

1
Chiari like malformation & Syringomyelia
Lecture synopsis
• What is syringomyelia
• Clinical signs of syringomyelia
• Diagnosis of syringomyelia
• Treatment of syringomyelia

2
Syringomyelia
Syringomyelia - fluid-filled cavities in the spinal cord
Due to obstruction of cerebrospinal fluid movement
Pan and Syrinx Peter Paul Rubens 1618
3
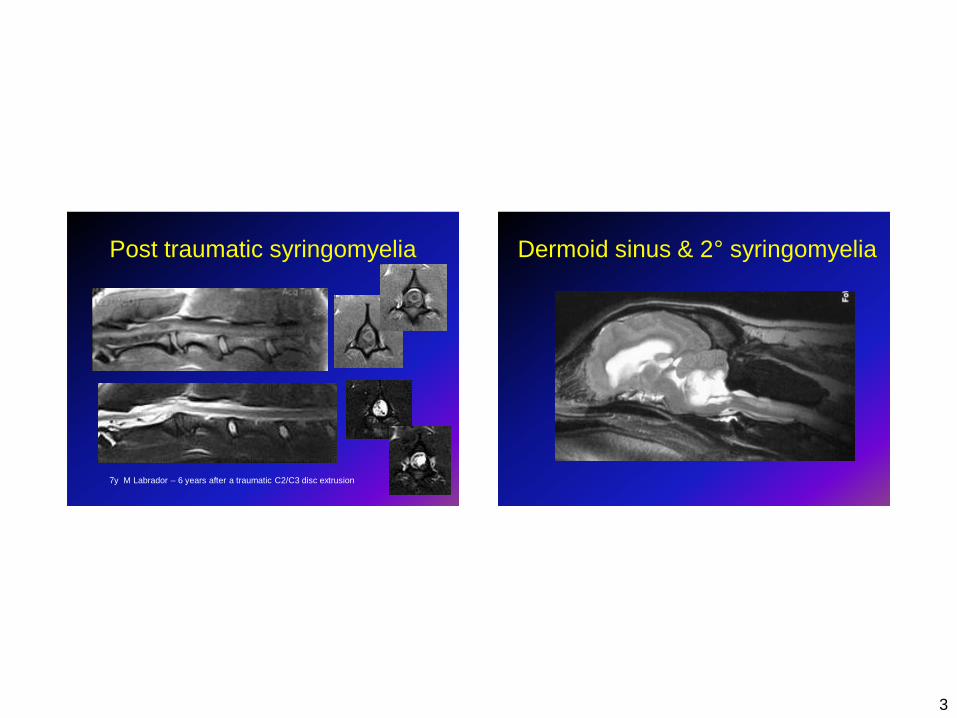
Post traumatic syringomyelia
7y M Labrador – 6 years after a traumatic C2/C3 disc extrusion
Dermoid sinus & 2° syringomyelia
4
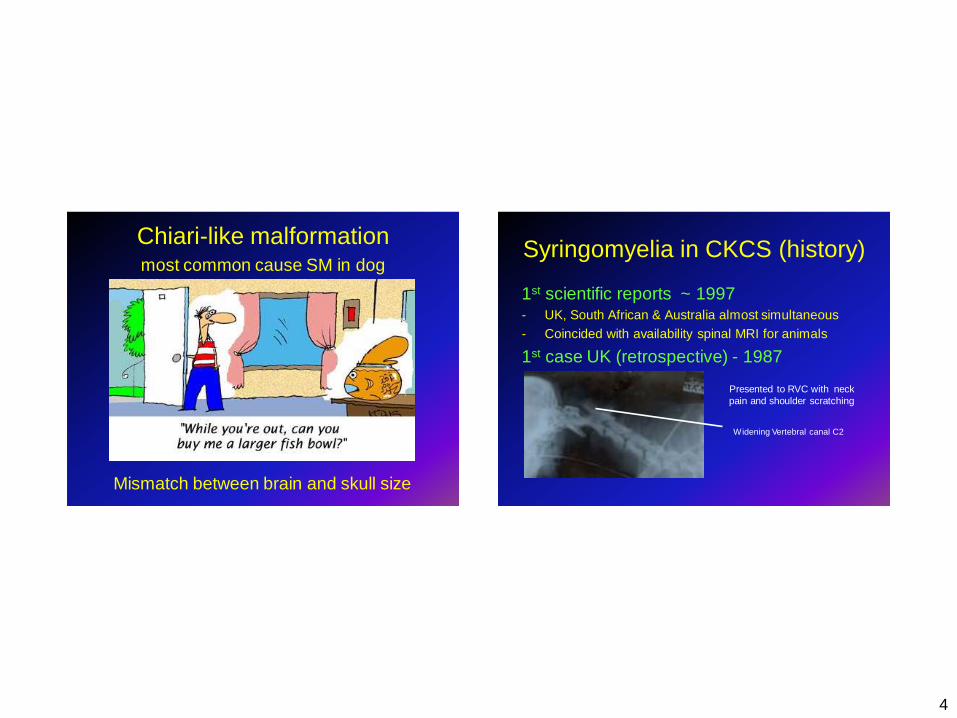
Chiari-like malformation
most common cause SM in dog
Mismatch between brain and skull size
Syringomyelia in CKCS (history)
1st scientific reports ~ 1997
- UK, South African & Australia almost simultaneous
- Coincided with availability spinal MRI for animals
1st case UK (retrospective) - 1987
Widening Vertebral canal C2
Presented to RVC with neck
pain and shoulder scratching

5
CM – characteristics
Overcrowding of the skull
Normal CM
Pathogenesis syringomyelia
High velocity jet
Spinal cord “pulled
out” and cavity forms
Piston like action
cerebellar vermis
Decreases hydrostatic pressure (Venturi effect)
Extracellular fluid
accumulates
Increased pressure within cord
Decreased pressure outside cord
Systolic pulse
pressure
6
Breeds CM/SM • Any toy breed dog and SBT
• Especially
– Cavalier King Charles spaniel
– King Charles spaniels
– Griffon Bruxellois
– Affenpinscher
– Maltese (miniature)
– Yorkshire terrier (miniature)
– Pomeranian (miniature)
– Chihuahua (miniature)
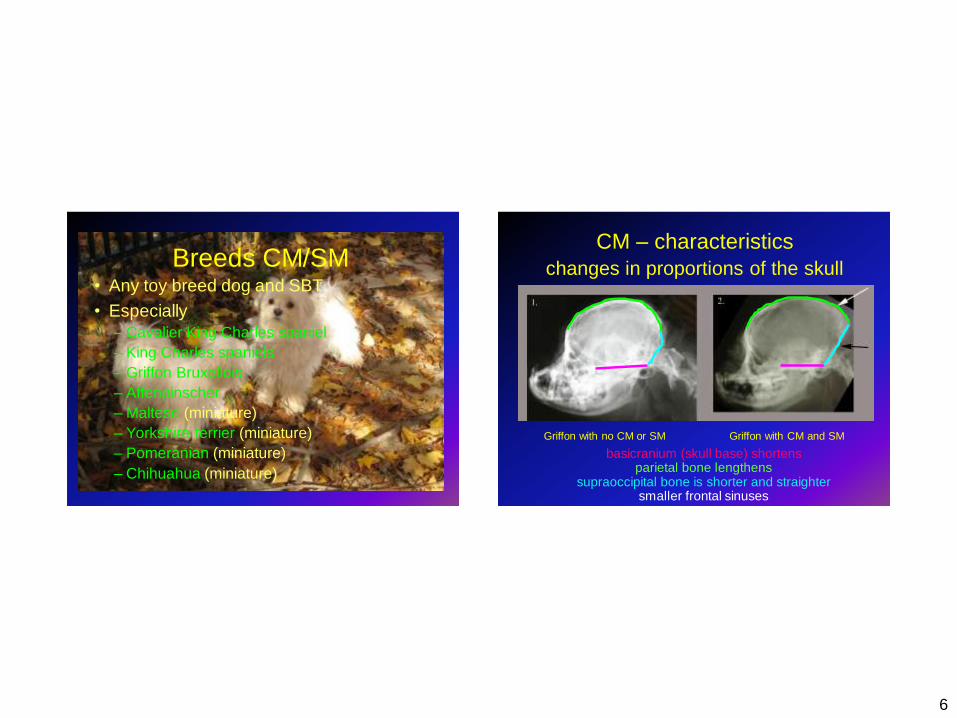
CM – characteristics
changes in proportions of the skull
Griffon with no CM or SM Griffon with CM and SM
basicranium (skull base) shortens parietal bone lengthens
supraoccipital bone is shorter and straighter smaller frontal sinuses
7
CKCS with CM
• Similar skull volume to other toys
• More brain tissue within skull
– Statistically similar volume to Labradors
Cross H. R., Capppello R, Rusbridge C Comparison of cerebral cranium volumes between CKCS with
chiari-like malformation, small breed dogs and Labradors JSAP 2009 50 399-405
CKCS with SM
• Skull (caudal fossa) volume
– Significantly smaller for CKCS with early onset SM
(<2y) compared to clear CKCS (> 5y)
• Parenchyma (brain) within skull
– significantly greater for CKCS with SM
– Especially in CKCS with early onset SM
• SM associated with brain / skull mismatch
– Early onset SM greater disparity
– Increased parenchyma (brain) within skull = larger syrinx
– Big syrinx = Big ventricles
Vet Rec. 2010 Dec 18;167(25):978-9. Morphometric assessment of cranial volumes in age-matched Cavalier
King Charles spaniels with and without syringomyelia. Driver CJ, Rusbridge C, McGonnell IM, Volk HA.

8
Clinical signs – CM/SM
PAIN
Before medication After medication
Pain face
Canine syringomyelia
Pain - Most common clinical sign

9
Unusual sleeping posture /
interrupted sleep Poor exercise tolerance

10
Unwilling / pain on jumping Shoulder scratching
Especially
• Walking
• Excited
• Touched
• “clothing”
– neck collar
– snoods
• “air guitar”
11
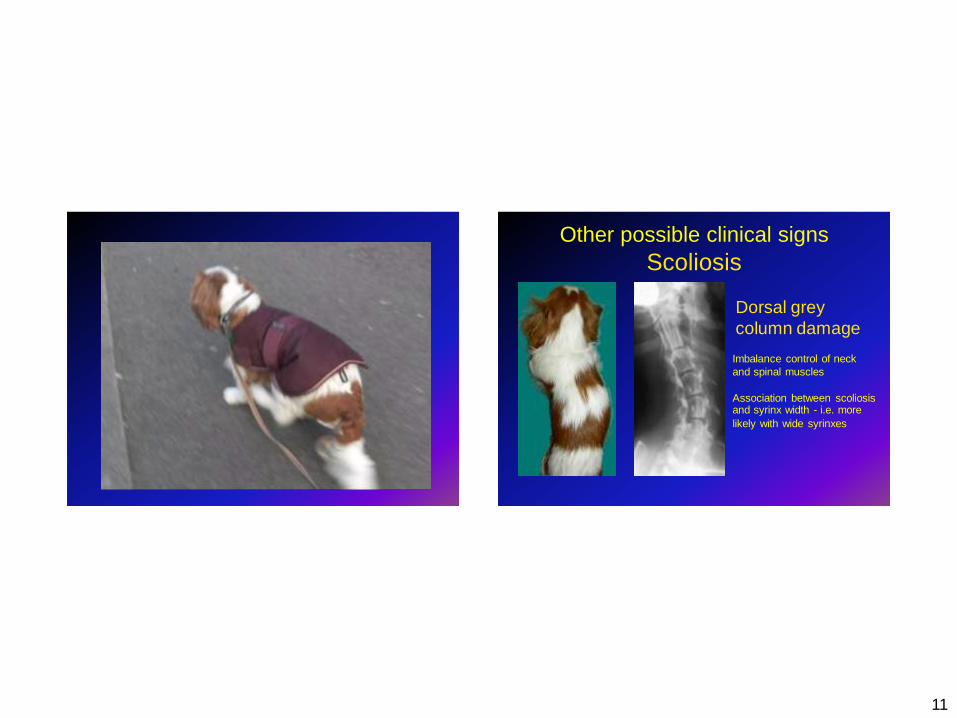
Other possible clinical signs
Scoliosis
Imbalance control of neck
and spinal muscles
Association between scoliosis and syrinx width - i.e. more
likely with wide syrinxes
Dorsal grey
column damage
12
Clinical signs of SM
• Not all dogs with SM have signs
• Depends on width and location of syrinx
– Wide syrinx = pain +/- scratching
• Many dogs with SM have no / subtle signs
– a “problem in waiting”
– May produce offspring with SM
– May produce offspring with pain from SM
MRI from 16 month CKCS in severe pain
Wide asymmetrical syrinx
White = fluid; light grey = spinal cord
CM associated pain
Cartoons - Thanks to Tania Ledger www.cavaliermatters.org
13
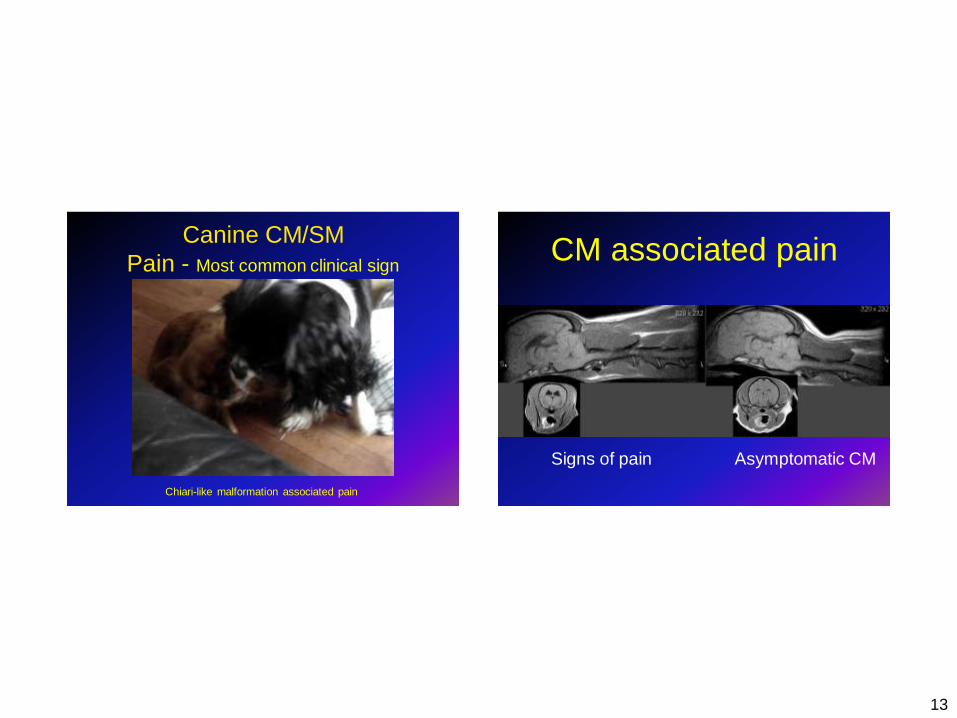
Canine CM/SM
Pain - Most common clinical sign
Chiari-like malformation associated pain
CM associated pain
Signs of pain Asymptomatic CM

14
Canine SM - Clinical signs Neurological deficits in more severe cases
2 year old female CKCS
Severe neurogical deficits - uncommon
15
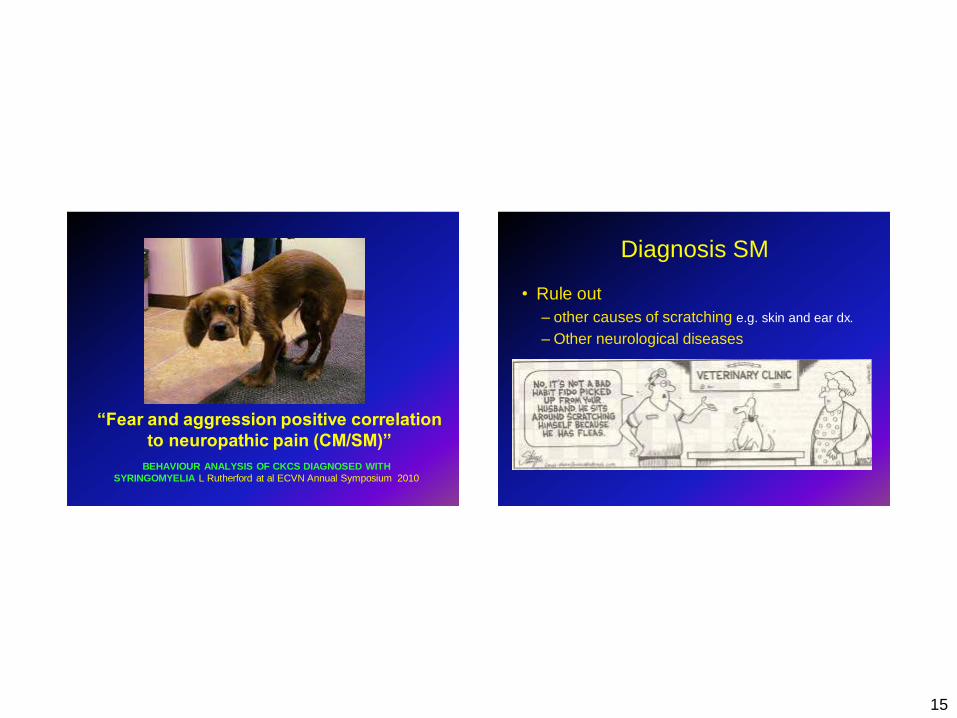
“Fear and aggression positive correlation
to neuropathic pain (CM/SM)”
BEHAVIOUR ANALYSIS OF CKCS DIAGNOSED WITH
SYRINGOMYELIA L Rutherford at al ECVN Annual Symposium 2010
Diagnosis SM
• Rule out
– other causes of scratching e.g. skin and ear dx.
– Other neurological diseases
16
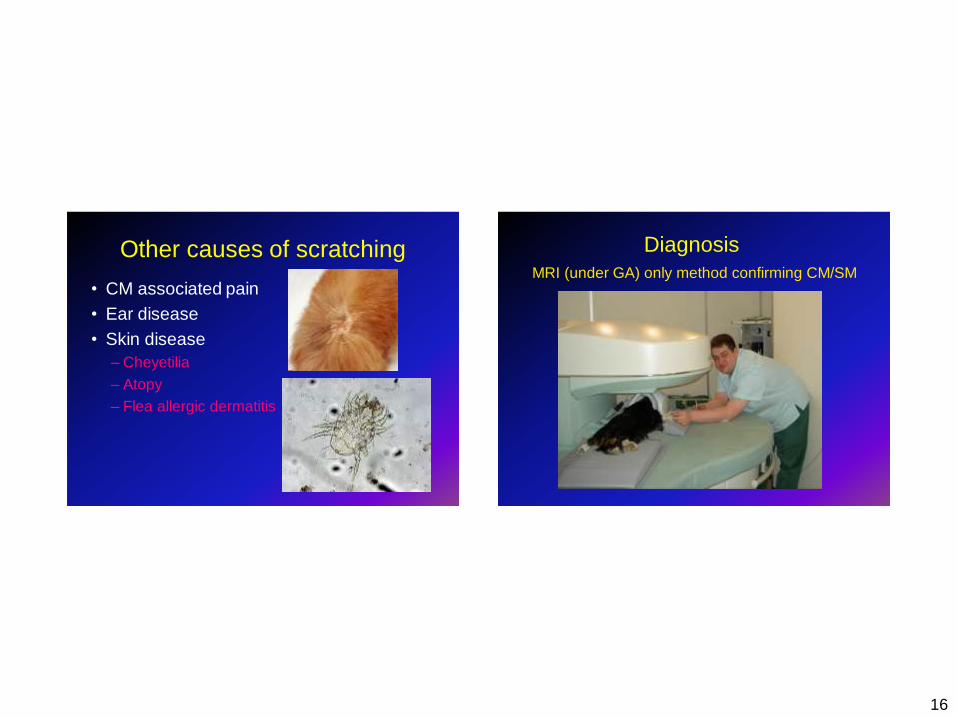
Other causes of scratching
• CM associated pain
• Ear disease
• Skin disease
– Cheyetilia
– Atopy
– Flea allergic dermatitis
Diagnosis
MRI (under GA) only method confirming CM/SM
17
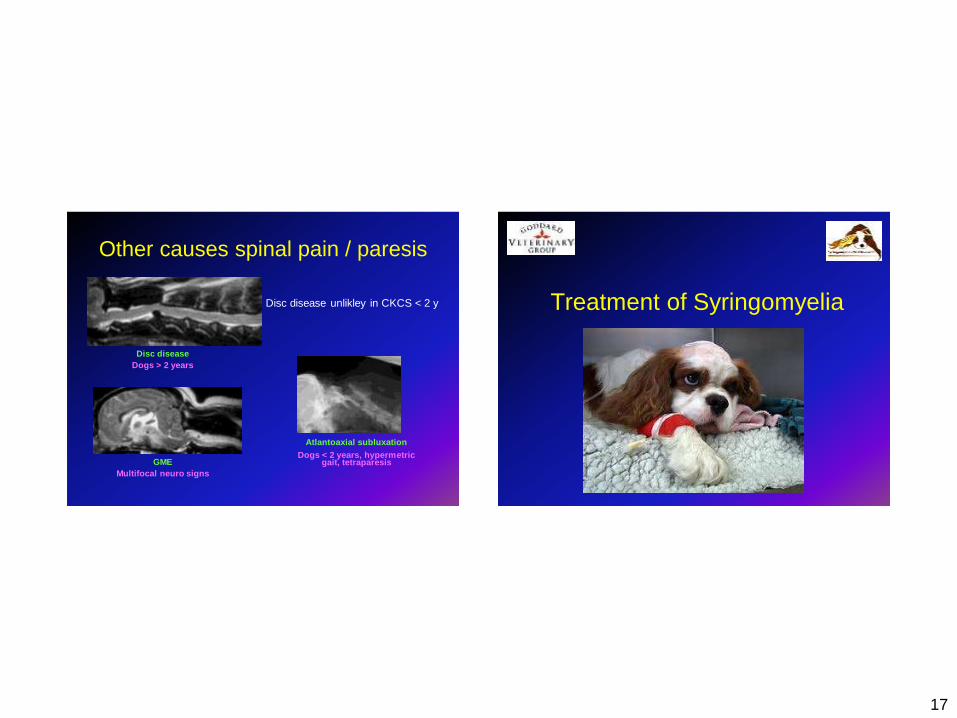
Other causes spinal pain / paresis
GME
Multifocal neuro signs
Atlantoaxial subluxation
Dogs < 2 years, hypermetric gait, tetraparesis
Disc disease
Dogs > 2 years
Disc disease unlikley in CKCS < 2 y Treatment of Syringomyelia
18
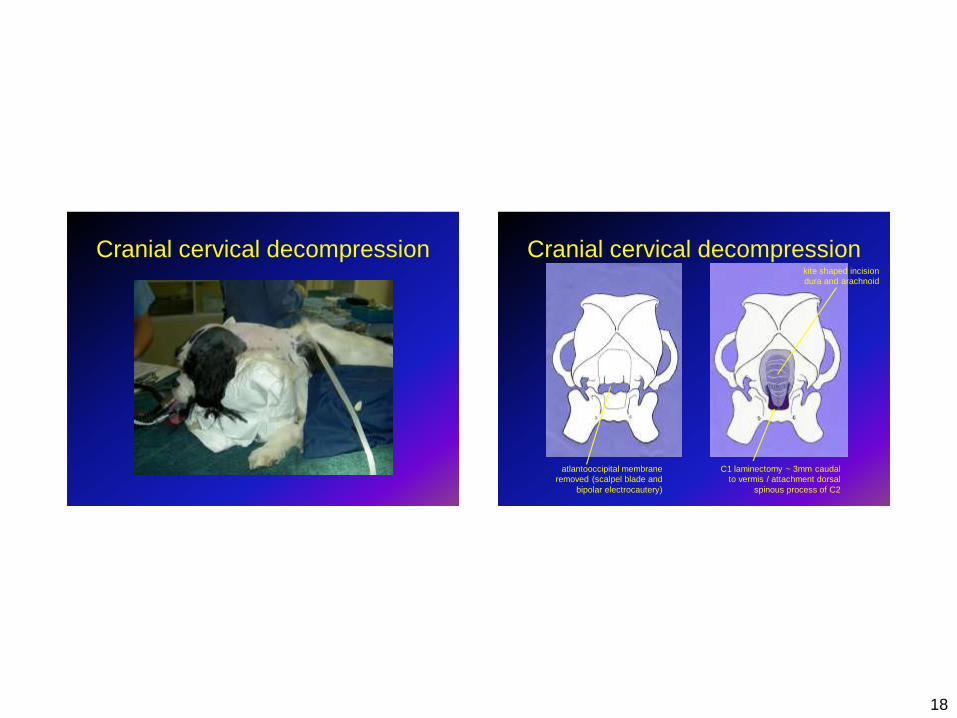
Cranial cervical decompression Cranial cervical decompression
C1 laminectomy ~ 3mm caudal
to vermis / attachment dorsal
spinous process of C2
kite shaped incision
dura and arachnoid
atlantooccipital membrane
removed (scalpel blade and
bipolar electrocautery)
19
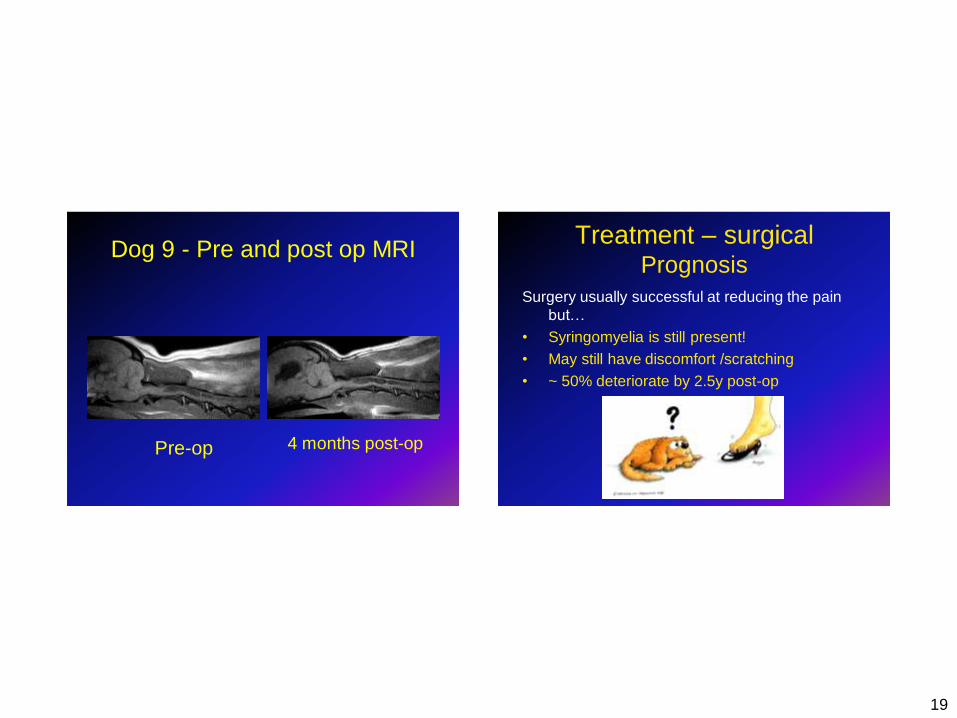
Dog 9 - Pre and post op MRI
Pre-op 4 months post-op
Treatment – surgical Prognosis
Surgery usually successful at reducing the pain
but…
• Syringomyelia is still present!
• May still have discomfort /scratching
• ~ 50% deteriorate by 2.5y post-op
20
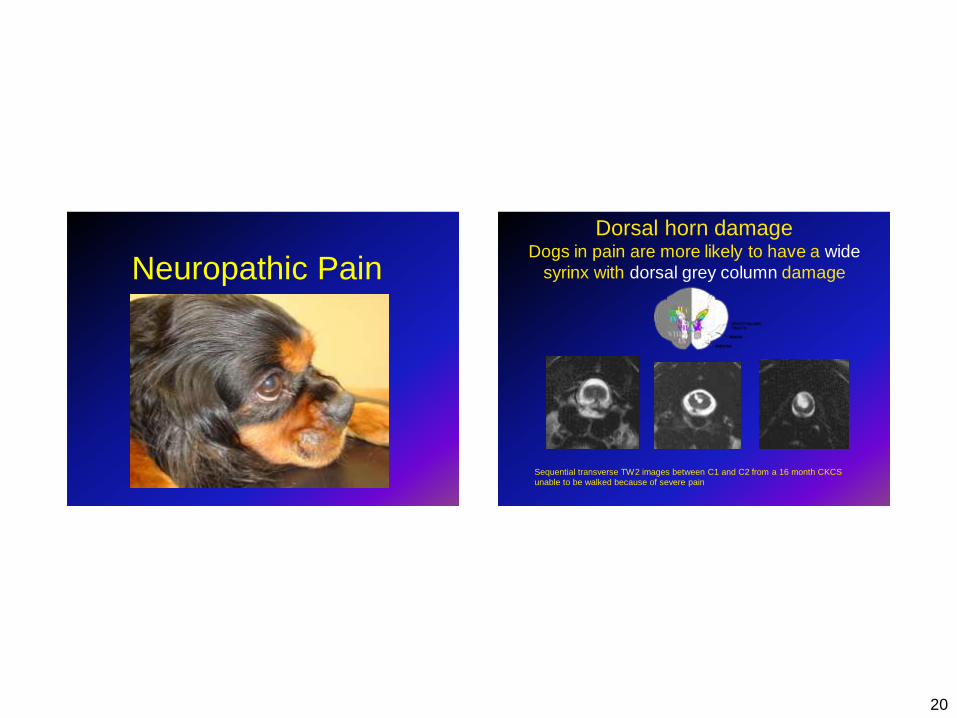
Neuropathic Pain
Dorsal horn damage Dogs in pain are more likely to have a wide
syrinx with dorsal grey column damage
Sequential transverse TW2 images between C1 and C2 from a 16 month CKCS
unable to be walked because of severe pain
21
Treatment – medical
Drugs which reduce CSF production
• Antacids
– Proton pump inhibitors
• Omeprazole
– H2 receptor antagonist
• Cimetidine
• Diuretics
– Furosemide
Treatment – medical Painkillers • NSAIDS
– May be effective for mild cases
– Coxibs more effective for central pain?
• Neurogenic analgesics – Gabapentin (Neurontin; Pfizer)
– Pregabalin (Lyrica; Pfizer)
– Amantadine
• antiviral drug, also used for Parkinson's Disease
• prevents pain “wind up” in spinal cord dorsal horn
– Tramadol
• μ-opioid receptor, inhibits reuptake serotonin & noradrenalin
• Useful for “bad periods”
• Oral opioids, e.g. pethidine or methadone • Only useful in short term

22
Treatment – medical
• Corticosteroids
– in short term effective at reducing pain and
improving neurological status
– Side effects of immunosuppression, weight
gait and skin changes
Medical Treatment – what I do Start Cimetidine 5-6mg/kg 2-3 x daily
Or
or Omeprazole at 0.5-1.5mg/kg 1x daily
• If response reconsider surgery
• If inadequate add NSAIDS
• If inadequate add gabapentin +/- NSAIDS
• If inadequate reconsider surgery – if not an option then add corticosteroids +/- gabapentin
• Also – Pregabalin
– Amantadine
23
Exercise • To within own limits
• Inability to exercise
– Indication more serious disease
• During aerobic exercise
– Heart beats faster and with more force
– Increases pulse pressure
– Signs are exacerbated
– Progression CM/SM accelerated?
• Humans – advised against aerobic
exercise prior to decompression
– Most symptomatic patients cannot anyway
Little things
24
Complementary therapy & CM/SM
Remember that touch can hurt! Must be tailored to the individual
Lack of data regarding CM/SM
What is appropriate?
• Gentle massage?
• Low level laser therapy
• Ultrasound therapy
• Acupuncture?
What is not appropriate?
• Spinal manipulation
• Guarded if…
– wide syrinx
– first clinical signs before 4 years of age.
• NeP progresses in ¾ CKCS with CM+/-SM
despite medical treatment (study of 48 dogs)
– Many still enjoy reasonable quality of life
– 15% euthanatised CMSM
– Live with CMSM and die from MVD
Prognosis Medical management
25
Conclusion
• Syringomyelia is a painful spinal cord disease
• A multimodal approach to pain relief is more
likely to be successful.
– Surgery
– Drugs
– Complementary therapy
www.veterinary-neurologist.co.uk
Thank you for listening!
Any questions?







