

Stroke: The First Six HoursEmergency Evaluation and Treatment
Introduction
The National Stroke Association (NSA) has preparedthisconsensus statement to bring attention to the importanceof thefirst minutes andhours afteronsetof stroke. Currently,preventionof strokeis thebest treatment. Thedramatic decreases in strokemortality andmorbidity overthepast 25 years havebeenlargelydue to hypertensioncontrol, atherosclerosis prevention, andtherapy for cardiacdiseaseto eliminate sources of emboli.8,18,24 Increasingpublic awareness of strokerisk factors has resultedinlifestyle changes suchas the cessation of cigarettesmoking, limiting alcohol consumption, avoiding obesity,andcontrolling bloodlipids. Individuals withstrokeriskfactors, mainlyhypertension, whoare appropriatelytreated and whomake neededchanges in lifestyle have asignificant reduction in the riskof subsequent stroke.
Unfortunately, manywhosuccessfully reducetheirriskmayhave one or morestrokes,andeventhose withoutriskfactors may havea stroke. For thoseindividuals, theNSAanticipates majorprogress over thenextfive to tenyears withspecific therapies for stroke. The NSA and theco-sponsors of this consensus statement recognize theimportance today of emphasizing to thepublicand tohealthprofessionals theimportance of the firsthours aftersymptom onset.Onlyif thoseearlyhours of therapeuticopportunity arc usedfor evaluation andearly treatmentcan the promise of new therapies be realized. When astrokeoccurs,treatments to limitbraindamage beguninthe earlyhoursof symptom onset arecritical andconstitute a medicalemergency.
Strokeis the leading causeof braindamage in adults.That damageresults from destruction of neurons followingeitherdisruption of cerebral bloodsupply or fromhemorrhage intoor around thebrain.Thisdestruction ofbrain tissueresults in a decrease in brainfunction and, forthepatient, reduced independence, a lossof self,andevendeath.
J t t
PPCOMING ISSU~S' .:
Acute Stroke Management Part IIICost of Stroke CareUrologicProblems After StrokeSubarachnoid Hemorrhage
This statement addresses the diagnostic and therapeuticprocedures available today that should be initiated assoonas thereare indications a stroke is beginning. Thesymptoms of strokeshouldhave the samealarmingsignificance in identifying a "brain attack" thatacutechestpain has in identifying a "heart attack." The Consensus Panelrealizes that this statement on themanagementof strokein thefirst six hours mustbe regularlyupdated as new treatments and diagnostic methodsbecome available.
Therapeutic Window
The Panelhas focused upon thefirst sixhoursafter theonsetof symptoms as criticalfor tworeasons. First,sixhours is a realistic goal todayfor a timeperiodwithinwhich strokepatients in nearlyall communities can beevaluated and treated. Second, andmore important, thebiology of strokeexperimentally andcJinicaUy is suchthateachhourof ischemia and tissueinjury increases thedegree of irreversible tissue death.Studies usingprimatemodels of focal ischemia and studies using other animalmodels haveestablished that thereis nouniformthreshold withregardto duration of ischemia and irreversibleinjury. Sixhours is a worthy goalfor themaximum timefor evaluation and treatment biologicaUy andmay beeventoo longfor sizablenumbers of patients. All studiesindicate thateachminuteof ischemia is harmful, whetherit be the 18thor the 180th.34 In the instance of intracerebralhemorrhage, ongoing bleeding withexpansion of thehematoma may occurin 20%or moreof patients withinthefirst several hours aftersymptom onset.7,38 Withsubarachnoid hemorrhage, mortality is initially high,rebleeding is common, and the mortality for rebleeding isalsohigh.28,36 In those whosurvivethe initial ictus,rebleeding mostcommonly occurs during thefirst day,particularly within12 hours after the initial hemorrhage.36
The earlierevaluation and treatment arcstartedafteronsetof strokesymptoms, the better. Thepublic andhealthprofessionals must be educated torecognize strokeas an emergency. Currently, thereis a lackof publicandprofessional awareness of the urgent nature of theproblem andtheneedfor trauma-like intervention.Fortunately, facilities for rapid access to and delivery ofemergency care are largely in placethroughout theUnited States. For trauma, systems havebeensuccess-
135
NSA CONSENSUSSTATEMENT
fullyestablished to carefor patients withacute injuries inthe"goldenhour"immediately afteronset. Similarly, formyocardial infarction, publicawareness is suchthat the6hourminimal standard is beingaccomplished. Initiatingacutestroke carewithin a 6-hourminimal period can beaccomplished.'?
In theensuing sections thosediagnostic evaluations areoutlined which areessential to identify thecauseof theimpending stroke. This is critical because treatments aredifferent, depending on the causeof thestroke.
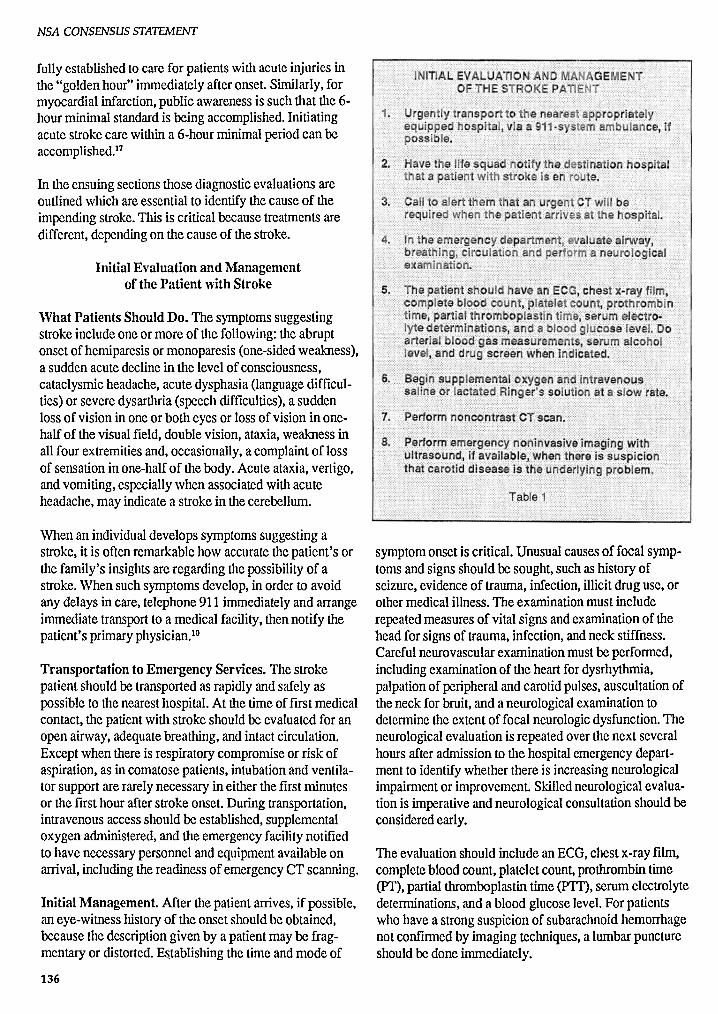
Initial Evaluation and Managementof the Patient with Stroke
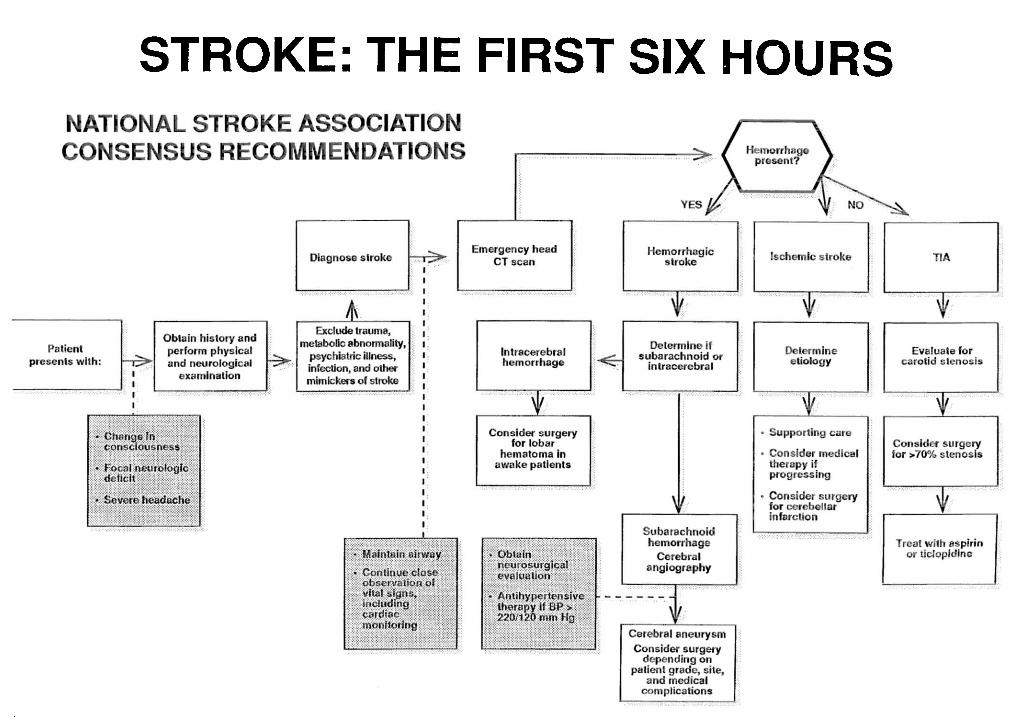
What Patients ShouldDo. The symptoms suggestingstroke include oneor moreof thefollowing: theabruptonsetof hemiparesis or monoparesis (one-sided weakness),a suddenacutedecline in the levelof consciousness,cataclysmic headache, acutedysphasia (language difficulties)or severe dysarthria (speech difficulties), a suddenlossof visionin oneor both eyesor lossof vision in onehalfof thevisual field, doublevision, ataxia, weakness inallfour extremities and,occasionally, a complaint of lossof sensation in one-half of thebody.Acuteataxia, vertigo,andvomiting, especially whenassociated withacuteheadache, mayindicate a strokein thecerebellum.
Whenan individual develops symptoms suggesting astroke, it is oftenremarkable how accurate thepatient's orthefamily's insights areregarding thepossibility of astroke. Whensuchsymptoms develop, in orderto avoidanydelays in care,telephone 911 immediately and arrangeimmediate transport to a medical facility, thennotifythepatient'sprimary physician."
Transportation to Emergency Services. Thestrokepatientshouldbe transported as rapidly andsafelyaspossible to thenearest hospital. At the timeoffirst medicalcontact, the patient withstrokeshould be evaluated for anopenairway, adequate breathing, andintactcirculation.Except whenthere is respiratory compromise or risk ofaspiration, as in comatose patients, intubation andventilatorsupportarerarely necessary in eitherthefirstminutesor thefirsthourafterstrokeonset. During transportation,intravenous access shouldbe established, supplementaloxygen administered, and theemergency facility notifiedtohavenecessary personnel andequipment available onarrival, including thereadiness of emergency CT scanning.
Initial Management. After thepatientarrives, ifpossible,aneye-witness history of theonsetshouldbe obtained,because thedescription givenby a patient maybe fragmentary or distorted. Establishing the timeandmodeof
136
symptom onsetis critical. Unusual causes of focal symptoms andsignsshouldbe sought, suchashistoryofseizure, evidence of trauma, infection, illicitdruguse,orothermedical illness. The examination mustincluderepeated measures of vitalsignsandexamination of theheadfor signs of trauma, infection, andneckstiffness.Careful neurovascular examination mustbe performed,including examination of the heartfordysrhythmia,palpation of peripheral andcarotid pulses, auscultation oftheneckfor bruit, and a neurological examination todetermine the extentof focal neurologic dysfunction. Theneurological evaluation is repeated overthenext severalhours afteradmission to thehospital emergency departmentto identify whether thereis increasing neurologicalimpairment or improvement Skilled neurological evaluationis imperative andneurological consultation should beconsidered early.
The evaluation shouldinclude anECG, chestx-rayfilm,complete bloodcount, platelet count, prothrombin time(PT), partial thromboplastin time(PTT), serumelectrolytedeterminations, anda bloodglucose level. Forpatientswhohavea strong suspicion of subarachnoid hemorrhagenotconfirmed by imaging techniques, a lumbar punctureshould be doneimmediately.
Unless the stroke is hemorrhagic, elevations in systemicarterialpressureshouldnot be treatedurgently unless 1)the systolic pressure exceeds220 mm Hg or the diastolicexceeds 120mm Hg on three repeated measurementsmade at IS-minuteintervals,or 2) cardiacfailureorarterialdissection has been identified. Elevated bloodpressurewill usuallydeclinespontaneously by about10%over the first 24 hours and over-zealous use ofcalciumantagonists andother antihypertensive drugs cancause further reduction in cerebralperfusion.6
DiagnosticTesting
Computed Tomography (CT). On arrival, thepatientshouldhavean emergency CT scanwithout contrasttodetermine whether thestrokeis hemorrhagic or ischemic.CThas become absolutely necessary forpatients suspectedof having a strokebecause all subsequent therapeuticdecisions depend on its results. It is welltolerated bygravely ill patients and is usuallyreliable for identifyingsubarachnoid hemorrhage. It can definealmost all intracerebralhematomas >1em and morethan95% of subarachnoidhemorrhages." Morethan90% ofhospitals with200or morebeds in thiscountry havecr scanners.'
The cr scanusually doesnot showischemic strokeoredemafor at least24 to 48 hoursafteronset.The edemafromstrokeis usually not visibleearlieron cr. However,a largeinfarction produces edemamorequickly, causingalocalized masseffectwitha decrease in thesizeof thecortical sulci andsubarachnoid cisternae alongwith adecrease in grayand white matterdifferentiation in theaffected region." The use of contrast mediaenhancementdoesnot resultin anearlierdiagnosis.
Magnetic ResonanceImaging (MRI) is usually notindicated for emergency diagnosis. Whenavailable, it hassomeadvantages overcranial cr, including bettergrayand whitematterresolution of allparenchymal structures.It provides significantly better identification of normalandabnormal tissues, has theabilityto perform multiplanarimaging withease,anddoesnot involve radiation. MRIwillshowevidence of ischemic strokesoonerthantilecranial cr.56,61
Disadvantages of MRI include the fact that it is notgenerallyavailable and is more expensive to utilize.Theconfiguration of tilescannermakes it difficultto monitora seriouslyill patientduring the MRI and, currently,thetime requiredto perform an MRI is greaterthancr.Motionartifacts in the ill, disoriented individual are aseriousproblem in getting an adequate MRI.In addition,acute subarachnoid hemorrhage can easilybe missed byMRI.
NSA CONSENSUSSTATEMENT
MRIAngiography, whichcan be doneduring theusualMRIprocedure, is usefulfor demonstrating largevesselocclusions at thebaseof theskullbut small intracranialvascular occlusions are not readilyapparent.
Although cr may settlewhetherthestroke is ischemic orhemorrhagic, othertechniques canhelpindecidingwhether or not to proceedwith surgicalormedicalmanagement.
Arteriography isdefinitive for demonstrating stenosesand occlusions of both large and smallbloodvessels inthe head andneck.It can detect more subtlearterialabnormalities, such as dissection, whichmay be missedwith otherneuroimaging techniques. It is the definitivetechnique for demonstrating the causeof subarachnoidhemorrhage due to aneurysms andfor defining theiranatomical relationships. It is not usefulfor demonstrating the extentof infarctionor otherparenchymal abnormalities. It is invasiveand requiressignificant time andexpertisebut is generallyavailablein hospitals in theUnitedStates andcan be performedwithminimalpermanent morbidity and mortality (0.5% or less).22,23
When an arteriovenous malformation is suspectedas tilecauseof subarachnoid hemorrhage, arteriography is tiledefinitive study.
Ultrasonography.Ifavailable in theemergency departmenton a 24-hour basis, cervical Doppler ultrasonography andduplex imaging canbe a useful noninvasive technique toscreen forcervical internal carotid stenosis. Differentiationbetween stenosis of 95%or greater andcomplete occlusionis usually notpossible, butdemonstration of stenosisexceeding 60%is quiteaccurate. Thistechnique is highlydependent onthecapabilities of theultrasonographer whichis a majordisadvantage. Furthermore, no imaging systemindicates thatthestroke hasoccurred as a result of thedemonstrated lesion. Onlythephysician canconfirm thediagnosis of stroke.
DifferentialDiagnosis.Currently, cr doneduringthefirstsix hours afterthe onsetof symptoms provides thephysician witha numberof answers about thecauseof thepatient's stroke. Thecr scandemonstrates whether thestroke is hemorrhagic or ischemic in morethan9S%ofpatients."Ifthe strokeis hemorrhagic, it canprovideinformation aboutwhether the hemorrhage is subarachnoid,intracerebral, or a combination of both.In patientswithhemorrhagic stroke,angiography helps identify thebleeding source.
The cerebral angiogramalso confirms whetherthere issignificant vessel stenosisand its location in patientswithcerebralinfarction presumedto be due to carotidocclu-
137
NSA CONSENSUSSTATEMENT
sivedisease. Basedon the results of these studies, thephysician is thenfaced with the decision of how toproceedwith treatment thatmay avoidfurther braindestruction. At thispoint, the firstdecision is whether touse surgical or medical management.
Management
Transient Cerebral Ischemia
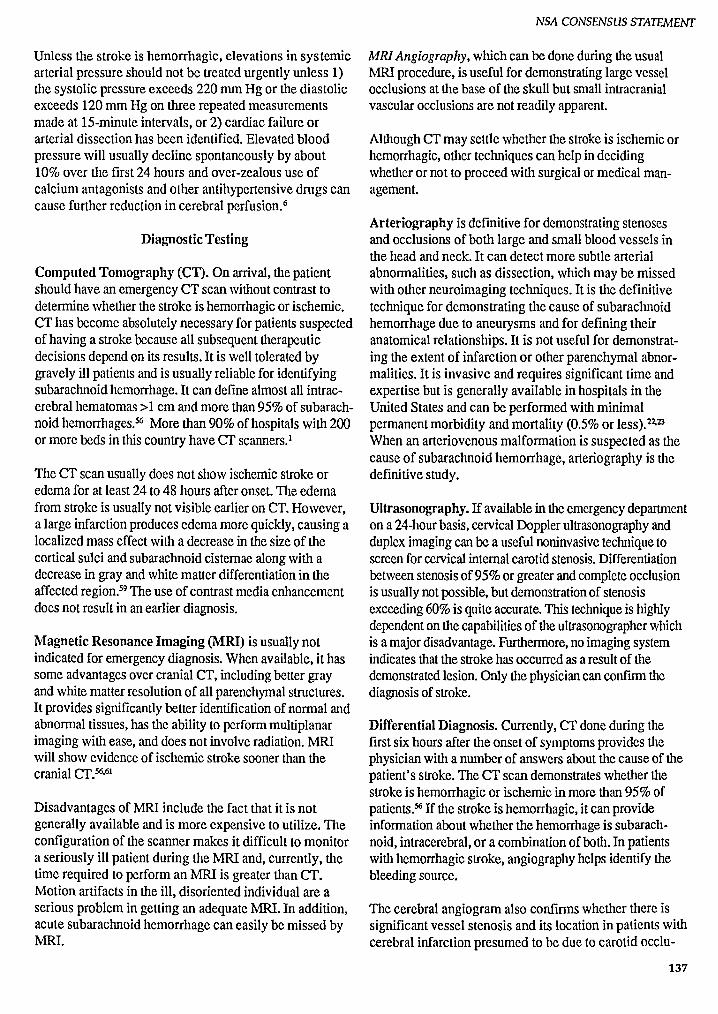
Surgical Management. For thepatientwhosecerebralischemia is transient and resolves during thefirst sixhoursafteronset, surgicaltreatment shouldbe considered.Thereis goodevidencethatendarterectomy for anarterial obstruction of 70 to 99% stenosis, on the side
• . ' .' ,' " .'. :.: . :: . ' . •. ' •... . :. . . . ",' .•• : .~...•...... '. ,. ,•.•...•. :.' •.•.•:...y •.. .•.. .. '" ' ," • ... : .:
. ,' .-..'....~ -.'.:.::::.: .;:::..- - ..',-. ........ '..:.','.:.'":: "
appropriate to the symptoms, effectively reduces futurechances of stroke. This has been demonstrated by several studies, bothin the UnitedStates andEurope, forpatients withinternal carotidstenosis obstructing anarterial lumenmorethan70%.16,48 Aftera transientischemic attack(TIA), the patientshouldbe evaluatedwitha senseof urgency but the evaluation shouldruleouta causefor theTIA unrelated to carotidstenosis. Althoughthereis no reasonto undulydelaysurgeryat thepresenttime, carotidendarterectomy is generally anelective procedure.
Medical Management. Patients withTIA withinthepastfew hours areconsidered to have a highrisk for recurrence in several situations. These include: 1) patientsknownto havea high-grade stenosis in a vascularterritory appropriate to the symptoms,2) patients alreadyon antiplatelet therapy, 3) a cardioemboliccause, or
138
4) attacks thatoccurwith increasing frequency (crescendo TIA).In theseinstances, it it is common practiceto consider anticoagulant therapy, initially withheparinandcontinued withwarfarin. For this treatment, there isno firm data to support predictable efficacy.
For patients withTIA who are selected for medicalmanagement, agents that inhibit platelet aggregation,such asaspirin and ticlopidine, should be givenifheparinis not usedY·19.26,57 There is no available data to supportthatplatelet aggregation-inhibiting agents have a predictableeffecton the courseof TIA in thefirst six hours afteronsetbut these medications havebeenshownto reducethe occurrence ofTIA and stroke whentakenchronically.The effectof aspirinon platelets is almostimmediate,depending on the rate of absorption. Doserequirementsof aspirin arevariable, as hasbeenshownby testing forevidence of inhibition of plateletaggregation." The fulleffectof ticlopidine on inhibition of plateletaggregationmay takeseveral days." For those patients who areunableto takeaspirin, and in some otherselected patients, ticlopidine shouldbe given.
Beforeconsideration of anticoagulant or plateletaggregation inhibition therapy the patientmusthavehad acomplete bloodcount,including a platelet count,PTT,and aPT.
Recent Stroke
Surgical Management. For thepatient who arrives witha continuing neurological deficit due to cerebral ischemia, evidence for the efficacy of immediate surgicalremoval of obstruction is controversial andunproven,13·29.41.44 Over thepast decade, emergencyendarterectomy has beenperformed in a sizablenumberof patients to remove obstruction or open an arterialocclusion but withoutsupportof efficacy fromcarefullycontrolled randomized studies."
Consideration of urgentcarotidendarterectomy for recentischemic strokegenerally is limited to conscious patientswith 1) strokein evolution whohavea minimal fixedneurological deficit,or 2) a moderately severeneurological deficitof abruptonset" whensurgery can be completedwithinthefirst few hours afterthe onsetof deficit.This usually means that patients arconlyconsidered forsurgery whenthe deficithas occurred while thepatient isin a hospital whereexpertfacilities are available for rapiddiagnosis and treatment. However, thereis no firmdatato mandate thisapproach.
Medical Management. Anticoagulant therapy is believedby someclinicians to prevent deterioration of a
patient's neurologicdeficit during the first hours afteronset or stroke in evolution." No studies of evolvingstroke treated within the first six hours after onset havebeen done that prove the benefit or risk of anticoagulants in reducing tissue injury.15.20 The use of heparininitially and continuing with warfarin for a stroke inevolution is based on the historical observation that, ifuntreated, this syndrome often results in poor neurologic outcome." In the setting of a stable but small areaof brain ischemia, heparin and warfarin use is considered if the ischemia is associated with arterial or cardiacmechanisms with a high risk of worseningbecause ofrccurrcnce.P-"
Anticoagulants are contraindicated where there is highrisk of worsening because of intraparenchymal bleeding,uncontrolledhypertension, or activebleedingelsewhere.The brain infarctions most prone to bleedingare large,usually the result of emboli, and showhypodensityorhemorrhagictransformation on an early CT scan. Themost serious complication of anticoagulant therapy,CNShemorrhage, occurs in 1% to 4% of patients with TIA,progressing stroke,or acute stroke."
Ifanticoagulant therapyis to be givenwithin the first sixhours after onsetof cerebral ischemia in a patient withoutcontraindications to such therapy, it is usually initiatedwith heparin,followedby warfarin. Exceptwithcardioembolic stroke, where there is increasedrisk forhemorrhagic transformation and where thepatient isusually not treatedwith a heparinbolus, heparin shouldbe given as follows. There shouldbe an initial dose of5000 to 10,000U, followedby continuous infusionof 10to 20 U/kg/hrto keep the PTT at 50 to 60 seconds orabout 1.5 to 2.0 times the patient's pretreatmentPTT.The needed amountof heparin mustbe gaugedbyrepeated PTTs.
Use of agents that prevent plateletaggregation, such asaspirinand ticlopidine, have been suggestedfor acutetreatmentof recentstroke. It is unlikely that these agentscan becomeeffectiveifgiven in the first six hours afteronset of symptoms, but they are useful in preventingstroke in patients with TIA and small strokeswhen givenchronically.
Intracranial Hemorrhage Management
Subarachnoid Hemorrhage Due toRuptured Aneurysm
Surgical Management. The CT scan is used to diagnosesubarachnoid hemorrhage (SAH),since it demonstratesapproximately 95% of all such hemorrhages.56 The CT
NSACONSENSUSSTATEMENT
scan is useful in detecting increased intracerebral densityin large arteriovenous malformations. When the diagnosis of SAH is highly suspectedand the CT scan is normal, a lumbarpuncture to detectbloodin the cerebrospinal fluid is necessary.
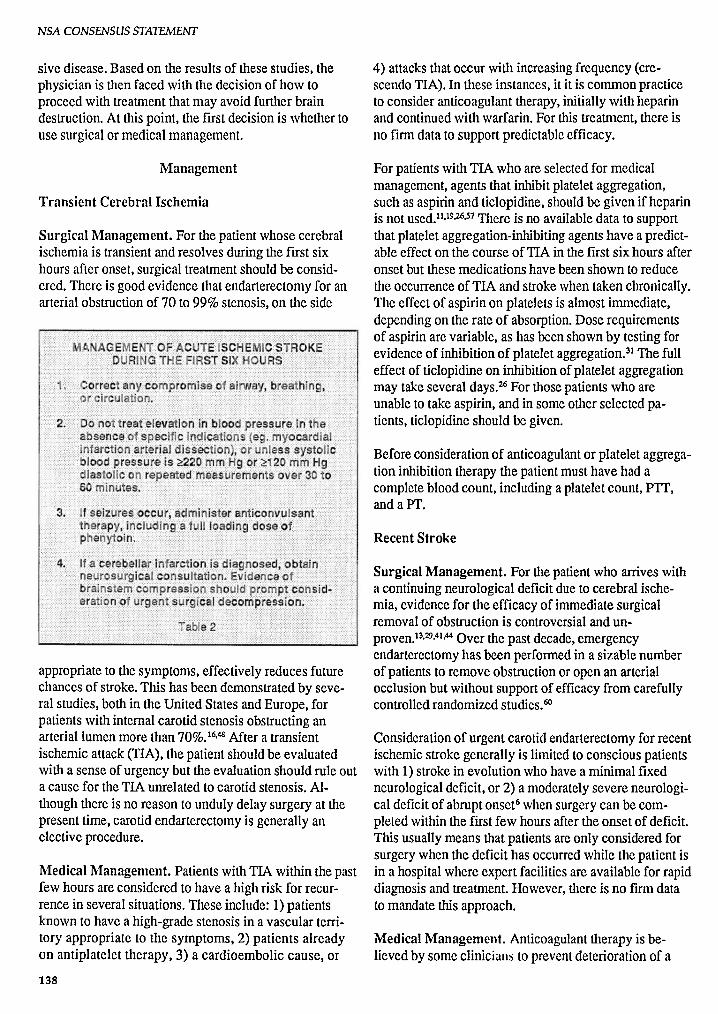
Early surgeryis usually consideredfor awakepatients ifthe aneurysmis surgically accessible and there arenomedicalcomplications which wouldprevent safe surgical
,. Corree any comprom ise of airway , r at •lng , or c ircula tion .
2. Obta n n e ros rgica co nsult ation .
3. Treat e levat ions of lood pr ssure whenhigh r th an pr e·SAH blood pre ss ur s (ie,t rea t to a rd n orm otens ive level In prev i·o usly n orm otensive patients).
4. Beg in nimodlpine 6 0 mg orally e e ry fourho rs in pa tient grad es 1 , 2, an 3 .
5. If se izures occ ur , give anticon lsanth erapy, i ncluding a full loa ding do se ofph enytoi n .
6. Give ana lge s ics a n se ave s s nee
7. Eme rgenc y ang i grap hy, invasi v hemo y.namic mon ito ring ;and early su ery sho Ibe co nsid ere with ane rys mal S H.
Tab le 3
treatment." However, it should be stated that there is nodata at the present time to mandate this approach. 31
Patientswith SAH should be transferred to a hospitalwhereskilledneurosurgical care is immediately available.
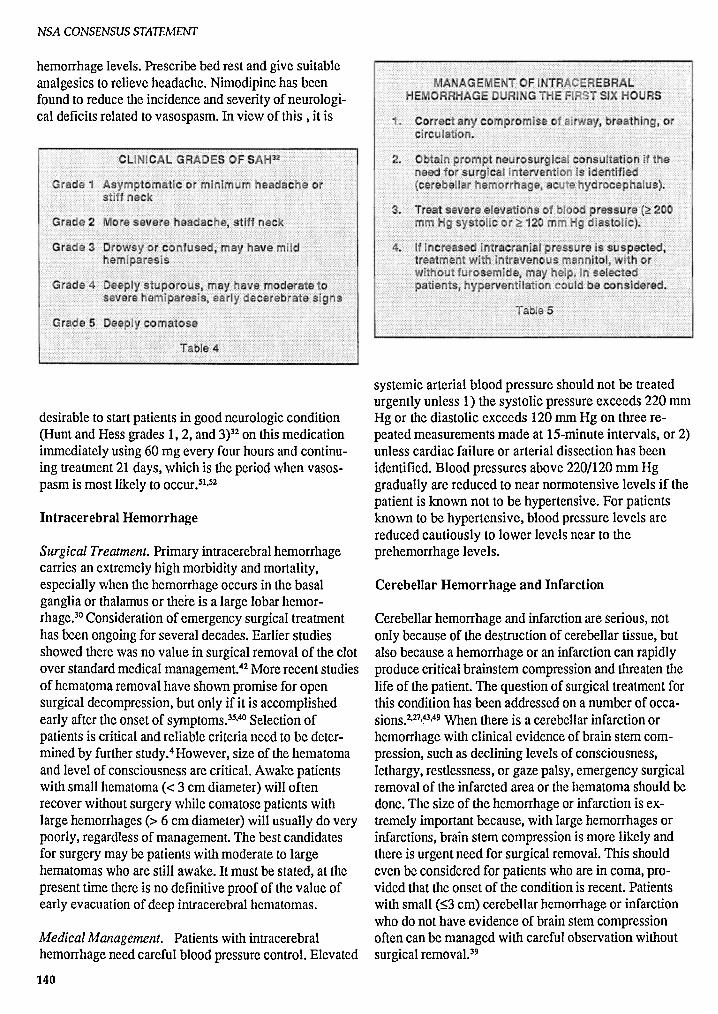
Managementrequires, in additionto identifyingthepresenceof SAH, the angiographic localizationof theaneurysmor aneurysms causing thebleed and the clinicalgradingof the patient (fable 4).3Z Patientsin grades 1, 2,and 3 shouldbe consideredfor earlysurgery.Patientsingrades4 and 5 are at greater risk of having a poor outcome following any surgicalprocedure to treat thebleedingsource. For patients in thesegrades who havehydrocephalus and intracerebral hematoma, surgicalcorrectionof hydrocephalus andhematoma removalmaybe life-saving.
Medical Management. PatientswithSAH shouldhavetheir bloodpressurebrought to nonnallevel or near pre-
139
NSACONSENSUSSTATEMENT
,-.;..-.;:: ;.:.• .. . :::: :i: ~ ij N. i.q ..... . .. .. ..... ...
hemorrhage levels. Prescribebed rest and give suitableanalgesics to relieveheadache. Nimodipine has beenfound to reducethe incidenceand severityofneurological deficitsrelated to vasospasm. In view of this , it is
desirable to startpatients in goodneurologic condition(Huntand Hessgrades 1,2, and 3)32 on thismedicationimmediately using 60 mg everyfour hours and continuing treatment21 days, which is the period whenvasospasm is most likely to occur.v-"
Intracerebral Hemorrhage
Surgical Treatment. Primaryintracerebral hemorrhagecarries an extremely high morbidity and mortality,especiallywhenthe hemorrhage occurs in the basalgangliaor thalamus or there is a large lobarhemorrhage." Consideration of emergency surgical treatmenthas been ongoing for severaldecades. Earlierstudiesshowedthere wasno value in surgicalremovalof the clotover standardmedicalmanagement.42 Morerecent studiesof hematoma removal have shownpromisefor opensurgicaldecompression, but only ifit is accomplishedearly after the onsetof symptoms.w" Selectionofpatients is criticalandreliablecriterianeed to be determined by furtherstudy.fHowever, size of the hematomaand levelof consciousness are critical.Awakepatientswith smallhematoma « 3 em diameter) willoftenrecoverwithoutsurgerywhilecomatose patientswithlarge hemorrhages (> 6 em diameter) willusually do verypoorly,regardless of management. The bestcandidatesfor surgerymaybe patientswithmoderateto largehematomas who arc still awake.Itmust be stated, at thepresent time thereis no definitiveproof of the value ofearly evacuation of deep intracerebral hematomas.
MedicalManagement. Patientswith intracerebralhemorrhage needcarefulbloodpressure control.Elevated
140
systemicarterial blood pressure shouldnot be treatedurgentlyunless 1) the systolic pressure exceeds 220 mmHg or the diastolic exceeds 120 romHg on three repeated measurementsmade at IS-minute intervals, or 2)unless cardiacfailure or arterial dissectionhas beenidentified. Blood pressures above 220/120 mm Hggraduallyare reduced to near normotensive levels if thepatient is known not to be hypertensive. For patientsknown to be hypertensive, blood pressure levels arereduced cautiously to lower levels near to theprehemorrhage levels.
Cerebellar Hemorrhage and Infarction
Cerebellar hemorrhage and infarction are serious,notonly becauseof the destructionof cerebellar tissue,butalsobecausea hemorrhageor an infarction can rapidlyproducecriticalbrainstemcompression and threatenthelife of thepatient.The questionof surgical treatmentforthis condition has been addressed on a number of occasions.2,27.~3,49 When there is a cerebellar infarctionorhemorrhage with clinicalevidenceof brain stem compression, such as declininglevelsof consciousness,lethargy, restlessness, or gazepalsy,emergencysurgicalremoval of the infarctedarea or the hematoma shouldbedone.The size of the hemorrhage or infarctionis extremely importantbecause, with largehemorrhages orinfarctions, brain stem compression is more likely andthere is urgentneed for surgicalremoval. This shouldeven be consideredfor patientswhoare in coma, provided that the onset of the condition is recent. Patientswith small ($3 em) cerebellarhemorrhage or infarctionwho do not have evidenceof brainstemcompressionoftencan be managedwith careful observationwithoutsurgicalremoval."
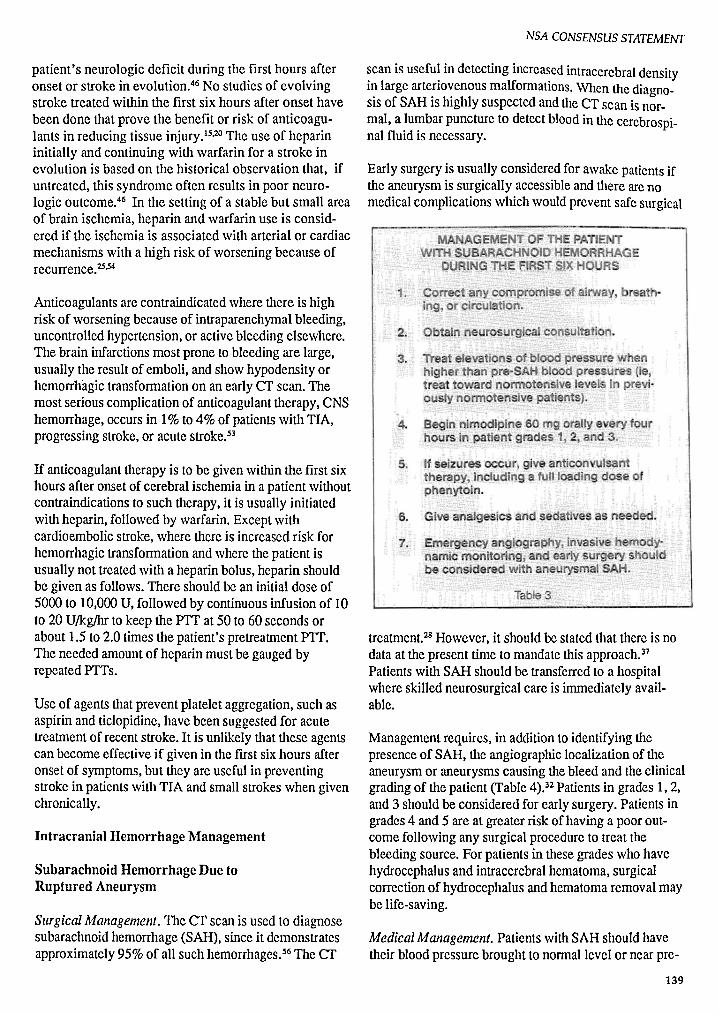
STROKE: THE FIRST SIX HOURS
Patie n tp resents with:
Obtain history a ndperform physicaland neu rologi cal
e xam inat io n
..... ; ..... :
Diagnose s troke
Exclude trauma,metabolic ab normality,
p sychiatric illness,Infection, lind othermhnlckCf s of s troke
IIII
Emerge nc y h eadCT sc a n
Int rac e re bra lhemorr hage
.: ''V' .'.-
Con sider surge ryfor lobar
hema toma Ina wake pa tien ts
,",'.
Hemorrh ag ics troke
'V:'
Dele rmln e ifsubarachno id or
in trace rebra l:
' . .-..... -.....
:
:
\ I.S u bar a chnoidhem orrhag e
Ce reb ra la ngiogra p hy
", " . ...'..- -:.- - -..-,-\ ,.
Ce re bral an eu rysm~~ Co n side r surg ery
depend ing onpati ent gr ad e, s ite,
a nd m edica lco mp lications
Isc hem ic s troke
De ler m ince tiolog y
"\Y.• S up por ting cOlre
• Con s id er m ed ica lther apy ifp rogre ssing
• Con sid e r sur ge ryfor ce rebell arIn farc tion
, ..
TI
Evaluate fo rcar otid s te nosi s
Co ns id er s urge ryfor >70"k s tenos is
Tre at wlth as pirinor ticlop ld lnc

NSA CONSENSUS STATEMENT
Future Developments with Promise inDiagnosis and Treatment of Stroke
Diagnostic Methods, When MRIbecomesmore widelyavailable, it maybecomethe imaging procedure ofchoicefor the diagnostic evaluation of ischemicstroke.With improved computerMRI software, there is thepotentialto demonstrate within six hours 1) accumulationof tissuewater,2) vascular transit time,3) tissueperfusion and metabolism, and 4) measurements of intracellular andextracellular water and electrolytes, in both thecore of the infarction and in the surrounding penumbra.
Transcranial Doppler(TCD)can identify obstructioninthe proximal middle cerebral artery and this findingmaybe important in selectingpatientsfor thrombolytictherapy,12·5o.55 Unfortunately, TCD may not demonstratethe middlecerebral artery in up to 25% of patients tested,a limitationthat will likelybe lessenedwith improvedtechnology.
During cerebral angiography, interventional neuroradiolgists are now able to deliver thrombolytictherapy bythreading a fine guidewire and infusion catheter to andthrough an intravascularclot in the internal carotidartery or its branches to administer intra-arterialthrombolyticagents that restore blood fiOW. 47 Carotidartery stenoses in the high cervical region and vertebralstenoses have been successfully dilated using intravascular inflatable balloons.These techniques require ahigh degree of expertise which is only available currently in large medical centers. They may become morewidely availablebut, first, need to be evaluated incarefully controlledstudies.
Promising Surgical Therapeutic Advances. Reportsofexperimental studies using stereotactic techniques toremovelobarhematomas, with or withoutclot lysis,using thrombolytic agentshave been imprcssive.v"Thistechnique needscarefulstudy to be sure it improvespatientoutcome.
Experimental MedicalTherapies Showing Promise.Several agentsto improveanticoagulant therapyarebeingstudiedin the US, Canada, Europe, and Australia.These include lowmolecularweightheparinoids whichcarry a lower riskof bleedingwhenusedforanticoagulation" and ancrod,a thrombin-like enzymederived from the venom of the Malayan pit viper. Patients treated with ancrod are "anticoagulated" by areduction in circulating fibrinogen. These agents arebeing evaluated in experimental trials in acute ischemicstroke because preliminary reports were favorable.
142
Thrombolytic agentssuch as urokinase and streptokinasewill lyse clots and they have beenshownto be useful inthe treatment of myocardialinfarction. For cerebralinfarction, pilot trials have been completed and theresultsareencouraging" but, as yet, theirvalue hasnotbeenproven.Recently, with thedevelopment of recombinant tissueplasminogen activator(tPA), therehas beenrenewed interestin thepossibilitythat theseagentscouldbe effective for treatingacutestrokeand, possibly,limiting or reversingischemia.9,IO.14
Several trialsusing these agentsare goingon in theUnitedStates andAustralia. Preliminary resultshaveprompted continuingthese studies. The main problemwith this treatment is that, to be effective, it must begivenwithina very short time after symptoms of cerebralischemia begin and theremust be certainty that thestrokeis not hemorrhagic. This has required a more urgentapproach to the problemof evaluating patients withcerebralischemic episodes.In studycenters,an emergencyprogram has beendesignedtoevaluatea patientwithextraordinary rapidityand to begin treatmentwithinone hour and a half after strokeonset.This has beendifficultto achieve but it is clear fromthose areas wherestudiesarebeingconductedthat it is possible. Ifthesestudiesshowit is possible to lyse a clot that has causedan acuteischemic stroke and preventor limit cerebralinfarction, emergency programsfor givingthis treatmentwillbecomea necessity. The use of thrombolytic agentsat this timeshouldonly be considered as part of a research protocol.
There are severalagents thought to provideneuronalprotection from ischemia. These include calciumchannelblockers whichreduceor preventcalcium entry intoneurons duringischemiaand, thus,avoidthe toxiceffectof intracellular calcium.These agents includethedihydropyridine calciumantagonists (nirnodipine andnicardidplnc). Duringischemia, excitatory neurotransmitters are releasedthat allowcalciumentry into neurons,activating a numberof proteolytic enzymes. The resultmay be theproductionof free radicals whichcan causeneuronal toxicity. Antagonists to theneurotransmitterglutamate have been used experimentally to blockcalciumentry intoneurons and are undergoingevaluation.Scavengers of free radicals suchas 21aminosteroids ("Lazaroids")have beeneffective inexperimental studies and are beingevaluated clinically."
Conclusions
Treatmentof acutestrokecan changedramatically by theend of thedecade. Methods to limitor reverse ischemia
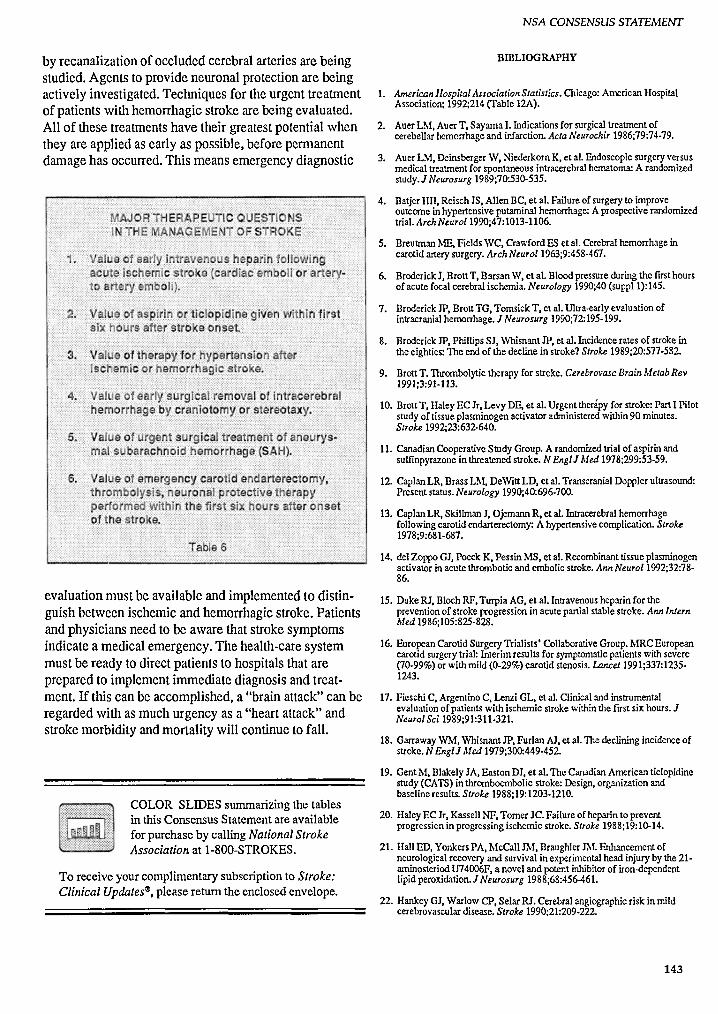
by recanalization of occluded cerebral arteries are beingstudied. Agents to provide neuronal protection are beingactively investigated. Teclmiques for theurgenttreatmentof patients withhemorrhagic strokearebeingevaluated.Allof thesetreatments have theirgreatest potential whenthey areapplied as earlyas possible, beforepermanentdamage has occurred. This meansemergency diagnostic
NSA CONSENSUSSTATEMENT
BIDLIOGRAPHY
1. Americanllospital AssociationStatistics.Chicago: AmericanHospitalAssociation; 1992;214(fable 12A).
2. AuerLM, AuerT, Sayama I. Indicationsfor surgicaltreatmentofcerebellarhemorrhageand infarction.ActaNeurochir 1986;79:74-79.
3. AuerLM, DeinsbergerW, NiederkomK, et at. Endoscopicsurgeryversusmedicaltreatmentfor spontaneousintracerebral hematoma: A randomizedstudy.J Neurosurg 1989;70:530-535.
4. BatjerHH, Reisch JS, Allen BC, et at. Failureof surgeryto improveoutcomein hypertensiveputaminalhemorrhage: A prospectiverandomizedtrial. ArchNeurol1990;47:1013-1106.
5. BreutmanME,FieldsWC, CrawfordESet al. Cerebralhemorrhageincarotidarterysurgery.Arch Neurol1963;9:458-467.
6. BroderickJ, Brott T, BarsanW, et at. Blood pressureduringthe firsthoursof acute focalcerebralischemia.Neurology 1990;40(suppll): 145.
7. BroderickJP, BrottTG, TomsickT, et at. Ultra-earlyevaluationofintracranialhemorrhage.J Neurosurg 1990;72:195-199.
8. BroderickJP, PhillipsSJ, WhisnantJP, et al, Incidencerates of strokeinthe eighties:The end of the decline in stroke?Stroke 1989;20:577-582.
9. BrottT. Thrombolytictherapyfor stroke. Cerebrovasc BrainMetabRev1991;3:91-113.
10. BrottT. HaleyEC Jr, Levy DE, et at. Urgent therapyfor stroke:PartI Pilotstudyof tissueplasminogenactivatoradministered within90 minutes.Stroke1992;23:632-640.
11. CanadianCooperativeStudy Group. A randomizedtrial of aspirin andsulfinpyrazone in threatenedstroke. N EnglJ Med1978;299:53-59.
12. CaplanLR, BrassLM, DeWittLD, et al. Transcranial Dopplerultrasound:Present status.Neurology 1990;40:696-700.
13. CaplanLR, SkillmanJ, OjemannR, et al. Intracerebral hemorrhagefollowingcarotidendarterectomy: A hypertensive complication.Stroke1978;9:681-687.
14. delZappaGJ, Poeck K, Pessin MS, et al. Recombinanttissue plasminogenactivatorin acute thromboticand embolicstroke.AnnNeuroI1992;32:7886.
evaluation mustbe available andimplemented to distinguishbetween ischemic and hemorrhagic stroke. Patientsandphysicians needto be awarethatstrokesymptomsindicate a medical emergency. The health-care systemmustbe ready to directpatientsto hospitals that areprepared to implement immediate diagnosis andtreatment.Ifthis canbe accomplished, a "brain attack"can beregarded with as muchurgency as a "heart attack"andstrokemorbidity andmortality will continue to fall.
COLOR SLIDES summarizing the tablesin this Consensus Statement are availablefor purchase by calling National StrokeAssociation at 1-800-STROKES.
To receive your complimentary SUbscriptionto Stroke:Clinical Updates", please return the enclosed envelope.
15. DukeRJ, BlochRF,Turpia AG. et al. Intravenous heparin for thepreventionof strokeprogressionin acutepartialstablestroke. AnnInternMed1986;105:825-828.
16. EuropeanCarotidSurgeryTrialists' Collaborative Group.MRC Europeancarotid surgerytrial: Interim results for symptomatic patients with severe(70-99%)or withmild (0-29%)carotid stenosis. Lancet1991;337:12351243.
17. FieschiC, ArgentinoC. Lenzi GL, et al. Clinicaland instrumentalevaluationof patientswith ischemic strokewithinthe first six hours.JNeurol Sci 1989;91:311-321.
18. GarrawayWM, WhisnantJP, Furlan Al, et at.The decliningincidenceofstroke.N EnglJ Med 1979;300:449-452.
19. Gent M, BlakelyJA, Easton OJ, et al.The CanadianAmericanticlopidinestudy(CATS)in thromboembolicstroke:Design,organizationandbaselineresults.Stroke1988;19:1203-1210.
20. HaleyEC Jr, KassellNF. Tomer JC. Failure of heparinto preventprogressionin progressingischemic stroke.Stroke 1988;19:10-14.
21. HallED, YonkersPA, McCall1M. BraughlerTht Enhancementofneurologicalrecovery and survival in experimental head injuryby the 21arninosteriod U74006F.a novel and potent inhibitorof iron-dependentlipid peroxidation. J Neurosurg 1988;68:456-461.
22. HankeyGJ, WarlowCP, Selar RJ. Cerebralangiographic risk in mildcerebrovascular disease.Stroke1990;21:209-222.
143
NSA CONSENSUSSTATEMENT
23. HankeyGJ, WarlowCP. Symptomaticcarotidischaemicevents:Safestand most cost effectiveway of selectingpatients for angiographybeforecarotid endarterectomy. Br MedJ 1990;300:1485-1491.
24. HarmsenP, TsipogianniA, WilhelmsenL. Stroke incidencerates wereunchanged,whilefatalityrates declinedduring 1971-1987in Goteborg,Sweden. Stroke1992;23:1410-1415.
25. Hart RG, CoullmI, Hart D. Early recurrentembolismassociatedwithnon-valvularatrial fibrillation:A retrospectivestudy.Stroke 1983;14:688693.
26. Ilass WK, EastonOJ.Tyelopidine, Platelets and Vascular Disease.NewYork:Springer-Verlag; 1993.
27. Heros RC. Surgicaltreatmentof cerebellar infarction. Stroke 1992;23:937938.
28. HerosRC, KistlerJP. Intracranialarterialaneurysms: An update. Stroke1983;14:628-631.
29. HerosRC, NelsonPB. Intracerebralhemorrhageaftermicrosurgicalcerebralrevascularization. Neurosurgery 1980;6:371-375.
30. Hier DB, BabcockOJ, Foulkes MA, et al.Influence of site on courseofintracerebral hemorrhage.J StrokeCerebrovasc Dis 1993;3:65·74.
31. Hermes IT, AustinJll, James G, ct al.Toward an optimal"antiplatelet"dose of aspirin:Preliminaryobservations. J StrokeCerebrovasc Dis1991;1:27·35.
32. Hunt RC. HessRN. Surgical risk as relatedto time of interventionin therepair of intracranial aneurysms.J Neurosurg 1968;28:1920-1968.
33. ItakuraT, KornalN, NakaiE, et al. Stereotactic evacuationof hypertensiveintracerebral hematomausing plasminogenactivator: Surgical techniquesand long-termresults. In Suzuki J, ed. AdvancesinSurgeryfor CerebralStokeNew York:Springer-Verlag; 1988:443-448.
34. JonesTIl, MorawetzRB, CrowellRM, ct al. 'Thresholds of focal cerebralischemiain awakemonkeys.J Neurosurg 1981;54:773-782.
35. KannoT, Sano H, ShinomiyaY. et al. Roleof surgeryin hypertensiveintracerebral hematoma: A comparativestudyof 305nonsurgicaland 154surgicalcases.J Neurosurg 1984;61:1091-1099.
36. KassellNl-, TomerJC. Aneurysmalrebleeding: A preliminaryreport fromthe cooperativeaneurysmstudy. Neurosurgery 1983;13:479-481.
37. Kassell NF,Tomer JC, HaleyEC Jr, et al. The international cooperativestudyon the timingof aneurysmsurgery.Part I: Overallmanagementresults.J Neurosurg, 1990;73:18-36.
38. KopitnikTA Jr, KaufmanHH.The future:Prospectsof innovativetreatmentof intracerebral hemorrhage.NeurosurgClln North Am1992;3:703.708.
39. MacdonellRAL,KalninsRt\f, DonnanGA. Cerebellarinfarctionnaturalhistory, prognosisand pathology.Stroke 1987;18:849-855.
40. MatsumotoK, HondoH, Tomida K. Aspirationsurgeryfor hypertensivebrain hemorrhagein the acute stage. In: Suzuki J, ed. AdvancesinSurgeryfor Cerebral Stroke.New York:Springer-Verlag; 1988:433-441.
41. McCormickPW.SpetzlerRF, BailesIE, et al. Thromboendarterectomy ofthe symptomaticoccludedintemal carotidartery. J Neurosurg1992;76:752·758.
42. McKissockW. RichardsonA,Taylor J. Primary intracerebralhaemorrhage: A controlled trial of surgicaland conservativetreatmentin180unselectedcases.Lancet 1961:2:221-226.
43. McKissockW, RichardsonA, WalshL. Spontaneous cerebellarhemorrhage: A study of 34 consecutive cases treatedsurgically. Brain1960;83:1·9.
44. MeyerFB, SundtTM Jr,Picpgras DG, et al. Emergencycarotidendarterectomy for patients with acutecarotidocclusionandprofoundneurological deficits. AnnSurg 1986;203:82·89 .
45. MeyerJS, HerndonRM, Gotoh F. Therapeuticthrombolysis.In: MillikanCII, SiekertRG, Whisnant JP, eds. Cerebrovascular Diseases,Philadelphia:Grune and Stratton; 1961;160-177.
46. MillikanCH.Anticoagulant therapyin cerebrovascular disease.In: Millikanell, SiekertRG, Whisnant JP, eds, Cerebrovascular Diseases, Philadelphia: Grune and Stratton; 1965:181·184.
47. MohadjerM,Eggert R, May J, MayfrankL. cr-guided stereotacticfibrinolysis of spontaneousand hypertensive cerebellarhemorrhage:Longtermresults.J Neurosurg 1990;73:217-222.
48. NACENTCollaborators. Beneficialeffectsof carotidendarterectomy insymptomaticpatients with high-gradecarotidstenosis. N EnglJ Med1991;325:445-453.
49. NorrisJW, Eisen AA, BranchCL.Problemsin cerebellarhemorrhageandinfarction. Neurology 1969;19:1043-1050.
SO. Petty GW, Wiebers DO, MeissnerI. TranscranialDopplerultrasonography: Clinicalapplicationsincerebrovasculardisease. MayoClinProc 1990;65:1350-1364.
51. PhillipponJ, Grob R, DagreauF, et al, Preventionof vasospasminsubarachnoid hemorrhage:A controlledstudywithnimodipine. ActaNeurochir 1986;82:110-114.
52. Pickard JO, MurrayGO, llIingwonhR, et al, Effect of oral nimodipineoncerebralinfarctionand outcomeafter subarachnoid haemorrhage.Britishaneurysmnimodipinetrial. Br MedJ 1989;298:636-642.
53. RothrockIF, Dittrich IIC, McAllenS, et al Acuteanticoagulationofcardiocrnbolic stroke andTIA. Stroke1989;20:730·734.
54 RothrockIF,lIart RG. Antithrombotic therapyin cerebrovasculardisease.AMIniMed 1991;115:885-895.
55. SpencerMP,Thomas GI, NichollsSC, SauvageLR. Detectionof middlecerebralartery emboli duringcarotidendarterectomy using transcranialDopplerultrasonography. Stroke 1990;21 :415-423.
56. Tarr RW, HechtST, HortonJA. Nontraurnatic IntraeranialHemorrhage.In: LatchawRE, ed, MRand cr Imagingof theIl ead, NeckandSpine,2nded, S1. Louis:Mosby, Year Book; 1991:267·299.
57. UnitedKingdomTransient IschemicAttackStudy Group (UK·TIA).Aspirintrial interimresults.Br MedJ 1988;296:316-320.
58. VerstrateM, WesslerS. Heparinsand oralanticoagulants.In Fuster V,VerstrateM, eds. Thrombosis inCardiovascular Disorders. Philadelphia:SaundersCo; 1992:121-140.
59. WallSO, Brant-Zawadzki M, JeffreyRH,et al, Highfrequencycrfindings within24 hours after cerebralinfarction. AmJRadial1982:138:307-311.
60. WaltersBB, OjcmannRG, HerosRC. Emergencycarotid endarterectomy.J Neurosurg 1984;66:817-823.
61. Yuhwcr, Crain MR, Loes OJ, etal. MRimagingof cerebral ischemia:Findingsin the rust 24 hours. AmJNeuroradioll991;12:621-629.
~.UoDal Stroke MsodaUon (SSA) Is. eet -rer-prcrn oraallluUon roundt.dIn1984 to reduce lbt.lncldcncc IDd Imp-el ofltrolLc throughprevention. b"ealmcD~ rthablUla.UoD. and research.
National Stroke Association. 8480 East Orchard Road. Suite 1000. Englewood,CO 80ll1-S0lS· (303) 771·1700. Fax (303) 771-1886ISSN 1049-7463. Copyright" 1993. All rights reserved.
144







