
Somatoform Disorders
By : Dr Seddigh
HUMS
Dr Seddigh
An Overview of Somatoform Disorders
Somatoform Disorders
Somatization disorder Conversion disorder Hypochondriasis Body dysmorphic disorder Pain disorder
Hypochondriasis
Hypochondriasis: An Overview
Clinical Description Anxiety or fear be or having a seriuos
disease
bodily symptoms
Hypochondrium
Hypochondriasis: An Overview
Statistics 4% to 6% of medical patients
15% rate Female : Male = 1:1 Onset at any age
Peaks: age (20-30)
Medical students
Hypochondriasis
Causes Familial history
Genetics Modeling/learning
Other factors Stressful life events “Benefits”
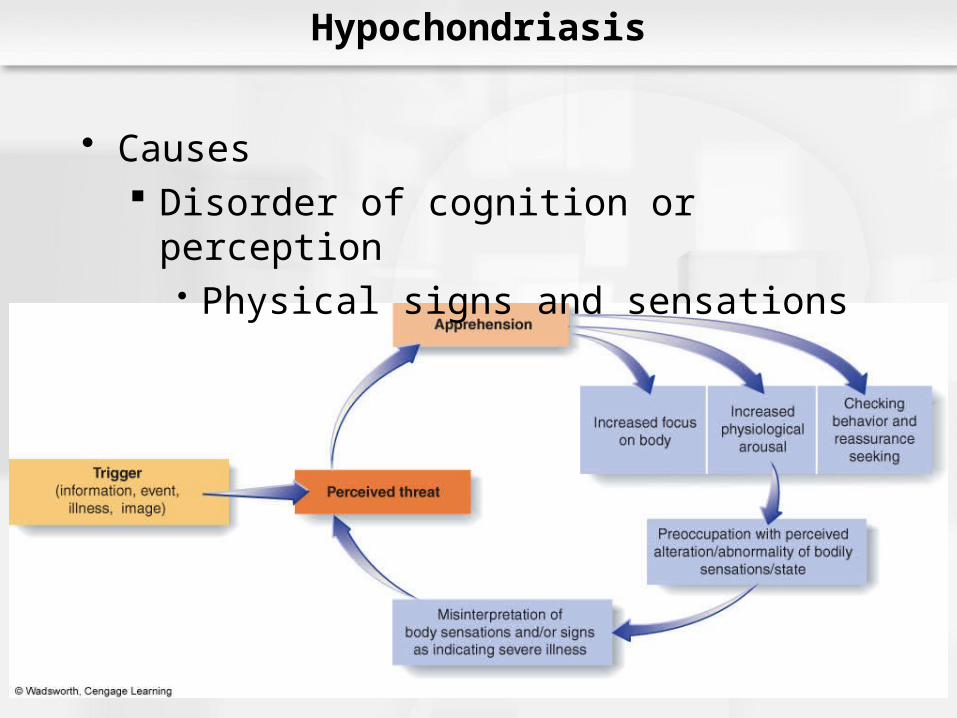
Hypochondriasis
Causes Disorder of cognition or perception
Physical signs and sensations
Hypochondriasis in DSM IV
A. Preoccupation with fears of having, or the idea that one has, a serious disease based on the person’s misinterpretation of bodily symptoms
B. The preoccupation persists despite apprpriate medical evaluation and reassurance
C. The belief in Criterion A is not of delusional intensity
Hypochondriasis
D. The preoccupation causes significant distress or impairment in functioning
E. The duration of the disturbance is at least 6 months
rumination about illness, suggestibility
unrealistic fear of infection, fascination with medical information
fear of prescribed medication. rumination about illness plus at least one of five other symptoms form a distinct diagnostic entity
performing better than the current DSM-IV hypochondriasis diagnosisAm J Psychiatry 161:1680-1691, September 2004
Hypochondriasis
Somatoform Disorder or Anxiety Disorder???

Hypochondriasis
Differ phobia
Hypochondriasis: already have
Reassurance temporary
Better prognosis 1- good socioeconomic 2- anxiety or depression (sensitive) 3-acute onset 4-no personality dx 5- no medical problem
accidents and criminal victimization develop various diseases.
Am J Psychiatry 163:907-912, May 2006
Hypochondriasis - Treatment
Group therapy Insight oriented and HX Cognitive-Behavioral
Identify and challenge misinterpretations “Symptom creation” Stress-reduction
Physical exammedications (SSRI)
Body Dsmorphic Disorder
Body Dysmorphic Disorder
Clinical Description Imagined defect in appearance Impaired function
Social Occupational
Not attracted Dysmorphophobia
Body Dysmorphic Disorder
Statistics 1% to 15% (unknown) Female >: Male = ~1:1
Onset = 15 – 30 y/o Most remain single Lifelong, chronic course With MDD, Anxiety & Psychosis
Body Dysmorphic Disorder: Causes
Little scientific knowledge
Cultural imperatives Body size Skin color
Serotonin ( OCD )
Body Dysmorphic Disorder in DSM IV
A. Preoccupation with an imagined defect in appearance. If a slight physical anomaly is present, the person’s concern is markedly excessive.
B. The preoccupation causes clinically significant distress or impairment in functioning
C. The preoccupation is not better accounted for by another mental disorder
Body Dysmorphic Disorder
Comorbidity with depression Some believe it is similar to OCD
Obsessions Compulsions
5 most common locations for perceived deficits: Skin – 73% Hair – 56% Nose – 37% Stomach – 22% Breasts/chest/nipples – 21%
partial remission 0.21 Gender and ethnicity did not significantly predict remission
Am J Psychiatry 163:907-912, May 2006
Body Dysmorphic Disorder
Clinical Description mirrors Suicidal ideation and behavior Unusual behaviors
Ideas of reference Checking/compensating rituals
Delusional disorder: somatic type?
Suicidal ideation mean of 57.8% per year attempted suicide mean of 2.6% per year. completed suicide (0.3% per year).
Am J Psychiatry 163:1280-1282, July 2006
Treatment
The Plastic Surgery Solution?Popular but ExpensiveMost are Disappointed with Results
CBT: Exposure and Response Prevention – very effectivePimozide,TCA,MAO INHClomipramine, SSRI’s – moderately effective
Treatment
The Plastic Surgery Solution?Popular but ExpensiveMost are Disappointed with Results
CBT: Exposure and Response Prevention – very effectivePimozide,TCA,MAO INHClomipramine, SSRI’s – moderately effective
Body Dysmorphic Disorder
With olanzapine treatment, body dysmorphic disorder symptoms minimally improved Pimozide augmentation of fluoxetine treatment for body dysmorphic disorder was not more effective than placebo,
Am J Psychiatry 162:377-379, February 2005
Pain Disorder
Clinical Description Pain is Real Pain May Have Organic Cause Psychological Factors Have an Important Role in:
onset severity exacerbation OR maintenance of the pain
Clinical Description Pain is Real Pain May Have Organic Cause Psychological Factors Have an Important Role in:
onset severity exacerbation OR maintenance of the pain
Pain Disorder
Pain Disorder
Clinical Description Pain in one or more areas Significant impairment Etiology may be physical Maintained by psychological factors
Pain Disorder
Statistics Fairly common 5% - 12%
Sex female 2 times Age from 30 & 40 y/o
Pain Disorder in DSM IV
A. Pain in one or more anatomical sites that is of sufficient severity to warrant clinical attention
B. The pain causes clinically significant distress or impairment in functioning
C. Psychological factors are judged to have an important role in the onset, severity, exacerbation, or maintenance or the pain
D. The symptom or deficit in not intentionally produced or feigned (as in Factitious Disorder or Malingering)
E. The pain is not better accounted for by another mental disorder
Treatment Behavioural Management,CBT& Insight oriented
Medication
not effective : analgesic ,antianxiety & sedative
effctive :TCA,SSRI & AMPHETAMINE
Others
BIOFEEDBACK
HYPNOSIS
Treatment Behavioural Management,CBT& Insight oriented
Medication
not effective : analgesic ,antianxiety & sedative
effctive :TCA,SSRI & AMPHETAMINE
Others
BIOFEEDBACK
HYPNOSIS
Pain Disorder
THANKS FOR
YOUR KIND ATTENTION







