

SUPPORTIVE CAREMatti AaproMatti Aapro
Genolier

FOR MORE INFORMATIONwww.mascc.orgwww.mascc.org
www.qualityoflife.elsevierresource.com
www.afsos.org

• Supportive Care is the prevention andmanagement of the adverse effects of cancerand its treatment.
• This includes physical and psychosocial
Definition of Supportive Care
• This includes physical and psychosocialsymptoms and side effects across the entirecontinuum of the cancer experience includingthe enhancement of rehabilitation andsurvivorship.
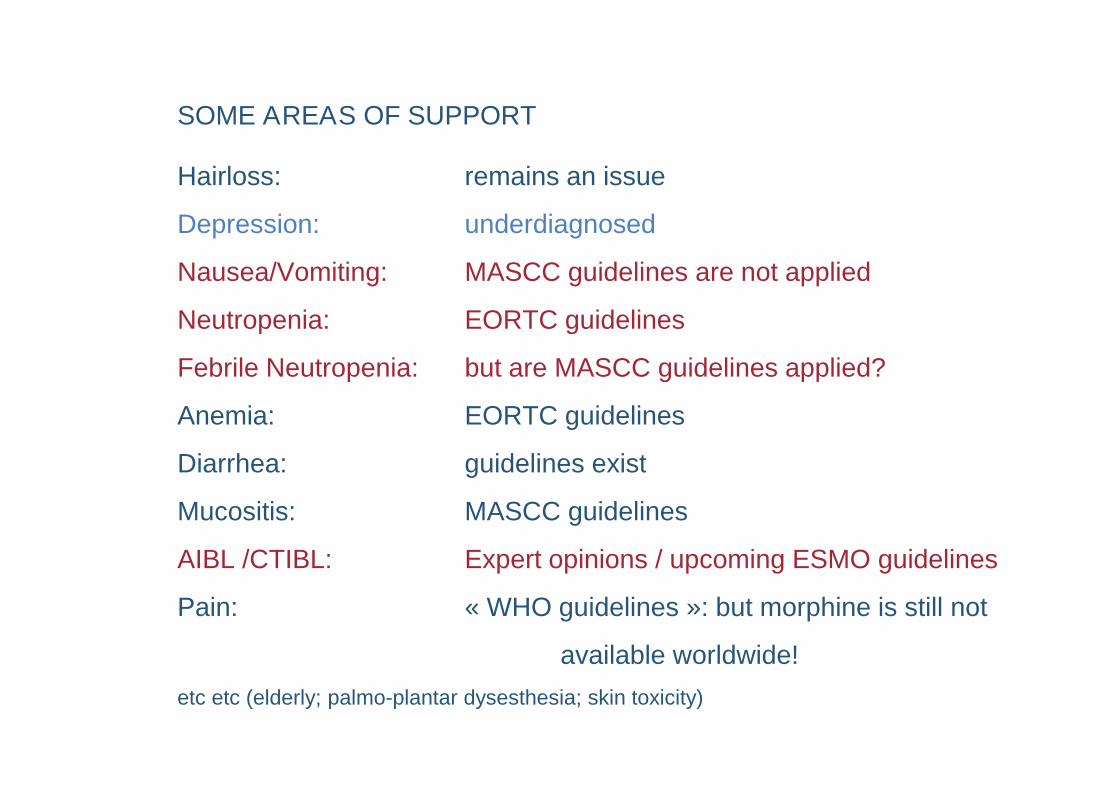
SOME AREAS OF SUPPORT
Hairloss: remains an issue
Depression: underdiagnosed
Nausea/Vomiting: MASCC guidelines are not applied
Neutropenia: EORTC guidelines
Febrile Neutropenia: but are MASCC guidelines applied?
Anemia: EORTC guidelines
Diarrhea: guidelines exist
Mucositis: MASCC guidelines
AIBL /CTIBL: Expert opinions / upcoming ESMO guidelines
Pain: « WHO guidelines »: but morphine is still not
available worldwide!
etc etc (elderly; palmo-plantar dysesthesia; skin toxicity)

Chosen chapters in Supportive Care
Why supportive / palliative care
The limits of futile treatment
G-CSFG-CSF
Antiemetics
Bone Health

ABOUT THE VALUE OF PROPER SUPPORTIVE AND PALLIATIVE CARE
Aapro M.S. EditorialAnn Oncol 2012See also Temel JS et alNEJM 2010; 363:733-42Zimmerman C et alLancet Oncol 14:219-227

INDICATORS OF SURVIVAL IN PHASE I STUDIESScore max 11 points[ECC 2013, Abs 1745].
Factors Points
Met sites ≥ 3 1
PS 1 1
LDH between 250 and 600 U/l 1
Hb < 6,2 mmol/l ( 110 g/l ) 1
Albuminemia < 35 g/l 2
LDH > 600 U/l 2
PS ≥ 2 3
Rotteveel K et al. Abstract 1745 ESMO 2013.

4 GROUPSMEDIAN SURVIVAL (MS) and MORTALITY D90
- Score ≥ 4: MS de 2,6 mths and D90 79%,- Score = 3: MS de 5,0 mths and D90 43%,- Score = 2: MS de 7,1 mths and D90 31%,- Score = 1: MS de 9,5 mths and D90 28%,- Score = 1: MS de 9,5 mths and D90 28%,- Score = 0: MS de 15,0 mths + D90 17%.
Rotteveel K et al. Abstract 1745 ESMO 2013.

The Facts
and my thoughts…

CASE ANNA
Anna is a healthy 68 years old patient with a history of recurrrent
urinary tract infections.
She is diagnosed with triple-negative breast cancer T2 N1(3/17)MO.
Adjuvant therapy with docetaxel / cyclophosphamide is planned.
What do you suggest?
1.Pegfilgrastim prophylaxis of FN
2.Filgrastim/lenograstim prophylaxis
3.Either one combined with a fluoroquinolone
4.No primary prophylaxis
5.Other choice

Febrile neutropenia
Chemotherapy for cancer is a cause of febrile neutropenia(FN: « fever « and less than 500 neutrophils )
FN is a high-risk situation for some and specially elderlypatients
G-CSF, not antibiotics, are the recommended prophylaxis G-CSF, not antibiotics, are the recommended prophylaxis

Hospitalized Cancer Patients with Febrile NeutropeniaMortality and Comorbidities
38.3
28.9
47.4
57.4
40
50
60
70
Documented infectionPresumed infection
Mort
alit
y(%
)
12 Kuderer et al. CANCER 2006;106:2258-66
1.2
6.7
12.9
23.8
4.9
14.7
28.9
0
10
20
30
0 1 2 3 >4Number of Major Comorbidities*
Mort
alit
y(%
)
*Major comorbidities are major organ dysfunction requiring diagnostic or therapeutic intervention,such as heart, lung, renal, or liver disease, diabetes mellitus, or anemia.

G-CSF supportive therapy reduces mortality:HR: 0.897 (95% CI, 0.857 to 0.938; p<0.001)
Greater mortality
reduction in:
larger trials
greater RDI
dose-densechemo
Lyman GH et al. J Clin Oncol 2010;28:2914–2924
chemo
More secondary
AML and MDS
RR: 1.92
AR: 0.41%
Updated Guidelines: 2011

PROPHYLACTIC APPROACH, NOT A REACTIVE ONE
20102010additions

And if FN hits?
De Narois et al: Management of Febrile Neutropenia:ESMO clinical practice guidelinesAnn Oncol 2010; 21:v252-v256 downloadable www.esmo.org
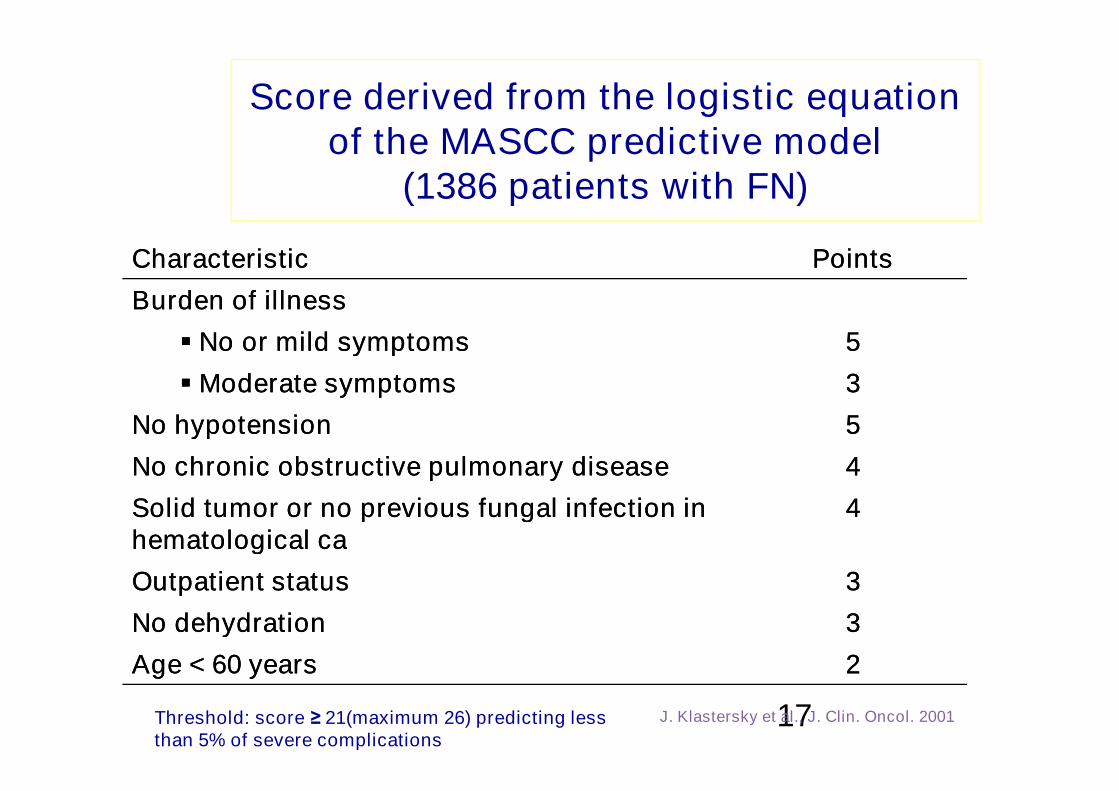
Score derived from the logistic equationof the MASCC predictive model
(1386 patients with FN)
CharacteristicCharacteristic PointsPoints
Burden of illnessBurden of illness
No or mild symptomsNo or mild symptoms 55
Moderate symptomsModerate symptoms 33
17J. Klastersky et al., J. Clin. Oncol. 2001
Moderate symptomsModerate symptoms 33
No hypotensionNo hypotension 55
No chronic obstructive pulmonary diseaseNo chronic obstructive pulmonary disease 44
Solid tumor or no previous fungal infection inSolid tumor or no previous fungal infection inhematological cahematological ca
44
Outpatient statusOutpatient status 33
No dehydrationNo dehydration 33
Age < 60 yearsAge < 60 years 22
Threshold: score ≥ 21(maximum 26) predicting lessthan 5% of severe complications

CASE ANNA
Anna is a healthy 68 years old patient with a history of recurrrent
urinary tract infections.
She is diagnosed with triple-negative breast cancer T2 N1(3/17)MO.
Adjuvant therapy with docetaxel / doxorubicin/ cyclophosphamide isplanned.
What do you suggest?
1. Pegfilgrastim prophylaxis of FN
2. Filgrastim/lenograstim prophylaxis
3. Either one combined with a fluoroquinolone
4. No primary prophylaxis
5. Other choice

CASE BIRGIT
Birgit is a 46 years old patient diagnosed with endocrine-responsive (ER 50% PgR 30) G3 Ki 67 30% HEr-2 neg (FISH)breast cancer T2 N0 MO.Adjuvant therapy with doxorubicin / cyclophosphamide followedby a taxane is planned. What do you USE as an acute-phaseantiemetic ?
1. (Fos)aprepitant + setron + corticosteroid
2. Palonosetron + corticosteroid
3. Setron + corticosteroid
4. Metoclopramide ( or similar ) + corticosteroid
5. Other choice

ANTIEMETICS
Nausea and vomiting (N/V) due tochemotherapy are unacceptable in the XXIcentury
Patients are at risk of renal and otherPatients are at risk of renal and othercomplications in case of N/V

Neurotransmitters/TreatmentsAssociated With Emesis
Histamine
Endorphins
Dopamine/DA RAs
Serotonin/5-HT3 RAs
Emetic reflex
GABA
Acetylcholine
Cannabinoids
Substance P/
NK-1 RAs
DA = dopamine; GABA = gamma-aminobutyric acid; NK = neurokinin; RAs = receptor antagonists.


ANTIEMETIC GUIDELINE CONSENSUS- Official Process Subscribed to by manyInternational Oncology Groups -
www.mascc.orgUpdated 2014 corrections to come
AND
Ann Oncol 2010; Supplt 5: v232-v243
AND
JSCC 2011

Aprepitant Drug Interactions
Should not be usedconcomitantly withPimozideTerfenadineAstemizoleCisapride
Caution withDocetaxelVinblastineVincristineIfosfamideother chemotherapy agents
metabolized primarily byCYP3A4 that were notstudied: oral vinorelbine;studied: oral vinorelbine;trabectedin
Based on and modifyingAprepitant package insert 2008
Oral dexamethasone dose should be decreased by50% when administered with aprepitant
Prothrombin time and INR may be decreased whenwarfarin is administered concomitantly with aprepitant
Not far from grapefruit juice or clarithromycinReview by Aapro and Walko, Annals of Oncology,2010

Potential Side Effects of Dexamethasone

M. Aapro,A. Fabi,F. Nolè,M. Medici,G. Steger,C. Bachmann,S. Roncoroni,and F. Roila
Double-blind, randomised, controlled study of theefficacy and tolerability of palonosetron plusefficacy and tolerability of palonosetron plusdexamethasone for 1 day with or withoutdexamethasone on days 2 and 3 in the preventionof nausea and vomiting induced by moderatelyemetogenic chemotherapy
Ann Oncol (2010) 21(5): 1083-1088
See also Celio et al, J Supp Care, 2010

MASCC/ESMO Antiemetic GuidelineMASCC/ESMO Antiemetic GuidelineSummary of Acute and Delayed PreventionSummary of Acute and Delayed Prevention
Emeticrisk group
Risk(% pts)
Acute prevention Delayed prevention
High >90%5-HT3 RA
+ DEX + (fos)aprepitantDEX + aprepitant
AC combinations -5-HT3 RA *
+ DEX + (fos)aprepitantaprepitant
* If a NK-1 RA is not available then palonosetron is the preferred5-HT3 RA also in AC regimens
www.mascc.org
Moderate 30-90% Palonosetron + DEX DEX
Low 10-30% single agent (DEX, 5-HT3 DRA) No routine prophylaxis
Minimal <10% No routine prophylaxis No routine prophylaxis
Recommended 5-HT3 RAs: Palo, Grani, Onda, Dola oral, TropiDEX, dexamethasone; AC, anthracycline-cyclophosphamide DRA: dopamine receptor antagonistAprepitant in delayed phase depends on (fos)apretitant use in acute phase
Emetic
risk group
Risk
(% pts)Acute prevention* Delayed prevention
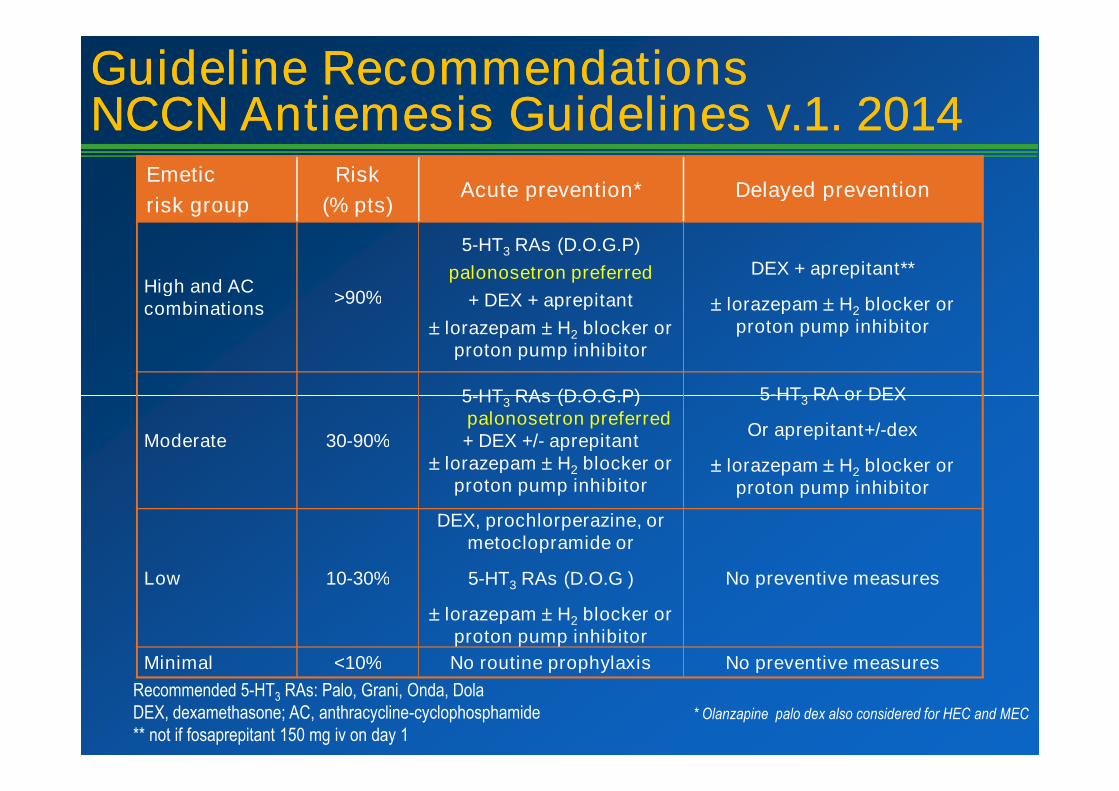
High and ACcombinations
>90%
5-HT3 RAs (D.O.G.P)
palonosetron preferred
+ DEX + aprepitant
lorazepam H2 blocker orproton pump inhibitor
DEX + aprepitant**
lorazepam H2 blocker orproton pump inhibitor
5-HT3 RAs (D.O.G.P) 5-HT3 RA or DEX
Guideline RecommendationsGuideline RecommendationsNCCN Antiemesis Guidelines v.1. 2014NCCN Antiemesis Guidelines v.1. 2014
Moderate 30-90%
5-HT3 RAs (D.O.G.P)palonosetron preferred+ DEX +/- aprepitant
lorazepam H2 blocker orproton pump inhibitor
5-HT3 RA or DEX
Or aprepitant+/-dex
lorazepam H2 blocker orproton pump inhibitor
Low 10-30%
DEX, prochlorperazine, ormetoclopramide or
5-HT3 RAs (D.O.G )
lorazepam H2 blocker orproton pump inhibitor
No preventive measures
Minimal <10% No routine prophylaxis No preventive measures
Recommended 5-HT3 RAs: Palo, Grani, Onda, DolaDEX, dexamethasone; AC, anthracycline-cyclophosphamide** not if fosaprepitant 150 mg iv on day 1
* Olanzapine palo dex also considered for HEC and MEC
A LOOK INTO THE NOT TOO DISTANT FUTURE
ROLAPITANT: oral and iv forms under development
NETUPITANT
Various formulations of existing agents

Efficacy and safety of NEPA, a fixed-dose combination of netupitantand palonosetron, in preventing chemotherapy-induced nausea and
vomiting (CINV) in patients receiving moderately emetogenicchemotherapy (MEC)
M. Aapro1, G. Rossi2,G. Rizzi2, M. E. Borroni2, V. Lorusso3, M. Karthaus4,S. Grunberg5
Study Design:•Phase 3, multinational, randomized, double-blind study in chemotherapy-naïve patientsundergoing AC chemotherapyundergoing AC chemotherapy
•Patients randomized to receive one of the following prior to chemotherapy on Day 1 :
Oral NEPA + Oral DEX 12 mg
(NEPA = NETU 300 mg + PALO 0.50 mg)
Oral PALO 0.50 mg + Oral DEX 20 mg
N = 1455
Randomized1:1
Presented in part at MASCC, ASCO and ECCO 2013

• NEPA was superior to PALO for complete response in the delayed 25-120h (77% vs70%, respectively), acute 0-24h (88% vs 85%, respectively) and for the secondaryendpoints in the overall phase:
Results: Complete Response in the Delayed (Primary Endpoint),Acute and Overall (Key Secondary Endpoints)
Overall (0-120h) % PatientsNEPA
(N=724)PALO
(N=725)
Complete ResponseComplete Protection
74.3*63.8*
66.657.9Complete Protection
No EmesisNo Significant Nausea
63.8*79.8*74.6*
57.972.169.1
• NEPA showed superior complete response rates compared with PALO during theacute, delayed, and overall phases following MEC
• NEPA was superior to PALO for secondary endpoints• NEPA was well tolerated with a similar safety profile to PALO
Conclusions:
* p-value <0.05

CASE BIRGIT
Birgit is a 46 years old patient diagnosed with endocrine-responsive (ER 50% PgR 30) G3 Ki 67 30% HEr-2 neg (FISH)breast cancer T2 N0 MO.Adjuvant therapy with doxorubicin / cyclophosphamide followedby a taxane is planned. What do you USE as an acute-phaseantiemetic ?
1.Aprepitant + setron + corticosteroid
2.Palonosetron + corticosteroid
3.Setron + corticosteroid
4.Metoclopramide ( or similar ) + corticosteroid
5.Other choice
CASE CHIARA
Chiara is a 71 years old patient who exercises daily ANDsmokes a pack/day. She has endocrine-responsive ( ER 50%PgR 30%) G2 Ki 67 15% HEr-2 neg (FISH) breast cancer T1N0 MO. Adjuvant therapy with an aromatase inhibitor is plannedand her BMD score is T-1.8. What would you suggest (assumethere is no restriction)
1.Calcium + vitD + bisphosphonate / denosumab
2.Calcium + vitD
3.Calcium + vitD + zoledronic acid every 6 months
4.Use tamoxifen
5.Tamoxifen +Calcium + vitD + oral bisphosphonate

BONE
Osteopenia/osteoporosis is prevalent among many male andfemale cancer patients
Bisphosphonates (BPs) and denosumab are established agentsfor supportive care in case of bone metastases
BPs might be more than supportive care?BPs might be more than supportive care?( on going studies with denosumab )

UPDATE PLANNED FOR 2010

7
16
2
ABCSG-12 (62 mo)
free
su
rviv
al,
%
ZOL vs no ZOL
Fir
st
even
tp
er
pati
en
t,n
Death without prior recurrence
Secondary malignancy
Contralateral breast cancer
Distant recurrence
Locoregional recurrence
ZOL
NO-ZOL
100
90
80
70
60
120
100
80
56
29
Time since randomization, months
Dis
ease-f
ree
su
rviv
al,
%
(n = 903)
No ZOL
(n = 900)
ZOL
Fir
st
even
tp
er
pati
en
t,n
NO-ZOL
HR = 0.68P = 0.008
Median follow-up = 62 mo
Gnant M, et al. J Clin Oncol 28:15s, 2010 (suppl; abstr 533).
60
50
40
30
20
10
0
12 24 36 48 60 72 84 96 1080
60
40
20
0
44
6
110
15
No-ZOL (110 events) vs. ZOL (76 events)Absolute Difference = 34

Myeloma IX (MRC) –ZOL Improved OS and PFS vs CLOa
ZOL significantly reduced the relative risk of death by 16% vs CLO(HR = 0.842; 95% CI = 0.736, 0.963; P = .0118)Median survival improved by 5.5 months (50 vs 44.5 months)
Riskreduction P value
0.842OS
Abbreviations: CLO, clodronate; OS, overall survival; PFS, progression-free survival; ZOL,zoledronic acid.a Cox model adjusted for chemotherapy, and minimization factors.
Hazard ratio (ZOL versus CLO)
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2
.01180.842
16%
In favor of ZOL In favor of CLO
OS
.017912%0.883
PFS
Morgan GJ, et al. J Clin Oncol 28:15s, 2010 (suppl; abstr 8021).

Denosumab in Early Adjuvant BC: ABCSG-18 & D-CARE Trials
ABCSG-18:
• Primary Endpoint: Rate of 1st clinical fracture
• Secondary Endpoints: Bone metastasis-free survival (BMFS), DFS, OS
Placebo SC q6 mo3,460 EBCpts R
Studyduration:
96 monthsDmab 60 mg SC q6 mopts R96 months
D-CARE:
• Primary Endpoint: Bone metastasis-free survival
Placebo 120mg SC monthly x 6 mo, q 3 mo for 4.5 yrs
Dmab 120mg SC monthly x 6 mo, q 3 mo for 4.5 yrs
4,500 EBCpts R
Treatment duration 5 yrs
http://www.abcsg.org/trials/trial18.html, http://clinicaltrials.gov/ct2/show/NCT01077154?term=d-care&rank=1

T-score < –2.0Any 2 of the following risk factors:
• T-score < –1.5
• Age > 65 years
• Low BMI (< 20 kg/m2)
• Family history of hip fracture
• Personal history of fragility fracture after age 50
• Oral corticosteroid use of > 6 months
T-score ≥ –2.0,No risk factors
Recommendations for Women With Breast Cancer Initiating AITherapyRecommendations for Women With Breast Cancer Initiating AITherapy
• Smoking (current and history of)
Monitor risk statusand BMD at
1 year
Bisphosphonate*
calcium and vitamin Dsupplements
EXERCISE
Monitor BMD…every 1-2 years if
oral BPs
Calcium and vitamin Dsupplements
EXERCISE
*≥ 10% drop in BMD (4-5% if osteorotic )
should trigger treatment. Use lowest T-score from 3 sites.
Adapted from Hadji P, et al. in press Annals of Oncology 2011
• *DENOSUMAB is a potential option for somepatients. Oral health precautions needed for BPsand denosumab
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
Effects Of Bisphosphonate Treatment OnRecurrence And Cause-specific Mortality
In Women With Early Breast Cancer:A Meta-analysis Of Individual Patient Data
From Randomised Trials
This presentation is the intellectual property of the EBCTCG. Contact [email protected] for permission to reprint and/or distribute.
R Coleman, M Gnant, A Paterson, T Powles, G von Minckwitz,
K Pritchard, J Bergh, J Bliss, J Gralow, S Anderson, D Cameron,
V Evans, H Pan, R Bradley, C Davies, R Gray.
Early Breast Cancer Trialists’ Collaborative Group(EBCTCG)’s Bisphosphonate Working Group.
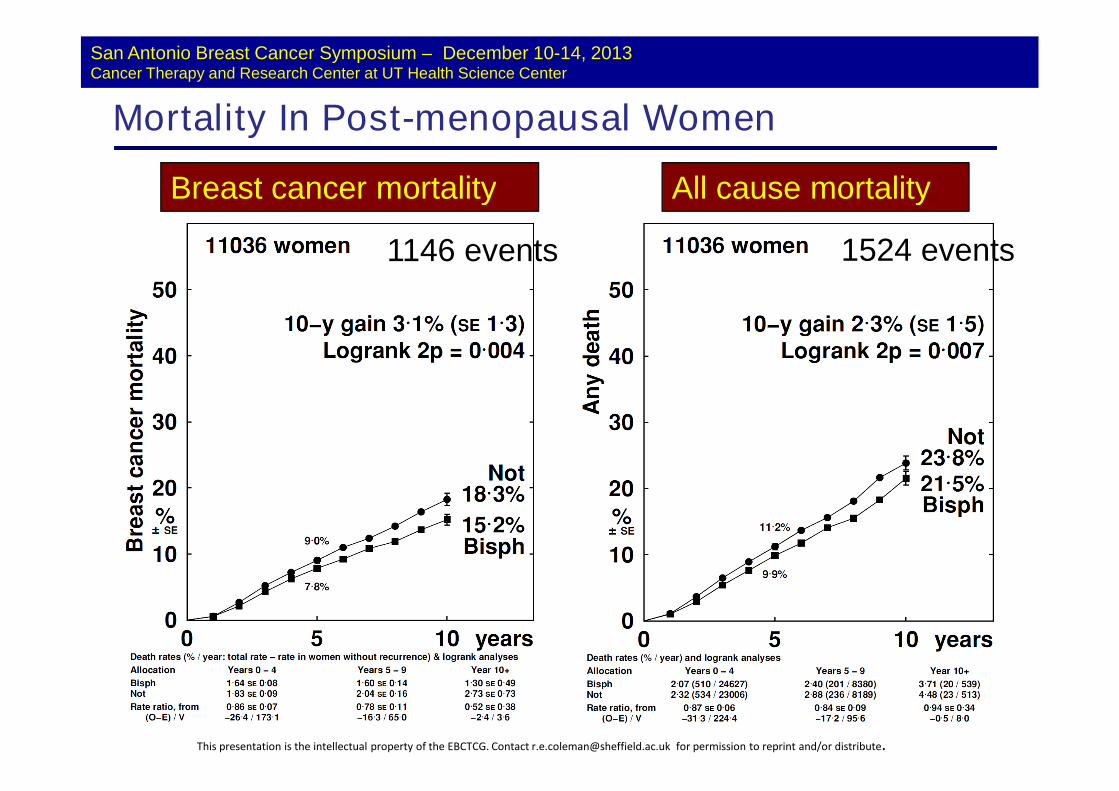
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
Mortality In Post-menopausal Women
Breast cancer mortality All cause mortality
1146 events 1524 events
This presentation is the intellectual property of the EBCTCG. Contact [email protected] for permission to reprint and/or distribute.


CASE CHIARA
Chiara is a 71 years old patient who exercises daily AND smokes apack/day. She has endocrine-responsive ( ER 50% PgR 30%) G2 Ki 6715% HEr-2 neg (FISH) breast cancer T1 N0 MO. Adjuvant therapy withan aromatase inhibitor is planned and her BMD score is T-1.8. Whatwould you suggest (assume there is no restriction), besides exercise
1. Calcium + vitD + bisphosphonate / denosumab1. Calcium + vitD + bisphosphonate / denosumab
2. Calcium + vitD
3. Calcium + vitD + zoledronic acid every 6 months
4. Use tamoxifen
5. Tamoxifen +Calcium + vitD + oral bisphosphonate

FOR MORE INFORMATIONwww.mascc.orgwww.mascc.org
www.qualityoflife.elsevierresource.com
www.afsos.org







