
Technological advances in Brachytherapy
Ekkasit Tharavichitkul, MDThe Division of Therapeutic Radiology
and Oncology, Faculty of Medicine, Chiang Mai University
History
• Greek word = short
–Interstitial brachytherapy
–Contact brachytherapy→ surface mould BT→ intracavitary BT→ endolumina BT

Brachytherapy history
• 1896: Becquerel• 1898: MarieSklodowska-Curie• 1901: Danlosand Block: Paris• 1905Abbe: US Radium implantations
• Different empirical methods and rules•Stockholm method for Gyne (1914)
•Paris method for Gyne (1919)
•Manchester system (1934) Paterson-Parker, Meredith
•Paris System for IS : Pierquin, Chassagne, Dutreix

• Discovery of artificial radioactive isotopes
• 1934 Irene Curie -FrédericJoliot
• 1958 Iridium-I92: U. Henschke• Development of afterloading concept
• 1958 -65 U. Henschke-D. Chassagne• Developmentof 3D dosimetry and fundamental rules of
dosimetry
• 1965 B. Pierquin-D. Chassagne-A. Dutreix

Brachytherapy

Developments in BT
• Source and loading methods• Imaging developments• Applicator developments• Planning developments• Clinical research developments

Source and loading method

Radioisotope sources and loading methods
• From Radium --- Iridium • From LDR --- HDR --- PDR• From manual loading to remote after-
loading
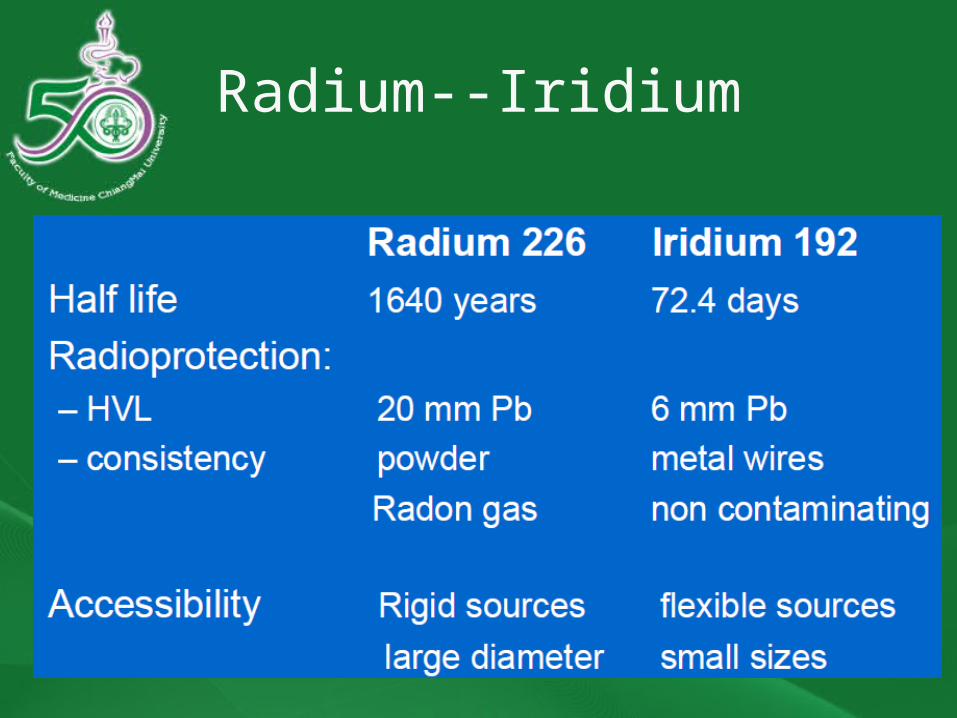
Radium--Iridium


Manual and remote loading
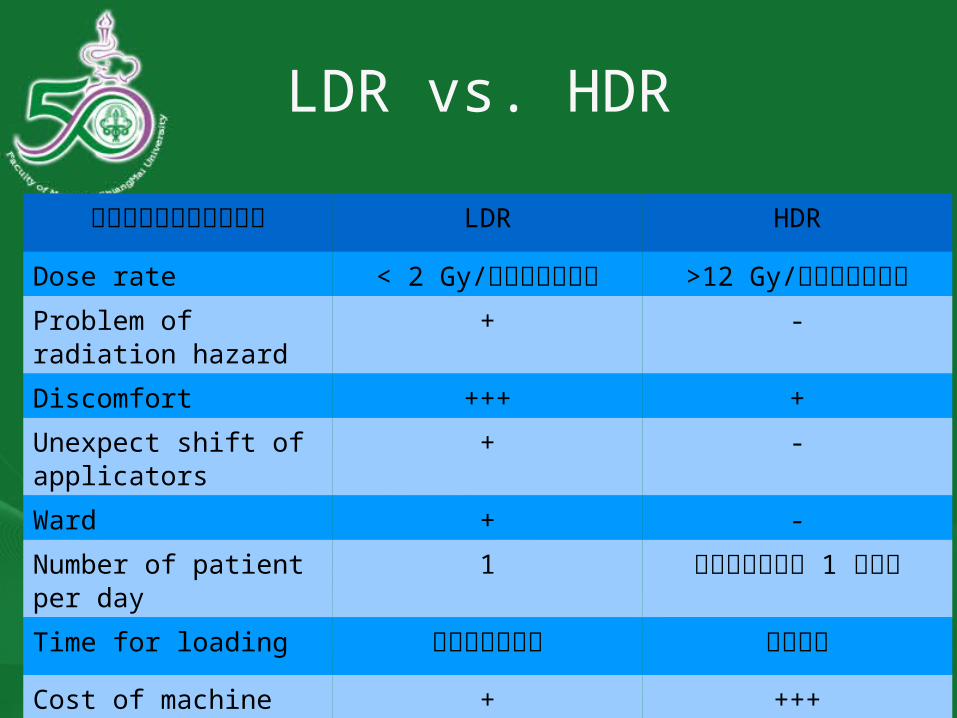
LDR vs. HDR
พารามิ�เตอร LDR HDR
Dose rate < 2 Gy/ชั่��วโมิง >12 Gy/ชั่��วโมิงProblem of radiation hazard
+ -
Discomfort +++ +
Unexpect shift of applicators
+ -
Ward + -
Number of patient per day
1 มิากกว�า 1 ราย
Time for loading ชั่��วโมิง นาที�
Cost of machine + +++

• Manual or remote control afterloading– Gynecological applicators– Guide needles: straight and curved– Plastic tubes– Moulds– Hypodermic needles– Silk wires– Endo-luminal catheters
• Remote control afterloaders

Imaging

• Modern imagingtechniques:
-US, CT, MRI
• 3D dosimetry-More accurate dose distribution-DVH relation to outcome for target + OAR
Imaging developments
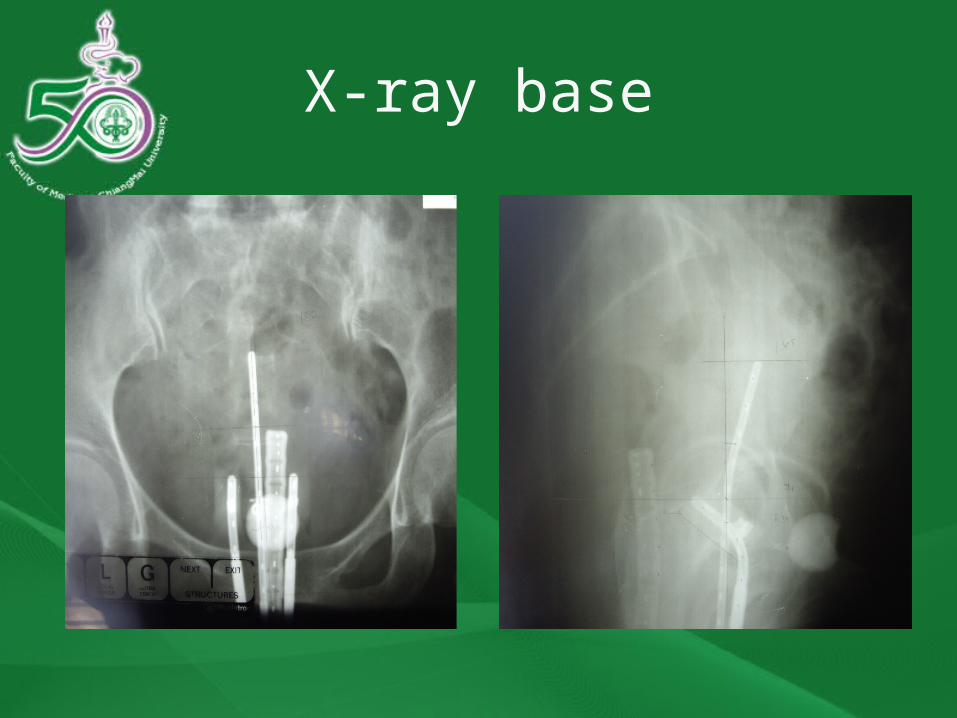
X-ray base
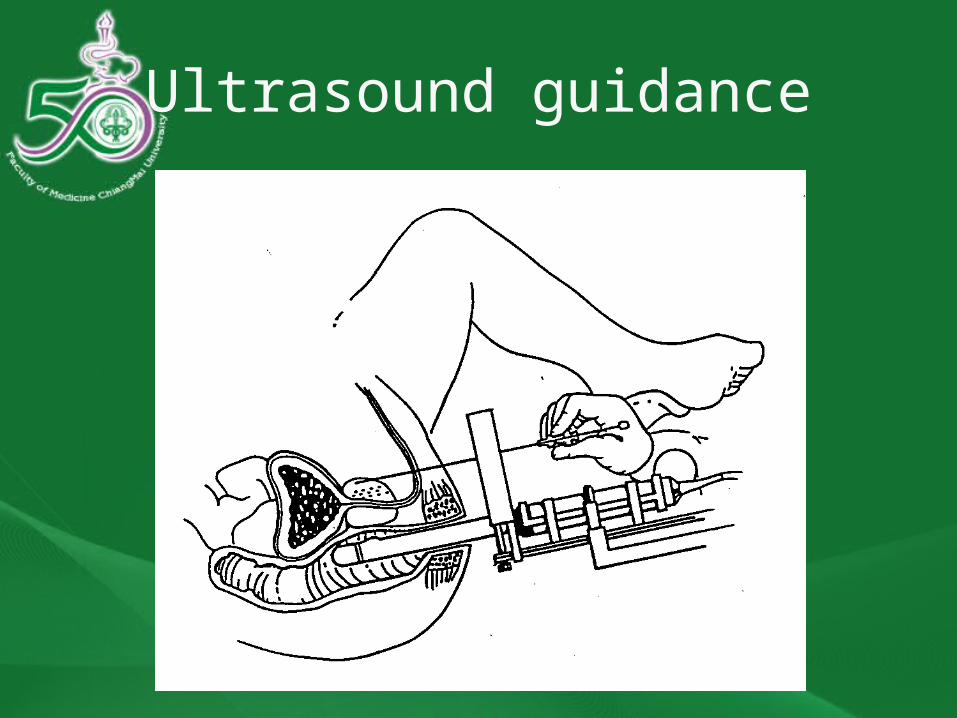
Ultrasound guidance

U/S guidance


Applicators

Applicator developments
• More compatible with imaging• CT/MR applicator
• Gynecological cancers
• Plastic catheter• Breast cancer• Prostate cancer

Standard applicators
Nucletron.com

Scatter; metallic applicator

CT/Applicator

Breast BT
Polgar, 2009
mammosite
Multicatheter
Clearpath

Volume concepts
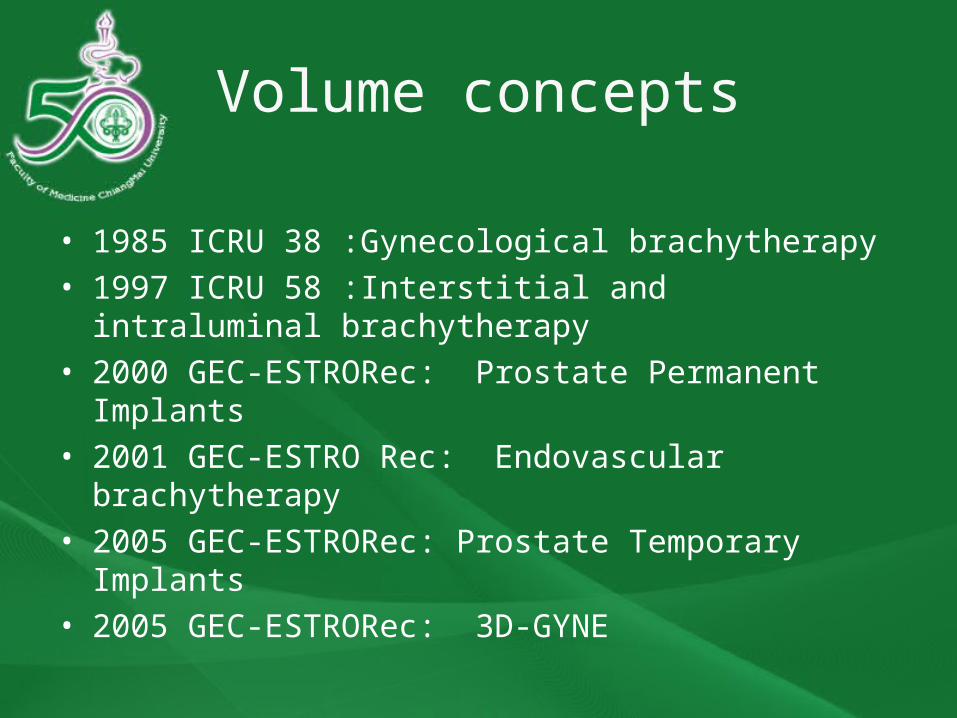
Volume concepts
• 1985 ICRU 38 :Gynecological brachytherapy• 1997 ICRU 58 :Interstitial and intraluminal brachytherapy• 2000 GEC-ESTRORec: Prostate Permanent Implants• 2001 GEC-ESTRO Rec: Endovascular brachytherapy• 2005 GEC-ESTRORec: Prostate Temporary Implants• 2005 GEC-ESTRORec: 3D-GYNE
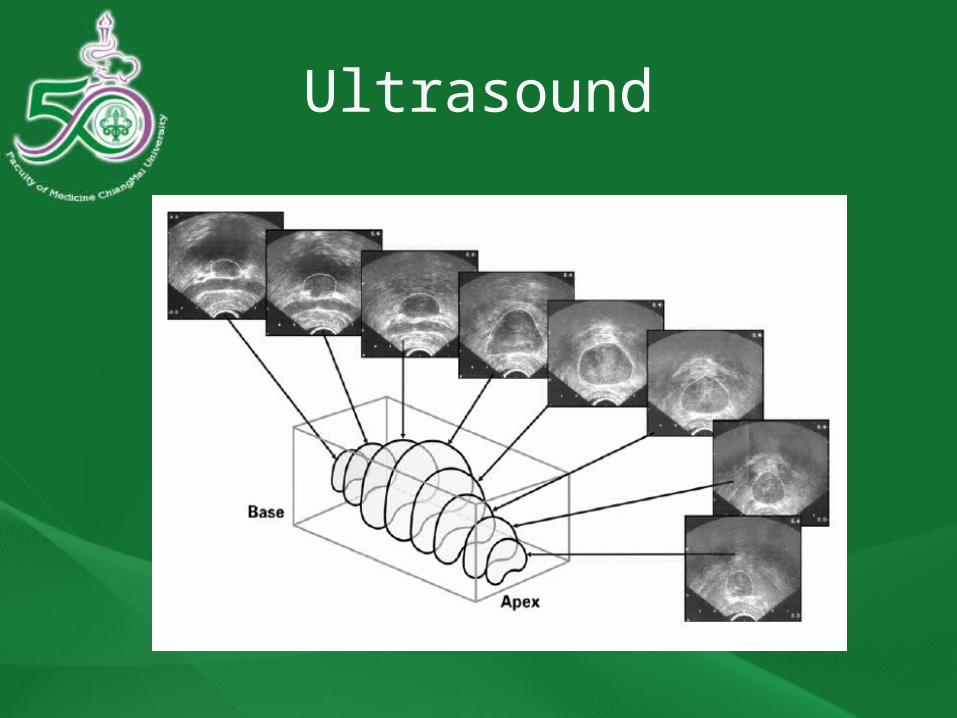
Ultrasound
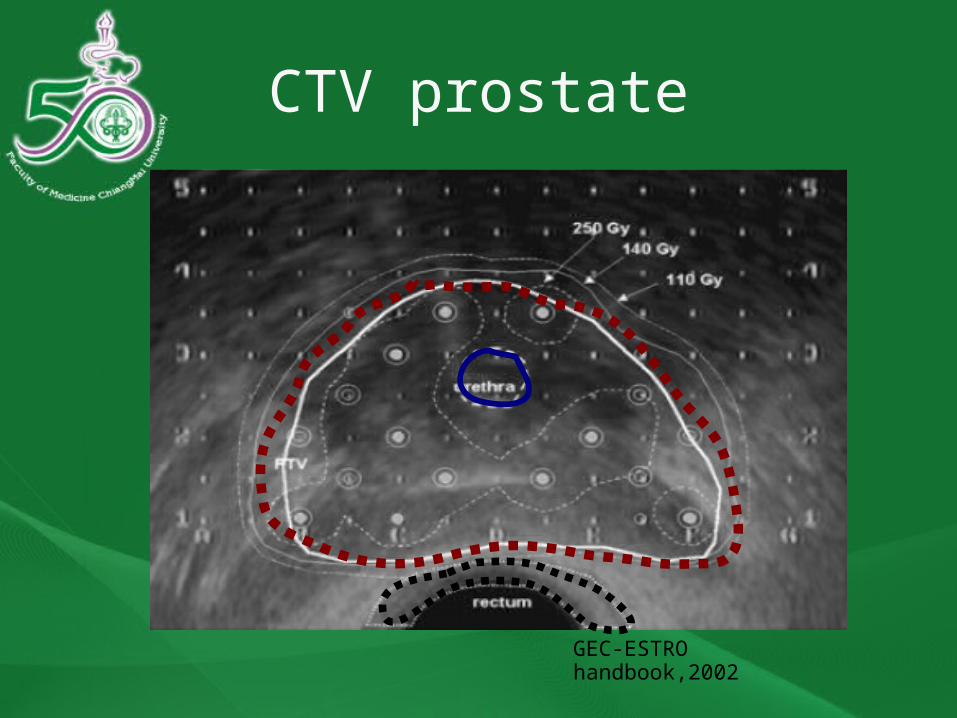
CTV prostate
GEC-ESTRO handbook,2002
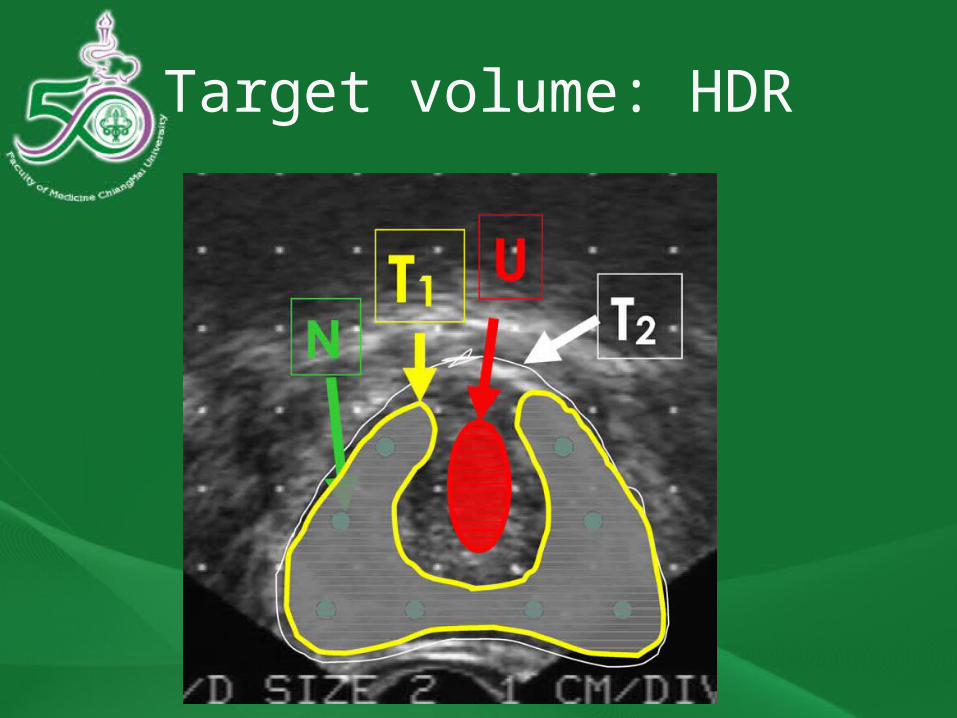
Target volume: HDR


Volume concepts of cervix
CHM, 2005

Diagram of CTVs
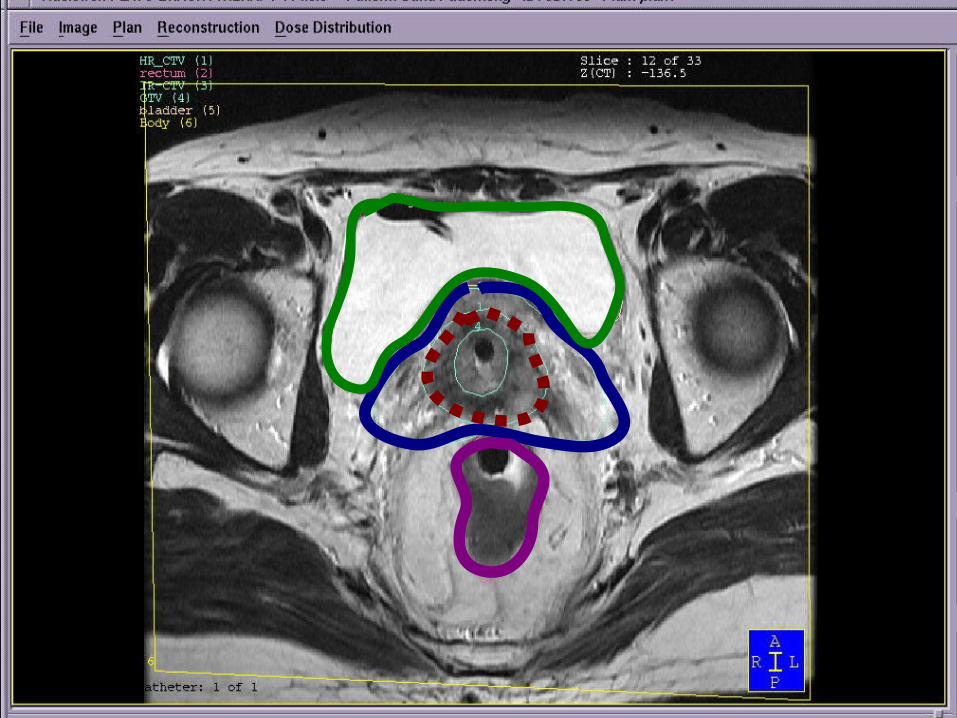

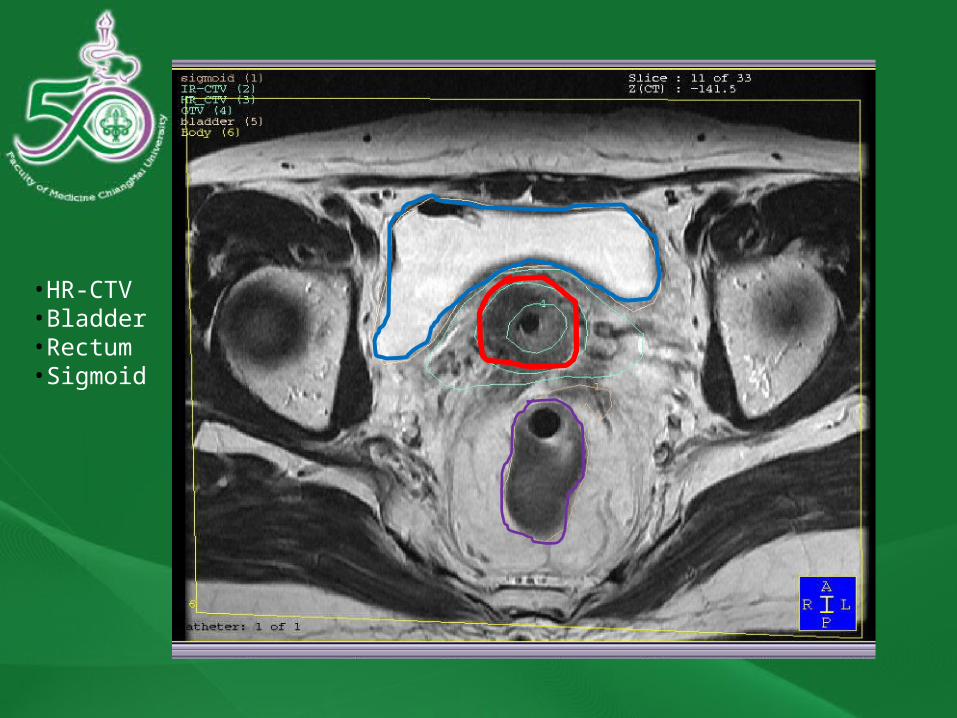
•HR-CTV•Bladder•Rectum•Sigmoid

D90 HR-CTVD2cc BD2cc RD2cc S

Chiang Mai
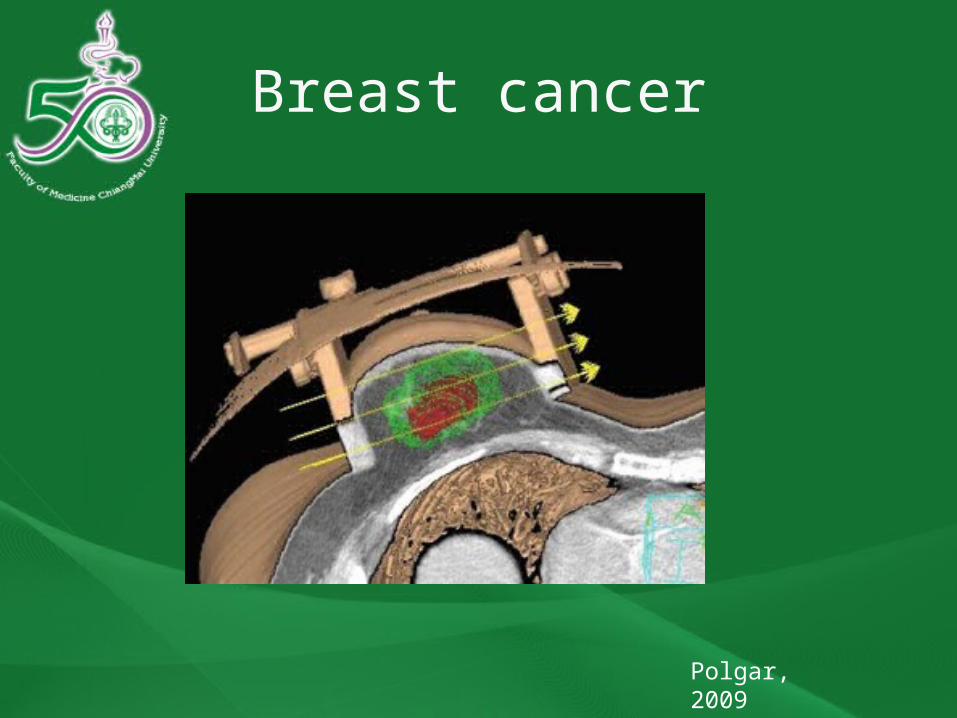
Breast cancer
Polgar, 2009

Planning developments

Planning developments
• Shifting from 2D to 3D• Target volume definition• Algorithm: AAPM TG43 to Monte Carlo• Inverse planning
• IPSA (Inverse Planning Simulated Annealing)• HIPO (the Hybrid Inverse Planning and
Optimization)


Clinical studies

Cervix

Breast BT
Polgar, 2009

Clinical studies
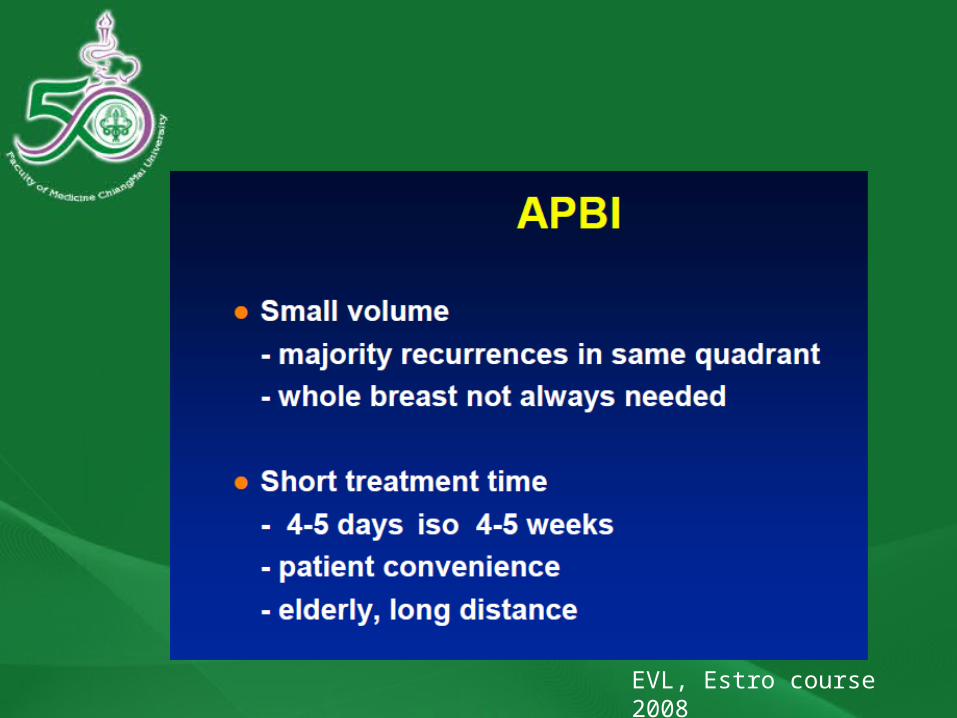
EVL, Estro course 2008
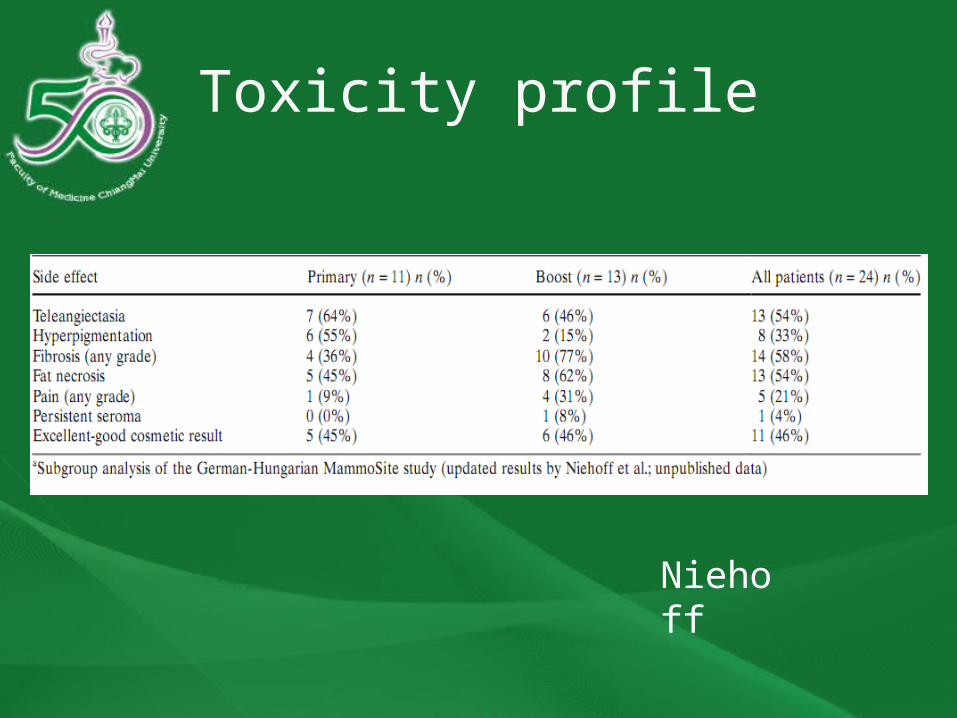
Toxicity profile
Niehoff

Clinical developments
All RCTsNSABP B-39/RTOG 0413 (4800 pts
enrolled) WBI 50 Gy plus boost to 60-66 Gy versus
Multicatheter (34Gy)/Mammosite(34 Gy) /3D-CRT(38.5Gy)
GEC-ESTRO working group trial (1170 pts enrolled) WBI 50 Gy plus boost 10 Gy versus HDR and
PDR
Pending for results

Conclusions
• Modern brachytherapy which is high Ballistic selectivity and adaptivity is a competitive tool in the multidisciplinary treatment of cancer patients
• A strong collaboration between-Radiation oncologists-Organ specialists-Medical physicists-Radiation technologists
is necessary to obtain optimal results for the patient(s)

Our researches: CT
From July 2008 - Dec 2009 16 pts in CT-based planning in EBRT and BT BT 6.5 Gy x Fx GEC-ESTRO recommendations concepts Image-guided planning (optimized plan) can
reduced the dose to the bladder and sigmoid colon with compromised dose to the target

Our research:MRI
From Feb 2009- nowadays Planned 14 pts will be enrolled MRI guided treatment: Dx, 1st BT, after
treatment With GEC-ESTRO recommendations Now 6 patients finished Pending results

![Volume-8 | Issue-5 | May-2019 | PRINT ISSN No. 2250 - 1991 ... · brachytherapy are as per the American Brachytherapy Society (ABS) consensus guidelines for sarcoma brachytherapy[7]](https://static.documents.pub/doc/80x56/5ee1cc87ad6a402d666c8c3a/volume-8-issue-5-may-2019-print-issn-no-2250-1991-brachytherapy-are.jpg)





