

Staphylococcal Bacteremia and Endocarditis:Epidemiological Considerations
March 6, 2006
John Edwards, Jr., M.DProfessor of Medicine
UCLA School of MedicineChief, Infectious DiseaseDepartment of Medicine
Harbor-UCLA Medical Center

Increased Incidence of Sepsis in General
Martin GS et al. N Engl J Med. 2003;348:1546-1554.

Increasing Incidence of Gram-Positive Sepsis
225,000
75,000
150,000
25,000
15,000
10,000
5,000
0
1979 1981 1983 1997 1999 200119951985 1987 1989 1991 1993
Gram-positive bacteria
Fungi
Gram-negative bacteria
Martin GS et al. N Engl J Med. 2003;348:1546-1554.
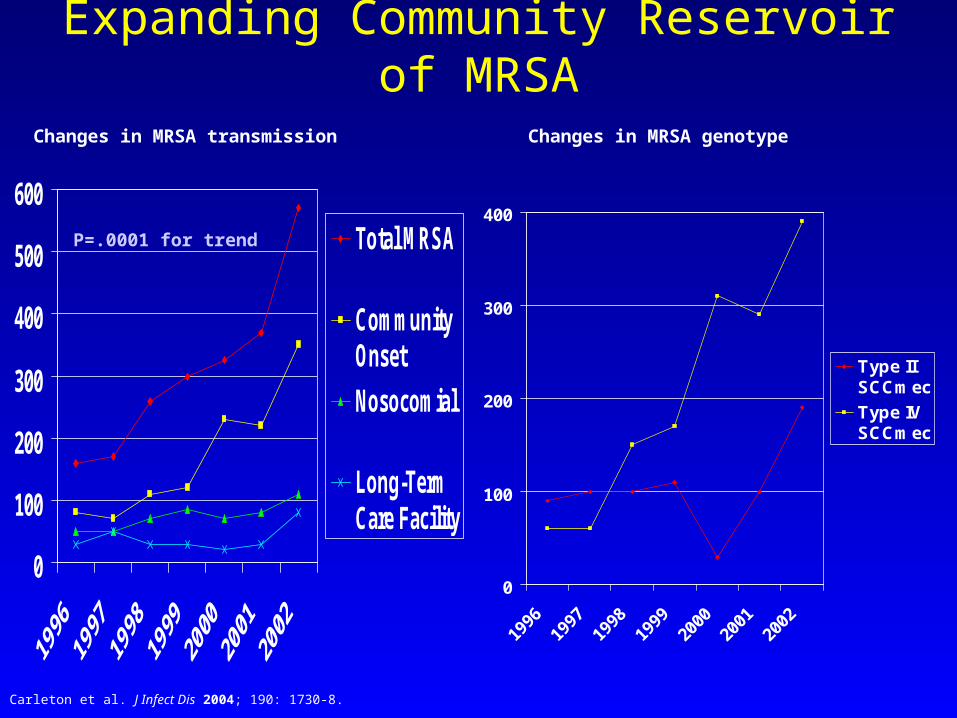
Expanding Community Reservoir of MRSA
0
100
200
300
400
500
600
Total MRSA
CommunityOnset
Nosocomial
Long-TermCare Facility
Carleton et al. J Infect Dis 2004; 190: 1730-8.
P=.0001 for trend
0
100
200
300
400
1996
1997
1998
1999
2000
2001
2002
Type IISCCmec
Type IVSCCmec
Changes in MRSA transmission Changes in MRSA genotype

Increase in Resistant Nosocomial MRSA
0
10
20
30
40
50
60
89 90 91 92 93 94 95 96 97 98 99 00
ICU Patients
Non-ICU Patients
% R
esis
tan
t Is
ola
tes
NNIS. Available at: www.cdc.gov/ncidod/hip/NNIS. Accessed July 8, 2003.

Hageman, JC et al. IDSA 2004 abst #1148
CA-MRSA in US is Clinically Distinct:Severe Secondary Pneumonia>6000 US patients with Influenza in 2003-04
263 ID MDs across US in Emerging Infection Network

• 116 Consecutive MRSA bloodstream isolates from Grady Hospital over 7 months available for genotyping
• MRSA USA300 - 28% Healthcare-associated BSI
- 20% Nosocomial BSI• MRSA USA300 - Injection drug use (3.67; 95%CI:1.10-12.28)
- Skin & Soft Tissue (4.26:95%CI:1.08-16.8)

Necrotizing Fasciitis Caused by CA-MRSAMiller New Engl J Med 2005;352:1445-53
• 14 patients at Harbor-UCLA• IDU: 50%• Homeless: 21%• Previous MRSA infection: 21%• Bacteremia: 28%• ST-8, USA 300 clone present in 100%• Distinct virulence repertoire: pvl, sdrC-E, icaA,
aroE, hemolysin

CA-MRSA in US: Conclusions
• Now common community pathogen in many parts of US
• Clinically distinct: severe sepsis, necrotizing pneumonia, empyema, musculoskeletal infections, necrotizing fasciitis
• Genotypically distinct: SCCmecIV, pvl, seh
• Hospital and community MRSA intermingling

InternationalCollaboration
OnEndocarditis
(ICE)
International Collaboration on EndocarditisMerged Data Base

ICE Structure 58 Sites / 26 Countries
• Argentina (2)
• Australia (8)
• Brazil (2)
• Chile (2)
• Croatia (1)
• Denmark (1)
• England (2)
• France (4)
• Germany (2)
• Lebanon (1)
• India (2)
• Ireland (1)
• Israel (1)
• Italy (3)• Lebanon (1)• The Netherlands (1)• New Zealand (1)• Romania (1)• Russia (2)• Singapore (2)• Slovenia (1)• South Africa (1)• Spain (5)• Sweden (1)• Thailand (1)• United States (10)

Increasing Frequency of S. aureus IEInternational Collaboration on Endocarditis (ICE)
~ 1700 Prospective IE Cases from 20 Countries
38%
13%7%
19%
12%
1%8%
2%S. aureus
Coag neg staph
S. bovis
Viridans streptococci
Enterococcus spp.
HACEK
Enteric Gram negatives
Other pathogens
Fowler VG et al. JAMA. 2005;293:3012-3021.
Results
• 48-month study period
• 1779 patients with definite IE from 16 countries enrolled in ICE
• Bloodstream isolates simultaneously collected
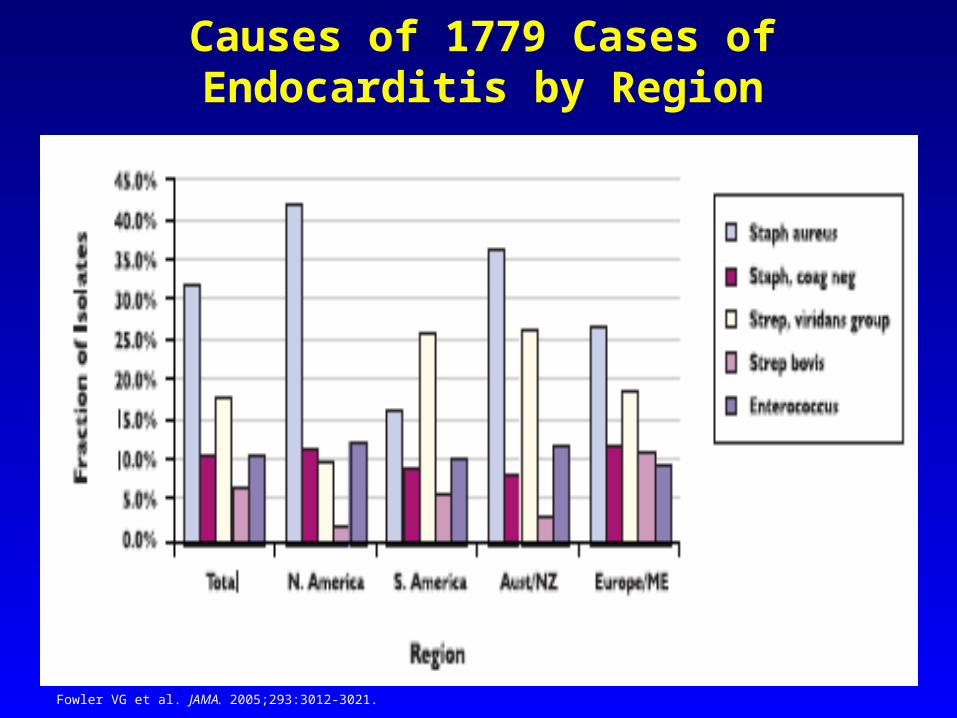
Causes of 1779 Cases of Endocarditis by Region
Fowler VG et al. JAMA. 2005;293:3012-3021.

Increasing Frequency of S. aureus IE: Evidence from > 2000 Patients from 5 Countries
Miro JM et al. Clin Infect Dis. 2005;41:507-514.

Mortality in Patients with S. aureus IE
0%
5%
10%
15%
20%
25%
30%
35%
40%
Overall (n=558) South America (n=24) Europe / Middle East (n=219) Australia / New Zealand (n=116) United States (n=199)
In-h
ospi
tal d
eath
Injection drug use Healthcare-associated Community
P < 0.0001
Fowler VG et al. JAMA. 2005;293:3012-3021.

0
0.5
1
1.5
2
2.5
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999
Year
Pe
r 1
00
0 M
ed
ica
re B
en
efi
cia
rie
s
P < 0.001 (for trend)
Cabell CH. Am Heart J. 2004;147:582-586.
Increasing Rates of Cardiac Device Infections in Medicare Beneficiaries:
1990-1999

Increasing Numbers of Cardiac Devices
Jauhar S. N Engl J Med. 2004;351:2542-2544.

$39,911
$62,325
$19,539
$57,292
$32,345
$37,498$40,574
$45,159$47,390
$82,287
$0
$10,000
$20,000
$30,000$40,000
$50,000
$60,000
$70,000$80,000
$90,000
Overall Other ChronicCatheter
Ortho Cardiac
Admitted with SAB Hospital-acquired SAB
S. aureus Bacteremia and Prosthetic Devices: Cost
Chu V et al. Am J Med. 2005;118: 1416.e19-24.
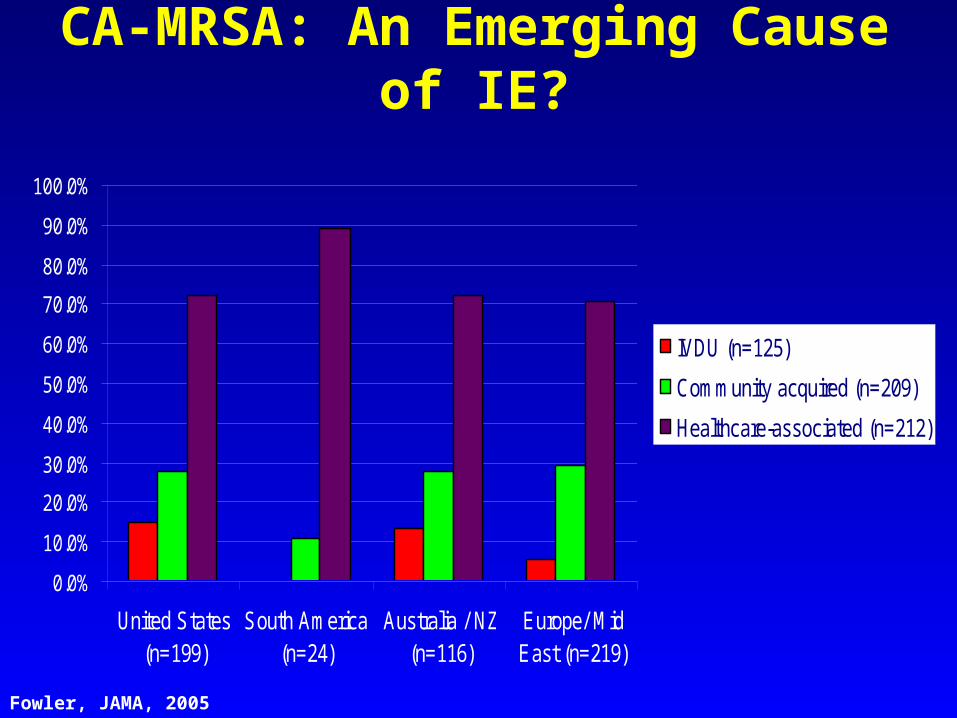
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
United States(n=199)
South America(n=24)
Australia / NZ(n=116)
Europe/ MidEast (n=219)
IVDU (n=125)
Community acquired (n=209)
Healthcare-associated (n=212)
CA-MRSA: An Emerging Cause of IE?
Fowler, JAMA, 2005

S. aureus with Reduced Susceptibility to Vancomycin
• Vancomycin Resistant S. aureus: (VRSA)
MIC> 32 µg/mL
• Vancomycin Intermediate S. aureus (VISA)
MIC: 8-16 µg/mL
• Heteroresistant S. aureus (heteroVISA)
MIC < 4 µg/mL; subpopulation MIC > 8-16µg/mL
• Vancomycin “Failures”
Cosgrove, SE. Clin Infect Dis 2004;39:539-45.

MMWR 2004; 53:322-3
Vancomycin Resistant S. aureus

General Summary Points: Epidemiology• Increased Incidence of Bacteremias in General• Increased Incidence of Gram Positive Bacteremias• Substantial Increase in Bacteremia Due To Staphylococcus• Staphlococcus aureus Is Now the Most Common Cause of Endocarditis• The Increase in Staphylococcal Endocardits is
Associated with Modern Health Care Advances• There is a Highly Significant Increase in both Community and Nosocomial Sources of MRSA Internationally• There is a Developing Increase in Staphylococcal resistance to vancomycin







