

1
“These data can inform policy discussion”
Am J Hum Genet, October 3, 2013, 93:631-40

2
Compare incidental findings (IFs) to prediction analysis
Nature, 470:748-52
prediction IFs
p known known/unknown
b Known (estimated) something actionable
x common variants rare variants inside Mendelian genes
3
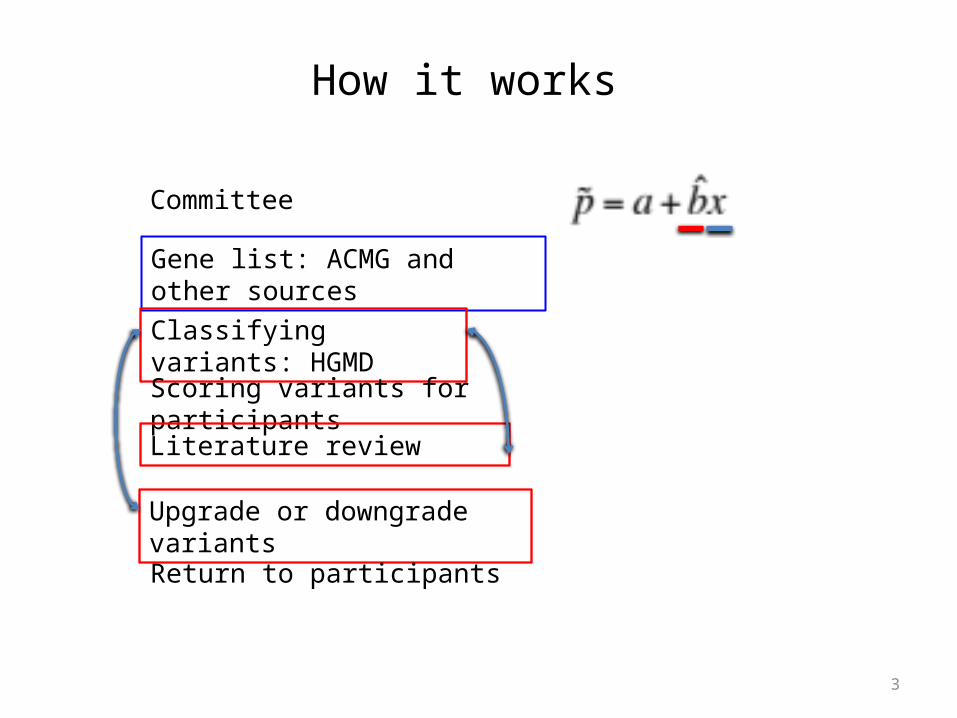
Committee
Gene list: ACMG and other sources
Classifying variants: HGMD
Scoring variants for participants
Literature review
Upgrade or downgrade variants
Return to participants
How it works

4
Data
• 500 EA, 500 AArandomly selected from 6,500 (~4,300 EA, ~2,200 AA) NHLBI Exom Project (Nature, 2013, 493:216-20)
• Exome Variant Server / Exome Sequencing Project• 114 genes (56 from American College of Medical Genetics and Genomics)
52 of the 56 gene are associated with adult-onset conditions

5
Return of Results Committee
• 24 experts (340 clinician years of medical genetics)• 14 practicing clinical medical geneticists• Two genetic counselors• Several other physicians and nonphysicians
• Other coordinating members help send literatures

6
Actionable genes• “’Actionable’ genes in adults were defined as having deleterious
mutation(s) whose penetrance would result in specific, defined medical recommendation(s) both supported by evidence and, when implemented, expected to improve an outcome(s) in terms of mortality or the avoidance of significant morbidity.”
• Actionable Genes are in Table 1, including 56 genes recommended by The American College of Medical Genetics and Genomes (Genet Med, 2013, 565-75), such as BRCA1 — breast cancerMSH2 – colon cancerSTK11 — Peutz-Jeghers syndromeVHL – Von Hippel-Lindau syndrome
Do they sound actionable?At least to somebody, they do.“My medical choice” New York Times, May 14, 2013, Angelina Jolie.

7
Classifying variants• Pathogenic (return to participants)• A likely pathogenic variant of uncertain
significance (VUS) (return to participants)• A VUS (if may cause potential diseases or
comorbidity)• A likely benign VUS
• Low MAF (<0.005)• de novo• More than one reported unrelated case• High cosegretation (1/16)
Database:Human Gene Mutation Database (HGMD), PubMed, Google.
8
Expert variant review
• 239 unique variants were identified• Checking the MAF• Reviewing the primary literature for evidence for
pathogenicity• Difficult-to-categorize variants: double-, triple-review

9
114 actionable genes
• 114 genes (Table 1)88 autosomal-dominance (AD)4 X-linked22 autosomal-recessive (AR)
• 239 (585 times) unique variants were identified as potentially pathogenic230 were in AD3 were in X-linked6 were in AR loci

10
Stats for these 239 variants
• 72/239 have MAF < 0.005 (not clear how MAFs were calculated or from)None of these 72 were pathogenic or likely
• 123/239 were observed once• 16 were pathogenic or likely:
15 were observed once in 1,000 subjects1 was observed in two subjects

11
Variants up and down
• Downgraded one from pathogenic to VUSone from likely pathogenic VUS to VUS
• Upgradedone was upgraded from VUS to likely VUS
• Five mutations, not listed in HGMD as disease-causing, were predicted to be disruptive.

12
Variants that are too common
• rs146102241, and rs15082281 in PKP2 (arrhythmogenic right ventricular cardiomyopathy, prevalence/incidence < 1 in 1,000)MAF=0.005 in 500 European-descent participants0.005 and 0.003 in ESP
• rs149633775 in TP53 (Li-Fraumeni syndrome, prevalence/incidence < 1 in 20,000)MAF=0.001 in 500 European-descent participants0.0004 in ESP

13
Variants by ancestry group• 419/585 (71.5%) were in EA• 146/585 (25.0%) were in AA• 20/585 (3.4%) were in Jewish descent
• 94 of 239 unique variants were found in AA.
• In pathogenic group: 7 EA, 2 AAIn likely pathogenic group: 8 EA, 2 AA
14
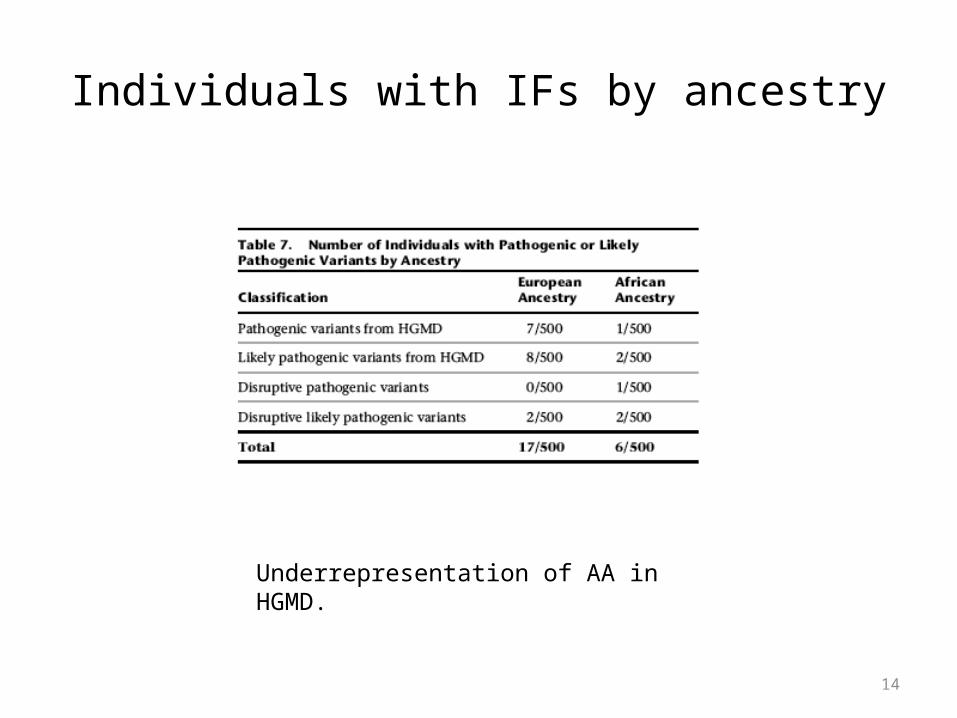
Individuals with IFs by ancestry
Underrepresentation of AA in HGMD.

15
18 participants carry pathogenic variants
• 16 unique AD variants in 17 participants• 1 AR variant pair were pathogenic or likely
• 8 with confirmed pathogenic mutations (versus likely pathogenic)BRCA1LDLR (familial hypercholesterolemia)PMS2 (Lynch syndrome)SERPINA1 (alpha-1-antitrypsin deficiency)

16
Time for literature review
• 5,636 min for 239 unique variants• Average 23 min (1-135 min)
• Would have been substantially more time if review was conducted for 585 variants on a per person basis
• Per variant or per person?
17
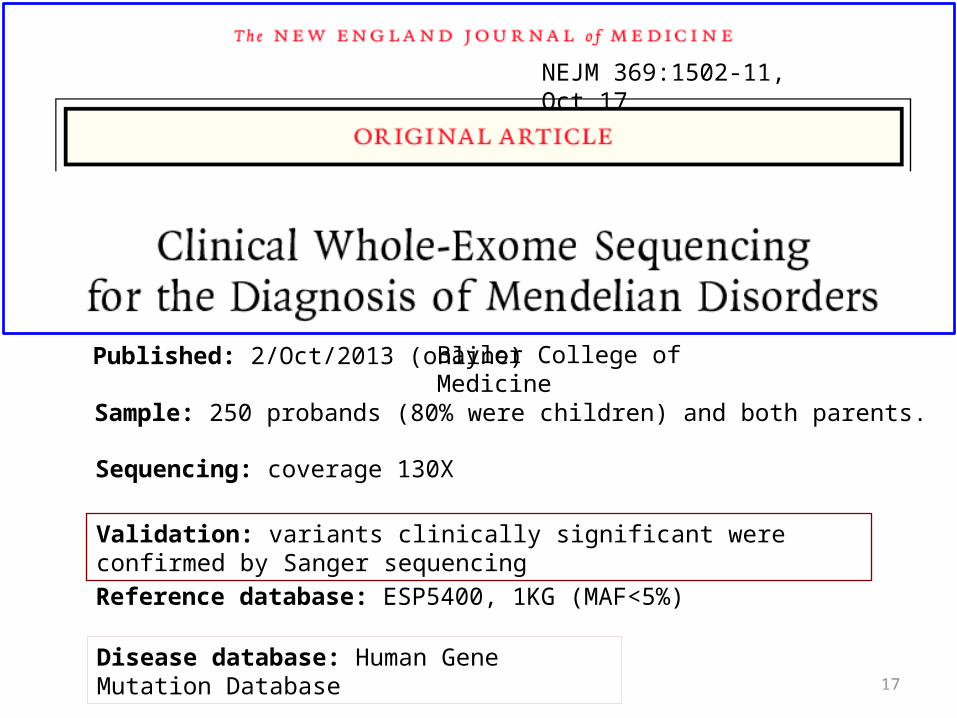
Baylor College of Medicine
Sample: 250 probands (80% were children) and both parents.
Sequencing: coverage 130X
Validation: variants clinically significant were confirmed by Sanger sequencing
Reference database: ESP5400, 1KG (MAF<5%)
Disease database: Human Gene Mutation Database
Published: 2/Oct/2013 (online)
NEJM 369:1502-11, Oct 17
18
Results
• 62 of 250 patients had total 86 mutated alleles that were highly likely to be causative.Achieved 25% molecular diagnostic rate.
• Incidental findings: 30 of 250 patients had medically actionable incidental findings in 16 genes.12% compared with 1.8% in AJHG paper.

19
Insurance coverage

20
Reporting
• Tier one: focused on the disease phenotype and included deleterious mutations and UCS related to the phenotype.
• Tier two: provided if they were requested by the physician or the patient
• Expanded report: mutations (of unknown clinical significance) were monitored every 6 months for new discovered disease genes.Once a match was found, report to the physician.Sounds horrible~

21
Using 1KG as the reference data.On average, every individuals carries 2 disease-causing mutation.Validated the rare variants in 1KG.

22
Some questions• How common/rare is common/rare for a disease?• Which MAF? 500 EA? 500 AA? 4,300 EA? 2,200 AA?• Expert review? To make sense for each patient or for all?• As a patient, how much would you like to know?• Low disease-causing mutations:
stringent criteriareporting criteria: not to return VUSs to participants for Ifs in genes unrelated to the presenting condition.

23
Exome Variant Server@Seattle
24
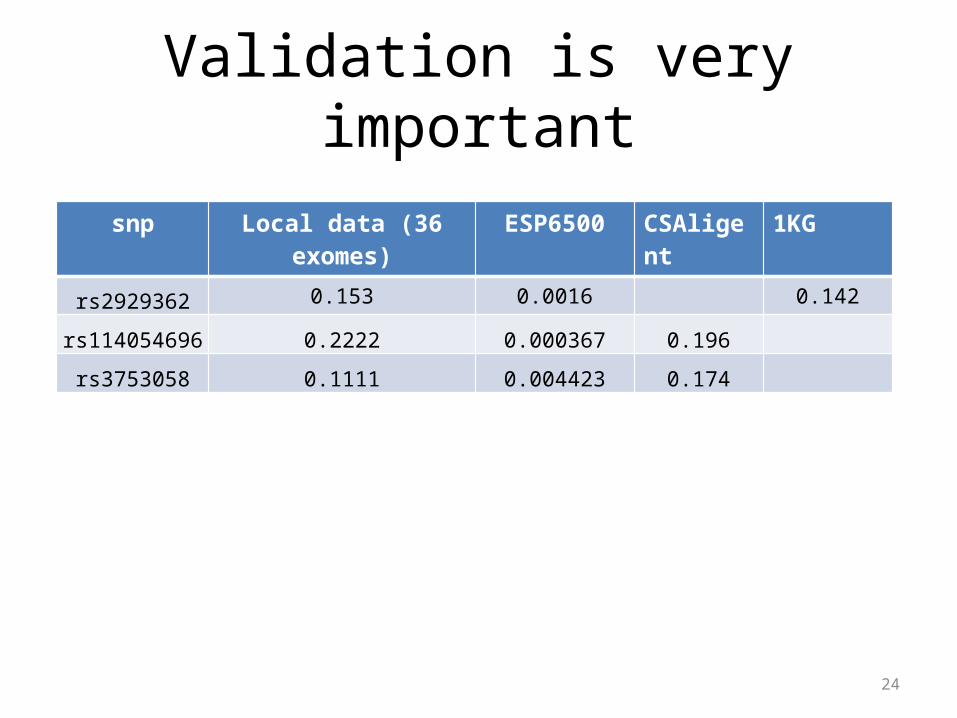
Validation is very important
snp Local data (36 exomes) ESP6500 CSAligent 1KG
rs2929362 0.153 0.0016 0.142
rs114054696 0.2222 0.000367 0.196
rs3753058 0.1111 0.004423 0.174
25
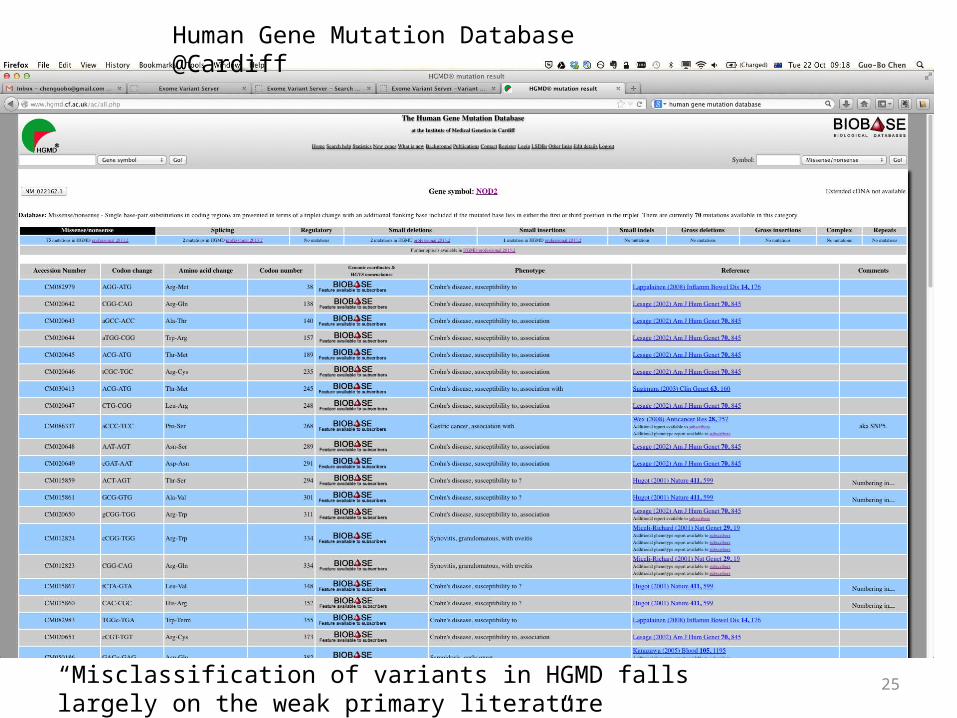
Human Gene Mutation Database @Cardiff
“Misclassification of variants in HGMD falls largely on the weak primary literature rather than HGMD extraction errors”

26
Patient autonomy• Whole-genome sequencing in health care
EJHG, 2013, May, 21:580-4• Call for prudence in whole-genome testing
Science, 2013, August, 341:958-9







