

THE S U R G I C A L A P P R O A C H TO NASAL GLIONIA
By PETER O'BRIEN, F.R.C.S.Ed.
Canniesburn Hospital, Glasgow
NASAL glioma is a comparatively rare tumour, approximately xoo cases being reported in the literature since the lesion was first described by Schmidt in I9OO. In 195 o, Black and Smith reviewed 34 cases and Smith et al. in 1963 reviewed these cases plus another 55.
Nasal gliomas appear to arise in a similar manner to encephaloceles (Schmidt, 19oo). During foetal development, a portion of neuro-ectoderm becomes isolated from the developing brain outside the skull, either in the olfactory region of the nasal cavity beneath the nasal mucosa or subcutaneously over the root of the nose. The tumour may be completely sequestrated or it may have a stalk which passes through a hole in the cribriform area to be connected to the brain or meninges. Smith et al. (I963) quotes 14 of 48 cases he studied to have intracranial connections. Should this stalk be avulsed during surgery via the nasal approach it is possible to produce cerebrospinal rhinorrhoea, which is unlikely to cease spontaneously and will require frontal craniotomy and repair of the dural defect in the anterior cranial fossa ; otherwise early meningitis is likely, as reported by Jamieson (1965).
Three types of nasal glioma are recognised : approximately 60 per cent. are extra- nasal, 3 ° per cent. are intranasal while IO per cent. are mixed, part being intranasal and part extranasal (Smith et al., 1963).
The mixed type originates beneath the nasal mucosa and with growth extends either through or under the lower edge of the nasal bones to present subcutaneously. All types can produce marked deformity due to pressure on the nasal skeleton and adjoining maxilla and orbital walls.
The tumour is benign and has no autonomous growth, its increase in size in p ro- portion to that of the body as a whole, and it has never been reported as being malignant. The histological features are usually aggregations of astrocytes surrounded by fibrous tissue and a capsule which is formed of processes of fibrous astrocytes, fibroblasts and collagen. Mitotic figures are not found but occasional giant multinucleated astrocytes are present.
Nasal glioma may often be suspected at birth as the majority present as a swelling over the root of the nose, not attached to the skin and of rubbery consistency. It must be differentiated from other lesions which may occur in this area in the infant, including encephalocele, dermoid and angioma. Biopsy is necessary to establish a definite diagnosis.
"Because of the uncommon nature of the turnout, considerable attention in the recorded cases has been given to a~tiology, pathogenesis and diagnosis ; but the surgical approach to these lesions has received less attention than warranted. According to Smith et al. (1963) in the 93 cases he reviewed there were I I recurrences after surgical excision, but following a second surgical attack on these, there was only one further recurrence. It is probable that these figures indicate incomplete excision at the first operation and it seems that recurrence is unlikely if the turnout is removed completely at the first procedure.
Once a nasal glioma is diagnosed clinically, it is helpful to know if there is an intra- cranial connection before attempting excision via the nasal approach. Smith et al. (1963) recommended that excision via the nasal approach should always be preceded by cranio- tomy, this being the only reliable means available to determine the presence of intra- cranial connections of the tumour. Should there be a cribriform area defect, the pedicle
30

THE SURGICAL APPROACH TO NASAL GLIOMA 3 I
of the tumour is divided and pushed down into the nasal cavity beneath the mucosa and the dural defect is closed. Then at a second operation some months later, the tumour can be excised. Should, however, nasal excision be embarked upon as the first procedure, a cerebrospinal fluid leak should be dealt with immediately by craniotomy and repair.
The surgical approach most often described for excision o f nasal glioma is a lateral rhinotomy to expose the nasal bone which is then elevated to remove the lesion. Occa- sionally the tumour is removed via the nostril using punch forceps. Hage (I95o) describes a method of exposure which elevates the nasal skin from the nasal cartilages which are then divided in order to provide wide exposure of the nasal cavity.
The ideal surgical approach should allow the posterior and superior limits of the tumour to be defined clearly so that the connection to the cribriform area can be identified and divided under direct vision. Removal of the lesion using punch forceps may readily create a cercbrospinal fluid leak. I f the nasal deformity which results f rom long con- tinued pressure should be marked, it is probably best corrected at this operation and an exposure of the nasal bones and adjoining maxilla would be advantageous. I f possible, the incisions should be placed in positions where scarring will be either minimal or invisible.
Case Repor t . - -The patient was noticed to have a small swelling of the left side of the nose soon after birth. She was kept under observation for 2½ years and was then referred to a neurosurgical unit where bifrontal craniotomy was performed. The anterior cranial fossa was found to be quite normal and nothing further was done at this stage. At 4½ years she was referred to Mr J. C. Mustards by the otolaryngologist under whose care she was and was admitted to this unit for excision of the turnout.
On examination a swelling 0.75 cm. in diameter presented subcutaneously at the lower border of the left nasal bone. It was rubbery in consistency and was firmly attached deeply. The nasal septum was deviated to the right, almost blocking the right nostril and there was considerable widening of the space between the medial canthi. The nasal bones were widely splayed and a gap approximately 0"5 cm. wide was palpable between them. However, this splaying had not caused the eyes to be displaced laterally and there was hence no hypertelorism (Fig. I). X-ray confirmed this distortion together with the marked deviation of the nasal septum (Fig. 2).
Operation (Mr J. C. Mustardd).--Under endotracheal anaesthesia a solution of cocain and adrenaline was applied to the nasal mucosa to reduce bleeding.
An endonasal incision was made between the upper and lower alar cartilages on each side. This was extended through both layers of the mucosa of the membranous septum and the columella was divided transversely at about its middle. Laterally the incisions were extended through the full thickness of the alar base into the alar-facial fold and in this groove as far upwards as its upper limit (Fig. 3). By blunt dissection the nasal skin and subcutaneous tissue were separated from the upper alar cartilages and the nasal bones. This gave excellent exposure of the superficial aspect of the tumour protruding below the lower edge of the left nasal bone. The turnout was dissected from the periosteum of the nasal bone and from the overlying nasal mucosa. It could then be followed medially on to the nasal septum on which it extended posteriorly under the mucosa for approximately 2 cm. During dissection a fine stalk of similar tissue was found to extend up into the cribriform area. It was quite easy to retract the deformed bones upwards and to remove the stalk completely with the tumour (Fig. 4). No cerebrospinal fluid was seen to issue from the olfactory area.
Following removal of the mass which was supporting the nasal bridge, the nasal bones tended to collapse, as very little support was provided by the badly buckled nasal septum. The nasal bones and adjoining maxilla were moulded into shape, so as to produce a normal looking midline nasal prominence. In order to hold the bones in this position and prevent post-opera- tive collapse of the nasal bridge, it was decided to pass a wire from one medial canthal ligament to the other. A bone awl was inserted through a small vertical incision just in front of the right medial canthus and was passed through the right fronto-nasal process of the maxilla and the
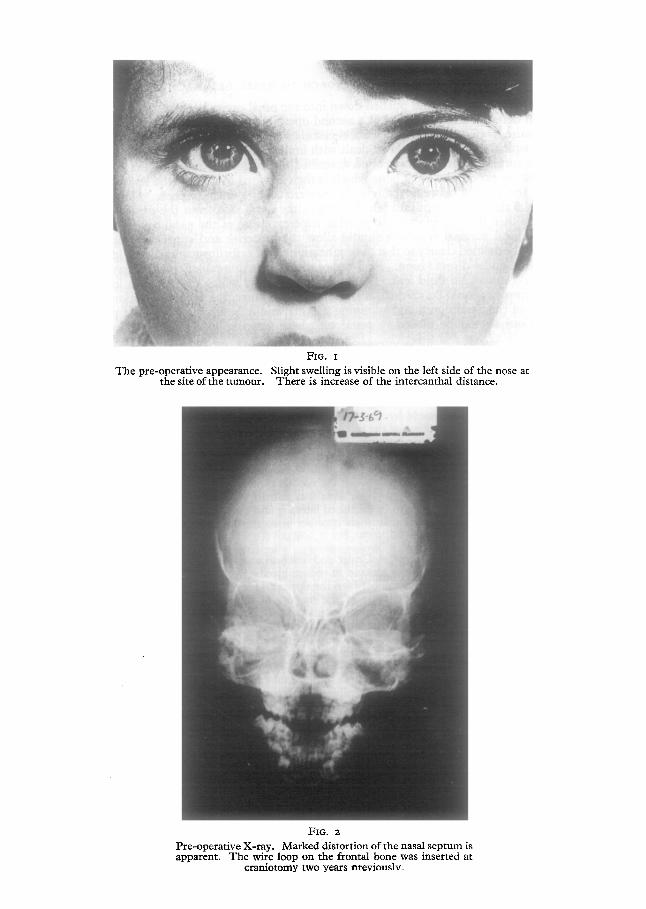
T h e pre-opera t ive appearance. the site o f the m m o u r .
FIG. I
Slight swell ing is visible on the left side of the nose at T h e r e is increase o f the in tercanthal distance.
FIG, 2
Pre-opera t ive X-ray . M arked dis tor t ion o f the nasal s e p t u m is apparent . T h e wire loop on the frontal bone was inserted at
c ran io tomy two years nreviouslv-

THE SURGICAL APPROACH TO NASAL GLIOMA 33
FIG. 3
Shows the nasal incision. T h e awl comes f rom a small incision just medial to the medial canthus th rough nasal bones and sep tum to emerge th rough a similar incision
on the other side.
J
FIG. 4
The nasal skin and alar cartilage reflected to show access. T h e tumour has been removed at this stage.

34 BRITISH JOURNAL OF PLASTIC SURGERY
Fit . 5 Eight days post-operation. At this early stage the incision marks are
disappearing rapidly.
FIG. 6 Eight days post-operation.

THE SURGICAL APPROACH TO NASAL GLIOMA 35
nasal septum so that it emerged through a similar incision on the left. A steel wire (I9 S.W.G.) was looped through the right canthal incision. It was then sutured through the right canthal ligament and the loop was tightened by twisting so as to provide support to the maxillary pro- cesses and the nasal bones. The telecanthus was slightly reduced and could probably have been reduced much more by further tightening of the wire. The small canthal incisions were sutured and the extranasal and intranasal incisions were closed using 6-0 chromic catgut. A plaster splint was applied and nasal packs were inserted.
The Pathology Report.w" A polypoid piece of tissue 3"5 × 2 × I cm. sections show the lesion to have abundant glial tissue with astrocytes, some of which are multinucleated and scattered true nerve cells. Foci of calcification are present in the lesion."
Discussion
This surgical approach proved satisfactory for excision of the nasal glioma by providing wide access to the nasal cavity and allowing the deformity to be corrected simultaneously with excision of the tumour.
A somewhat similar approach is described in Hage's paper (I96O), but his incision begins as a para-marginal one stripping the skin from alar and upper cartilages. The incision differs in the described case in that it was made between the upper and alar cartilages hence the position of the alar cartilage in its relationship to the skin was not disturbed and by retracting these alar cartilages upwards, a much wider exposure is achieved.
SUMMARY
A case of nasal glioma is described together with a method of surgical excision.
I am indebted to Mrff. C. Mustardd and Mr T. Gibson for their help in producing this paper and to Mr A. Mcllroy for the photographs.
REFERENCES
BLACK, B. K. and SMITH, D. E. (195o). Archs Neurol. Psychiat., Chicago, 64, 614. HAGE, J. (I960). Br. ft. plast. Surg. i2, 327. ]AMIESON, K. G. (1965). Pediatrics, 35, 342. SCHMIDT, M. D. (19oo). Virchows Arch. path. Anat. Physiol. 164, 340. SMITH, J. R., JR., SCHWARTZ, H. G., LOSE S. A0 and OGURA, J. H. (1963). ]. Neurosurg.
20, 968.







