

The State of the Art of Invasive Candidiasis Management in Asia
Prof George Dimopoulos MD, PhD, FCCP
Department of Critical Care
Medical School, University of Athens, Greece
Indonesia, 13-15 April 2013

Worldwide incidence of Candida spp ARTEMIS project (134,715 isolates, 127 medical centres, 39 countries) (1991–2006)
Canada 415 isolates 1 study
USA 7,151 isolates 6 studies
Latin America 1,710 isolates
2 studies
Europe 2,089 isolates
8,923 isolates 7 studies
Asia-Pacific 1,344 isolates 1 study
Africa 73 isolates
C. albicans C. glabrata C. parapsilosis C. tropicalis C. krusei Other
Pfaller MA et al, Clin Microbiol Rev 2007;20:133–63,
Tortorano M et al Eur J Clin Micr Infect Dis 2004; 23:317–22, Colombo L et al. Eur J Clin Microbiol Infect Dis 2003;22:470–4

Candida spp the predominant fungal pathogen in the ICU setting
88%
7% 5%
Candida Aspergillus Other
Global surveillance study of
13,796 adults in 1265 ICUs
in 75 countries
Candida responsible for
88% of fungal infections
(n=963)
89% in Europe (n=633)
85% elsewhere (n=330)
Vincent JL et al. JAMA. 2009;302:2323–9

Candida non-albicans in the ICU 4 Geographically Diverse Intensive Care Units
0
20
40
60
80
100
2001 2002 2003 2004 2005 2006
% o
f p
ati
en
ts
0
20
40
60
80
100
Australia Belgium Greece Brazil
% o
f p
ati
en
ts
12
8
13
10
15
15
23
15
19
23
22
14
25
18
29
26
31
18
19
23
Per cent albicans and non-albicans
candidemia over study period
Per cent albicans and non-albicans
candidemia by country
Holley A, Dulhunty JM, Blot SI, Lobo S, Dancer C, Rello J, Lipman J, Dimopoulos G. Intern J Antimicrob Agents 2009

Predominance of Candida tropicalis BSIs in a Singapore teaching hospital
18-month investigation of Candida BSIs in a Singapore hospital where 52 candidemic patients were identified
- 36% C. tropicalis - 29% C. albicans - 10% C. parapsilosis - 21% C. glabrata
A predominant clonal C. tropicalis strain was demonstrated
No association with - ICU stay - prior exposure to fluconazole / broad-spectrum antibiotics or - increased mortality was found
Chai YA, Wang Y, Khoo AL, Chan FY, Chow C, Kumarasinghe G, Singh K, Tambyah PA.
Med Mycol. 2007 Aug;45(5):435-9.

Fungal Infections in India
Indian
Experience
with
Fungaemia

Management of invasive candidiasis
in ICUs in the Asia-Pacific Region
Candida albicans • Predominant cause in ICUs followed by C. tropicalis, C. glabrata and C. parapsilosis
Candida spp • Highly susceptible to fluconazole (>90%)
Asia-Pacific countries • Susceptibility rate of C. glabrata to fluconazole 22%- 72%
Early diagnosis- prompt initiation of antifungal therapy
Considerable regional variability • Local epidemiological knowledge is critical in Asia-Pacific
Hsueh PR et al, Int J Antimicrob Agents. 2009 Sep;34(3):205-9.

SHEEP meeting Sharing Eraxis Experience Program
TREATING INVASIVE FUNGAL INFECTIONS
John Simon,1 Hsin-Yun Sun,2 Hoe Nam Leong,3 Marie Yvette C Barez,4 Po-Yen
Huang,5 Deepak Talwar,6 Jen-Hsien Wang,7 Melor Mansor,8 Bambang Wahjuprajitno,9
Atul Patel,10 Siriporn Wittayachanyapong,11 B Shoib Mohd Sany,8 Sheng-Fong Lin,12
and George Dimopoulos13
1University of Hong Kong, Pokfulam, Hong Kong; 2National Taiwan University Hospital,
Taipei, Taiwan; 3Raffles Medical Hospital, Singapore; 4Davao Doctors Hospital, Davao,
The Philippines; 5Chang Gung Memorial Hospital, Taoyuan, Taiwan; 6Metro Group of
Hospitals and Heart Institute, Delhi, India; 7China Medical College-Hospital, Taichung,
Taiwan; 8Hospital Ampang, Kuala Lumpur, Malaysia; 9Dr Soetomo General Hospital,
Surabaya, Indonesia; 10Vedanta Institute of Medical Sciences, Ahmedabad, India; 11Bangkok-Pattaya Hospital, Chonburi Province, Thailand; 12Pfizer Inc., Hong Kong; 13National and Kapodistrian University of Athens and Department of Critical Care,
University Hospital “Attikon”, Athens, Greece
Sharing Eraxis Experience Program SHEEP meeting Hong Kong 7 October 2010
Mycoses 2013 (in press)

Worldwide incidence of Candida spp.
Data are originally from Pfaller et al. J Clin Microbiol, 2010; 48: 1366-1377 (DOI:
10.1128/JCM.02117-09) and have been reproduced/amended with permission from
American Society for Microbiology.

Predisposing and risk factors for Candida spp.
infections in critically ill patients
Host factors Iatrogenic factors
Neutropenia
Candida spp. colonization
Necrotizing pancreatitis
Gastrointestinal perforation
Acute renal failure
Bacterial sepsis
Malignant haematological disease
High Acute Physiology And Chronic
Health Evaluation (APACHE) II score
Diabetes mellitus
Increased age
Mucositis
Immunosuppressive therapy
Broad-spectrum antibiotic therapy
Total parenteral nutrition
Central venous catheter
Mechanical ventilation
Major surgical procedures
Leaking gastrointestinal anastomosis
Antineoplastic chemotherapy
Haemodialysis
Radiotherapy
Corticosteroids
Hospital environment

Predisposing Factors for
Fungal Infections in the ICU
Immune system alterations
↑ AIDS patients
Aggressive treatments
↑ BMT, SOT
↑ Number of elderly patients
Medical technology advances
Mechanical ventilation
Medical devices
Main risk factors
Chemotherapy (agent, dose, duration)
Radiotherapy
Corticosteroids
Immunosuppression
Antibiotics
Central venous lines
Mucositis
TPN/malnutrition
Hospital environment
Dimopoulos G, Vincent JL. Clin Intens Care 2002;13(1):1-12.

What we know………..
What we don’t know………..
What we practice………..

Overgrowth Modified microbiota
Diabetes Burns
Neutropenia Antibiotics
Prematurity
Mucosal colonization
Oropharyngeal Upper-Lower GT
Genital Tract Urinary Tract
Micro-invasion
Multiple antibiotics Vascular accesses
Parenteral nutrition ICU stay > 7 days
Candida colonisation Renal failure
Major abdominal surgery
Candidaemia
Candidaemia
Disseminated disease
Endophthalmitis Endocarditis
Catheter-related Abscess
CNS Hepatosplenic
Eggimann P, et al. Ann Intens Care 2011;1:37

…. the diagnosis is a challenge
Diagnosis is often delayed
• Non-specific signs and symptoms
• Cultures may become positive late
• Serologic tests or molecular methods
not currently used in clinical practice
• Blood cultures
positive in only approximately 50% of patients
Groll AH et al, J Infect 1996;33(1):23-32 Ellepola AN et al, J Microbiol. 2005;43:65-84
Diagnosis of fungal infections
Laboratory
• Microscopic Examination
• Culture & Identification
• Histopathology
• Antibody detection
• Antigen detection
• PCR
“High tech”
• Antibodies
• Metabolites
• Fungal cell wall components
• Fungal PCR
Van Burik J et al. J Clin Microbiol 1998;36:1169-75, Obayashi T et al. Lancet 1995;345:17-20, Yeo SF & Wong B, Clin Microbiol Rev 2002;15:465
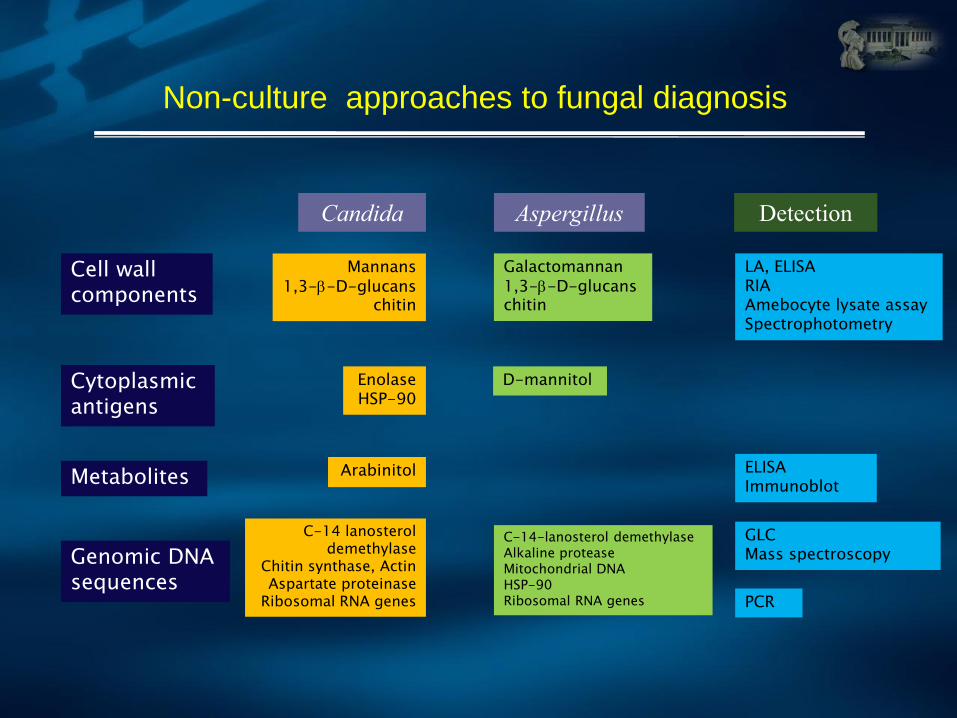
Non-culture approaches to fungal diagnosis
Candida Aspergillus Detection
Cell wall components
Cytoplasmic antigens
Metabolites
Genomic DNA sequences
Mannans 1,3--D-glucans
chitin
Enolase HSP-90
Arabinitol
C-14 lanosterol demethylase
Chitin synthase, Actin Aspartate proteinase
Ribosomal RNA genes
Galactomannan 1,3--D-glucans chitin
D-mannitol
C-14-lanosterol demethylase Alkaline protease Mitochondrial DNA HSP-90 Ribosomal RNA genes
LA, ELISA RIA Amebocyte lysate assay Spectrophotometry
PCR
GLC Mass spectroscopy
ELISA Immunoblot

(1,3)-Beta-D-Glucan Detection Glucatell® test, FDA license for IFI, May 21st, 2004
It takes 2 h
Test detects
yeast
filamentous fungi
no differential
diagnostic potential
No Detection
Mucorales
Cryptococcus spp.
Cut-off value
> 60 pg/ml
Specificity:
90% single test
96% for 2
sequential positive
results
Odabasi et al. CID 2004; 39: 199-205
Kinetics of BG

(1→3) Beta-D-glucan (BG) Assay Sensitivity in IFI
Fungitell 80 pg/ml +/total (%) Reference Year
Candidiasis 72/92(78%)
10/12 (83%)
13/15 (87%)
10/35 (29%)
Ostrosky
Odabasi
Pickering
Digby
2005
2004
2005
2003
Aspergillosis 10/10(100%)
4/4 (100%)
Ostrosky
Odabasi
2005
2004

Time to onset of candidemia and relation
between mortality and start of therapy
0
5
10
15
20
25
30
35
1-2 days 3-7 days 8-14days
15-21days
22-28days
>28 days
% CASES
Days of hospitalization
Garey 2006 CID
0
5
10
15
20
25
30
35
40
45
Culture day Day 1 Day 2 > Day 3
% Mortality
Days to start fluconazole

Empirical treatment using “Candida Score” in
non-neutropenic critically ill patient staying ≥ 7 days in ICU
León C, et al, Crit Care Med. 2009;37:1624-1633.
How to use “Candida Score”
Variables are coded (0) when absent and (1) when present (sever sepsis coded “2” when present)
A “Candida Score” ≥3 selected patients at high risk for invasive candidiasis (IC) – A linear association between increasing the value of CS and IC rate was observed (P≤0.001)
0 or 2
0 or 1
0 or 1
0 or 1

Early diagnosis of candidemia in the ICU (1-3)-b-D-glucan assay vs Candida score vs Colonization Index
Flow chart of the study patients ROC AUC curves of BG, CS and CI for proven IC cases The AUC of BG was significantly higher than those of CS (P < 0.001) and colonization index (P < 0.001)
Posteraro B et al, Crit Care 2011, 15:R249

Inappropriate treatment and outcome
No (%) of patients Fungal isolate
Inappropriate
treatment Hospital mortality Total
81 (96.4) 24 (28.6) 84 (53.5) C. albicans
25 (100) 6 (24) 25 (15.9) C. parapsilosis
19 (95) 8(40) 20 (12.7) C. glabrata
19 (95) 10(50) 20 (12.7) C. tropicalis
2 (100) 1 (50) 2 (1.3) C. krusei
Morrell et al AAC 2005

Catheter removal decreases mortality
Population-based candidaemia survey of 288 episodes of Candidaemia
in those with malignancies, including 150 in those with solid tumours
Removal of the central venous catheter at the time of or within 5 days of diagnosis of candidaemia decreased mortality (p=0.0096)
0 10 20 30
1.00
0.75
0.50
0.25
0.00
Analysis time(days)
Catheter removed after diagnosis Catheter not removed after diagnosis
Survivor function for removal of catheter
Slavin et al. J Antimicrob Chemother 2010
Just pull it out !!!!

Antifungal prophylaxis in critically ill patients ?
Guidelines Preemptive treatment
Prophylaxis
BSAC CID 1994 yes
Edwards CID 1997 data
Vincent ICM 1998 SDD ?
Rex CID 2000 yes, but
Buchner EJCMID 2002 yes at risk patients
Denning Lancet ID 2003
Pappas CID 2004 carfully selected pts
SFAR/SPILF/SRLF 2004 yes, but indication
FUNGINOS 2006 yes, but carfully selected pts
IDSA CID 2008 ? ?

AmB and Azoles
Amphotericin B
• Toxicity – nephrotoxicity
infusion-related toxicity
hypokalemia
hypomagnesemia
LFT abnormalities
• Limited efficacy (toxicity)
At times lack of efficacy mortality rates > 40%
• Lipid formulations
– too costly
Azoles
• Well tolerated
• Good safety profile
• Resistance Candida glabrata
Candida krusei (fluconazole)
• Cross resistance Candida glabrata (voriconazole)

In vitro antifungal susceptibilities of Candida from patients with IC in Kuala Lumpur Hospital
159 Candida species, patients with IC in Kuala Lumpur Hospital
Amphotericin B, fluconazole, voriconazole, itraconazole, caspofungin
C. albicans (71), C. parapsilosis (42), C. tropicalis (27), C. glabrata (12)
E-test, MIC breakpoits CLSI
- Amphotericin B, Voriconazole = best activities
1 C. lusitaniae R to amphotericin B
2 C. albicans, 2 C. parapsilosis, 1 C. tropicalis , 1 C. glabrata R to fluconazole
All these isolates showed cross-resistance to itraconazole
- MIC90 of itraconazole was highest for C. glabrata and C. parapsilosis
- Caspofungin was active against all the isolates except for 5 of C. parapsilosis
Amran F, Aziz MN, Ibrahim HM, Atiqah NH, Parameswari S, Hafiza MR, Ifwat M. Med Microbiol. 2011 Sep;60(Pt 9):1312-6.

Antifungal therapies - Clinical trials
Fluconazole AMB
Phillips, 1995
P=.04
Flu
AMB + Flu Rex, 2003
Voriconazole AMB->Flu
Kullberg, 2005
P=.82
Caspofungin Micafungin
Pappas, 2007
Micafungin
Liposomal AMB Kuse, 2007
P=.27
AMB
Caspofungin Mora-Duarte, 2002
P=.09 P=.64
Anidulafungin Fluconazole Reboli, 2007
P=.009 Fl
uco
naz
ole
(8
00
)
Am
ph
ote
rici
n B
+ F
lu
Cas
po
fun
gin
Mic
afu
ngi
n
L-A
mp
ho
teri
cin
B
Mic
afu
ngi
n
Cas
po
fun
gin
Am
ph
ote
rici
n B
Am
ph
ote
rici
n B
F
luco
naz
ole
Vo
rico
naz
ole
Flu
con
azo
le
An
idu
lafu
ngi
n
Am
ph
ote
rici
n B
Flu
con
azo
le
56%
69% 71% 72% 74% 70%
62%
73% 72% 72%
60%
76%
53% 50%
P=.39
Adapted from Kullberg BJ, et al. Lancet. 2007;366:1435-1442

2011 ESCMID Guidelines for Candida Diseases Targeted Treatment of Candidaemia in the ICU Setting
ECCMID, 2011 Milan EW16 Working Group, CMI 2012
Compound SoR QoE Comments
Echinocandins - Anidulafungin 200/100 mg daily
- Caspofungin 70/50 mg daily
- Micafungin 100 mg daily
A
I
Broad spectrum, safety, no drug-drug
interactions, C. glabrata and C. krusei rare resistance, fungicidal
Voriconazole B I Less broad spectrum that –candins,
drug interactions, IV in renal failure,
Fluconazole C I Limited spectrum, inferiority to
anidulafungin (high APACHE II scores)
Polyenes - Amphotericin B liposomal
- Amphotericin B lipid complex
- Amphotericin B colloidal dispersion
- Amphotericin B deoxycholate
B
C
D
D
I
IIa
Iia
I
Similar efficacy with echinocandins,
More AEs
Higher toxicity
Other antifungal classes or
combinations with biological agents
C or
D
No data or without superiority
regarding efficacy
SoR = Strength of Recommendation, QoE = Quality of Evidence.

Critically ill patient
Fungal infection
Suspected
Proven Blood cultures (+) Biopsy (+)
Targeted treatment according to - Guidelines
- Local Epidemiology
How to select the antifungal agent ?
Hemodynamically unstable patient
NO
Azole resistance Recent exposure
Local epidemiology Colonization
NO
FLUCONAZOLE
Alternatives -Echinocandins
-Voriconazole -L-AmphoB
YES
Alternative
L-AmphoB
Echinocandins
Risk factors (+) Clinical signs (-) Biomarkers (-) Mycology (-)
Prophylaxis Fluconazole
Risk factors (+) Biomarkers (+) Clinical signs (-) Mycology (-)
Pre-emptive Treatment
Risk factors (+) Clinical signs (+) Biomarkers (-) Mycology (-)
Empirical treatment
YES
Patient is stabilized ? Consider step-down to
Voriconazole or Fluconazole
Dimopoulos G et al J Crit Care 2013 (in press)
Echinocandins
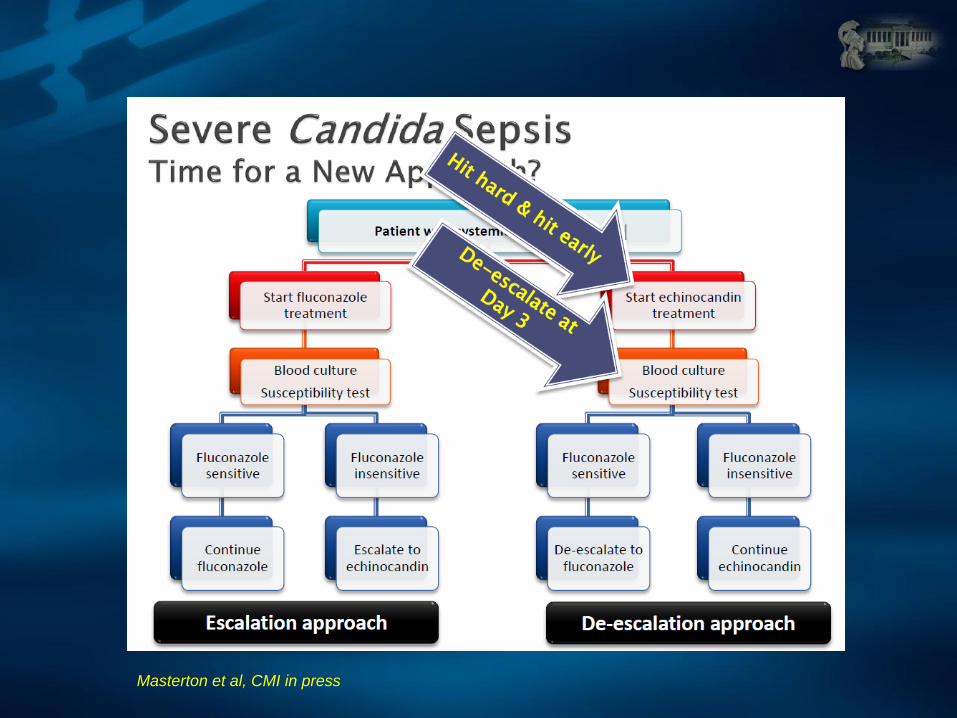
Masterton et al, CMI in press

Differences among echinocandins (I)
Variable Caspofungin Micafungin Anidulafungin
PAFE ± SD (h) Candida albicans
5.6 ± 0.57
5.0 ± 1.0
>12
MIC90 (µg/mL) All Candida spp.
C. albicans C. glabrata C. tropicalis C. krusei C. parapsilosis C. guilliermondii
0.25 0.06 0.06 0.06 0.25
1 1
1
0.03 0.03 0.06 0.12
2 1
2
0.12 0.12 0.06 0.06
4 2
Cmax (g/mL) 9.9 10.1 7.2
t½ (h) 9–11 11–17 24–26
Volume of distribution (L/kg) * 0.26 0.57
AUC (mg·h/L) 87.9–114.8 11.3 44.4–53.0
Protein binding, % 96 99.8 84
Mycoses 2013 Sharing Eraxis Experience Program
SHEEP meeting
Hong Kong 7 October 2010

Differences among echinocandins (II)
Variable Caspofungin Micafungin Anidulafungin
Metabolism
Hydrolysis and N-acetylation.
Spontaneously degrades to
inactive product
Catechol-O- methylt-
ransferase Pathway Chemical degradation
Clearance (mL/min) 10.0–12.5 10.5 12.5–19.2
Elimination 35% faeces. 41% urine
(1.4% as unchanged drug)
40% faeces.
<15% urine
Primarily in faeces
(<10% intact drug), 1% urine
CSF penetration* ? low ? low <0.1%
Urinary concentration* 1.4% 0.7% <0.1%
Renal insufficiency No dose adjustment needed No dose adjustment needed No dose adjustment needed
Hepatic insufficiency
Child-Pugh 7–9: (Reduce
maintenance dose to 35 mg/day)
Child-Pugh >9: No data
Child-Pugh 7–9)
Cmax not significantly
decreased compared with
healthy subjects
No dose adjustment needed
*% of plasma)
Simon et al , Mycoses 2013
Sharing Eraxis Experience Program SHEEP meeting Hong Kong 7 October 2010

Economic Evaluation of Micafungin for the Treatment
of Candidaemia and Invasive Candidiasis
Vs Caspofungin
• micafungin (AU$52,816) : lower total
cost than caspofungin (AU$52,976)
• Net cost-saving of $160 per patient
• Lower cost associated with alternative
antifungal treatment in the micafungin
arm
• Micafungin was cost-equivalent to
caspofungin in treating candidaemia/IC
Vs Liposomal Amphotericin B
- micafungin (AU$61 426) : lower total cost
than LAmB (AU$72 382)
- Net cost-saving of AU$10 957 per patient
- lower cost associated with initial antifungal
treatment and shorter length of stay for
patients in the micafungin arm
- Micafungin was non-inferior to liposomal
amphotericin B (LAmB) for the treatment
of candidaemia and IC
Main outcomes ( treatment success and treatment failure due to mycological persistence, or death
Neoh CF et al, Mycoses. 2013 Mar 18. doi: 10.1111/myc.12071 Neoh CF et al, Intern Med J. 2013 Mar 6. doi: 10.1111/imj.12110.

Persistent Candidemia : what you have to do ?
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Study Day
0
10
20
30
40
50
60
70
80
90
100%
Caspofungin (N=92)
Amphotericin B (N=94)
20% still candidaemic by Day 4
11% still candidaemic by Day 7
6% candidaemic beyond Day 10
Time to clearance of Candida from the blood stream
% o
f p
atients
still
ca
nd
idaem
ic
Mora-Duarte et al. N Engl J Med 2002

Prolonged candidaemia
Post-op Hickman cath-related Candidaemia and tissue involvment
Vitreous body aspirate C. albicans
Septic thromphoplebitis of the left subclavian and jugular vein
due to Candida albicans

Rare fungal infections in the ICU
Digital nephrostomogram from the left (a)
and right (b) nephrostomy catheter depicts
moderate dilatation and multiple fillings
defects which are caused by the fungus balls
located in the pelvicalyceals systems.
Digital nephrostomogram obtained fifteen
days following the bilateral percutaneous
nephrostomies depict resolution of the
filling defects of the both the left (A), and
the right (C) kidneys. Note good patency
of the distal anastomosis (B).
Dimopoulos et al, Mycoses (under review)

Rare fungal infections in the ICU
Dimopoulos et al, Mycoses (under review)
Candida meningitis
Brain MRI showing high signal intensity of
fast fluid attenuated inversion recovery
(FLAIR), involving periventricular and
subcortical gray matter of bilateral brain
hemispheres, hippocampus, internal capsule
bilaterally, thalami, pons, cerebral peduncles
and substantianigra of midbrain.

Rare fungal infections in the ICU
Dimopoulos et al, Mycoses (under review)
Necrotic lesions with a blackish
escharto the left cheek and upper
lip, extended rapidly to the tongue
and the hard and soft palate.
Chest computer tomography revealing
thrombophlebitis of left internal jugular vein, left
subclavian vein and left brachiocephalic vein.

Practical
Scientific
Prospective clinical trials
Animal studies In vitro studies
Mechanisms of synergy
Spectrum of therapy Intensity of therapy
Safety of therapy
Pragmatism vs. Science and
Decisions to Use Combination Therapy
Lewis REL & Kontoyiannis DP. Br J Hematology 2005

In conclusion
• Fungal infections in Asia
– Local epidemiology
– Risk factors
– Early Diagnosis
– Prevention
- Prophylaxis (selected cases in the ICU)
- Antifungal agents - safe
- well tolerated and
- with broad spectrum activity
- Echinocandins - Attractive option
- Differences among them (mainly safety and Pk/PDs)







