participated. This study used Minimum
International Classification of Sleep Disorders.1 In this study, ES was defined by an Epworth

7
Sleepiness Scale(ESS)7 score of the total sample mean + 1 standard deviation (effectively, an
ESS score of ≥13, compared with the more commonly applied ES diagnostic score of ≥10).
Insomnia was diagnosed using Diagnostic and Statistical Manual of Mental Disorders. Drake
and colleagues reported that 32.1% and 26.1% of night-shift and rotating-shift workers,
respectively, met their pre specified ES and/or insomnia criteria, compared with 18.0% of day
workers.
Calculating the ―true‖ prevalence of ES and insomnia—and therefore SWD—in
night-shift and rotating-shift workers was reported to be approximately 14.1% and 8.1%,
respectively. When it is considered that approximately 6% of all workers in the United States
perform night or rotating shift work, the overall prevalence of SWD in the general population
was estimated to be approximately 1%.This study simply deducted the prevalence of SWD
among day workers from those of shift workers. This prevalence may not correct, as this
value seems to be actually the excessive risk or prevalence among shift workers.
Also, this result is lower than the 2% to 5% estimated in the ICSD–2 coding manual
and some sleep specialists have argued that the figure put forward by Drake and colleagues is
conservative.15
However, Drake and colleagues had also applied the more usual ES diagnostic
measure of an ESS score of ≥10 and, using this criterion, found a much higher prevalence of
ES in their study population: 44.8% of night-shift workers and 35.8% of rotating-shift
workers were found to have ES and therefore would also be considered to have SWD,
provided their symptoms persisted for ≥1 month.
A 2007study of 4471 US police officers reported that 2.0% of this population had
SWD, which was defined by the occurrence of both insomnia and ES in associated with a
recurrent schedule of work that overlapped the normal rest period.16
8
During the 1998 Helsinki Heart Study, researchers had also examined the occurrence
of insomnia and/or ES over a 3month period in a population of approximately 3000 middle
aged men participating in a coronary heart disease prevention trial.17
Persistent insomnia was
reported by approximately 50% of rotating- and night-shift workers, whereas persistent ES
was reported by approximately 25% of shift workers overall; those with ES and/or insomnia
therefore met the diagnostic criteria for SWD.
Contrastingly, a study using the Multiple Sleep Latency Test in a population of shift-
working, long-haul bus drivers reported that the criteria for ES were met by 38% to 42% of
subjects.18
Also in contrast, in a study among Italian police officers, insomnia or hypersomnia
were reported by a significantly higher proportion of shift-working personnel compared with
their day-working colleagues (insomnia, 25.9% vs 15.8% , hypersomnia 4.9% vs 2.2%).19
Alternatively, other studies have reported the prevalence of unplanned napping at
work, which may be indicative of ES or sleep deprivation. For example, in a study of almost
700 registered female nurses, approximately 35% and 32% of participants working rotating
or night shifts, respectively, reported episodes of unplanned sleep at work and may therefore
have been at risk for developing shift work disorder.20
In another study of 400 shift workers it
was found that the proportion with a very negative attitude to work hours constituted 8% and
were mainly characterized by marked sleepiness and sleep complaints.21
Summarily, the estimates of the prevalence of shift work sleep disorders have used
different criteria, measures of insomnia or sleepiness and different methodologies. Today,
little overt data exist for the prevalence of SWD. Although the occurrence of insomnia and/or
ES has been studied in various shift-working populations, frequently only one symptom is
analyzed.22

9
Interestingly, Population based polls have found a different prevalence among
respondents. NSF's 2005 Sleep in America poll says that shift workers are more likely to
suffer from insomnia as well as excessive daytime sleepiness. Their poll found a higher
prevalence (61% vs. 47% and 30% vs. 18% respectively).22
If data from United states census is extrapolated, the estimated prevalence of sleep
related disorders in 2004 India would be reportedly 156,628,027 from a population of
10,650,706,072.23
Data available and sleep specialists in United States affirm to these figures
presently.15, 22
Dr. Anuj Chandra, a Chattanooga sleep specialist who has been a leader in
bringing cutting edge sleep medicine to India, is categorical in his opinion that the prevalence
of sleep disorders in India is very similar to what it is in the United States.24
He is also
supportive about the NSF‘s 2005 Sleep in America poll and has advised that these may be the
realistic figures actually seen at the population level.
Studies in India in this arena of sleep disorders are sparse but growing.
The first population based study was undertaken to know prevalence of Obstructive
Sleep Apnea Syndrome (OSAS) at the Vallabhbhai Patel Chest Institute, Delhi, India .A total
of 7975 participants were included. Sleep-related symptoms were seen in 5.1% of subjects.
They estimated prevalence of OSAS is 2.4% in males and 1% in females.25
An article by Dr.Chokroverty provides basic information about some important
laboratory tests and principles of treatment of sleep disorders to the general
physicians.26
Another article in the Indian journal of Medical research , talks about
Circadian rhythm and sleep disorders (CRSD)2 and describes the problem and highlights the
issue as elaborated in the International Classifications of SleepDisorders-2.27
An Editorial in
the Indian journal of Medical research shows how the physicians in India have finally
10
wakened to the reality of sleep disorders. But still research is mainly concentrated on
Obstructive Sleep Apnea syndrome, its research and treatment at large.28
In India, there are no statistics available on the shift working population. Even the
total number of persons in the work force is unknown. According to official figures, from
1981 to 2001 the total number of workers grew more than 50 per cent from approximately
245 million to 402 million persons.29
These figures count only those who are considered to
have ―engaged in economically productive activity for 183 days or more.‖ The actual number
of persons in the work force is likely to be much higher. The Survey results of 2008-09 reveal
that about 94% factories are covered under manufacturing activities giving employment to
about one crore employees, which accounts for nearly 97% of the total number of persons
engaged in the total factory sector.29
2.3. Biomedical theory-Normal Sleep cycle and shift work disorder
Humans and almost all organisms have predictable daily patterns in function and
functionalities. In spite of minor variations in heart rate, blood pressure, and the release of
digestive enzymes, most physiological processes, have a set rhythm. This may be attributed
to the neuroendocrine cycle or the inbuilt human sleep wake cycle.30,31
The word ‗circadian‘ from circa dies (Latin), means ―around a day‖ and refers to the
innate clock within the hypothalamus in the brain. This clock functions on an 24.2 hour cycle
approximately.31
Daylight and social cues tune the circadian rhythm to the 24-hour day.The
current understanding of the circadian system in mammals may be used to describe the
features of the 6 recognized circadian rhythm sleep disorders (CRSDs).

11
2.3.1. The Circadian system-The circadian system consists of 3 parts:
(1) Input pathways (2) Central oscillator and (3) Output pathways.
In Humans, the circadian clock governs sleep in a linear pathway. Retina captures
light and is via melanopsin in ganglion cells of the retinohypothalamic tract transfers it to the
suprachiasmatic nuclei (SCN) in the hypothalamus. The hypothalamus is the vortex of
circadian cycle. The hypothalamus reads it as length of day and transfers signals further to the
pineal gland. The pineal gland is located near the centre of the brain, between the
two hemispheres. It secretes melatonin during night for a duration corresponding to the
usual dark period of the day (scotoperiod) .
FIGURE 1.-Entertainment of sleep wake cycle by light.
Source:Christopher L. Drake,The characterization and pathology of circadian rhythm sleep
disorders.35
The SCN activates other output pathways, like the adrenal gland. This releases the
stress hormone cortisol in the morning prior to waking.The SCN is also found to rhythmically
transcribe clock genes controlled by auto regulatory feedback. It ensures autonomous
working and also responsiveness to external light and dark cycle. Clock genes that have been

12
described in humans are hPer (period homolog)1, hPer2, hPer3, hCLOCK (circadian
locomotor output cycles kaput), hCK(casein kinase)1δ, and hCK1ε. 32
Interestingly, the sleep-
wake cycle is not solely ruled by the circadian system. Sleep pressure or a homeostatic sleep
drive is inevitable after successive waking hours. Usually two systems act together
synergistically, with the homeostatic system encouraging sleep, while the circadian signal
opposes this process by promoting wakefulness
Normally, the circadian wakefulness increases as the day progresses and then dips
with the melatonin secretion at the start of evening. This triggers sleep onset. In normal case,
circadian and homeostatic factors work synergistically to promote sleep and wakefulness
alternately. 33
However, when the body‘s internal circadian phase is disturbed, the homeostatic
and circadian systems are unable to maintain appropriate sleep and wake cycle. In Shift work,
workers may struggle to stay awake at night in the face of increased homeostatic pressure for
sleep, without the benefit of a wake-promoting signal from the SCN
FIGURE 2A The Normal sleep cycle
Source:Christopher L. Drake,The characterization and pathology of circadian rhythm sleep
disorders

13
During shift Work, circadian drive for wakefulness, works against forced sleep at day
time. During night-time work hours, homeostatic drive for sleep acts against the circadian
need and demand for wakefulness
FIGURE 2B-Sleep cycle in a shift worker
Source:Christopher L. Drake,The characterization and pathology of circadian rhythm sleep
disorder.
2.3.2. Types of circadian rhythm sleep disorder
The 6 main CRSDs can be broadly classified into 2 types: Intrinsic and Extrinsic.
Intrinsic CRSDs are characterized by asynchrony between the patient‘s sleep-wake cycle and
the external day-night cycle, due to dis-regulation within the internal circadian system. These
are Delayed sleep-phase disorder, advanced sleep-phase disorder, free-running disorder (non–
24-hour sleep/wake syndrome, and irregular sleep/wake rhythmExtrinsic CRSDs result from
an imposed or forced change in the behavioral timing of sleep and wakefulness compared to
internal circadian timing. Shift-work disorder and jet lag disorder are extrinsic CRSDs

14
2.3.3. Shift-work sleep disorder
Shift work sleep disorder occurs when work or occupation demands that the worker
function at times that are in opposition to his or her body‘s normal circadian-controlled
periods of sleep and wake.
Generally, workers with SWD experience insomnia when trying to sleep and/or have
conversely excessive sleepiness when trying to remain awake. Sleep in patients with SWD is
broken, with marked difficulty in maintaining sleep during day hours. Sleep lost due to shift
work over successive nights eventually snowballs into a sleep debt that intensifies the
homeostatic sleep drive.34
Over time, the circadian drive competes with this overwhelming
sleep debt, further exacerbating excessive sleepiness. This leads to impaired work
performance, and increases the risk of accidents in individuals with SWD.4
The high degree of variation between individuals in terms of the severity of symptoms
associated with shift work seems complicated. Research in melatonin rhythms indicate that
adapting circadian rhythms to their varying patterns of sleep and wake is not always possible.
Some workers may be physiologically unable adjust their circadian rhythms.35
Again;
adaptation may be possible in night-shift workers who are forced to go back to a night-time
sleep schedule on their days off. They thus do not have a regular circadian sleep/wake
adjustment with the light/dark cycle. Night-shift workers mal-adapting to their new shift
schedule report reduced sleep during the daytime, thus increasing the risk of developing
Shift work sleep disorder .36
Summarily, in patients with SWD in spite of trying to adapt and
adjust to the varying work schedule, unfortunately insomnia and/or excessive sleepiness seem
to persist.

15
2.4.Diagnositic and therapeutic features.
2.4.1. Diagnosis: Diagnosis is indicated by the presence of typical history combined
with work or occupational history of being engaged in shift work.
ICDS gives the Diagnostic Criteria for Shift Work Sleep Disorder. (307.45-1) .1
A. The patient has a primary complaint of insomnia or excessive sleepiness.
B. The primary complaint is temporally associated with a work period (usualy night work)
that occurs during the habitual sleep phase.
C. Polysomnography and the MSLT demonstrate loss of a normal sleep-wake pattern (i.e.,
disturbed chronobiologic rhythmicity).
D. No medical or mental disorder accounts for the symptoms.
E. The symptoms do not meet criteria for any other sleep disorder producing
insomnia or excessive sleepiness (e.g., time-zone change [jet lag] syndrome).
Minimal Criteria: A plus B.
Severity Criteria:Mild: Mild insomnia or mild excessive sleepiness, the Sleep deficit is
often one to two hours.Moderate: Moderate insomnia or moderate excessive sleepiness; the
sleep deficit is often two to three hours.Severe: Severe insomnia or severe excessive
sleepinessThe sleep deficit is greater than three hours.
Duration Criteria:Acute: 7 days or less.Subacute: More than 7 days but less than 3
months.Chronic: 3 months or longer
Polysomnographic Features: Polysomnographic recordings may be useful if the sleep
disorder is severe or the etiology of the sleep disturbance is in question. A 24-hour recording
over the first and last of the series of rotating shift is to be performed. Monitoring of an

16
episode of usual daytime wakefulness and night sleep during a daytime shift is ideal for
comparative purposes. If excessive sleepiness is part of the complaint, a multiple sleep
latency test should be carried out in the standard manner at least three times: at the beginning,
middle, and end of the work shift.
Polysomnography demonstrates impaired quality of sleep, with either a prolonged
sleep latency or shortened total sleep time. The sleep period may be fragmented, with
frequent arousals and awakenings. The MSLT may demonstrate excessive sleepiness during
the time of the work shift.
Other Laboratory Test Features: Actigraphy may be helpful to demonstrate a
disrupted sleep-wake pattern consistent with shift work sleep disorder. There may be a loss of
the normal pattern of circadian rhythmicity, as demonstrated by 24-hour temperature or
biochemical patterns.
2.4.2.Differential Diagnosis:
Disorders of initiating sleep disorders of sleep maintenance, depending on morning or night
shift. The excessive sleepiness should be differentiated from that due to narcolepsy or sleep
apnea syndrome. Sometimes, patients with sleep disorders such as narcolepsy tend to adopt
shift work as an attempt to rationalize symptoms of excessive sleepiness.
2.4.3 Treatment
Most essential thing is to identify and address any co morbid conditions that might
contribute to poor sleep hygiene and/or cause ES or fatigue during required periods of
wakefulness. Important co morbidities are other sleep disorders, such as obstructive sleep
apnea (OSA), and mood disorders, such as depression.

17
An algorithm for the management of SWD in the primary care setting, including steps
to evaluate co morbid disorders is given by Dr. Michael J. Thorpy.37
Non pharmacologic
interventions, available for the treatment of SWD are improvement of sleep hygiene,
exercise, and timed exposure to light.38,39,40
Pharmacologic interventions
The wakefulness-promoting agents modafinil and armodafinil are the only
interventions with FDA approval for use in patients with SWD and have been evaluated
specifically among individuals with ES associated with SWD.41,42,43
A number of studies among individuals undergoing simulated night-shift work
suggest that caffeine or stimulants such as methamphetamine may be useful to promote
wakefulness during the work period, although there may be some residual effects on daytime
sleep depending on the caffeine drink selected.44,45,46,47
Administration of the sleep-mediating
hormone melatonin is also reportedly effective in promoting daytime sleep.48
2.5 Impact of shift work sleep disorder
2.5.1 How shift work affect health
Mainly three pathways have been used to elucidate the relationship between shift
work and other concomitant problems.49,50,51
1) Disruption of circadian rhythms (this leads to sleep/wake disturbances producing
desyncronisation of biological clock finally leading to an increased susceptibility to disease)
2) Disturbed social and temporal systems from odd work hours leading to family problems
and stress

18
3) Behavioral changes in such as irregular or poor diet and, smoking. Also cholesterol, blood
pressure and cardiac activity show changes, and may act as mediators of morbidities.49
Shift workers have usually been noticed to have erratic lifestyles owing to their
behavioral and biological risk factor or both .52,53
Shift work has been reported to have
adverse effects on health even in the absence of SWD, there is growing evidence that shift
work may affects lifespan.14,15
Figure No.3.Disease mechanisms in shift work
Source:Knutsson A. Shift work and coronary heart disease
2.5.2. Gastrointestinal disorders
Gastrointestinal complaints are a regular among shift workers. These are about 2 to 5
times more common among night shift workers as compared with those not working nights
.54
Circadian disturbance is reported to affect the digestion, and absorption of food. After

19
adjusting for demographic variables, job, and lifestyle variables, shift workers have reported
higher prevalence of indigestion, heartburn, constipation, loss of appetite, and nausea than
day workers.55,56
. Evidence also links shift work to peptic or duodenal ulcer.57
In an Japanese study which used endoscopic examination, the prevalence of gastric
ulcer was 2.38% among shift workers, and 1.03% in day workers.58
Duodenal ulcers also
showed higher prevalence among shift workers in the same study. In an Italian study shift
work was also found to be associated with significant metabolic disturbance. The study
correlated shift work with with 3 of the 5 diagnostic symptoms of metabolic syndrome.59
In
an Japanese study, diabetes prevalence has been seen to increase with duration of exposure
to shift work. Here markers of insulin resistance was more common seen among in shift
workers .60
2.5.3. Cardiovascular disease
Shift work seems to be a significant risk factor associated with cardiovascular disease.
A meta-analysis of 17 studies of cardiovascular disease and shift work elaborates on this
assocations.61
Overall , shift workers were found to have a 40% excess risk for cardiovascular
disease when compared to day workers. Reportedly, night work limits the normal night time
reductions in blood pressure and also reduces heart rate variability.62
Such workers without
normal fluctuations are likely to develop hypertension, snowballs into adverse cardiovascular
outcomes.63
Also there is has been published evidence that ES may be a risk factor for
increased blood pressure.64
Tenkanen et al analyzing the Helsinki study in 1997 on a 6-year
prospective study of cardiovascular (CHD) risk, followed up 1806 industrial workers. He
found that overall, the relative risk of CHD among shift workers as compared to day workers
was 1.5 (CI 1.1- 2.1) .65
Shiftwork was also found to interact with smoking and obesity to

20
increase CHD risk. A review by Knutsson in 2003 reported evidence of an association
between shift work and coronary heart disease.50
2.5.4 Mental Health
Depression has been reported and linked to shift workers, especially among women.
Drake and colleagues‘s study had also reported that symptoms of SWD were associated with
elevated rates of depression (OR, 2.57 (CI 2.01-3.27)).14
He cautions us that although SWD
seems associated with depression, shift work does not increase the risk of developing mood
disorders .A study of radar controllers in the US Air Force using the Zung Anxiety and
Depression Scales reveal that shift workers with SWD were more likely to experience anxiety
and also more prone to depression.66
2.5.5. Accidents
Shift workers are more likely to have work-related accidents than are day workers.67
Chances of a medical resident or a nurse to have a injury ,or report an error was found to be
two times during a night shift or rotating than during a day shift.68
Police officers working shifts were seen to be more likely to experience a sleep
related accident at work or at home than were their regular work counterparts.(OR 2.24,p
<.0005).14
Accidents reported by workers going home after the night shift are more than those
reported by day workers.69,70
Excessive sleepiness in morning hours is also hypothesized to
be responsible for the increased rate of military flight accidents.71
2.5.6. Social and Domestic life
Working in shift seems to affect the quality of life. In the same study of American radar
controllers, it was seen that shift workers in general experienced more anxiety and irritability,

21
and that sleep disorder seems to lower the quality of life.51
Drake and colleagues‘s study also
had similar findings. They found more individuals with sleep disorder seem to miss social
and family interactions due to sleep problems than those without SWD.14
2.5.7. Cognition and Executive functions.
Independently, sleep deprivation and excessive sleepiness seems to impair memory, learning,
alertness, and work performance, even in the absence of overt circadian problmes.72,73
Also a study that assessed mathematical learning, reports that circadian disturbances
could be detrimental to learning, even among normal people who temporarily failed to adapt
their circadian cycles.74
Shift workers who suffer from a snowball effect of sleep deprivation
and excessive sleepiness have also been reported to have reduced attention, alertness and
consequently performance .Again alertness and cognitive processes may be impaired during
the transition from of shifts.75,76,77
2.6. Prognosis
Earlier it was thought that shift working would be better tolerated as time elapsed.
Shift workers might have fewer domestic pressures from children, and perhaps more coping
ability. The fact that older people seem to require less sleep than younger people, was also
supposed to help. Today the research findings seem to teach us otherwise.
Recent evidence seems to tell us that aging worker may not tolerate shift work as
deftly as young workmen .With age, sleep becomes shorter and fragmented. This can again
complicate the situation.78
But if recognized, diagnosed and treated, workers may be able to
adapt and resynchronize themselves in their bio rhythms, life and person. At its extreme, shift
work disorder may lead to Cancer. The International Agency for Research on Cancer (IARC)

22
has concluded that "shift work that involves circadian disruption" is considered a Group 2A
carcinogen and "probably carcinogenic to humans.‖79
2.7. Current Recommendations.
Today there are recommendations available at various levels to prevent and diagnose
this growing problem. National Institute of Occupational Safety and Health (NIOSH), USA,
has recommended measures to be taken at Organization level and also for the Individual
worker. 80,81
At the individual level some of them are -a healthy diet and exercise
program..82
Avoiding caffeine and alcohol close to bedtime.Developing a relaxing sleep ritual
and following good sleep hygiene.Keeping a regular sleep schedule—going to sleep and
waking up at the same time every day, including weekends.
The National Institute for Occupational Safety and Health (NIOSH) recommends that
organizations design health work schedules, allotting free time for needy workers, efficient
work load distribution and health work environments along with counseling programs.
2.8. Rationale of the study
There been little work to examine prevalence and consequences of shift work sleep
disorder in comparison to the difficulties with insomnia and excessive sleepiness experienced
by day workers. I have chosen to base my study among industrial worker as they are the most
affected due to shift work (They lack the cushioning of comfort provided by similar shift
working professionals)
23
2.9. Research Question
What are the detrimental effects of working in a varying pattern of work on the
quality of sleep and consequently work alertness, general health and social roles?
2.10. Objectives
1. To ascertain the prevalence of shift work sleep disorders and their associations with
performance and safety in terms of self reported injuries/accidents
2. To assess the impact of shift work on physical health with emphasis to
gastrointestinal system and cardiovascular system.
3. To find out the Impact of shift work on personal and family life as perceived by the
worker

24
CHAPTER 3. METHODOLOGY
3.1 Study Design: Cross sectional design
3.2 Cross sectional survey:
3.2.1 Study setting: The study was conducted among workers of Kerala Minerals and
Metals Ltd , Chavara, Kollam and Travancore Titanium Ltd ,two Public sector enterprises in
Kerala. Both have continuously running chemical plants, producing Titanium dioxide and
employ both shift and regular workers. Both have same shift timings and almost similar
salary packages. The work processes and factory setting are mostly similar, if not same.
3.2.2 Sampling Unit-Sampling unit was the ―Shift worker‖ as compared to
―Regular/Day worker‖
3.2.3 Sample size:
The difference in excessive daytime sleepiness (a key component of shift work sleep
disorder) obtained as per literature review to be 30 percent among shift workers and 18
percent among regular workers. This difference was used to fix the sample size. Sample size
was fixed to be 215 for each group of workers. This sample size was calculated using epi-info
version 3.5.2 statcalc to get a study result with 80% power and a maximum alpha error of
5%.Accounting for a non response rate or drop out of 30% the sample size was then rounded
to 280.Therefore final sample size was 560(280 regular workers and 280 shift workers)
During the course of the study, 560 workers were recruited, but due to drop outs, final
sample size obtained was 482. The study had 255 shift workers (intended 280) and 227
regular workers (intended 280).Coverage was therefore 86.07 percent.
3.2.4 Sample selection:

25
Random sampling method was followed by using employee roll, and spss random
selection procedure. It was duly seen that that the workers ―adjusted‖ and often interchanged
their shifts and work stations amongst themselves. Therefore in about 60 workers, the worker
who was working at the work station was taken in place of the worker chosen by the random
selection procedure.
For the clinical tests, again random sampling was done to obtain 30 random shift
workers and 30 random regular workers. They were obtained from among the workers
previously selected and from those who had given consent to undergo clinical testing. If any
of the workers were unavailable or expressed inability to undergo testing, the next worker in
the serial order was taken.
3.2.5 Inclusion and exclusion criteria-Workers who are on company rolls and have
been working in their respective shifts-regular or rotating, for 6 months were included in the
study. Exclusion criteria-workers who have been diagnosed with any kind of sleeping
disorder or are on therapeutic treatment for any sleeping disorder were excluded.
3.2.6 Data collection: Written Informed Consent was taken after assuring
confidentiality and non effect on Employee review, records, benefits and medical records.
Data was collected in 3 stages
(1) Recruitment of workers after explaining the study and obtaining informed
consent. The sleep log was assigned to be completed.
(2)A pretested questionnaire was used comprising of 2 instruments-A Work
log-to record shift work or normal working schedules, and a comprehensive
Questionnaire comprising of shift work sleep index, Insomnia questionnaire and

26
Epworth sleep questionnaire was then given to the worker to be returned after 2 weeks
along with the sleep log.
(3)Rey Auditory verbal learning tests (immediate and quick recall),Trail A,
Trail B and Digit span tests-forward and backward were done to check for fronto-
temporal functions, at a later date upon a selected subset of the sample.
All clinical tests were taught to the investigator, by a practising neuropsychologist,
under guidance of the consultant neurologist and sleep specialist. They were practiced upon
normal people and then upon screened patients attending a neurology clinic, after due
consent.
The Rey Auditory verbal learning tests (RAVLT) are useful in evaluating verbal
learning and memory. There are comprehensible ‗lay‘15 words, which read out read aloud at
the rate of one per second. The subjects were asked to repeat all the words he can remember,
in any order. This procedure is carried out a total of five times. Then second list of 15 words,
was presented a allowing the subject only one attempt at recall. Immediately following this,
the subject was asked to remember as many words as possible from the first list.83,84
The Trail Making Test is a measure of attention, speed and mental flexibility. Both
parts of the Trail Making Test consist of 25 circles distributed over a sheet of paper. In Part
A, the circles are numbered 1 – 25, and the subject was asked draw lines to connect the
numbers in ascending order. In Part B, the circles include both numbers (1 – 13) and letters
(A – L).The subjects were asked to draw lines to connect the circles in an ascending pattern,
but with the added task of alternating between the numbers and letters (e.g. 1-A-2-B-3-C).
The subjects were timed as they connected the "trail."85
27
Digit span is a common measure of short-term memory, the number of digits a person
can absorb and recall in correct serial order after hearing them .The has to remember a small
amount of information for a relatively short time, and the order of recall is important. To test
the auditory digit span of respondents, numbers were said slowly in one second intervals and
subjects were asked to repeat it back.86
3.2.7 Data storage: All data obtained were kept safely with the principal investigator,
who bears the sole responsibility for safe keeping and any breach of confidentiality. Data
shall be maintained by principal investigator for any future reference.
3.2.8 Data Entry, Analysis and Statistical Measures: All these data were entered in
Epidata version 3.1 and analyzed in SPSS version 17.Descriptive analysis was done to look at
the sample characteristics. Bivariate analysis was done to find the relation between the
predictor and outcome variables. Further multivariate analysis was done using binary logistic
regression and came up with the final models.
3.2.9 .Variables used in the study
3. 2.9.1.Dependent variables
Insomnia -Based on insomnia questions -described in Appendix B 2 and contained in
questions 3.16,3.21,3.23 and 3.15 of the questionnaire. Insomnia was taken to be present if
respondent had difficulty in going to sleep, sustaining sleep or had early awakening, any of
the above three accompanied with un refreshed sleep.
Excessive Sleepiness-Excessive Sleepiness was taken to be present if the Epworth Sleepiness
Scale described in Appendix B 3 and contained in question 3.28 of the questionnaire, gave a
total score of more than or equal to 10.

28
Insomnia or Excessive Sleepiness- This is based on the above two dependent variables,
Insomnia as well as Excessive sleepiness. For the prevalence of shift work sleep disorder, this
is also the working definition among workers who are in the shift work schedule.
Satisfaction with job-This is taken as general job satisfaction more or general job satisfaction
less, based on the median score calculated based on total score. Respondents scoring more
than 29 were taken as more satisfied, while respondents scoring 29 or lesser were taken as
less satisfied with job.
Gastro intestinal problems-This is based on the Physical health questionnaire-described in
Appendix B 4 and contained in section 4 question 4.1 (a) to 4.1 (h) in the questionnaire.
Median score was calculated. Respondents with score of 15 or more were taken to have
Symptoms suggestive of gastro intestinal diseases.
Cardiovascular problems-This is based on the Physical health questionnaire-described in and
Appendix B 4 contained in section 4 question 4.1 (i) to 4.1 (p) in the questionnaire. Median
score was calculated and respondents with score of 12 or more were taken to have Symptoms
suggestive of cardiovascular diseases.
Mental Health score-This is based on the GENERAL HEALTH QUESTIONNAIRE-
described in Appendix B 5and contained in question 4.7 of the questionnaire. Median score
was calculated and respondents with score of 10 or more were taken to have Poor Mental
health
Overall Socio and domestic Score-This is based on the SOCIAL AND DOMESTIC
SURVEY- described in Appendix B 6and contained in question 5.1 to 5.5 of the
questionnaire. Median score was calculated and respondents with score of 55 more were
29
taken to be more satisfied with time available after or around work in relation to their social
and domestic life.
3.2.9.2. Independent variables
Socio demographic variables-Age, Height, Weight, and Years in service, marital status and
Number of children were asked.
Work related variables-Work schedule was captured by work log. Among Shift workers,
reasons for working shifts, its perceived advantages and disadvantages were asked. They
were asked whether, they feel advantages outweigh disadvantages. They were also asked if
all things remaining equal, whether they would change over to regular shift.
Sleep related variables-Sleep quantity and quality were assessed by different questions.
Quantity of sleep was verified in a subsample using the sleep log.
Accidents and injuries variables-Accidents and injuries were asked for by asking for even
been witness to accident or injuries, or having had an accident or injury or having one on the
way back home after work. The shift /or timing of each of these was also asked.
Variables to capture Habits-Cigarettes smoked, units of alcohol, and cups of tea or coffee
taken in were asked. Also before and after shift information, regarding the same was asked.
3.3. Ethical considerations
3.3.1. Risks to the participants
There were no risks involved in participating in the study in the wake of all
precautions taken, to protect the identity of workers and anonymity maintained.
30
3.3.2. Privacy and confidentiality
Identity of the participants is known only to the principal investigator. A
dummy code was used and all personal details were erased after data collection. This
coding contained in the dummy code register, is maintained by the principle
investigator. Only the faculty guide, other than principle investigator has had access
to raw data that has already been coded anonymously. Whatever has been and will be
shared, for academic purposes is the summarized data of the whole sample. Access to
the personal identification data through the dummy code not only anonymised the
worker and also enabled to direct the worker to a sleep specialist in the case the
worker had a sleep disorder.
3.3.3. Benefits
This study offered the participant the chance to be diagnosed, if he suffers from
insomnia, excessive sleepiness or both. All workers diagnosed thus shall be referred to the
Comprehensive sleep clinic at Sri Chitra Institute for Medical Sciences and Technology .If
recognized, diagnosed and treated, workers may be able to adapt and resynchronize
themselves in their bio rhythms, life and person. They may be able to tide over the effects of
sleep defects and cure themselves of the sleep disorder. Also the study results may bring forth
policy changes which may prove beneficial to the community at large.
3.3.4. Informed consent process
Informed consent was taken by the principal investigator right before administering
the interview schedule at stage of recruitment. Clearance was obtained from the institutional
ethics committee before commencement of the study.

31
3.3.5. Funding source
Funding was applied for and part of funds required was obtained from Kerala
state Council for Science, Technology and Environment. All research work done and
presented herewith are independent of any influence whatsoever, and there are no
conflict of interests.

32
CHAPTER 4. RESULTS
This chapter describes the outcomes of data analysis in concurrence with the stated
objectives. After scrutiny, data entered was analyzed using SPSS for windows version
17.Baseline characteristics of the sample population were first understood. Using the
conceptual framework and based on literature review, data was analyzed for associations
between various independent variables and outcome variables.
4.1 General description of Survey outcome
Out of the 580 workers recruited for the study, only 482 returned their questionnaire,
despite best efforts. Not all workers responded to all questions in various sections of the
questionnaire. Therefore the number of respondents is also given wherever all the 482
respondents did not answer a question or section. Total workers in each category total are 227
in the Regular shift group and 255 in the Shift working group. Therefore final coverage is
86.07% of targeted size.For the Clinical tests, the tests were done by the principal
investigator who, at the time did not know about their responses or results of their
questionnaire replies.30 random regular workers and 30 shift workers who had been part of
the earlier survey were taken as a sub sample and tested.
4.2 Univariate analysis
4.2.1. Demographic description of the study subjects.
The mean age of regular workers was 45.14 (SD 9.029),while that of the shift
workers was 42.45(SD 9.330).Most regular workers were in the above 50 age group ,when
age was segregated into five year age groups. Five year age group was taken so as to
facilitate calculation of prevalence as compared to the WHO standard population. The shift

33
working group mainly composed of younger workers as indicated by 46 percent of them
falling in the 30-34 and 35-39 age group.The Mean Body Mass Index of regular workers was
25.24 (SD 2.96),while that of shift worker was 26.49 (SD 2.69).When categorized into
Undernourished, Normal BMI, Overweight and Obese, majority of the workers in both
category were overweight. More shift workers (67.2%)were overweight than regular
workers(50.4%).The mean number of years, served in the industry was comparable among
both categories of workers. On an average regular worker group had 17.33 yrs in service
while the shift workers had put in 15.87 yrs of service. Majority of the workers in both
groups had put in more than 14 yrs of service
Demographic
and Physical
characteristics
Regular worker, n=227
Mean(Confidence
interval)
Shift worker. n=255
Mean(Confidence
interval)
p value
Age 45.14(43.96-46.31) 42.45(41.30-43.59) 0.001
Body Mass
Index
25.24(24.85-25.62) 26.49(25.96-27.01) <0.001
Body Mass
Index
(n=479)
Underweight
Normal BMI
Overweight
Obese
(Grouped) n=226 (%)
2(.9)
102(45.2)
114(50.4)
8(3.5)
n=254(%)
1(.4)
62(24.5)
170(67.2)
20(7.9)
Total-479(%)
3(.6)
164(34.3)
284(59.3)
28(5.8)
<.001
Years in service Mean(Confidence
interval)
17.33(16.23-18.42)
Mean(Confidence
interval)
15.87(14.82-16.91)
0.59
Years in service
upto14yrs
>14 yrs
(Grouped) n (%)
95(41.9)
132(58.1)
n (%)
125(49)
130(51)
Total(%)
219(45.5)
262(54.5)
0.126
Table 1.Mean Age, Body Mass index and Years in service between regular and shift workers

34
Age groups Work schedule Total(%)
Regular workers (%) Shift workers (%)
20-24 yrs 1(0.4) 2(0.8) 3(0.6)
25-29yrs 16(7.0) 8(3.1) 24(5.0)
30-34yrs 17(7.5) 59(23.1) 76(15.8)
35-39yrs 35(15.4) 59(23.1) 94(19.5)
40-44yrs 29(12.9) 24(9.5) 53(11.0)
45-49yrs 41(18.1) 16(6.3) 57(11.8)
50-54yrs 53(23.3) 51(20.0) 104(21.6)
55-59yrs 35(15.4) 36(14.1) 71(14.7)
Total 227(100.0) 255(100.0) 482(100.0)
Almost 90 % of the men were married in both regular and shift working group.7.1 %
of the regular workers were unmarried as compared to 4.1 % of shift workers.
Regarding the habits of workers, 134 workers had responded to the question about
smoking. Smoking was uniformly seen in both work groups.30 percent of regular workers as
well as shift workers were smokers.155 workers had responded to the question regarding
alcohol consumption. 33 % of regular workers were alcohol users while 38.9% of shift
workers used alcohol. Due to the stigma regarding use of alcohol and smoking, probably
fewer people responded to these questions. 466 workers responded to question about tea or
coffee drinking. Both groups had high consumption of coffee and tea, typical of the culture
and work environment.
Table 2. Age of Regular and Shift workers segregated into five year age groups

35
Variable
Regular worker
225 (%)
Shift worker
255 (%)
Overall n(%) p value
Marital status
(n=480)
Married
Divorced
Widower
Unmarried
203(90.2)
5(2.2)
1(0.5)
16(7.1)
238(93.3)
3(1.2)
1(1.2)
11(4.3)
441(91.9)
8(1.7)
4(0.8)
27(5.6)
.342
Habits
Smokers(n=450)
Alcohol users
(n=441)
Tea/coffee users
(n=466)
64(30)
69(33)
202(93.1)
72(30.4)
90(38.9)
244(98.0)
136(30.2)
159(36.1)
446(95.7)
.939
.207
.009
4.3 Bi variate analysis-Three sets of analysis were attempted.
The first set of analysis intended to arrive at the problems of shift work. For this,
proportion of regular and shift workers were cross-tabulated against various co morbidities.
The second set of analysis aimed to arrive at the associations of sleep disorder, namely
Insomnia, Excessive Sleepiness and Insomnia or excessive sleepiness. For shift workers, this
corresponds to shift work sleep disorder‘s working definition. The third set of analysis aimed
to correlate the clinical findings between types of workers.
4.3.1 Type of shift cross tabulated against various morbidities and co morbidities.
4.3.1.1. Sleep disorders
Sleep variables collected from sleep section were used for bivariate analysis.
Insomnia, excessive sleepiness was calculated using questions and the Epworth sleepiness
Table 3-Marital status and Habits of Regular and Shift workers

36
scores as described before. The presence of either insomnia or excessive sleepiness was also
looked for, in order to calculate the prevalence of shift work sleep disorder, among shift
workers, according to the working definition of shift work sleep disorder.20(8.8%) regular
workers reported insomnia and 27(12%) had excessive sleepiness. In shift workers, 54
workers (21.2%) reported insomnia, while 71(28.1%) reported excessive sleepiness. Among
regular workers 41 (18.1) workers had either Insomnia or Excessive sleepiness. Among shift
workers, 103 workers (40.4) had either Insomnia or Excessive sleepiness. These results were
significantly different between both the groups of workers.
Thus as per definition, the prevalence of Shift work sleep disorder -insomnia or
excessive sleepiness among this population is 40.4%.
The risk difference may be calculated as follows. The prevalence of sleep disorders
being 18.1% in regular workers, the risk difference is 22.3% with a 95% CI of 14.47 to
30.13%. This estimate is suggestive of the actual location of the prevalence of shift work
sleep disorder after ruling out sleep disorders due to other causes. If the regular and shift
workers be considered as retrospective cohorts with the exposure being shift work and the
outcome to be sleep disorder, we may be able to assess relative risks ,since they are mutually
exclusive groups. The Relative Risk (RR) among shift workers as compared to regular
workers is 2.24 (95% CI 1.63-3.06)
When adjusted to age , according to the new World Health Organisation-2000-2005
standard population, the prevalence of shift work sleep disorder(insomnia or excessive
sleepiness among this sample is 30.74%. Similarly the prevalence of insomnia or excessive
sleepiness among regular workers is 26.14%.

37
Sleep Disorder Regular
worker n(%)
Shift
worker n(%)
Overall
n(%)
Odds ratio
(95% CI)
p value
Insomnia 20(8.8) 54(21.2) 74(15.4) 2.78(1.61-4.81) <0.001
Excessive
Sleepiness
27(12) 71(28.1) 98(20.5) 2.86(1.75-4.65) <0.001
Insomnia or
Excessive
Sleepiness
41(18.1) 103(40.4) 144(29.9) 3.07(2.02-4.68) <0.001
4.3.1.2. Symptoms suggestive of gastrointestinal, cardiovascular disease, and
mental health status of workers.
Based on the Physical health questionnaire, 16 symptoms along with their
severity or frequency were put forward to the worker, to capture any undetected morbidities
regarding the gastrointestinal system or cardiovascular disease. 84 regular workers (42.6%)
had symptoms suggestive of gastrointestinal disorder. More shift workers, 115 in number
(53.1%) had similar symptoms. Regarding Symptoms suggestive of cardiovascular diseases,
71 regular workers (36.2%) reported to having them, as compared to the higher number128
among shift workers (56.6%). This result is significantly different among both the groups and
is in alliance with the accepted current review of literature.
The General Health Questionnaire was used to arrive at the mental health status of the
workers. The mental health of both group of workers were comparable. Better mental health
was taken as the variable, compared to poor mental health based on median scores, and duly
cross tabbed with work schedule 98 regular workers (49.7%) were found to have better
mental health . Among shift workers, 120 workers (51.5%) were seen to have better mental
health based on their mental health score
Table 4- Insomnia, Excessive Sleepiness and Insomnia or Excessive Sleepiness
of Regular and shift worker

38
Table 5-Symptoms of Health problems among Regular and shift worker
Symptoms of
Health Conditions
Regular
worker n(%)
Shift worker
n(%)
Overall
n(%)
Odds ratio
(95% CI)
p
value
Symptoms
suggestive of
Gastrointestinal
diseases
84(42.6) 115(53.1) 119(48.1) 1.52(1.03-2.24) .035
Symptoms
suggestive of
Cardiovascular
diseases
71(36.2) 128(56.6) 199(47.2) 2.30(1.55-3.40) <0.001
Better Mental
Status
98(49.7) 120(51.5) 218(50.7) 1.07(.73-1.56) .717
4.3.1.3. Occupational issues among workers
History of other diseases commonly seen as occupational, was asked for among the
workers. These were either diagnosed diseases or self reported as having had them. Chronic
Back pain, Stomach or duodenal ulcers, Sinusitis/Tonsillitis, Bronchial Asthma, Angina,
Heart Attack, Hypertension, Arrythmia, Hypercholesterolemia ,Diabetes, Urinary infection,
Skin diseases, Chronic anxiety Depression, Arthritis, Hemorrhoids and Varicose veins were
the diseases asked among the workers.
Among these, Stomach or duodenal ulcers, Sinusitis/tonsillitis Angina, Hypertension,
Hypercholesterolemia, and diabetes prevalence was found to be significantly different among
the two groups of workers.31 regular workers(13.8%) had Stomach or duodenal ulcers,
compared to 57 shift workers(22.4%).Sinusitis/Pharyngitis prevalence was lower among the
regular workers. Only 28 of regular workers (12.6%) reported it, while 57 shift workers
(22.6%) had the same. Angina was also found to have a lower prevalence among regular
workers, with 15 percent cases (6.7%) as compared to th33 shift workers who reported to

39
have angina (13%).63 regular workers were reportedly hypertensive (28.3%),while 103 shift
workers were hypertensive(40.4%). 49 regular workers had high cholesterol(21.9%),while 81
of the shift workers had high cholesterol(31.8%). 55 regular workers (24.6%)were reportedly
diabetic while 87 of the shift workers were diabetic(34.3%).
Table 6-Self reported health problems among Regular and shift worker
Disease
(self reported)
Regular worker
n (%)
Shift worker
n (%)
Overall
n (%)
Odds ratio
(95% CI)
p value
Chronic Backache 30(13.7) 47(18.4) 77(16.1) 1.45(.88-2.39) .140
Stomach ulcers 31(13.8) 57(22.4) 88(18.4) 1.79(1.55-3.40) .016
Sinusitis/Pharyngitis 28(12.6) 57(22.6) 85(17.9) 2.04(1.24-3.34) .004
Asthma 35(15.7) 39(15.3) 74(15.5) .97(.54-1.59) .904
Angina 15(6.7) 33(13) 48(10) 2.08(1.09-3.94) .022
Heart attacks 6(2.7) 12(4.7) 18(3.8) 1.79(.662-4.86) .245
Hypertension 63(28.3) 103(40.4) 166(34.7) 1.72(1.17-2.52) .005
Arrythmias 23(11.3) 40(15.7) 65(13.7) 1.47(.86-2.517) .155
Hypercholesterolemia 49(21.9) 81(31.8) 130(27.1) 1.66(1.10-2.51) .015
Diabetes 55(24.6) 87(34.3) 142(29.7) 1.60(1.07-2.38) .021
Urinary Tract
Infections
17(7.6) 16(6.3) 33(6.9) .815(.40-1.65) .571
Skin diseases 22(9.8) 40(15.7) 62(12.9) 1.70(.98-2.97) .056
Chronic anxiety 21(9.4) 25(9.8) 46(9.6) 1.05(.57-1.94) .863
Depression 30(13.5) 50(19.7) 80(16.8) 1.57(.96-2.58) .069
Arthritis 23(10.3) 24(9.4) 47(9.8) .91(.49-1.65) .753
Hemorrhoids 18(8.1) 29(11.4) 47(9.8) 1.46(.79-2.71) .227
Varicose veins 18(6.8) 25(9.9) 40(8.4) 1.51(.77-2.94) .221
40
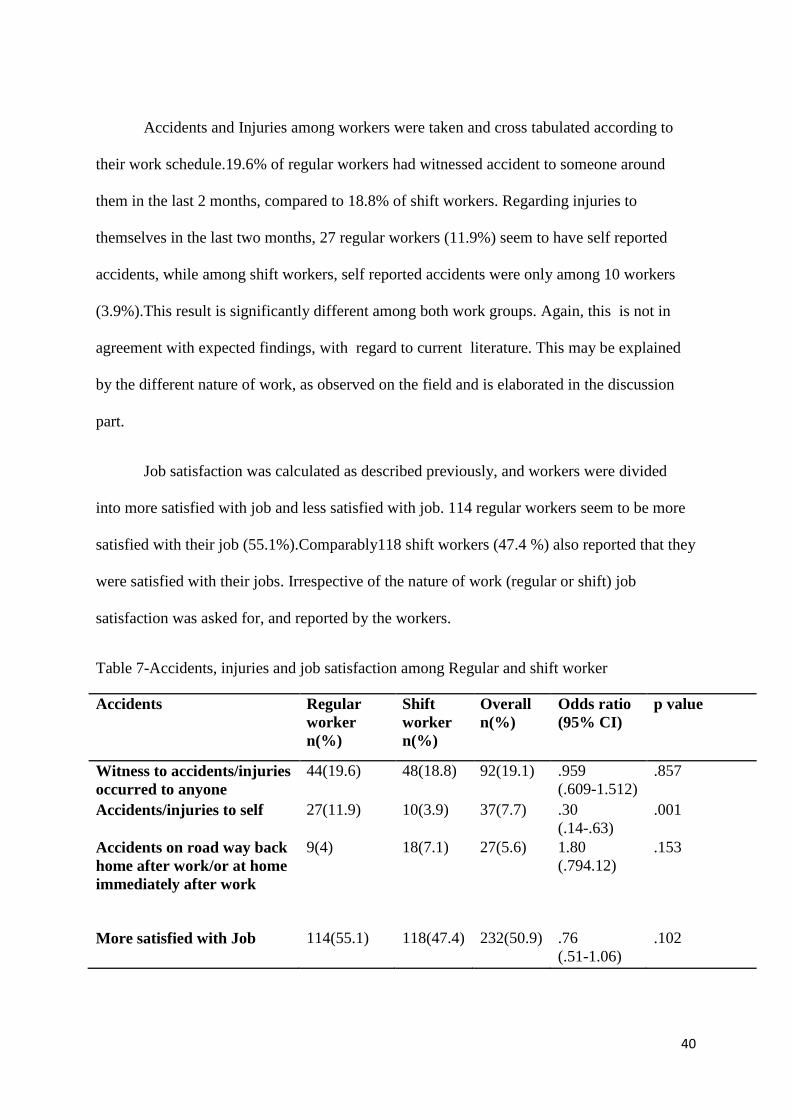
Accidents and Injuries among workers were taken and cross tabulated according to
their work schedule.19.6% of regular workers had witnessed accident to someone around
them in the last 2 months, compared to 18.8% of shift workers. Regarding injuries to
themselves in the last two months, 27 regular workers (11.9%) seem to have self reported
accidents, while among shift workers, self reported accidents were only among 10 workers
(3.9%).This result is significantly different among both work groups. Again, this is not in
agreement with expected findings, with regard to current literature. This may be explained
by the different nature of work, as observed on the field and is elaborated in the discussion
part.
Job satisfaction was calculated as described previously, and workers were divided
into more satisfied with job and less satisfied with job. 114 regular workers seem to be more
satisfied with their job (55.1%).Comparably118 shift workers (47.4 %) also reported that they
were satisfied with their jobs. Irrespective of the nature of work (regular or shift) job
satisfaction was asked for, and reported by the workers.
Table 7-Accidents, injuries and job satisfaction among Regular and shift worker
Accidents Regular
worker
n(%)
Shift
worker
n(%)
Overall
n(%)
Odds ratio
(95% CI)
p value
Witness to accidents/injuries
occurred to anyone
44(19.6) 48(18.8) 92(19.1) .959
(.609-1.512)
.857
Accidents/injuries to self 27(11.9) 10(3.9) 37(7.7) .30
(.14-.63)
.001
Accidents on road way back
home after work/or at home
immediately after work
9(4) 18(7.1) 27(5.6) 1.80
(.794.12)
.153
More satisfied with Job 114(55.1) 118(47.4) 232(50.9) .76
(.51-1.06)
.102

41
The social and domestic life of the workers was assessed using the social and
domestic survey. The overall satisfaction score is not found to be significantly different
between the two groups of workers. As expected more shift workers reported more
satisfaction in finding time for domestic tasks, such as helping at home or looking after
children. They also found more time for their Non domestic activities such as going to bank,
hairdresser etc. Both these were significantly different between the two groups. Being
negatively coded, these had to be interpreted conversely-103 regular workers (56.9 %)
reported lesser time for domestic things, while 111 shift workers (45.7%) reported the same
problem. Again 86 regular workers reported that their work schedule interfered with non
domestic tasks (60.1%), while only 86 of their shift work counterparts (39%) reported the
same problem.
Table 8-Social and domestic situation among regular and shift worker.
Social and Domestic
situations (number of
respondents)
Regular
worker
n(%)
Shift
worker
n(%)
Overall
n(%)
Odds ratio
(95% CI)
p value
More satisfied with time
for Social and domestic
activities (301)
84(57.1) 80(51.9) 164(54.5) .88(.56-1.28) .366
Lesser time for
activities one like to do
( sports, hobbies..) (450)
94(47.7) 137(54.2) 231(51.3) 1.29(.89-1.88) .175
Lesser time for
domestic things(tasks,
children)(424)
103(56.9) 111(45.7) 214(50.5) .637(.432-.938) .022
Interfere with non
domestic activities (371)
86(60.1) 89(39) 175(47.2) .424(.277-1.56) <0.001
4.3.2. Associations of Insomnia or Excessive sleepiness, against various factors :Insomnia or
Excessive sleepiness was cross tabulated against various factors to look for its associations.
Age, years in service, body mass index, marital status, work schedule, Smoking, use of
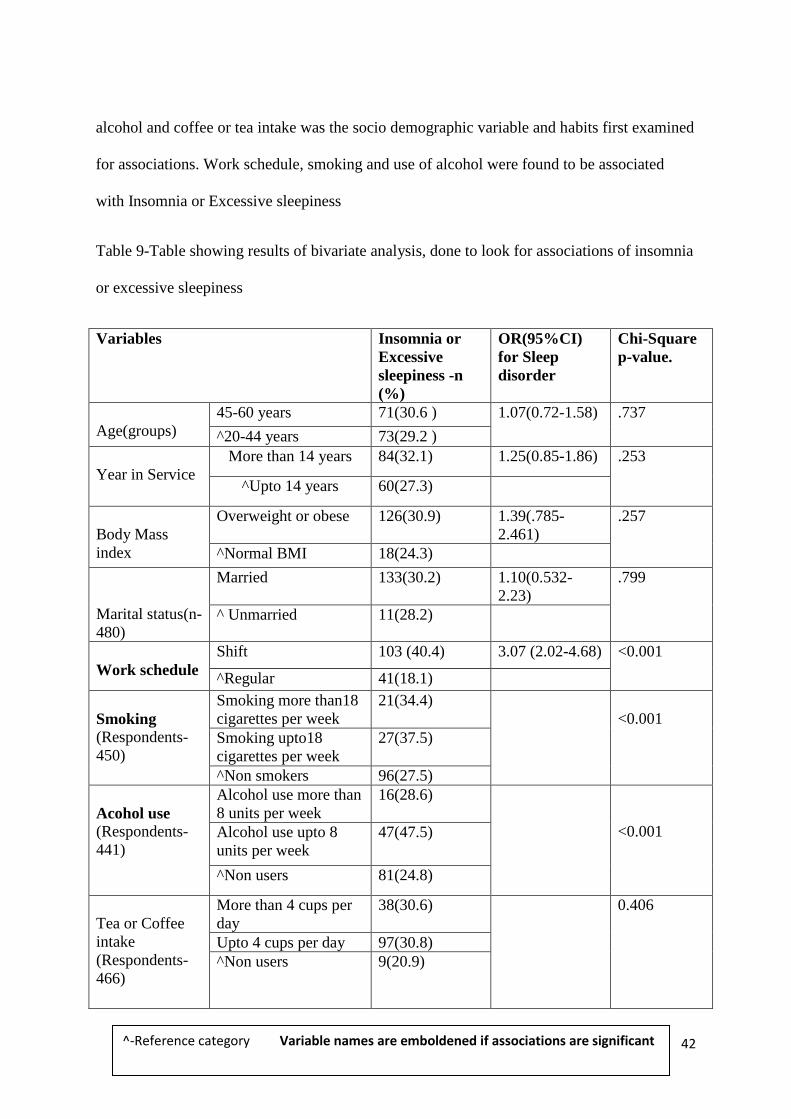
42
alcohol and coffee or tea intake was the socio demographic variable and habits first examined
for associations. Work schedule, smoking and use of alcohol were found to be associated
with Insomnia or Excessive sleepiness
Table 9-Table showing results of bivariate analysis, done to look for associations of insomnia
or excessive sleepiness
Variables Insomnia or
Excessive
sleepiness -n
(%)
OR(95%CI)
for Sleep
disorder
Chi-Square
p-value.
Age(groups)
45-60 years 71(30.6 ) 1.07(0.72-1.58) .737
^20-44 years 73(29.2 )
Year in Service
More than 14 years 84(32.1) 1.25(0.85-1.86) .253
^Upto 14 years 60(27.3)
Body Mass
index
Overweight or obese 126(30.9) 1.39(.785-
2.461)
.257
^Normal BMI 18(24.3)
Marital status(n-
480)
Married
133(30.2) 1.10(0.532-
2.23)
.799
^ Unmarried 11(28.2)
Work schedule
Shift 103 (40.4) 3.07 (2.02-4.68) <0.001
^Regular 41(18.1)
Smoking
(Respondents-
450)
Smoking more than18
cigarettes per week
21(34.4)
<0.001
Smoking upto18
cigarettes per week
27(37.5)
^Non smokers 96(27.5)
Acohol use
(Respondents-
441)
Alcohol use more than
8 units per week
16(28.6)
<0.001 Alcohol use upto 8
units per week
47(47.5)
^Non users 81(24.8)
Tea or Coffee
intake
(Respondents-
466)
More than 4 cups per
day
38(30.6) 0.406
Upto 4 cups per day 97(30.8)
^Non users 9(20.9)
^-Reference category Variable names are emboldened if associations are significant

43
Next, the morbidities detected as part of the survey and the self reported morbidities
were examined for possible association with insomnia or excessive sleepiness.
Gastrointestinal problems, cardiovascular problems, mental health, hypertension, diabetes,
anxiety and depression were found to be significantly associated with Insomnia or excessive
sleepiness.
Table 10-Table showing results if bivariate analysis, done to look for associations of
insomnia or excessive sleepiness
Variables Insomnia
or
Excessive
sleepiness
-n (%)
OR(95%CI)
for Sleep
disorder
Chi-Square
p-value.
Gastro
intestinal
problems
Symptoms suggestive 78 (39.2) 2.07 (1.36-3.17) 0.001
^No symptoms suggestive 51(23.7)
Cardiovascular
problems
Symptoms suggestive 77 (38.7) 2.43 (1.57-3.74) <0.001
^No symptoms suggestive 46 (20.6)
Mental
health
Better mental health 49(22.5) .451(.296-.686)
<0.001 ^Poorer mental health 83(39.2)
Blood Pressure(self
reported)
Hypertensive 64(38.6) 1.85 (1.24-2.77) 0.003
^Non Hypertensive 79 (25.3)
Diabetes(self
reported)
Diabetic 55(38.7) 1.78 (1.18-2.70) 0.006
^Non-diabetic 88(26.2)
Anxiety(self
reported)
Anxiety 20 (43.5) 1.93 (1.04-3.59) 0.035
^No Anxiety disorder 123(28.5)
Depression (self reported)
Depressed
38 (47.5)
2.52 (1.54-4.12) 0.001
^No Clinical Depression
105(26.4)
^-Reference category Variable names are emboldened if associations are significant
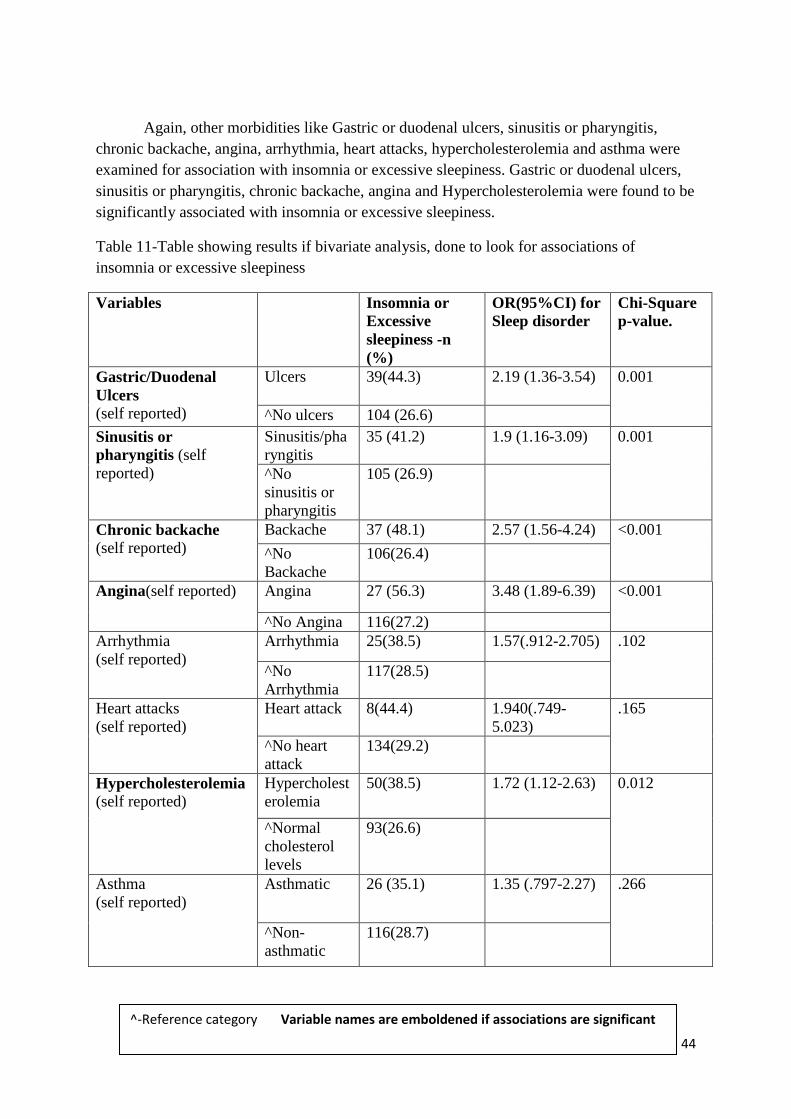
44
Again, other morbidities like Gastric or duodenal ulcers, sinusitis or pharyngitis,
chronic backache, angina, arrhythmia, heart attacks, hypercholesterolemia and asthma were
examined for association with insomnia or excessive sleepiness. Gastric or duodenal ulcers,
sinusitis or pharyngitis, chronic backache, angina and Hypercholesterolemia were found to be
significantly associated with insomnia or excessive sleepiness.
Table 11-Table showing results if bivariate analysis, done to look for associations of
insomnia or excessive sleepiness
Variables Insomnia or
Excessive
sleepiness -n
(%)
OR(95%CI) for
Sleep disorder
Chi-Square
p-value.
Gastric/Duodenal
Ulcers (self reported)
Ulcers 39(44.3) 2.19 (1.36-3.54) 0.001
^No ulcers 104 (26.6)
Sinusitis or
pharyngitis (self
reported)
Sinusitis/pha
ryngitis
35 (41.2) 1.9 (1.16-3.09) 0.001
^No
sinusitis or
pharyngitis
105 (26.9)
Chronic backache (self reported)
Backache 37 (48.1) 2.57 (1.56-4.24) <0.001
^No
Backache
106(26.4)
Angina(self reported) Angina 27 (56.3) 3.48 (1.89-6.39) <0.001
^No Angina 116(27.2)
Arrhythmia
(self reported)
Arrhythmia 25(38.5) 1.57(.912-2.705) .102
^No
Arrhythmia
117(28.5)
Heart attacks
(self reported)
Heart attack 8(44.4) 1.940(.749-
5.023)
.165
^No heart
attack
134(29.2)
Hypercholesterolemia (self reported)
Hypercholest
erolemia
50(38.5) 1.72 (1.12-2.63) 0.012
^Normal
cholesterol
levels
93(26.6)
Asthma
(self reported)
Asthmatic 26 (35.1) 1.35 (.797-2.27) .266
^Non-
asthmatic
116(28.7)
^-Reference category Variable names are emboldened if associations are significant

45
Finally, social and domestic life variable was also looked for associations. Overall
time available or socio domestic life, and the interference of work schedule on hobbies,
domestic activities and also for non domestic activities were looked for associations with
insomnia or excessive sleepiness. None were found to have significant correlations with
Insomnia or excessive sleepiness.
Table 12-Table showing results if bivariate analysis, done to look for associations of
insomnia or excessive sleepiness
Variables Insomnia or
Excessive
sleepiness -n
(%)
OR(95%CI) for
Sleep disorder
Chi-Square
p-value.
Time available
for socio
domestic life
(Overall)
Better socio
domestic life
49(29.9) 1.24(.746-2.06) .404
^Poorer socio
domestic life
35(25.5)
Work schedule
Interference with
Hobbies
Interfered 73(31.6) 1.00(.675-1.49) .983
^No
interference
69(31.5)
Work schedule
Interference with
domestic activities
Interfered 66(30.8) .873(.581-1.31) .513
^No
interference
71(33.8)
Work schedule
Interference with
other non domestic
activities
Interfered 59(33.7) 1.03(.665-1.58) .911
^No
interference
65(33.2)
^-Reference category Variable names are emboldened if associations are significant
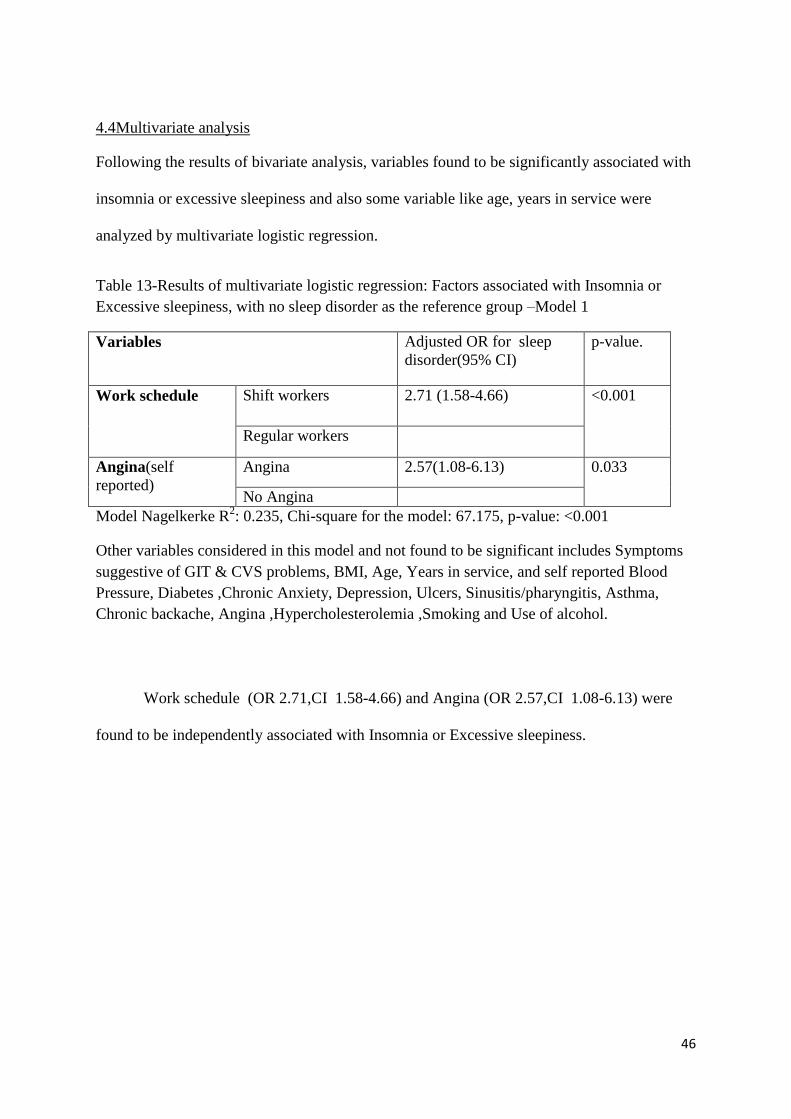
46
4.4Multivariate analysis
Following the results of bivariate analysis, variables found to be significantly associated with
insomnia or excessive sleepiness and also some variable like age, years in service were
analyzed by multivariate logistic regression.
Table 13-Results of multivariate logistic regression: Factors associated with Insomnia or
Excessive sleepiness, with no sleep disorder as the reference group –Model 1
Variables Adjusted OR for sleep
disorder(95% CI)
p-value.
Work schedule Shift workers 2.71 (1.58-4.66) <0.001
Regular workers
Angina(self
reported)
Angina 2.57(1.08-6.13) 0.033
No Angina
Model Nagelkerke R2: 0.235, Chi-square for the model: 67.175, p-value: <0.001
Other variables considered in this model and not found to be significant includes Symptoms
suggestive of GIT & CVS problems, BMI, Age, Years in service, and self reported Blood
Pressure, Diabetes ,Chronic Anxiety, Depression, Ulcers, Sinusitis/pharyngitis, Asthma,
Chronic backache, Angina ,Hypercholesterolemia ,Smoking and Use of alcohol.
Work schedule (OR 2.71,CI 1.58-4.66) and Angina (OR 2.57,CI 1.08-6.13) were
found to be independently associated with Insomnia or Excessive sleepiness.

47
Further, different models were explored for shift workers and regular workers.
For Regular workers, Symptoms suggestive of cardio vascular diseases was found to
have an independent association with insomnia or excessive sleepiness.
Table 14-Results of multivariate logistic regression among regular workers only: Factors
associated with Insomnia or Excessive sleepiness, with no sleep disorder as the reference
group –Model 2
Variable Adjusted OR for sleep
disorder(CI)
p value.
Symptoms suggestive
of cardiovascular
diseases
Has symptoms 3.43(2.90-5.16) 0.032
No symptoms
Model Nagelkerke R2: 0.273, Chi-square for the model: 31.769, p-value: 0.046
Other variables considered in this model and not found to be significant includes Symptoms
suggestive of GIT & CVS problems, BMI, Age, Yrs in service, and self reported Blood
Pressure, Diabetes ,Chronic Anxiety, Depression, Ulcers, Sinusitis, Asthma, Chronic
backache, Angina ,Hypercholesterolemia ,Smoking and Use of alcohol.
For Shift workers, symptoms suggestive of depression were found to have an
independent association with insomnia or excessive sleepiness.
Table 15-Results of multivariate logistic regression among shift workers only : Factors
associated with Insomnia or Excessive sleepiness, with no sleep disorder as the reference
group –Model 3
Variable Adjusted OR for sleep
disorder(CI)
p value.
Depression(self
reported
Depressed 3.62(1.45-8.995) 0.006
Not depressed
Model Nagelkerke R2: 0.215, Chi-square for the model: 34.06, p-value: 0.026
Other variables considered in this model and not found to be significant includes Symptoms
suggestive of GIT & CVS problems, BMI, Age, Yrs in service, and self reported Blood
Pressure, Diabetes ,Chronic Anxiety, Depression, Ulcers, Sinusitis/pharyngitis, Asthma,
Chronic backache, Angina ,Hypercholesterolemia ,Smoking and Use of alcohol.

48
4.5 Clinical tests-a bivariate analysis
This is the third set of analysis aimed to correlate the clinical findings between types
of workers.
A battery of clinical tests was done on a subsample of the workers, who had returned
the questionnaires, and also had consented to undergo clinical testing. Rey‘s Auditory Verbal
Learning, Trail A, Trail B, Digit span (forward and backward) were done on a subset of the
sample (30 regular workers and 30 shift worker) First the age and educational levels of both
groups of workers were analyzed and the difference was not found to be significantly
different (p value for age-0.508, p value across 4 categories- 0.478; Categories-masters,
degree or industrial training, passed 10th
standard, did not pass 10th
standard of educational
attainment)
Rey Auditory Verbal Learning tests (RAVLT) results were found to be significantly
different upon comparing the mean words learnt during each round of learning among the
two groups of workers.
Regarding memory,again the two groups were found to score significantly different
from each other. In Immediate recall tests, regular workers scored a mean score of 8.13+-
1.75,while the shift worker scored a mean of 5.97+-1.54.Also in delayed recall testing,
regular workers scored a mean score of 8.47+-2.417,while the shift workers scored a mean
score of 5.40+-1.45.

49
Table 16-Clinical test scores among Regular and shift worker
Regular worker(n=30) Shift worker(n=30) p values
Tests (mean+-SD) Median(IQR) (mean+-SD) Median(IQR) p value
for Mean
p value for
median
RAVLT1 6.20+-1.54 6(2) 5.43+-1.43 6(1.25) .05 .103
RAVLT2 8.83+-1.70 9(2.25) 7.40+-1.63 7(1.25) .002 .002
RAVLT3 10.40+-1.71 10(3) 8.80+-1.84 9(2) .001 .002
RAVLT4 11.71+-1.88 11.50(3.25) 10.17+-2.18 10(4) .004 .008
RAVLT5 12.87+-1.75 13(3.25) 11.13+-2.18 11(4.25) .003 .005
Immediate
recall
8.13+-1.75 8(2) 5.97+-1.54 6(2) <0.001 <0.001
Delayed
Recall
8.47+-2.417 8(3) 5.40+-1.45 5(2) <0.001 <0.001
Repeated measures anova test was done to see if learning across each round of
RAVLT (5 rounds) were significantly different among the work groups. It is seen that the
two groups are significantly different and the RAVLT scores in each round are also
significantly different. But the learning curve may not be significantly different.
Also it was checked if RAVLT was different across work schedule with insomnia or
excessive sleepiness adjusted using multiple factor repeated measures anova. It appears that
RAVLT scores across each round is significantly different across work groups even when
irrespective of insomnia or excessive sleepiness.
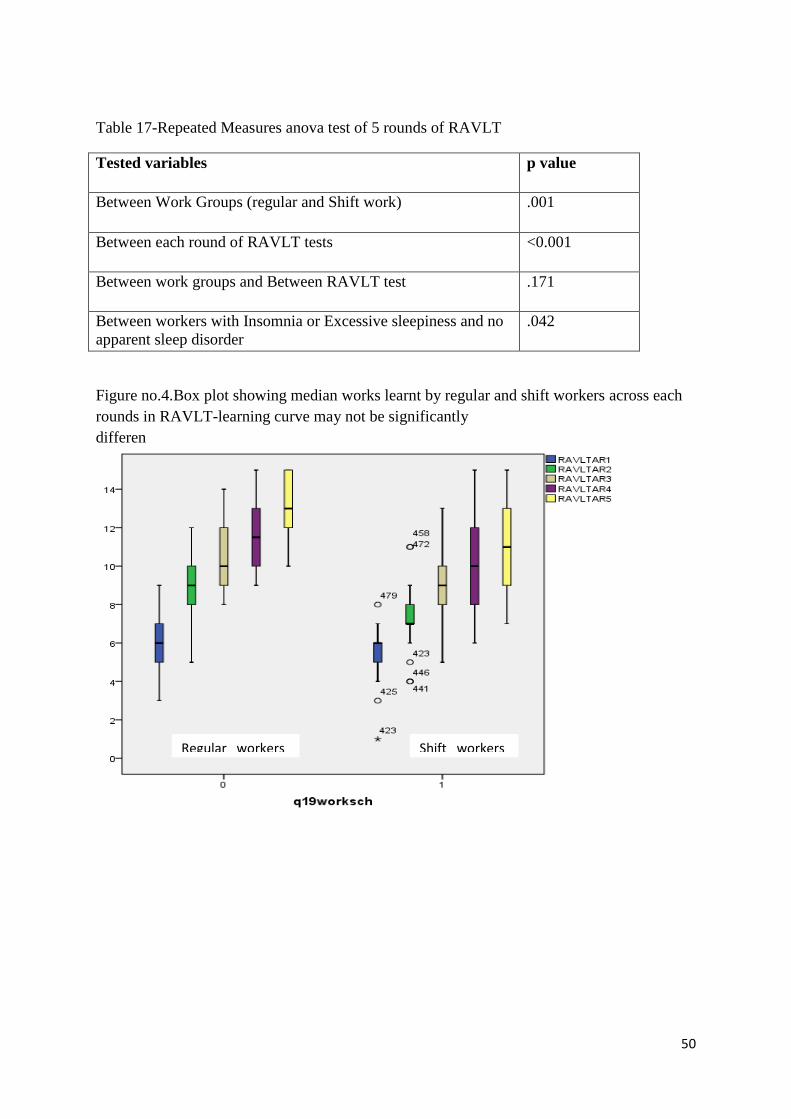
50
Table 17-Repeated Measures anova test of 5 rounds of RAVLT
Tested variables p value
Between Work Groups (regular and Shift work) .001
Between each round of RAVLT tests <0.001
Between work groups and Between RAVLT test
.171
Between workers with Insomnia or Excessive sleepiness and no
apparent sleep disorder
.042
Figure no.4.Box plot showing median works learnt by regular and shift workers across each
rounds in RAVLT-learning curve may not be significantly
differen
Regular workers Shift workers

51
Also, other tests such as trail A, Trail B, Digits pan forward and backward were done
on the two sets of workers. The results of these tests were not found to be significantly
different.
Table 18-Clinical test scores among Regular and shift worker
Tests Regular worker(n=30) Shift worker(n=30)
(mean+-SD) Median
(IQR)
(mean+-SD) Median
(IQR)
p value
For mean
p value
For median
Trail A 89.23+-
31.278
84(45) 91.90+-28.11 81(35.5) .730 .615
Trail B
185.07+-
54.32
179(73.3) 190.27+-
73.08
174(61)
.756 .935
Digit span
Forward
5.70+-1.31 6(1) 5.43+-1.61 5(2) .486 .425
Digit span
Backward
4.47+-1.35 4.5(1.5) 4.27+-1.43 4(1) .358 .517
Digit span
Total
10.23+-23 10(3) 9.69+-2.40 9(1.25) .310 .291
52
CHAPTER 5-DISCUSSION AND CONCLUSIONS
5.1. Discussion
The problems of working in shifts and it correlations with sleep are discussed first.
Secondly work schedule and its correlation with health, accidents and socio domestic life of
workers are discussed. Next, insomnia or excessive sleepiness and its correlates are
discussed. Finally the results of clinical tests are discussed.
5.1.1 Relation with sleep-Prevalence of insomnia or Excessive sleepiness
The prevalence of Insomnia, Excessive sleepiness and a combination of both is
significantly higher in the shift working group. This duly conforms to the available evidence
linking shift work and sleep disorders.14,17
When adjusted to age , according to the new World Health Organisation-2000-2005
standard population, the prevalence of shift work sleep disorder(insomnia or excessive
sleepiness) among this population is 30.74%. Similarly The prevalence of insomnia or
excessive sleepiness among regular workers is 26.14%.This rate is higher than what was
found by a similar study done by Drake and colleagues in Detroit, USA, and by Garbarino S
and colleagues among Italian policemen.14,19
This prevalence is however lower than what was found in several other studies in by
Hrma M and colleagues in Helsinki, Santos EH and and collegues in Brazil,and in a study by
Gold DR among hospital nurses.17,18,20
This is also lower than the estimate of sleep disorders
as estimated by the National sleep foundation Sleep in America poll.22
This difference of prevalence may be due to the various factors. The work
environment is tiring in Indian settings. Informally the workers may be taking rest or maybe

53
even naps in free hours. Also due to the reason that this is a survey conducted at workplaces,
it may have been under reported.
5.1.2. Shift work and other co morbidities
Working in shift was significantly associated with having symptoms of
gastrointestinal and also cardiovascular diseases.
It was seen than shift workers were about 1.52(1.03-2.24) times more likely to be
associated with symptoms of gastrointestinal diseases. They were also 2.3(1.55-3.4) times
more likely to be associated with symptoms of cardiovascular diseases. This is in
concordance with available literature in Japan, Italy and Helsinki which looked at
associations of shift work.54, 55,56,61,65
Stomach ulcers were seen to more than those reported abroad, but had a significantly
higher prevalence among the shift workers, as evidenced in Japan.57,58
.Similarly
Hypercholesterolemia and diabetes were seen to been more prevalent among shift workers,
which is in accordance with earlier research.59,60
Angina and hypertension are also found to
be significantly higher in the shift work group and is in agreement with available knowledge
regarding shift work.64,65
Sinusitis or pharyngitis is also found to be significantly associated
with shift work
Accidents and injuries looked for among the two groups suggest a rather uncommon
finding. In contrast to available literature ,in this population regular workers(11.9%) had
more accidents than their shift workmates(3.9%).4,14,67,68,69,70
This is explainable, considering
the work environment which drastically differs in the chemical plant where this study was
undertaken. Shift workers are mostly plant workers and run the automated chemical plant,

54
while regular workers are mostly maintenance workers, who repair and fix machinery.
Therefore regular workers probably have more occupational risks of accidents.
Next the socio domestic situations of the workers were looked into. 56.9 % of regular
workers reported lesser time for domestic things, while only 45.7% of shift workers reported
the same problem. Again 60.1% regular workers reported that their work schedule interfered
with non domestic tasks, while only 39 %of their shift work counterparts reported the same
problem. This is different from other published studies, which state poorer quality of life
among shift worlers.14
I t seems to suggest that shift workers in this population are at an
advantage here, being able to find time for domestic and other non domestic activities while
managing their works shift together
Regarding cognition and executive function, learning or attention here was not found
to be affected as found previously in other settings.74,75
.But memory, as tested by verbally
learnt words were found to be impaired both in the short term and long term.
5.1.3 Insomnia or Excessive sleepiness, and its correlates.
3 models were attempted to find out independent associations for insomnia or
excessive sleepiness-
1) A general model for all workers. 2) Model for regular workers. 3) Model for shift
workers. These models were built using by multivariate logistic regression by entry method,
using all variable which were found significant during bivariate analysis. Extra correlates
which were included were, age and years in service. Work schedule was duly excluded for
models two and three.

55
In general, Work schedule (OR 2.71,CI 1.58-4.66) and Angina (OR 2.57,CI 1.08-
6.13) were found to be independently associated with Insomnia or Excessive sleepiness
(model 1)
Among regular workers, symptoms suggestive of cardio vascular diseases were found
to have an independent association with insomnia or excessive sleepiness. Regular workers
with symptoms of cardiovascular disease were 3.43(OR 2.90-5.16) times more likely to be
associated with insomnia or excessive sleepiness.
Among shift workers, symptoms suggestive of cardio vascular diseases were found to
have an independent association with insomnia or excessive sleepiness. Shift workers with
depression were 3.62(OR 1.45-8.995) times more likely to be associated with insomnia or
excessive sleepiness.
5.1.4. Clinical tests done
30 regular workers and 30 shift workers were administered Rey Auditory Verbal
Learning, Trail A, Trail B, Digit span (forward and backward) .First the age and educational
levels of both groups of workers were analyzed and the difference was not found to be
significantly different.
Rey‘s Auditory Verbal Learning tests results were found to be significantly different
upon comparing the mean words learnt during each round of learning among the two groups
of workers.
While testing for Immediate and delayed recall, the two groups were found to score
significantly different from each other. In Immediate recall tests, regular workers scored a
mean score of 8.13+-1.75,while the shift worker scored a mean of 5.97+-1.54(p

56
value<0.001).Also in delayed recall testing, regular workers scored a mean score of 8.47+-
2.417,while the shift workers scored a mean score of 5.40+-1.45(p value-<0.001).
RAVLT measures were taken as progressive learning outcomes and analyzed.
Repeated measures anova test was done to see if learning across each round of RAVLT (5
rounds) were significantly different among the work groups. It is seen that the two groups are
significantly different and the RAVLT scores in each round are also significantly different.
But the learning curve was not found to be significantly different. This seems to suggest that
memory may be affected, while learning abilities may be spared. This has implications in the
personal and professional life of workers. More evidence needs to be collected as only verbal
learning was tested here.
Repeated measures anova test was against 2 factors done to check if RAVLT was
different across work schedule irrespective of insomnia or excessive sleepiness, as captured
by the study. It appears that RAVLT scores across each round is significantly different across
work groups even when adjusted for with insomnia or excessive sleepiness. This indicates
that irrespective of insomnia or excessive sleepiness, shift work seems to have an impact on
RAVLT scores. This requires further exploration and research.
Trail A, Trail B tests were done on the two sets of workers. These were done to look
for visual attention and task switching. The results of these tests were not found to be
significantly different.
Digit span forward and backward tests were used to check for short term memory.
These results were also were not found to be significantly different between the two work
groups.
57
5.2. Strengths and Limitations of the study.
• Strengths
– Among the early studies to look at effects of shift work especially among
industrial workers.
– Among the emerging studies in India looking at the nascent field of sleep
epidemiology.
– Collaborative effort between industrial health workers , public Health & Sleep
specialist(neurologist) to look at a occupational health problem, which has
public health implications.
– The study was designed and carried out in response to a Clinical observation
by a vigilant Occupational health specialist.
• Limitations
– Cross sectional study with all its inherent weaknesses. No causality can be
ascribed to associations.
– Morbidity variables were self reported, some of them could have been
measured in field with more resources.
58
5.3. Conclusions
Summarily, shift work seems to have a significant impact on health of workers.
It is seen to be associated with sleep disorders like Insomnia or Excessive Sleepiness,
or both. Regarding Insomnia or excessive sleepiness (shift work sleep disorder in the shift
working group as per definition), it seems to be significantly associated with work schedule
and also having angina, after having been adjusted for potential correlates and co morbidities.
Conclusively, working in shifts seems to be associated with sleep disorders.
Shift work is also associated with general health of the workers. Shift workers have
significantly more problems like ulcers, sinusitis, angina, hypertension, hypercholesterolemia
seen among them. Symptoms suggestive of gastro intestinal and cardiovascular problems are
also more among the shift workers. It seems to affect the memory (both immediate and
delayed) among workers, as suggested by clinical tests.
Interestingly in their Personal lives, more shift workers seem to find time for domestic
activities and non domestic personal matters, than their regular work mates.
More resources and research need to be directed in order to capture finer nuances of
the health problems of shift work. Screening for various disorders which have significant
associations with shift work needs to be considered as a policy outcome among industrial
workers.

59
References
1. The International Classification of Sleep Disorders: Diagnostic and Coding Manual,
Revised. Westchester: American Academy of Sleep Medicine; 2001
2. Brandon S. L,Phyllis CZ.Circadian Rhythm Sleep Disorders.Chest 2006;130:1915-1923
3. Akerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med 2003;53:89–94.
4. Akerstedt T. Sleepiness as a consequence of shiftwork. Sleep 1988;11:17–34.
5.Perrucci R. The Significance of Shift Work: Current Status and Future Directions.J Fam
Econ Iss 2007;28:600–617.
6. APA. Diagnostic and statistical manual of mental disorders. 4th edition. Washington:
American Psychiatric Association; 2000.
7. Boisard P,Cartron , Gollac M & Valeyre A. Time and work: Duration of work 2003
Dublin,Ireland: European Foundation for the Improvement of Living and Working
Conditions.
8. Beers T M.Flexible schedules and shift work: replacing the '9 - 5' workday.
Monthly Labor Review 2000;June:33-40.
9. Costa G. The 24-hour society: Between myth and reality. Journal of Human
Ergology 2001; 30:15-20.
10. Rajaratnam SM & Arendt J. Health in a 24-h society. Lancet 2001;358:999-1005.
11. Schwartz JRL, Roth T. Shift work sleep disorder: Burden of illness and approaches to
management. Drugs 2006;66:2357-2370

60
12. Rosa RR, Colligan MJ.Plain language about shift work 1997:DHHS (NIOSH) Publication
No. 97-145
13. Coleman RM. The 24-Hour Business. New York: 1995. American Management
Association
14. Drake CL, Roehrs T, Richardson G, et al. Shift work sleep disorder: prevalence and
consequences beyond that of symptomatic day workers. Sleep. 2004;27:1453-1462.
15. Sack RL, Auckley D, Auger R, et al. Circadian rhythm sleep disorders: part I, basic
principles, shift work and jet lag disorders. Sleep 2007;30: 1460-1483.
16. Rajaratnam SM, Barger LK, Lockley SW.Screening for sleep disorders in North
American police officers [abstract]. Sleep 2007;30(suppl):A209.
17. Harma M, Tenkanen L, Sjoblom T. Combined effects of shift work and life-style on the
prevalence of insomnia, sleep deprivation and daytime sleepiness. Scand J Work Environ
Health 1998;24:300-307.
18. Santos EH, de Mello MT, Pradella-Hallinan M. Sleep and sleepiness among Brazilian
shift-working bus drivers. Chronobiol Int 2004;21:881-888.
19.Garbarino S, De Carli F, Nobili L. Sleepiness and sleep disorders in shift workers: a study
on a group of Italian police officers. Sleep 2002;25:648-653.
20.Gold DR, Rogacz S, Bock N. Rotating shift work, sleep, and accidents related to
sleepiness in hospital nurses. Am J Public Health 1992;82: 1011-1014.
21.Axelsson J, Åkerstedt T, Kecklund G.Tolerance to shift work: how does it relate to sleep
and wakefullness? Int Arch Occup Environ Health 2004;77:121–9.

61
22. Culpepper L. The social and economic burden of shift-work disorder Supplement to the
Journal of Family practice.January 2010 / Vol 59
23. US Census Bureau, International Data Base, 2004.
24.The Chattanoogan.com. Dr. Anuj Chandra To Offer Workshops On Sleep Awareness
posted January 3, 2011.http://www.chattanoogan.com/articles/article_191507.asp(accessed
24 Feb 2011)
25. Vijayan VK, Patial K.Prevalence of obstructive sleep apnea syndrome (OSAS) in delhi,
india . Chest 2006 130: 92S-c
26.Chokroverty S.Overview of sleep and sleep disorders Indian J Med Res 2010;131 : 126-
40.
27. Martinez D,Lenz MCS.Circadian rhythm sleep disorders.Indian J Med Res 2010;131:141-
9.
28. Sharma SS. Wake-up call for sleep disorders in developing nations. Indian J Med Res;
February 2010;131:115-118
29. Annual survey of industries report press note.Jan14,2011.
http://mospi.nic.in/Mospi_New/upload/press_note_ASI_14jan10.pdf.(accessed 3Mar2011.)
30.Moore RY. Circadian rhythms: basic neurobiology and clinical applications.Annu Rev
Med 1997;48:253-266.
31. Drake CL.The characterization and pathology of circadian rhythm sleep
disorders.Supplement to the journal of family practice 2010;Vol 59:13-16.

62
32.Katzenberg D, Young T, Finn L, et al. A CLOCK polymorphism associated with human
diurnal preference. Sleep 1998;21:569-576.
33. Borbély AA, Achermann P. Concepts and models of sleep regulation: an overview. J
Sleep Res 1992;1:63-79.
34. Park YM, Matsumoto PK, Seo YJ, et al. Sleep-wake behavior of shift workers using wrist
actigraph. Psychiatry Clin Neurosci 2000;54:359-360.
35. Reinberg A, Ashkenazi I. Internal desynchronization of circadian rhythms and tolerance
to shift work. Chronobiol Int 2008;25:625-643.
36. Quera-Salva MA, Defrance R, Claustrat B, et al. Rapid shift in sleep time and acrophase
of melatonin secretion in short shift work schedule.Sleep 1996;19:539-543.
37.Thorpy MJ,Managing the patient with shift-work disorder ;Supplement to the Journal of
Family practice.January 2010 / Vol 59:24-30
38.Crowley SJ, Lee C, Tseng CY, et al. Complete or partial circadian re-entrainment
improves performance, alertness, and mood during night-shift work. Sleep 2004;27:1077-
1087
39.Eastman CI, Stewart KT, Mahoney MP, et al. Dark goggles and bright light improve
circadian rhythm adaptation to night-shift work. Sleep 1994;17:535-543.
40. Crowley SJ, Lee C, Tseng CY, et al. Combinations Of bright light, scheduled dark,
sunglasses, and melatonin to facilitate circadian entrainment to night shift work. J Biol
Rhythms 2003;18:513-523

63
41.Erman MK, Rosenberg R, for the US Modafinil Shift Work Sleep Disorder Study Group.
Modafinil for excessive sleepiness associated with chronic shift work disorder: effects on
patient functioning and health-related quality of life. Prim Care Companion. J Clin
Psychiatry 2007;9:188-194.
42. Drake C, Walsh J, Roth T. Armodafinil improves sleep latency in patients with shift
work disorder. Sleep 2006;29(suppl):A64.
43.Roth T, Czeisler CA, Walsh JK, et al. Randomized, double-blind, placebo-controlled
study of armodafinil for the treatment of excessive sleepiness associated with chronic shift
work disorder [abstract 161]. Neuropsychopharmacology 2005;30:S140.
44. Muehlbach MJ, Walsh JK. The effects of caffeine on simulated night-shift work and
subsequent daytime sleep. Sleep 1995;18:22-29.
45.Walsh JK, Muehlbach MJ, Humm TM, et al. Effect of caffeine on physiological sleep
tendency and ability to sustain wakefulness at night. Psychopharmacology 1990;101:271-
273.
46.Hart CL, Haney M, Nasser J, et al. Combined effects of methamphetamine and zolpidem
on performance and mood during simulated night shift work. Pharmacol Biochem
Behav2005;81:559-568.
47.Darke S, Kaye S, McKetin R, et al. Major physical and psychological harms of
methamphetamine use. Drug Alcohol Rev 2008;27:253-262.
48.Hughes RJ, Badia P. Sleep-promoting and hypothermic effects of daytime melatonin
administration in humans. Sleep 1997;20:124-131.

64
49. Boggild H, Knutsson A. Shift work, risk factors and cardiovascular disease. Scandinavian
Journal of Work, Environment & Health 1999; 25: 85-99.
50. Knutsson, A. Shift work and coronary heart disease. Scandinavian Journal of Social
Medicine Supplementum1989;44:1-36.
51. Knutsson, A, Boggild, H. Shiftwork and cardiovascular disease: review of disease
mechanisms. Reviews on Environmental Health 2000;15:359-372.
52. Lac G,ChamouxA. Biological and psychological responses to two rapid shiftwork
schedules. Ergonomics 2004; 47:1339-1349.
53. Parkes KR. Shift work and age as interactive predictors of body mass index
amongoffshore workers. Scandinavian Journal of Work, Environment & Health 2002; 28: 64-
71.
54. Costa G. The impact of shift and night work on health. Applied Ergonomics 1996;27:9-
16.
55. Parkes KR. Shiftwork, job type, and the work environment as joint predictors of health
outcomes. Journal of Occupational Health Psychology 1999;4:256-268.
56.Costa G,Sartori S,Facco P,Apostoli, P. Health conditions of bus drivers in a 6 year follow
up study. Journal of Human Ergology 2001;30:405-410.
57. Knutsson A. Health disorders of shift workers. Occupational Medicine 2003;53:103-108
58. Segawa K,Nakazawa S,Tsukamoto Y,Kurita Y,Goto H. Peptic ulcer is prevalent among
shift workers. Digestive Diseases and Sciences1987;32: 449-453.

65
59.Biggi N, Consonni D, Galluzzo V. Metabolic syndrome in permanent night workers.
Chronobiol Int 2008;25:443-454.
60. Nagaya T, Yoshida H, Takahashi H, et al. Markers of insulin resistance in day and shift
workers aged 30-59 years. Int Arch Occup Environ Health 2002;75:562-568
61. Boggild H,Knutsson A. Shift work, risk factors and cardiovascular disease. Scandinavian
Journal of Work, Environment & Health 1999; 25: 85-99
62.Yamasaki F, Schwartz JE, Gerber LM, et al. Impact of shift work and race/ethnicity on the
diurnal rhythm of blood pressure and catecholamines.Hypertension 1998;32:417-423.
63. Birkenhager AM, van den Meiracker AH. Causes and consequences of a non-dipping
blood pressure profile. Neth J Med 2007;65:127-131.
64. Thurnheer R. Obstructive sleep apnea and cardiovascular disease—time to act! Swiss
Med Wkly. 2007;137:217-222.
65. Tenkanen L,Sjoblom T,Kalimo R,Alikoski T, Harma M. Shift work, occupation and
coronary heart disease over 6 years of follow-up in the Helsinki Heart Study. Scandinavian
Journal of Work, Environment and Health 1997;23:257-265
66. Puca FM, Perrucci S, Prudenzano MP, et al. Quality of life in shift work syndrome. Funct
Neurol 1996;11:261–268.
67. Ohayon MM, Lemoine P, Arnaud-Briant V, et al. Prevalence and consequences of sleep
disorders in a shift worker population. J Psychosom Res 2002;53:577–583.
68.Ayas NT, Barger LK, Cade BE, et al. Extended work duration and the risk of self-reported
percutaneous injuries in interns. JAMA 2006;296:1055–1062

66
69.Akerstedt T, Peters B, Anund A, et al. Impaired alertness and performance driving home
from the night shift: a driving simulator study. J Sleep Res 2005;14:14–20.
70.Steele MT, Ma OJ, Watson WA, et al. The occupational risk of motor vehicle collisions
for emergency medicine residents. Acad Emerg Med 1999;6:1050–1053.
71. Price W, Holley DC. The last minutes of flight 2860: an analysis of crew shift work
scheduling. In: Reinberg A, Vieux N, Andlauer P, eds. Night and shift work: biological and
social aspects. Oxford, UK: Pergamon Press; 1981:287–298
72. Dijk DJ, Duffy JF, Czeisler CA. Circadian and sleep/wake dependent aspects of
subjective alertness and cognitive performance. J Sleep Res 1992;1:112–117.
73.Walker MP, Stickgold R. It‘s practice, with sleep, that makes perfect: implications of
sleep-dependent learning and plasticity for skill performance. Clin Sports Med 2005;24:301–
317.
74. Wright KP Jr, Hull JT, Hughes RJ, et al. Sleep and wakefulness out of phase with
internal biological time impairs learning in humans. J Cogn Neurosci 2006;18:508–521.
75. Czeisler CA. The Gordon Wilson Lecture: work hours, sleep and patient safety in
residency training. Trans Am Clin Climatol Assoc 2006;117:159–188
76. Smith L, Folkard S. The impact of shiftwork on nuclear power personnel: an exploratory
study. Work Stress 1993;7:341–350
77. Santhi N, Horowitz T, Duffy JF, et al. Acute sleep deprivation and circadian
misalignment associated with transition onto the first night of work impairs visual selective
attention. PLoS ONE. 2007;2:e1233

67
78. Harrington J M. Health effects of shift work and extended hours of work. Occup Environ
Med 2001;58:68-72.
79. IARC 2007. Press Release N°180. "IARC Monographs Program finds cancer hazards
associated with shift work, painting and firefighting.
80. Knauth P and Hornberger S.Preventive and compensatory measures for shiftworkers.
Occupational Medicine 2003 ;53:109-116.
81. Smith CS, Robie C, Folkard S, Barton J, Macdonald I, et al. A process model of
shiftwork and health. Journal of Occupational Health Psychology 1999;4207-218.
82. Rosa RR, Colligan MJ.Plain language about shift work 1997:DHHS (NIOSH) Publication
No. 97-145
83.Rey Auditory Verbal Learning Test, A Handbook. Michael Schmidt.
http://www.psychassessments.com.au/Category.aspx?GrpId=11&cID=209 (accessed 28th
january 2011).
84. Vogel A, Stokholm J, Jorgensen K. Performances on Rey Auditory Verbal LearningTest
and Rey Complex Figure Test in a healthy, elderly Danish sample - reference data and
validity issues. Scand J Psychol 2011 Aug 24. doi:0.1111/j.1467-9450.2011.00909.x. [Epub
ahead of print]
85.Lezak MD, Howieson DB, Loring DW. Neuropsychological Assessment. 4th ed. New
York: Oxford University Press; 2004.
68
86.Cambridge Brain sciences website.
http://www.cambridgebrainsciences.com/browse/memory/test/digit-span (accessed 28th
january 2011).

69
APPENDICES
Appendix A
Written informed consent form; English version
Consent form
I am Dr.Anoop Velayudhan, doing my Masters in Public Health,at the Achutha
Menon Centre for Health Science Studies (AMCHSS), Sree Chitra Tirunal Institute for
Medical Sciences and Technology, Trivandrum. As part of my research, I am conducting a
study titled ―Safety, health & social effects of shift work-a case of rapid rotating schedule
among male industrial workers‖, under the guidance of Assistant Professor Dr.Ravi Prasad
Varma.
I am studying the effect of shift work on health,safety social and personal life.I
assume that working at different periods of time and sleeping at different times each day
interrupts the body‘s internal rhythm. I intend to find out how many people have a form of
problem ,what we doctors call shift work sleep disorder,which is characterized by increased
sleepiness and lack of sleep as a result of shift work.
This study is expected to generate information regarding this problem and other
associated problems in the health and life of workers. The results of this study may act as
policy guidelines for industry and other workers.
I have prepared a sleep log,a work log and a questionnaire for you to respond to, with
assistance from me. A total of 560 persons shall be answering the same questionnaires, here
in this centre and another industry nearby.First I shall give you the sleep log to check for
changing sleep timings and collect it from you 2 weeks later.After 2 weeks,I would like you
to fill up this questionnaire and the work log for my study. This asks questions about your
personal details, your work details, your sleep details, your general health,and your social and
domestic situation.The work log is to chart out your work schedule.I shall also be testing
some of you randomly,for checking your alertness,concentration,presence of mind etc.It will
be a series of clinical,noninvasive which are some basic neurological screening tests.This will
take about 45 minutes to one hour.This will not cause any discomfort to you physically or
mentally. Please give me separate permission for this.
The whole procedure will take about 40-45 mins.You are free to withdraw from the
interview at any point of time. Also you can refuse to answer any question without giving any
explanations.
All information shall be made anonymous and recognizable by a DUMMY CODE ONLY (a
new number code that will be used to refer to you but is available with only me, stored in a
separate register maintained and accessible to me only).Your Name,employee code or any
personal information will be therefore be anonymised and know only to me. The information
obtained from you will be kept confidential, stored securely and will be used only for
research purpose. None of this information will be conveyed to the Management. Personal
details will never be revealed to the Industrial or Labour council. Only the final report of the
study will be published and made available to the industry and to also to you. This

70
information shall in no way will affect your career prospects, incentive, promotions or be
marked in your employee records or medical records.
I shall be happy to refer you to a doctor specializing in sleep medicine, a neurologist
if you happen to recognize and identify with some of the symptoms that you find here. Also
if this questionnaire suggests that you having a sleep problem, due to shift work I shall refer
you to a the sleep specialist at Sri Chitra Thirunal Centre for Science and Technology for
further management, in a discreet and confidential manner. For this I may have to access your
other medical records in total. if you are ok with this, please give me permission separately to
collect your Medical information available here in this industry in the following page.
If you have any queries or doubt, please feel free to clarify with me now.Later on, I shall be
available on phone at 9497758488. In case you need any clarifications about my credentials
or the study you can contact Dr. Ravi Prasad Varma, Assisstant Professor, AMCHSS,
SCTIMST, Thiruvananthapuram-695011 Tel: 0471-2436864 or Dr. Anoop Kumar
Thekkuveettil, Member-Secretary of the Institutional Ethical Committee at SCTIMST,
Thiruvananthapuram. Tel:0471-2348394
Signature of the Principle Investigator: ------------------
Time:
Date:
Place:
71
INFORMED CONSENT FORM
I ………………………………………………………………………………have understood
about the study,its wants and requirements.I have had an opportunity to ask questions and
clear my doubts.I am willing to participate in the study
Signature of the responder: ------------------
If you are not willing to take part thank you for your time, but could you please write down
your age and indicate your shift work patter for academic purposes?
Age………………… Shift work :
Regular day shift only
Rotating shift work.
I am willing to share your Medical records available in this institute with me(results of
monthly/yearly Medical tests, blood tests, available diagnoses etc)
Signature of the responder: ------------------
I am willing to undergo this clinical tests to check for my memory, learning, alertness, coordination
etc.I understand that it will not affect me in any way.
Signature of the responder: ------------------
Time:
Date:
Place:

72
APPENDIX B
Special Tools used in the study
1. General Job satisfaction questionnaire-question 2.7
SOURCE: Standard Shift Work Index, adapted from Hackman JR, Oldham
GR. Development of the Job Diagnostic Survey. Journal of Applied Psychology1975;
60: 159-170.This has five items and gives an overall measure of the degree to which
the employee is satisfied and happy with the job. This scale forms part of the larger
Job Diagnostic Survey (Hackman and Oldham 1975)
SCORING: A seven point response option was provided (range from disagree
strongly through disagree, disagree slightly, neutral, agree slightly, agree to agree
strongly)scored 1 to 7 with a median score being computed. Items B and E were
reversely scored.
2. Insomnia questionnaire- questions 3.13 to 3.27
Adapted from Comprehensive sleep questionnaire, Ray Mayo clinic, which
was altered in consultation with Sleep specialist and Neurologists.
3. Epworth Sleepiness Scale- question 3.28
SOURCE: The Epworth Sleepiness Scale (ESS) is a scale intended to measure
daytime sleepiness that is measured by use of a short questionnaire.
SCORING: The scores for the eight questions are added together to obtain a
single number. A number in the 0–9 range is considered to be normal while a number
in the 10–24 range indicated Excessive sleepiness

73
4. The Physical health questionnaire-Section 4 question 4.1 to 4.6
SOURCE: Standard Shift Work Index, adapted from Gianni Costa, Istituto di
Medicina del lavoro, Verona.
The physical health questionnaire contains two subscales, measuring cardiovascular and
gastrointestinal disorders, both known to have a high incidence in shift workers (8 questions
on each). A four point response option is used in order to avoid a tendency towards a central
answer. Subjects are asked to rate how frequently they experience symptoms, such as heart
palpitations and digestive difficulties. The response options are: almost never; quite seldom;
quite often; almost always.
A general screening questions was also included concerning diseases suffered
in most industrial settings. This was modified and included in consultations with
occupational health specialists. Subjects are asked to indicate on a yes/no response
option whether or not they have experienced any of the listed diseases.
SCORING: The two subscales, digestive and cardiovascular problems are
scored separately
A Likert type scale is used with response options ranging from 1 to 4, from
"almost never" to "almost always" or "definitely not" to "definitely".
5. General health questionnaire- question 4.7
SOURCE: Standard Shift Work Index, adapted from Goldberg DP. The
detection of psychiatric illness by questionnaire. 1972 Oxford: Oxford University
Press. The General Health Questionnaire is a self administered screening test for
detecting minor psychiatric disorders in the general population, and gives a single
74
measure of mental health. It covers recent levels of self-confidence, depression,
sleep loss and problem solving. Its 12 item version was chosen for the present study.
Four response options are provided for each item, e.g. better than usual, same as
usual, less than usual, much less than usual, with a higher score indicating poor
mental health.
SCORING: Multiple response scale was used instead of the bimodal scale.
The multiple-response scale or "Likert scale", was used where weights are assigned to
each position, e.g. the response options are scored 0, 1, 2 and 3, from "less so than
usual" to "much more than usual". A total score is then produced by adding together
each of the scores. A higher score indicated poorer psychological health.
6. Social and domestic survey -Section 5 question 5.1 to 5.5
SOURCE: Standard Shift Work Index, based on the Quality of Life Survey,
Section 4, used by Meredith Wallace and The Impairment in Social Activities scale of
the 1974-Survey, used by Friedhelm Nachreiner. The questionnaire consists of 19
items, covering social (e.g. sports, hobbies) and domestic (e.g. childcare, shopping)
activities. A 5 point response option was provided for Questions 5.1 - 5.4, ranging
from "not at all" to "very much".
SCORING:
Q 5.1A total score of general satisfaction by adding the item scores. The
higher the score the more satisfied.
Q 5.2 - 5.4-Separate scores were calculated for both these questions.
75
APPENDIX C
SLEEP LOG
The sleep log attempts to capture your sleeping time in hours.Please shade the hours you slept for the
last 2 weeks.
Eg
PM MIDNIGHT AM NOON
DAY 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Thursday
Friday
WEEK 1 PM MIDNIGHT AM NOON PM
DAY 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Thursday
Friday
Saturday
Sunday
Monday
Tuesday
Wednesday
WEEK 2 PM MIDNIGHT AM NOON PM
DAY 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Thursday
Friday
Saturday
Sunday
Monday
Tuesday
Wednesday







