
Third Sino-U.S. Conference on Third Sino-U.S. Conference on Medical ProfessionalismMedical ProfessionalismThird Sino-U.S. Conference on Third Sino-U.S. Conference on Medical ProfessionalismMedical Professionalism
Allan M. Korn M.D., FACPAllan M. Korn M.D., FACP
Blue Cross Blue Shield AssociationBlue Cross Blue Shield Association
Happier DoctorsHappier DoctorsHealthier PatientsHealthier Patients
2© 2008 Blue Cross Blue Shield Association
Happier Doctors, Healthier PatientsHappier Doctors, Healthier Patients
● Evidence Based Care
● Better Outcomes
● Meaningful doctor-patient relationship
● Durable doctor-patient relationship
● Trusting doctor-patient relationship
● Much more pride in medical practice
● The basis for a harmonious society
3© 2008 Blue Cross Blue Shield Association
Medical ProfessionalismMedical Professionalism
● Results in more satisfaction with clinical practice
● Results in patients trusting you while engaging in their own care
● Nurtures trust between doctors, hospitals and patients
● Meets the needs of society with personal pride and scientific accuracy
● Opens minds, opens hearts, and demands integrity in all that is done for patients, peers, and nation.
4© 2008 Blue Cross Blue Shield Association
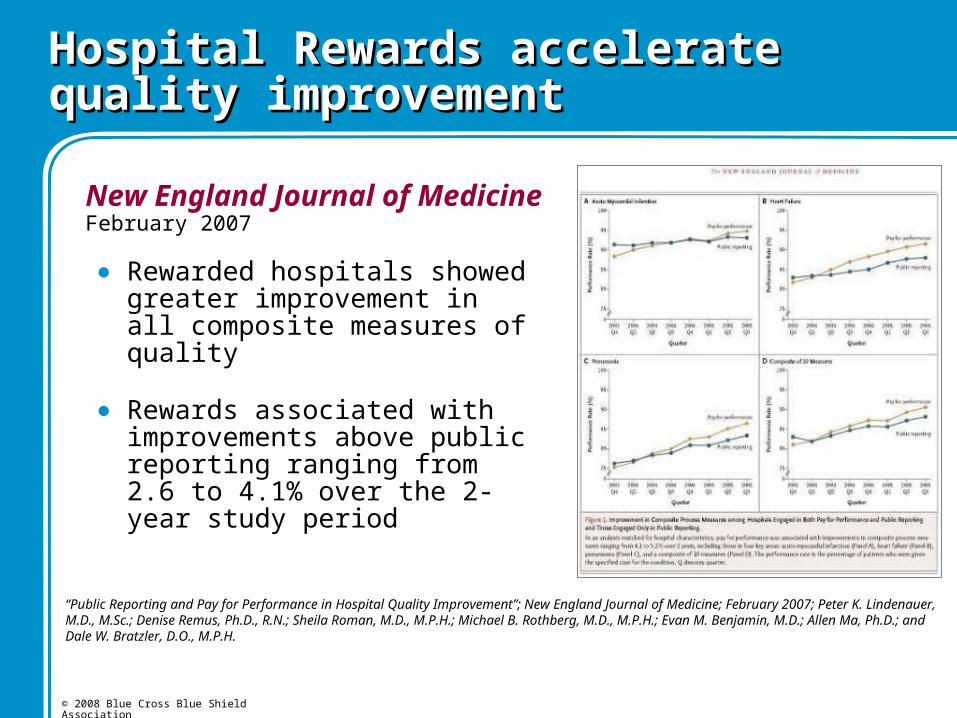
Hospital Rewards accelerate quality improvementHospital Rewards accelerate quality improvement
New England Journal of Medicine February 2007
“Public Reporting and Pay for Performance in Hospital Quality Improvement”; New England Journal of Medicine; February 2007; Peter K. Lindenauer, M.D., M.Sc.; Denise Remus, Ph.D., R.N.; Sheila Roman, M.D., M.P.H.; Michael B. Rothberg, M.D., M.P.H.; Evan M. Benjamin, M.D.; Allen Ma, Ph.D.; and Dale W. Bratzler, D.O., M.P.H.
● Rewarded hospitals showed greater improvement in all composite measures of quality
● Rewards associated with improvements above public reporting ranging from 2.6 to 4.1% over the 2-year study period
5© 2008 Blue Cross Blue Shield Association
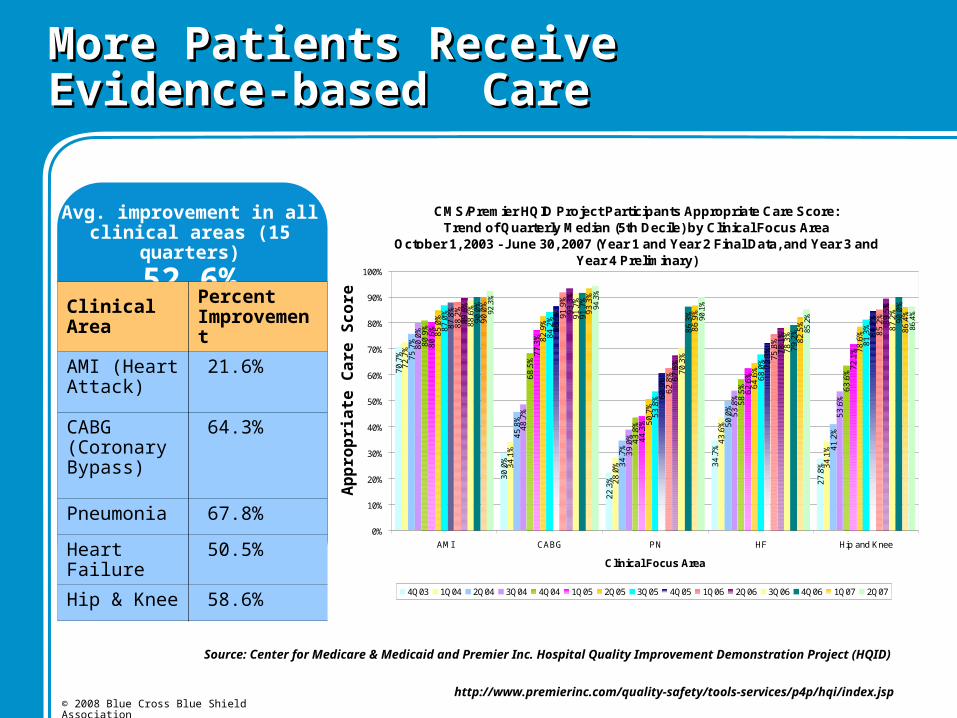
CMS/Premier HQID Project Participants Appropriate Care Score: Trend of Quarterly Median (5th Decile) by Clinical Focus Area
October 1, 2003 - June 30, 2007 (Year 1 and Year 2 Final Data, and Year 3 and Year 4 Preliminary)
70
.7%
30
.0%
22
.3%
34
.7%
27
.8%
72
.7%
34
.1%
28
.0%
43
.6%
34
.1%
75
.7%
45
.8%
34
.7%
50
.0%
41
.2%
80
.0%
48
.7%
39
.0%
53
.8%
53
.6%
80
.9%
68
.5%
43
.8%
58
.5% 63
.6%
80
.6%
77
.3%
44
.3%
62
.6%
72
.1%
85
.0%
82
.9%
50
.7%
64
.6%
78
.6%
87
.0%
84
.2%
53
.8%
68
.0%
81
.3%8
7.8
%
86
.6%
60
.9%
72
.3%
84
.7%
88
.2%
91
.9%
62
.8%
75
.8%
85
.2%
89
.6%
93
.3%
67
.6%
78
.1%
89
.5%
88
.6%
91
.7%
70
.3%
78
.3%
87
.2%
90
.0%
91
.7%
86
.3%
79
.2%
90
.0%
90
.0%
93
.3%
86
.9%
82
.5%
86
.4%92
.3%
94.3
%
90.1
%
85.2
%
86.4
%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
AMI CABG PN HF Hip and Knee
Clinical Focus Area
4Q03 1Q04 2Q04 3Q04 4Q04 1Q05 2Q05 3Q05 4Q05 1Q06 2Q06 3Q06 4Q06 1Q07 2Q07
More Patients Receive Evidence-based Care More Patients Receive Evidence-based Care
Avg. improvement in all clinical areas (15 quarters)
52.6%Clinical Area
Percent Improvement
AMI (Heart Attack)
21.6%
CABG (Coronary Bypass)
64.3%
Pneumonia 67.8%
Heart Failure 50.5%
Hip & Knee 58.6%
Ap
pro
pri
ate
Ca
re S
co
re
Source: Center for Medicare & Medicaid and Premier Inc. Hospital Quality Improvement Demonstration Project (HQID)
http://www.premierinc.com/quality-safety/tools-services/p4p/hqi/index.jsp
6© 2008 Blue Cross Blue Shield Association
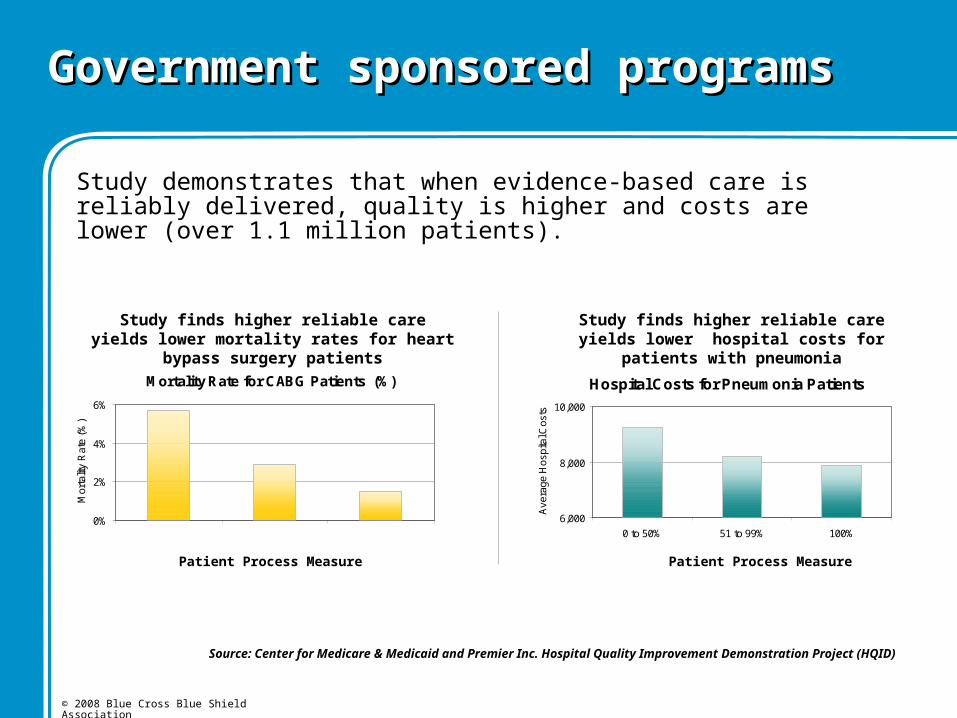
Government sponsored programs Government sponsored programs
Hospital Costs for Pneumonia Patients
6,000
8,000
10,000
0 to 50% 51 to 99% 100%A
vera
ge H
ospi
tal C
osts
Study demonstrates that when evidence-based care is reliably delivered, quality is higher and costs are lower (over 1.1 million patients).
Mortality Rate for CABG Patients (%)
0%
2%
4%
6%
0 to 49% 50 to 74% 75-100%
Mor
talit
y R
ate
(%)
Patient Process Measure Patient Process Measure
Study finds higher reliable care yields lower mortality rates for heart bypass surgery patients
Study finds higher reliable care yields lower hospital costs for patients with pneumonia
Source: Center for Medicare & Medicaid and Premier Inc. Hospital Quality Improvement Demonstration Project (HQID)
7© 2008 Blue Cross Blue Shield Association
Findings from Government sponsored Findings from Government sponsored programs programs
● Financial incentives combined with public reporting of transparent data can drive significant improvement in quality
– Hospitals held the gains and continued to improve
● More patients are reliably receiving evidenced-based care
● Improved quality is associated with saving lives and reducing costs

8© 2008 Blue Cross Blue Shield Association
Designation for quality recognition in physician directories, award certificates for office display, etc.
Recognition
Aligning incentives is a key driver for successful collaboration.
Physician Specialist IncentivesPhysician Specialist Incentives
Integration of American Board of Internal Medicine Practice Improvement Modules, or
Blue Cross Blue Shield quality based recognition programs, or
Special recommendations to patients to seek physicians and hospitals which have achieved high-quality, evidence-based care.
Reward
9© 2008 Blue Cross Blue Shield Association
Evidence: Recognized physicians have Evidence: Recognized physicians have higher quality results!higher quality results!
Study 1 examined routine screening for a variety of patients:– Cancer screening
– Routine laboratory screening for diabetics
– Routine laboratory screening for heart disease patients
– Routine laboratory screening for hypertensive patients
Study 2 examined several dimensions of diabetic care:– Routine laboratory screening
– Eye exams
In two separate studies, it was demonstrated that recognized physicians score higher at essential elements of patient care.
10© 2008 Blue Cross Blue Shield Association
When Primary Care Doctors Treat Patients… When Primary Care Doctors Treat Patients…
● Chronic diseases receive better care – Patients with congestive heart failure had 35% fewer hospital days;
– Patients with diabetes had significant reductions in cardiovascular risk;
– Asthma and diabetes patients were more likely to receive appropriate therapy.
● Access to needed care, receipt of routine preventive screenings, and management of chronic conditions improve substantially.
● If every American had access to comprehensive primary care, national health care expenditures would drop by 5.6% -- equal to national savings of at least $67 billion per year.
11© 2008 Blue Cross Blue Shield Association
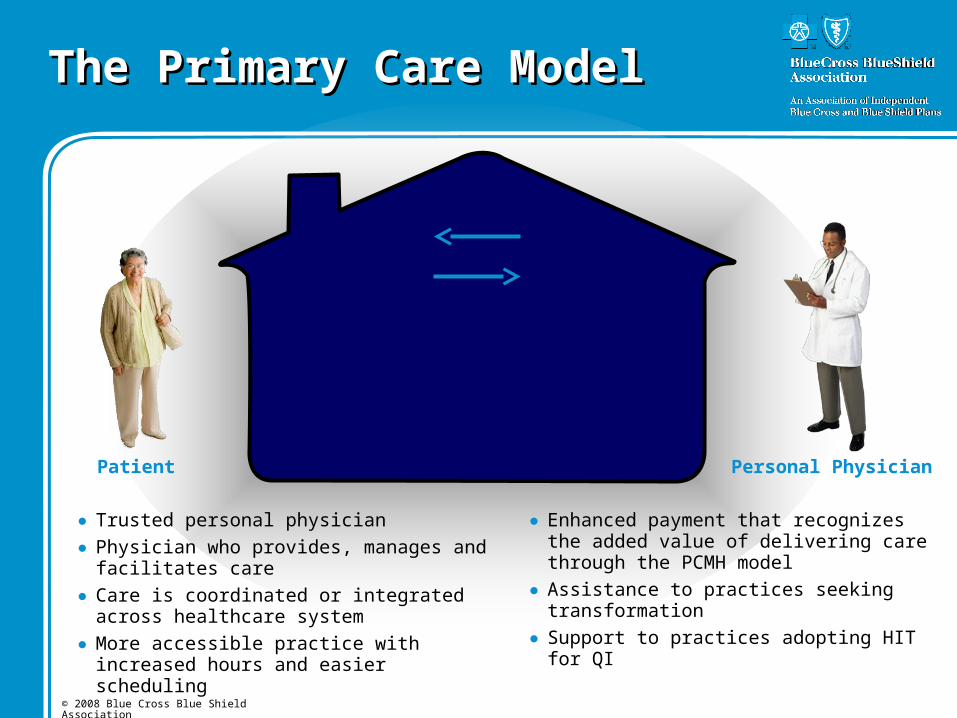
The Primary Care ModelThe Primary Care Model
● Trusted personal physician● Physician who provides, manages and facilitates
care● Care is coordinated or integrated across
healthcare system● More accessible practice with increased hours
and easier scheduling
● Enhanced payment that recognizes the added value of delivering care through the PCMH model
● Assistance to practices seeking transformation ● Support to practices adopting HIT for QI
Patient Personal Physician
12© 2008 Blue Cross Blue Shield Association
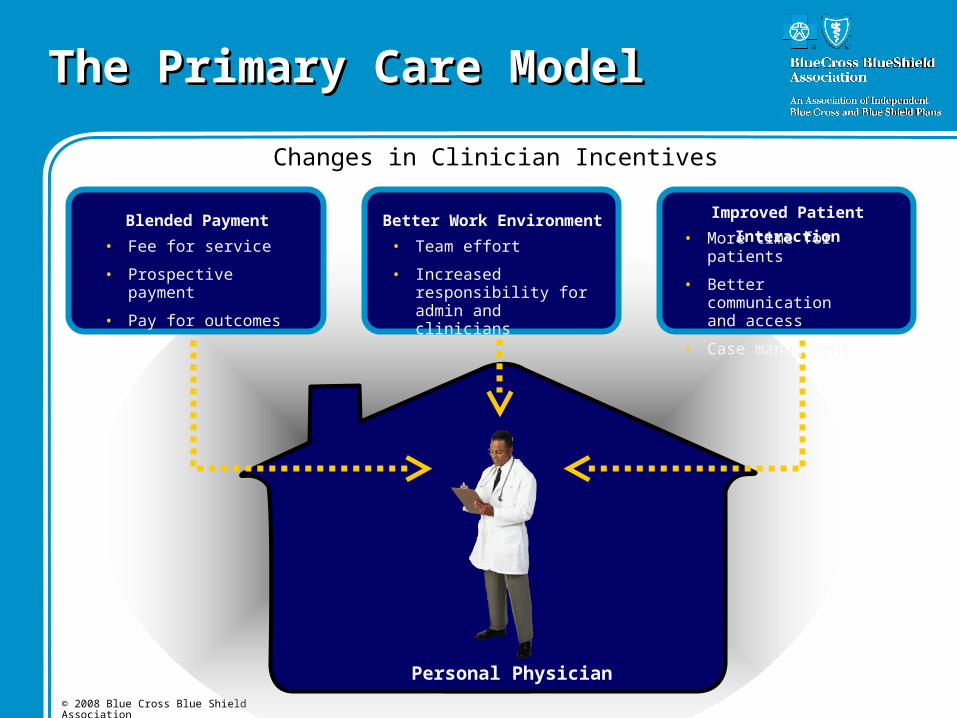
The Primary Care ModelThe Primary Care Model
Changes in Clinician Incentives
Fee For Service• Fee for service
• Prospective payment
• Pay for outcomes
Blended Payment Improved Patient InteractionBetter Work Environment
• Team effort
• Increased responsibility for admin and clinicians
• More time for patients
• Better communication and access
• Case management
Personal Physician
13© 2008 Blue Cross Blue Shield Association
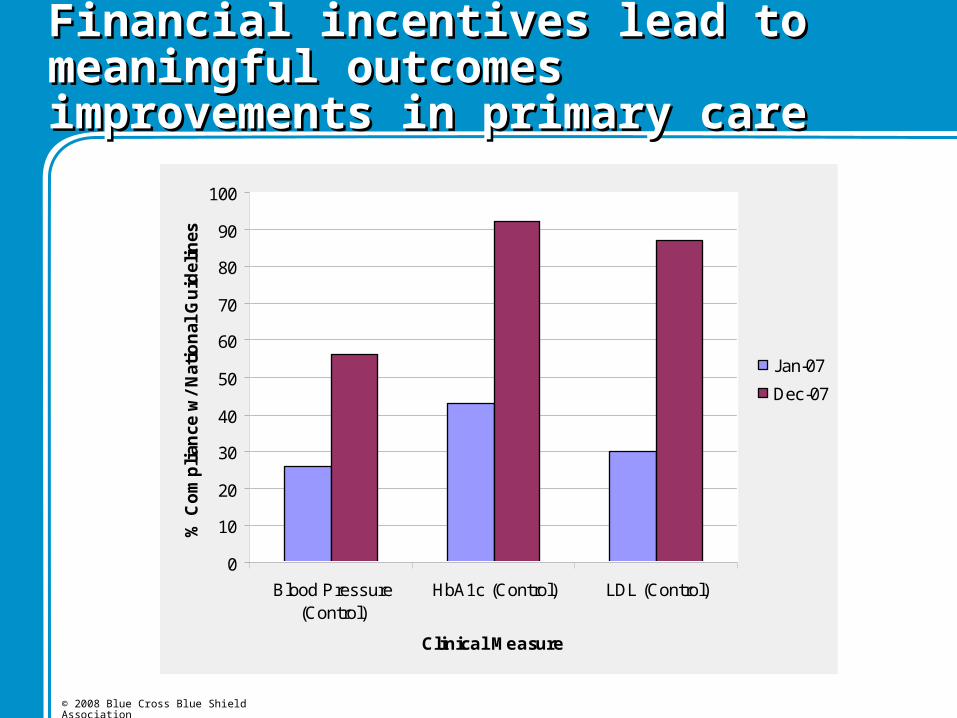
Financial incentives lead to meaningful Financial incentives lead to meaningful outcomes improvements in primary careoutcomes improvements in primary care
0
10
20
30
40
50
60
70
80
90
100
Blood Pressure(Control)
HbA1c (Control) LDL (Control)
Clinical Measure
% C
om
pli
ance
w/
Nat
ion
al G
uid
elin
es
Jan-07
Dec-07
14© 2008 Blue Cross Blue Shield Association
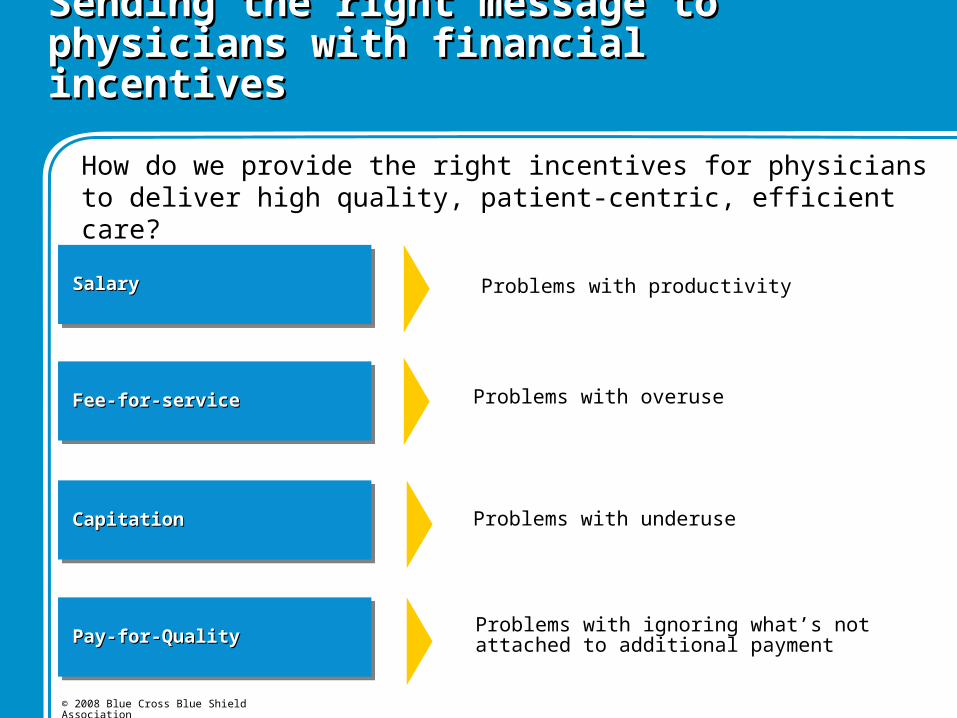
Sending the right message to physicians with Sending the right message to physicians with financial incentivesfinancial incentives
How do we provide the right incentives for physicians to deliver high quality, patient-centric, efficient care?
Problems with productivitySalarySalarySalarySalary
Problems with overuseFee-for-serviceFee-for-serviceFee-for-serviceFee-for-service
Problems with underuseCapitationCapitationCapitationCapitation
Problems with ignoring what’s not attached to additional paymentPay-for-QualityPay-for-QualityPay-for-QualityPay-for-Quality
15© 2008 Blue Cross Blue Shield Association
Blue Distinction raises the level of care delivered across the country by focusing on evidence-based quality and outcomes that are reinforced through national incentives
Physician Controlled, Evidence Based
Blue Distinction VisionBlue Distinction Vision
16© 2008 Blue Cross Blue Shield Association
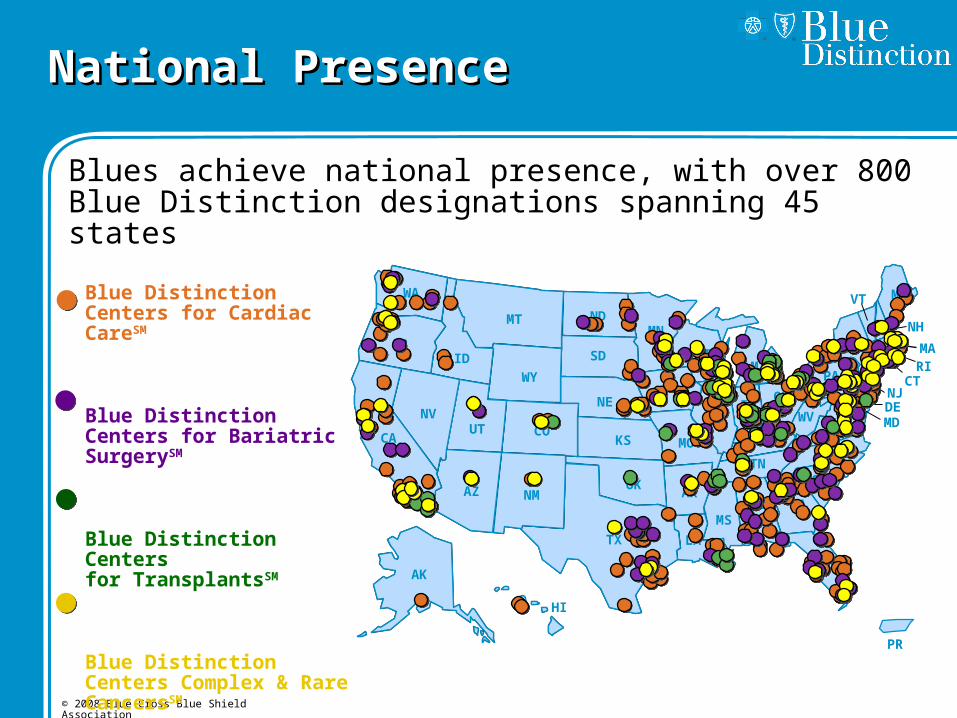
National PresenceNational Presence
Blues achieve national presence, with over 800 Blue Distinction designations spanning 45 states
WA
OR
CA
AK
HI
TX
NMAZ
UTNV
ID
MT ND
SD
NE
WY
COKS
OKAR
LA
MSAL GA
FL
SC
NCTN
KYMO
IL
IA
MN
WIMI
INOH
WV VA
PA
NY
MEVT
NH
RIMA
CTNJDEMD
PR
Blue Distinction Centers for Cardiac CareSM
Blue Distinction Centers for Bariatric SurgerySM
Blue Distinction Centersfor TransplantsSM
Blue Distinction Centers Complex & Rare CancersSM
17© 2008 Blue Cross Blue Shield Association
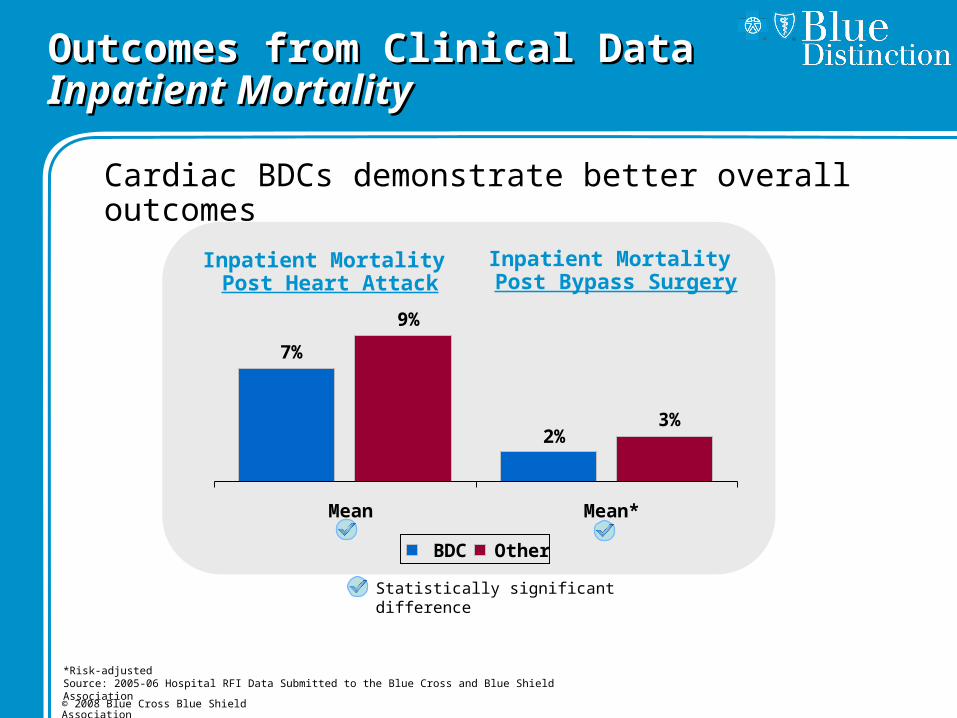
Outcomes from Clinical DataOutcomes from Clinical Data Inpatient MortalityInpatient Mortality
Cardiac BDCs demonstrate better overall outcomes
Inpatient Mortality Post Heart Attack
Statistically significant difference
Inpatient Mortality Post Bypass Surgery
*Risk-adjustedSource: 2005-06 Hospital RFI Data Submitted to the Blue Cross and Blue Shield Association
7%
9%
3%2%
Mean Mean*
BDC Other

18© 2008 Blue Cross Blue Shield Association
Outcomes from Clinical DataOutcomes from Clinical Data
Blue Distinction Centers demonstrates better, more consistent overall outcomes
Source: Hospital RFI Data Submitted to the Blue Cross and Blue Shield Association
Inpatient MortalityPost Heart Attack
Mortality Rate One-year Post Heart Transplant
BDC Other
11%
19%
Mean
7% 9%
Mean
19© 2008 Blue Cross Blue Shield Association
Happier DoctorsHappier Doctors
● Reward from medical practice: pride and peer approval
● Reward from payers: higher income based on better patient outcomes
● Reward from the nation: admiration and gratitude
● Reward from international colleagues: acceptance and integration of joint programs and initiatives
20© 2008 Blue Cross Blue Shield Association
Healthier PatientsHealthier Patients
● Better clinical outcomes
● Consistent management of chronic illness
● Trust that there is a caring relationship with a healer
● Belief that someone with special knowledge cares for him or her
● Safety from ineffective or unnecessary care
● Security for families and individuals

21© 2008 Blue Cross Blue Shield Association
Harmonious SocietyHarmonious Society
● Doctors and professional societies have aligned incentives
● Doctors, hospitals, and patients have aligned incentives
● Ministries and all healthcare stakeholders have aligned incentives
● Chinese patients deserve optimal health and productivity.
THE INCENTIVE: Doing the right thing right, the first time, based on the best available clinical evidence. This creates the opportunity for medical and financial security.

22© 2008 Blue Cross Blue Shield Association
Contact InformationContact Information
Allan M. Korn, M.D., FACP
Senior Vice President Clinical Affairs
and Chief Medical Officer
Blue Cross Blue Shield Association
225 North Michigan Avenue
Chicago, Illinois 60601
312.297.6840







