

This article was downloaded by: [Mount Royal University]On: 12 May 2013, At: 03:19Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office:Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Cognitive NeuropsychiatryPublication details, including instructions for authors and subscriptioninformation:http://www.tandfonline.com/loi/pcnp20
Symptomatology and social inference: Atheory of mind study of schizophrenia andpsychotic affective disorderDominic Marjoram a , Clare Gardner b , Jonathan Burns c , Patrick Miller a ,Stephen Lawrie a & Eve Johnstone aa Royal Edinburgh Hospital, Edinburgh, UKb Nottingham City Hospital, Nottingham, UKc University of KwaZulu-Natal, Durban, South AfricaPublished online: 10 Sep 2010.
To cite this article: Dominic Marjoram , Clare Gardner , Jonathan Burns , Patrick Miller , Stephen Lawrie &Eve Johnstone (2005): Symptomatology and social inference: A theory of mind study of schizophrenia andpsychotic affective disorder, Cognitive Neuropsychiatry, 10:5, 347-359
To link to this article: http://dx.doi.org/10.1080/13546800444000092
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantialor systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that thecontents will be complete or accurate or up to date. The accuracy of any instructions, formulae,and drug doses should be independently verified with primary sources. The publisher shall notbe liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever orhowsoever caused arising directly or indirectly in connection with or arising out of the use of thismaterial.

Symptomatology and social inference: A theory of
mind study of schizophrenia and psychotic affective
disorder
Dominic Marjoram
Royal Edinburgh Hospital, Edinburgh, UK
Clare Gardner
Nottingham City Hospital, Nottingham, UK
Jonathan Burns
University of KwaZulu-Natal, Durban, South Africa
Patrick Miller, Stephen M. Lawrie, and Eve C. Johnstone
Royal Edinburgh Hospital, Edinburgh, UK
Introduction. There is evidence that certain patients with schizophrenia havedeficits in theory of mind (ToM) capabilities. It is, however, unclear whether theseare symptom or diagnosis-specific.Methods. A ToM hinting task was given to 15 patients with a DSM-IV diagnosis ofschizophrenia, 15 patients with affective disorder and 15 healthy controls. Severityof the current psychopathology was measured using the Krawiecka standardisedscale of psychotic symptoms (Krawiecka, Goldberg, & Vaughan, 1977); IQ wasestimated via the Ammons and Ammons Quick Test (Ammons & Ammons, 1962).Results. The group with schizophrenia performed significantly worse than theaffective and control groups. Poor performance on the hinting task was found to besignificantly related to the presence of positive symptoms (instead of negativeones) and specifically related to delusions and hallucinations. These findingsremained when covariance for potentially confounding variables was applied.Conclusions. Individuals with high levels of delusions and hallucinationsperformed significantly worse on this ToM task, regardless of diagnosis, implyingToM impairment is not exclusive to schizophrenia but is evident in other forms ofpsychosis. Between-group analyses showed the schizophrenia group had asignificicantly poorer performance on this task than the others.
Correspondence should be addressed to Dominic Marjoram, University Department of Psy-
chiatry, Kennedy Tower, Royal Edinburgh Hospital, Morningside Park, Edinburgh EH10 5HF, UK;
e-mail: D.K.S. [email protected]
# 2005 Psychology Press Ltd
http://www.tandf.co.uk/journals/pp/13546805.html DOI:10.1080/13546800444000092
COGNITIVE NEUROPSYCHIATRY
2005, 10 (5), 347±359
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

Theory of mind
The term theory of mind (ToM), sometimes referred to as mind-reading (Baron-
Cohen, 1995) and mentalising (Corcoran, Cahill, & Frith, 1997), was first coined
by Premack and Woodruff (1978) and refers to the ability of individuals to
correctly determine the intentions and behaviour of others. This is a necessary
skill for successful complex social interactions and it is known to be compro-
mised in autism and schizophrenia (Abu-Akel, 2003). In schizophrenia, the
degree of impairment of ToM fluctuates in relation to psychotic episodes and
severity of particular symptoms. Individuals with formal thought disorder,
paranoid delusions, and chronic negative symptoms perform the worst on ToM
tasks. Frith (Frith 1992) hypothesised that positive symptomatology could result
in an impairment in ``metarepresentation'', this being the ability to represent
abstract cognitive processes about oneself and others.
Using the Hinting Task, Corcoran, Mercer, and Frith (1995), found symptom-
specific findings consistent with Frith's (1992) model. In Corcoran's original
study, patients with schizophrenia and paranoid delusions and related positive
features, and also those with negative features had the greatest difficulty with the
hinting task. The present study aims to develop the hinting task. The major
difference between the present study and that of Corcoran et al. (1995) is that in
Corcoran's original study the psychiatric controls did not have psychotic illness.
The study of ToM deficits in psychiatric disorders other than schizophrenia is
currently a sparsely investigated area. Doody, Gotz, Johnstone, Frith, and Owens
(1998) had 12 patients with nonpsychotic affective disorder as one of their
experimental groups and found no observed ToM deficits among them. Kerr,
Dunbar, and Bentall (2003) exclusively studied nonpsychotic bipolar groups
against healthy controls and found impaired ToM performance in symptomatic
(both manic and depressed) bipolars. Drury, Robinson, and Birchwood (1998)
had a group of 10 deluded psychotic individuals (the majority of who were
schizoaffective) and 12 nonpsychotic depressed patients and both groups sig-
nificantly outperformed a schizophrenia group on ToM tasks.
The aims of this study were to compare performance on a ToM task in
patients with affective psychoses and healthy controls, with that of patients with
schizophrenia, to test the hypothesis that a deficit in ToM skills is associated
with particular psychotic symptoms (specifically delusions and hallucinations),
regardless of diagnosis.
METHODS
Participants
Fifteen people with a DSM-IV diagnosis of schizophrenia and 15 with DSM-IV
bipolar disorder or major depressive illness (seven of which were bipolar and the
remaining eight were classified as severe depressive illness) were recruited. All
348 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

were aged 18±60 years. These patients were drawn from inpatients of an acute
psychiatric ward, outpatients, and attendees of the day hospital at the Royal
Edinburgh Hospital. All participants gave written informed consent to partici-
pate in the study, which was approved by the local hospital ethical committee.
The current level of overall intellectual functioning was estimated using the
Quick Test (Ammons & Ammons 1962). In addition, a control group of 15
healthy volunteers were studied, derived from staff of the Department of Psy-
chiatry. Individuals with any form of autistic spectrum disorder or head injury
were excluded.
Demographic characteristics of both subjects and controls are shown in Table
1 and the patient medications are detailed in Table 2.
To take account of current symptomatology, patients were also assessed using
a standardized scale for rating chronic psychotic patients (Krawiecka et al., 1977).
Scores on a 5-point scale are assigned to symptoms experienced over the previous
week. Ratings were given on a 5-point scale (where 0 = absent, 1 = mild, 2 =
moderate, 3 = Marked, 4 = severe) for coherently expressed delusions, hallu-
cinations, incoherence/irrelevance of speech, and incongruity giving a maximal
possible score of 16 for positive symptoms. Likewise, negative symptoms were
rated for poverty of speech and flattened affect giving a maximal possible score of
8 and the nonspecific symptoms of depression, anxiety, and psychomotor
retardation were assessed giving a possible maximal score of 12.
In order to look closely at the positive symptomatology of delusions and
hallucinations and to see what effect these had on ToM capabilities, the Kra-
wiecka scores for these were used in the following ways: (1) Presence of
delusions against performance: patients were divided into those scoring 0 and 1
(none to low) and those scoring 2±4 (moderate to severe). (2) Presence of
hallucinations against performance: likewise, those scoring 0±1 and those
scoring 2±4.
The Hinting Task. The task comprises 10 short passages involving two
characters, and each scenario ended with one of the characters dropping a very
obvious hint. The subject is then asked what the character really meant when he/
she said this. An appropriate response is given a score of 2 and the interviewer
TABLE 1Demographic details of the subject groups: Means and (standard deviations)
Group n (m:f) Age IQ
Duration of
illness (yrs)
Schizophrenic 15 (13:2) 28.3 (8.2) 96.5 (10.0) 11.3 (5.1)
Affective 15 (6:9) 41.7 (9.7) 101.8 (10.8) 17.3 (7.4)
Healthy controls 15 (10:5) 34.3 (12.7) 106.0 (9.7)
THEORY OF MIND AND PSYCHOSIS 349
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

proceeds on to the next story. However, if the subject fails to give an appropriate
response (e.g., by simply paraphrasing what was said and thus using no infer-
ential skills), a further sentence is added to the story containing an even more
obvious hint. Then the subject is asked what the character wants the other one to
do. A successful response is given a score of 1 whilst a score of 0 is given for an
inappropriate one. Some of the patients (7 schizophrenic and 8 affective) and
controls (9) had the Corcoran 10 hinting tasks and the remainder did the task of
new hinting sentences devised for this study (the Gardner tasks). All hinting
items were read aloud to the subjects, and were repeated as required, to ensure
adequate encoding of the information presented and overcome the poor prose
recall associated with schizophrenia (Shallice et al., 1994). Furthermore, in order
to reduce the potential memory load of the task, a sheet containing all the tasks
was placed in front of the subjects for them to read if they so desired. The 10
new hinting task items are in the Appendix. These were selected, in consultation
with Professor Chris Frith, from a pool of 20 devised for consideration.
Statistical analysis. Data analysis was carried out using SPSS for Windows
Version 11.0. Mean Hinting Task scores were compared between groups with an
ANOVA and post hoc Tukey HSD. Relations of delusions and hallucinations
and the Krawiecka totals for positive and negative symptoms were then
examined with multiple regression with current IQ, age, sex, type of task
(Corcoran or present), and medication dose as covariates.
RESULTS
Diagnosis
There was a significant effect of diagnosis in terms of performance on the
hinting task (F = 3.27, p < .05). Using Tukey's HSD test, the schizophrenia
group performed less well than either the controls or patients with affective
TABLE 2Medication details of the patient groups
Medication
Schizophrenics
(n = 15)
Affectives
(n = 15)
Typical antipsychotic only 4
Typical antipsychotic + Anticholinergic 5
Atypical antipsychotic only 5
Atypical antipsychotic + Anticholinergic 1
Antidepressant only/antidepressant + other
nonantipsychotic medicine
9
Antidepressant + Typical antipsychotic 5
Antidepressant + atypical antipsychotic 1
350 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

disorder (p < .0001). There was no significant difference in performance
between these latter two groups (Table 3).
It is, however, clear that the groups differ in terms of IQ, though both are well
within the normal range. There is also a marked difference with respect to age
and sex distributions. Given these variables, multiple regression was performed,
with allowances made for variations in type of test given, age, sex, and IQ. The
difference in performance between schizophrenics and controls was still highly
significant (p < .001). The variables of age, sex and IQ were then analysed
against ToM performance and it was found that none of these had a significant
affect.
However, when data were analysed in terms of whether subjects received the
original (Corcoran-devised) or the newly developed hinting task (Gardner-
devised), via an independent samples t-test, it appeared that the latter was more
difficult; giving a mean of 16.8 (SD = 2.8, n = 21) in comparison to a mean of
18.3 (SD = 1.6, n = 24) for the original test (p < .005). There was, however, no
significant task type by group interaction.
Symptoms
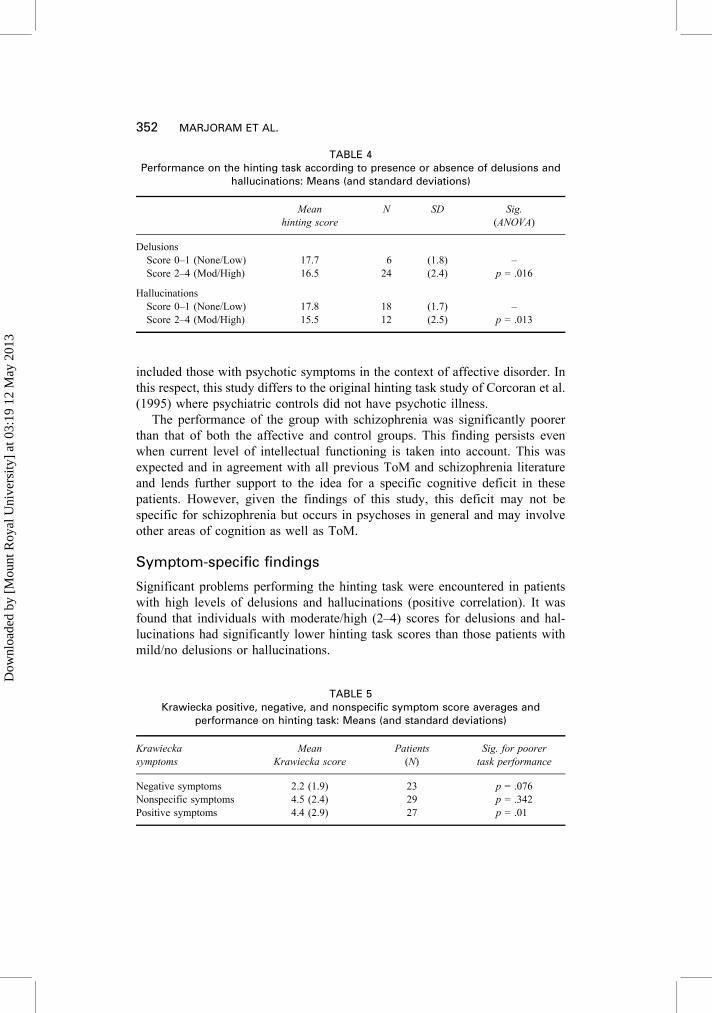
When data were analysed using scores from the Krawiecka 5-point scale for
both the schizophrenia and affective disorder patients it was found, as shown in
Table 4, that poor performance by patients was significantly associated with the
presence of both moderate to severe delusions and hallucinations, regardless of
diagnostic group. No significant group effect over and above symptom effect
was found.
Further investigation via multiple regression analysis, allowing for age, sex,
type of hinting test, and IQ, showed a significant relationship between positive
symptoms and performance on the hinting tasks (p = .01, beta-value of 7.558)
as shown in Table 5.
CONCLUSIONS
The major finding of this study is that there was an observed deficit in ToM
skills on this task of simple social inference that was associated with particular
psychotic symptoms. This was not specific to patients with schizophrenia, but
TABLE 3Performance on the hinting task between the groups: Means (and standard deviations)
Schizophrenics
(n = 15)
Affectives
(n = 15)
Controls
(n = 15)
Hinting score 15.5 (2.2) 18.2 (1.7) 19.2 (1.1)
THEORY OF MIND AND PSYCHOSIS 351
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3
included those with psychotic symptoms in the context of affective disorder. In
this respect, this study differs to the original hinting task study of Corcoran et al.
(1995) where psychiatric controls did not have psychotic illness.
The performance of the group with schizophrenia was significantly poorer
than that of both the affective and control groups. This finding persists even
when current level of intellectual functioning is taken into account. This was
expected and in agreement with all previous ToM and schizophrenia literature
and lends further support to the idea for a specific cognitive deficit in these
patients. However, given the findings of this study, this deficit may not be
specific for schizophrenia but occurs in psychoses in general and may involve
other areas of cognition as well as ToM.
Symptom-specific findings
Significant problems performing the hinting task were encountered in patients
with high levels of delusions and hallucinations (positive correlation). It was
found that individuals with moderate/high (2±4) scores for delusions and hal-
lucinations had significantly lower hinting task scores than those patients with
mild/no delusions or hallucinations.
TABLE 4Performance on the hinting task according to presence or absence of delusions and
hallucinations: Means (and standard deviations)
Mean
hinting score
N SD Sig.
(ANOVA)
Delusions
Score 0±1 (None/Low) 17.7 6 (1.8) ±
Score 2±4 (Mod/High) 16.5 24 (2.4) p = .016
Hallucinations
Score 0±1 (None/Low) 17.8 18 (1.7) ±
Score 2±4 (Mod/High) 15.5 12 (2.5) p = .013
TABLE 5Krawiecka positive, negative, and nonspecific symptom score averages and
performance on hinting task: Means (and standard deviations)
Krawiecka
symptoms
Mean
Krawiecka score
Patients
(N)
Sig. for poorer
task performance
Negative symptoms 2.2 (1.9) 23 p = .076
Nonspecific symptoms 4.5 (2.4) 29 p = .342
Positive symptoms 4.4 (2.9) 27 p = .01
352 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

When the Krawiecka et al. (1977) scores for positive and negative symptoms
were compared through regression analysis, positive symptoms were found to be
highly significantly associated with lower scoring on the hinting task. As far as
negative symptoms were concerned, there was no significant association but
there was a trend (p = .076) for higher symptom scores to be associated with
lower hinting task scores as was found in the original Corcoran study.
Antipsychotic medication dose at time of testing was recorded for each
patient and using standard published tables (Atkins, Burgess, Bottomly, &
Riccio, 1997; Woods, 2002) was converted into daily chlorpromazine equivalent
dosage. No significant correlation was found between this measure and the
hinting task. Antidepressant dosage was also recorded and was graded as either a
low dose [if the daily dose was less than or equal to half the British National
Formulary (BNF) (2002) recommended daily dosage] or a high dose (if the daily
dose was greater than half the BNF recommended daily dosage). The biserial
correlation with the hinting task performance was also found to be non-
significant although there was a slight trend (p = .063) implying the greater the
dose the better the performance on the task.
It may be argued that since the development of schizophrenia occurs during
adolescence or early adulthood, and that ToM skills are acquired in childhoodÐ
generally by the age of four years (Leslie, 1987), it is likely that such patients
developed mentalising skills to a normal level before becoming compromised by
the subsequent onset of the illness. If this were so, these patients would be
accustomed to making social inferences, and would continue to do so, appar-
ently unaware that their judgements are incorrect. This may also apply to those
individuals with affective disorder who had significantly impaired ToM
performance.
Metarepresentation
The finding for positive symptomatology in general and specifically delusions
and hallucinations being significant for poor performance on the hinting task
supports Frith's (1992) metarepresentation theory. Metarepresentation is the
ability to represent both one's own mental state and those of others, in this way,
Frith's theory views schizophrenia as a disorder of the representation of mental
states.
Individuals with schizophrenia who have predominately negative symptoms
can be thought as having a ToM deficit in that they lack representational
understanding of mental states. However, in individuals with positive symptom
schizophrenia there is a theory of mind impairment where over attribution
of mental states occurs: This has been labelled as a ``hyper-theory of mind''
(Abu-Akel, 1999, 2003; Abu-Akel & Bailey, 2000).
Using this hyper ToM concept, a mental state impairment continuum can be
envisaged, as described by Abu-Akel and Bailey (2000): The first variety of
THEORY OF MIND AND PSYCHOSIS 353
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

ToM impairment involves having no representational understanding of mental
states; the second involves having representational understanding of mental
states, but (due to a reality bias), a deficit in application of this understanding;
the third variety involves representational understanding of mind but over
attribution of mental states or over generation of hypotheses about mental life
(such as paranoid delusions).
How positive symptoms, particularly those of delusions and hallucinations,
actually interfere with ToM capabilities is not known and it remains to be
elucidated whether there is a special relationship between mentalising cap-
abilities and symptoms (Frith, 2004).
State vs. trait
Whether compromised ToM function in individuals is a state effect that fluc-
tuates with symptom severity has been studied by incorporating a remission
group into the experimental design of several studies, allowing psychotic and
nonpsychotic individuals with the same disorder to be compared. Corcoran et al.
(1995, 1997) and Frith and Corcoran (1996) found that there was no sig-
nificantly impaired ToM performance in the remission groups compared with
the control groups. Drury et al. (1998) used a novel approach of testing a
schizophrenia group in an acute phase and in remission, against a nonschizo-
phrenia psychosis group and a depressed group. There were significant differ-
ences between the schizophrenia group in the acute phase and the other groups
on a second order ToM task; however these differences disappeared in remis-
sion. However, Herold, Tenyi, Lenard, and Trixler (2002) found contrary results,
in that their schizophrenia group in remission did perform significantly worse
than the control group. These studies used different ToM tasks, and had dif-
ferences in group sizes, as well as varying average lengths of patient illness and
medication duration.
The potential alternative to a transient state effect which fluctuates with
symptom severity is the possibility that the observed ToM deficits are a trait
effect, underpinned by a genetic predisposition to schizophrenia. This theory has
been investigated by testing relatives of individuals with schizophrenia on ToM
tasks: Wykes, Hamid, and Wagstaf (2001) found siblings of people with schi-
zophrenia to perform significantly worse than control participants on ToM tasks.
Janssen, Krabbendam, Jolles, and Van Os (2003) found first degree relatives to
perform better than the schizophrenia group but worse than the control group on
the hinting task.
These findings suggest the possibility that in some forms of schizophrenia
there is a failure of ToM capacities to fully develop and this could be a precursor
to the disorder, and could at least potentially be a diagnostic marker for those at
enhanced risk.
354 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

Type of Hinting Task administered
As mentioned previously, there were two sources of the 10 hinting tasks given to
subjects. The original 10 tasks used by Corcoran et al. (1995) and a new set of
10 (see Appendix) written specifically for this project. It was decided to give
subjects all of one set as opposed to a mixed set to allow for statistical analysis
in order to see whether the two tasks could be used interchangeably in future
studies or needed to be kept separate due to different degrees of difficulty. It was
found that the Gardner tasks were in fact significantly harder than the original
Corcoran ones (means of 18.3 vs. 16.8, respectively). This particular study is a
pilot study for a larger planned study that will be looking at a selection of
clinical subgroups. These will include individuals at high risk of schizophrenia
for genetic reasons (Edinburgh High Risk Cohort) and schizotypal individuals
with mild learning disability (comorbids cohort). The mild LD group may be
able to perform the easier sentence test. Likewise, a harder set of hinting sen-
tences will be able to help limit the ceiling effect in adult controls and could
perhaps be used in conjunction with easier sentences to produce a graded dif-
ficulty hinting task.
Role of IQ
The extent to which IQ plays a role in the understanding of ToM remains to be
fully elucidated. An earlier study found that out of several schizophrenic sub-
groups, only in paranoid patients were there difficulties in understanding the
ToM tasks associated with lower IQ. The authors took this as an implication that
those paranoid patients with higher IQs could possibly compensate ToM deficits
by solving the tasks using general capacities (Pickup & Frith, 2001). Doody et
al. (1998) found that schizophrenic patients with comorbid learning disability
performed worst on ToM tasks and interpreted this as a possible cumulative
effect of lowered IQ and psychopathology.
In this particular study, the findings were found to still be significant after the
IQ differences were covaried out, hence implying that IQ was not entirely
responsible for the between-group differences in performances on the hinting
task. There is, however, a need to reliably distinguish between a compromised
information-processing capacity, IQ and a general ToM impairment (As sug-
gested by BruÈne, 2003).
Limitations
With this being a pilot study testing new hinting sentences, the size of the groups
was relatively small (n = 15). This size constraint meant that the schizophrenia
group was heterogeneous, unlike the original hinting study (Corcoran et al.,
1995), in which the schizophrenia group was symptom-orientated and divided
into particular subgroups (e.g., passivity and paranoid for the different delusion
THEORY OF MIND AND PSYCHOSIS 355
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

types). The use of the Krawiecka standardised scale of psychotic symptoms, did
however, allow the groups to be subdivided into subgroups for symptom severity
(none/low and moderate/severe for delusions and hallucinations). Cumulative
scores for positive symptoms (coherently expressed delusions, hallucinations,
incoherence/irrelevance of speech and incongruity), negative symptoms (pov-
erty of speech, flattened behaviour), and nonspecific symptoms (depression,
anxiety, and psychomotor retardation) were then used in further analysis. In
terms of negative symptoms our findings are not significant (see above) and this
is in contrast with the finding of Corcoran et al. (1995) in which this group of
patients produced the worst scores on the task. It may well be that this difference
is due to the fact that this study did not have a particular subgroup of schizo-
phrenia patients with the particular diagnosis of negative features.
It is apparent from Table 1 that the age, sex ratios, and IQs were not matched
across the groups. However, as mentioned previously, regression analysis was
performed to covary for these possible limitations. Medication dose was also
covaried for as it is widely believed that long-term use of medication, particu-
larly antipsychotics, may have a significant impact on cognitive functioning.
This study has confirmed, as hypothesised, that the schizophrenia group
performed less well as either the affective and control groups on this ToM task.
As regards the symptomatology of psychosis, the study found that poor per-
formance could be linked to positive symptoms, independent of diagnosis. The
presence of hallucinations and delusions was also found to be significant. These
findings add validation to the earlier mentioned Frith (1992) model linking
positive symptomatology of schizophrenia to mental state impairments. With
regard to the major finding of this study, this model could be enlarged to
encompass all psychoses.
We think that the hinting task is an adequate tool for testing ToM abilities in
adults, and that this study lends further support to the argument that there are
symptom-specific difficulties in the ability to infer mental states of others.
Manuscript received 2 April 2004
Revised manuscript received 21 May 2004
REFERENCES
Abu-Akel, A. (1999). Impaired theory of mind in schizophrenia. Pragmatics and Cognition, 7,
247±282.
Abu-Akel, A. (2003). A neurological mapping of theory of mind. Brain Research Reviews, 43,
29±40.
Abu-Akel, A., & Bailey, A. L. (2000) Correspondence to the Editor. Psychological Medicine, 30,
735±738.
Ammons, R. B., & Ammons, C. H. (1962). The Quick Test. Missoula, MT: Psychological Test
Specialists.
356 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

Atkins, M., Burgess, A., Bottomly, C., & Riccio, M. (1997). Chlorpromazine equivalents: A con-
sensus of opinion for both clinical and research implication. Psychiatric Bulletin, 21, 224±226.
Baron-Cohen, S. (1995). Mindblindness: An essay on autism and theory of mind. Cambridge, MA:
MIT Press.
British Medical Association and Royal Pharmaceutical Society of Great Britain. (2002). British
National Formulary. London: Author.
BruÈne, M. (2003). Theory of mind and the role of IQ in chronic disorganized schizophrenia. Schi-
zophrenia Research, 60, 57±64.
Corcoran, R., Cahill, C., & Frith, C. D. (1997). The appreciation of visual jokes in people with
schizophrenia: A study of `mentalizing' ability. Schizophrenia Research, 24, 319±327.
Corcoran, R., Mercer, G. & Frith, C. D. (1995). Schizophrenia, symptomatology and social infer-
ence: investigating ``theory of mind'' in people with schizophrenia. Schizophrenia Research, 17,
5±13.
Doody, G. A., Gotz, M., Johnstone, E. C., Frith, C. D., & Owens, D. G. (1998). Theory of mind and
psychoses. Psychological Medicine, 28, 397±405.
Drury, V. M., Robinson, E. J., & Birchwood, M. (1998). `Theory of mind' skills during an acute
episode of psychosis and following recovery. Psychological Medicine, 28, 1101±1112.
Frith, C. D. (1992). The cognitive neuropsychology of schizophrenia. Hove, UK: Psychology Press.
Frith, C. D. (2004). Schizophrenia and theory of mind Psychological Medicine, 34, 385±389.
Frith, C. D., & Corcoran, R. (1996). Exploring ``theory of mind'' in people with schizophrenia.
Psychological Medicine, 23, 521±530.
Herold, R., Tenyi, T., Lenard, K., & Trixler, M. (2002). Theory of mind deficit in people with
schizophrenia during remission. Psychological Medicine, 32, 1125±1129.
Janssen, I., Krabbendam, L., Jolles, J., & Van Os, J. (2003). Alterations in theory of mind in patients
with schizophrenia and non-psychotic relatives. Acta Psychiatra Scandinavica, 108, 110±117.
Kerr, N., Dunbar, R., & Bentall, R. (2003). Theory of mind deficits in bipolar affective disorder.
Journal of Affective Disorders, 73, 253±259.
Krawiecka, M., Goldberg, D., & Vaughan, M. (1977). A standardized psychiatric assessment scale
for rating chronic psychotic patients. Acta Psychiatrica Scandinavica, 55, 299±308.
Leslie, A. (1987). Pretense and representation: The origins of `Theory of Mind'. Psychological
Review, 94, 412±426.
Pickup, G. J., & Frith, C. D. (2001). Theory of mind impairments in schizophrenia: Symptomatology,
severity and specificity. Psychological Medicine, 31, 207±220.
Premack, D., & Woodruff, G. (1978). Does the chimpanzee have a theory of mind? Behavioral and
Brain Sciences, 4, 515±526.
Shallice, T., Fletcher, P., Frith, C. D., Grasby, P., Frackowiak, R. S., & Dolan, R. J. (1994). Brain
regions associated with acquisition and retrieval of verbal episodic memory. Nature, 368,
633±635.
Woods, S. (2003). Chlorpromazine equivalent doses for newer atypical antipsychotics. Journal of
Clinical Psychiatry, 64, 663±666.
Wykes, T., Hamid, S., & Wagstaff, K. (2001). Theory of mind and executive functions in the non-
psychotic siblings of patients with schizophrenia. Schizophrenia Research, 49(Suppl.), 148.
THEORY OF MIND AND PSYCHOSIS 357
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

APPENDIX
The 10 new hinting tasks used in conjunction with the 10 Corcoran tasks
Lisa is about to leave the house when her father's car pulls up in the driveway. When he enters she
says to him: ``I really need to go shopping, but it's so far away and the rain is terrible''.
Question: What does Lisa really mean when she says this?
Hint: Lisa goes on to say: ``It's only five minutes in the car''.
Question: What does Lisa want her father to do?
Alan is watching television, and his wife Jill sits down to join him. She says: ``I see you're watching
the football. Isn't there anything else on at the moment?''
Question: What does Jill really mean when she says this?
Hint: Jill then says to Alan: ``I thought there was a good play on the other channel''.
Question: What does Jill want Alan to do?
Sarah is spending the morning with her next-door neighbour Caroline, having coffee. They are
talking about Sarah's forthcoming holiday abroad, when Sarah says to Caroline: ``I'm worried that
all my plants will be dead by the time I get back''.
Question: What does Caroline really mean when she says this?
Hint: Caroline then says to Sarah: ``I have a spare key for the front door''.
Question: What does Caroline want Sarah to do?
Jack and his father are talking about the recent form of the local football team, which they both
support. Jack says: ``You know United are playing at home to their big rivals this weekend. I'm sure
it will be very exciting.''
Question: What does Jack really mean when he says this to his father?
Hint: Jack goes on to say: ``I have never been to watch a football match''.
Question: What does Jack want his father to do?
Jim and his brother Richard are getting ready for work in the morning. Jim goes to the bathroom and
finds that Richard is about to use the shower, and says to him: ``I've got an early start today and I'm
running late''.
Question: What does Jim really mean when he says this to Richard?
Hint: Jim goes on to say to Richard: ``It won't take me long to get ready''.
Question: What does Jim want Richard to do?
Harry and Chris work together in the same office. One day Harry says to Chris: ``I would really like
an extra long lunch break today, as I have to go to the bank. Will you be going out for lunch today?''
Question: What does Harry really mean when he says this?
Hint: Harry then says to Chris: ``Do you think our boss would mind if only one of us were here?''
Question: What does Harry want Chris to do?
On a weekday evening, Martin goes to see his friend Lucy at home. He is trying to persuade her to go
out for a meal, but she says: ``I'm really busy writing a report tonight. I don't even have time to
chat''.
Question: What does Lucy really mean when she says this?
Hint: Lucy then says: ``I really have to be getting on with my work, is there someone else you could
ask''.
Question: What does Lucy want Martin to do?
358 MARJORAM ET AL.
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

Two children, Emma and Katie are playing, when Emily breaks an old statue belonging to Katie's
mother. Emma says to Katie: ``If your Mum finds out it was me that broke it, I won't be allowed to
come here anymore''.
Question: What does Emma really mean when she says this?
Hint: Emma then says to Katie: ``She wouldn't punish you though''.
Question: What does Emma want Katie to do?
Tony and his girlfriend Alison are giving a dinner party at their new flat. They are going through the
list of guests when Alison exclaims: ``Oh! It says here you've invited your ex-girlfriend. Is that
right?''
Question: What does Alison really mean when she says this?
Hint: Alison goes on to say to Tony: ``I don't get on with her very well''.
Question: What does Alison want Tony to do?
Simon is enjoying an evening out at the pub with his friend Gareth. Gareth is about to buy some more
drinks when Simon says: ``I have a very busy day tomorrow, and I need to be at my best''.
Question: What does Simon really mean when he says this?
Hint: Simon then says to Gareth: ``We have already had quite a lot to drink''.
Question: What does Simon want do?
THEORY OF MIND AND PSYCHOSIS 359
Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3

Dow
nloa
ded
by [
Mou
nt R
oyal
Uni
vers
ity]
at 0
3:19
12
May
201
3







