
Traumatic Brain Injury
Fall 2009
Fall 2009
Traumatic Brain Injury
• TBI results from a jolt to the head or a penetrating injury
• Complications may include change in cognition and behavior, and physical functioning
• TBI may occur as the result of a traffic accident; fall; assault; and, other causes (Centers for Disease Control and Prevention [CDC], 2008)
Traumatic Brain Injury
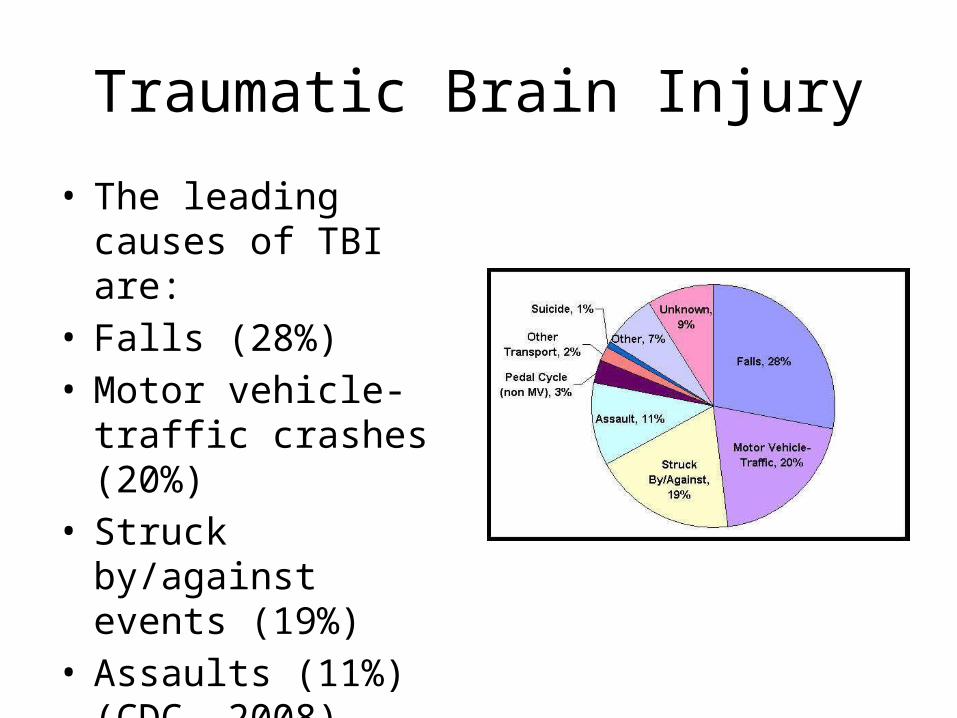
• The leading causes of TBI are:
• Falls (28%) • Motor vehicle-traffic
crashes (20%) • Struck by/against
events (19%) • Assaults (11%) (CDC,
2008)
Traumatic Brain Injury
• Nearly 7 million traumatic brain injuries occur in the U.S./year
• 100,000 result in permanent disability• Half a million people are hospitalized with
TBI/year in the U.S. (Ignatavicius & Workman, 2010)
• Over a million people with TBI are treated and released (CDC, 2008)
Traumatic Brain Injury
• Who is at risk?– Males are 3 times more likely to sustain a TBI than
are females– Highest risk are children 0 – 4 years of age and
those who are 15 – 19 years of age Why?– What about the elderly?– Highest death rate associated with TBI are African
Americans (CDC, 2008) Why?
Traumatic Brain Injury
• TBI increases the risk for development of Parkinson’s Disease and Alzheimer’s Disease
• Effects of TBI can be long-term or life-long• CDC (2008) reports that one year after TBI
nearly half of individuals continue to require assistance with ADLs
• Cost of care for individuals with TBI exceeds that of stroke patients
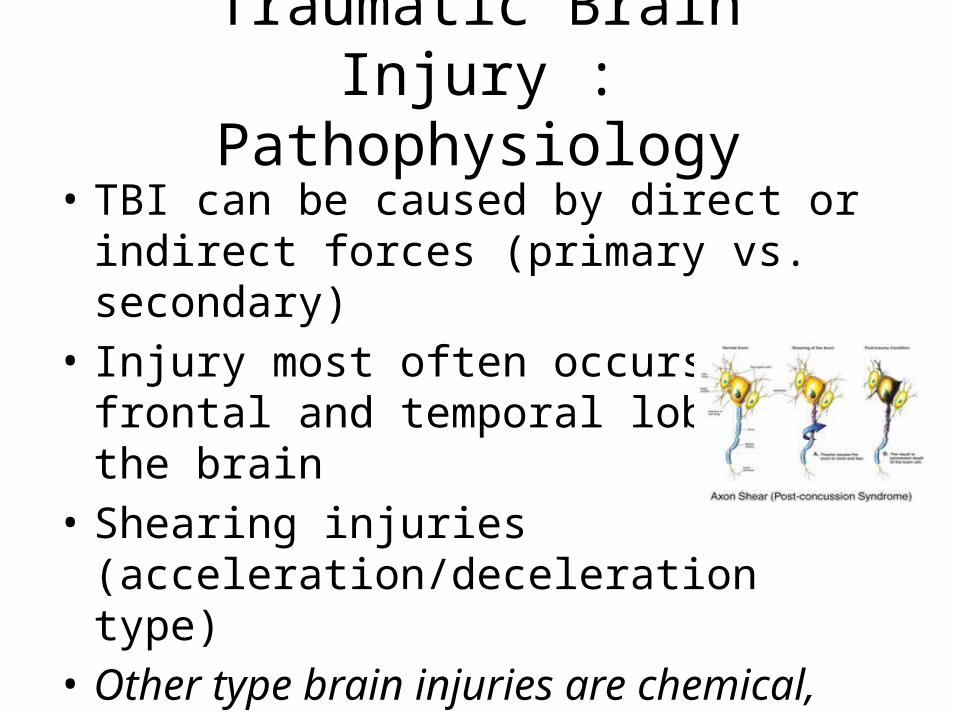
Traumatic Brain Injury : Pathophysiology
• TBI can be caused by direct or indirect forces (primary vs. secondary)
• Injury most often occurs in the frontal and temporal lobes of the brain
• Shearing injuries (acceleration/deceleration type)
• Other type brain injuries are chemical, hypoxic, or r/t stroke, tumors, or infection
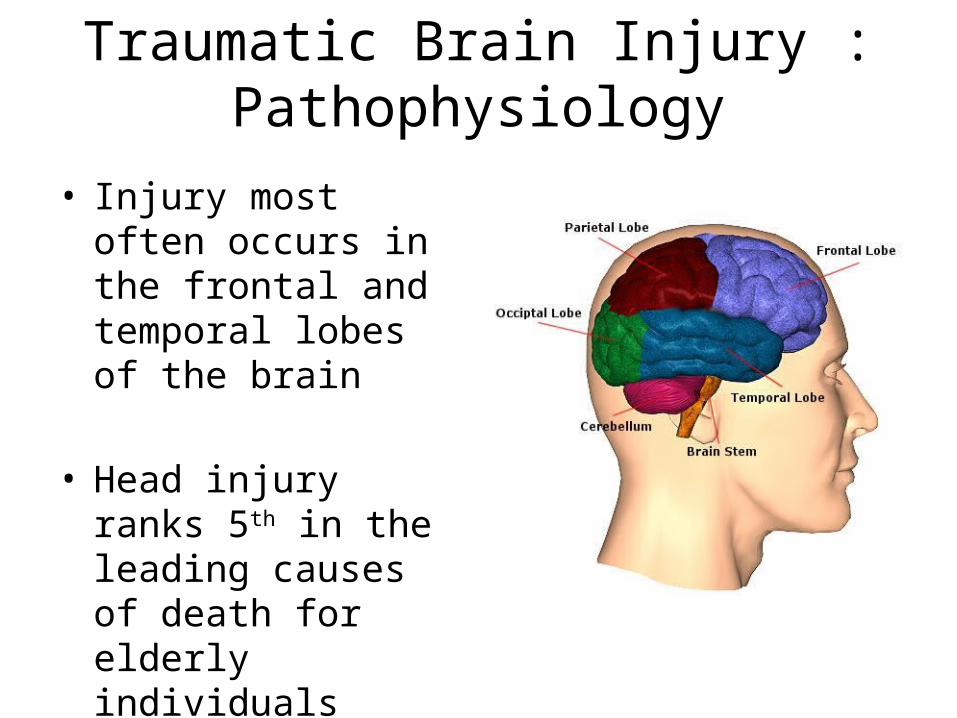
Traumatic Brain Injury : Pathophysiology
• Injury most often occurs in the frontal and temporal lobes of the brain
• Head injury ranks 5th in the leading causes of death for elderly individuals
Traumatic Brain Injury : Pathophysiology
• What occurs during TBI …– The brain is housed in the cranial vault and base– Trivia : There are 8 cranial bones, 14 facial bones
and 20 primary teeth, or 32 permanent teeth– Trivia: The brain consists of the cerebrum,
cerebellum and brainstem (medulla, pons, and midbrain)
Traumatic Brain Injury : Pathophysiology
• What occurs during TBI (continued) …– Trivia: Gray matter primarily consists of neuron
cell bodies (nerve cells)– Trivia: White matter primarily consists of axons
which connect to other parts of the brain and to the spinal cord
– Brain is limited in its capacity for protection– Bathed in cerebrospinal fluid within the skull – May be injured by the skull itself
Traumatic Brain Injury : Pathophysiology
• Brain tissue is gelatin-like, very fragile and susceptible to injury
• Brain responds to force induced trauma by moving within the skull (space is limited)
• Brain may also rebound or rotate on the brain stem resulting in a shearing-type injury
• Give an example of a shear-type brain injury
Traumatic Brain Injury : Pathophysiology
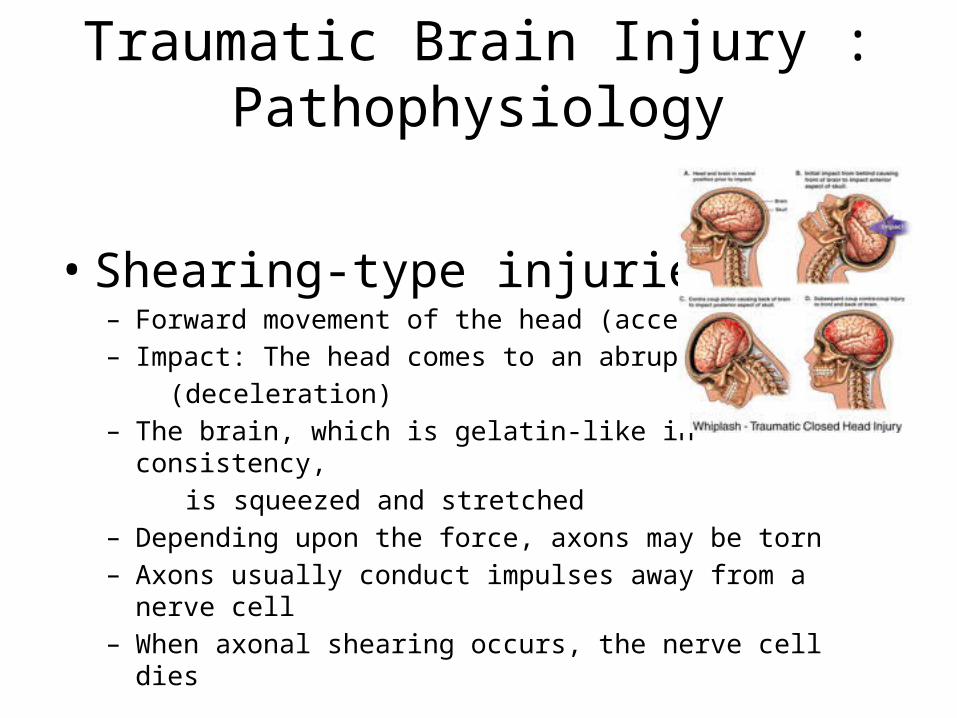
• Shearing-type injuries:– Forward movement of the head (acceleration) – Impact: The head comes to an abrupt stop (deceleration) – The brain, which is gelatin-like in consistency, is squeezed and stretched– Depending upon the force, axons may be torn– Axons usually conduct impulses away from a nerve cell– When axonal shearing occurs, the nerve cell dies
Traumatic Brain Injury
• Other type:– Chemical injury can damage neurons and may result
from exposure to carbon monoxide, lead poisoning (or other heavy metals) , solvents, etc.
– Hypoxic or anoxic brain injury may occur secondary to heart attack; stroke; respiratory failure; may result in significant cognitive impairment
– Tumor– Infection such as meningitis and encephalitis
Primary Brain Injury
• Open-head injury– Penetrating-type injury– Secondary to skull fracture or penetration of an of
object – Damage to the brain, blood supply, or cranial
nerves may occur – Contamination – Blood-brain barrier
Closed Head Injury
• Most severe type of head injury (MRI is critical to make diagnosis as soon as possible)
• Skull remains intact• Occurs as a consequence of trauma• Can be mild (concussion) or severe (diffuse axonal tearing)• Mild concussion is associated with brief LOC (LOC is cue that
you must act immediately) • Post concussion (30 % of individuals) symptoms may include
irritability, headache, memory loss, depression, inability to sleep
• Severity of concussion characterized by the period of LOC
Response to TBI
• Most common response is an increase in intracranial pressure (ICP) caused by – – Bleeding and hematoma formation
• Subdural (slower to develop; r/t laceration of brain or tearing)
• Epidural (an emergency; “lucid interval”)• Intracerebral (space-occupying accumulation of blood
in brain tissue; r/t direct trauma, fx or torsion
– Swelling – Compromised cerebral autoregulation ( ICP)
TBI Assessment
• Individuals with TBI are treated as though they also have cervical SCI (present in 5% to 20%)
• Signs of SCI include– Loss of motor and sensory function– Tenderness along the spine– Abnormal head tilt
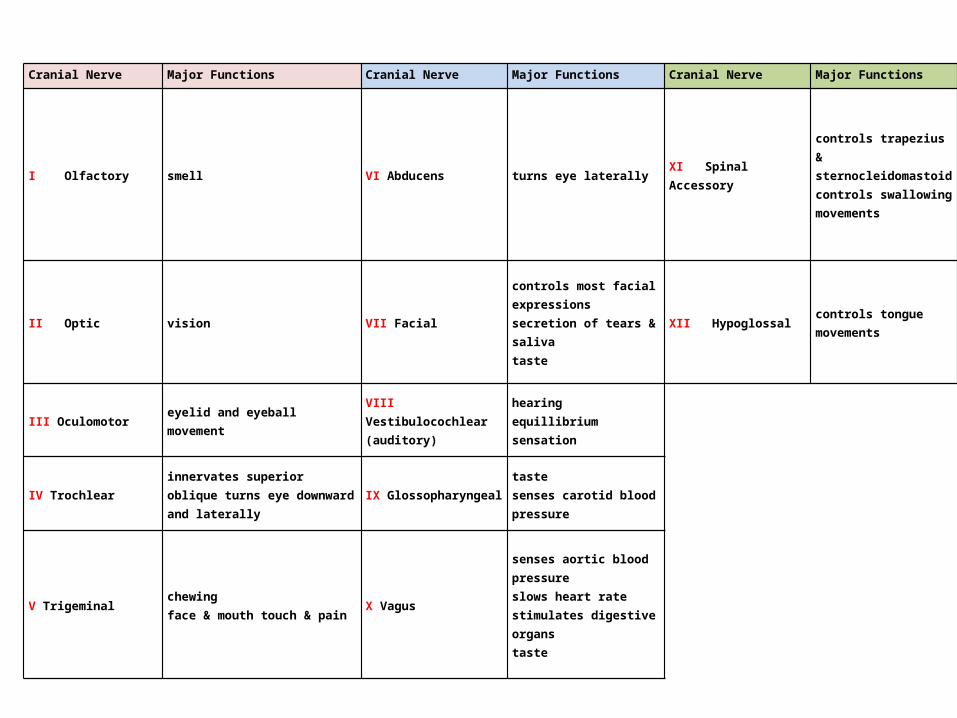
Cranial Nerve Major Functions Cranial Nerve Major Functions Cranial Nerve Major Functions
I Olfactory smell VI Abducens turns eye laterally XI Spinal Accessory
controls trapezius & sternocleidomastoidcontrols swallowing movements
II Optic vision VII Facial
controls most facial expressions secretion of tears & salivataste
XII Hypoglossal controls tongue movements
III Oculomotor eyelid and eyeball movement VIII Vestibulocochlear(auditory)
hearing equillibrium sensation
IV Trochlear innervates superior oblique turns eye downward and laterally
IX Glossopharyngeal taste senses carotid blood pressure
V Trigeminal chewing face & mouth touch & pain
X Vagus
senses aortic blood pressure slows heart rate stimulates digestive organstaste
Level of Consciousness
• Glasgow Coma Scale- Three types of responses are measured and their scores added together
• Best motor response - maximum score of 6 Best verbal response - maximum score of 5 Eye opening - maximum score of 4
– Used as a tool in assessing head injury– Focuses on the ability to open the eyes; respond to verbal
commands; movement of the extremities – Scores are combined to determine level of consciousness – Scores range from 3 – 15– Score of 3 – 8 characteristic of coma
Glasgow Coma Scale
• A score of 3 to 8 is characteristic of severe head trauma• A score of 9 to 12 is indicative of a moderate head trauma• A score of 13 to 15 is associated with a mild head injury • Motor Response (movement of extremities)• 6 Obeys commands to move arms and legs• 5 Withdraws from pain locally (where pinched) • 4 Withdraws from pain generally • 3 Flexes limb in response to pain • 2 Straightens limb in response to pain • 1 No movement in response to pain
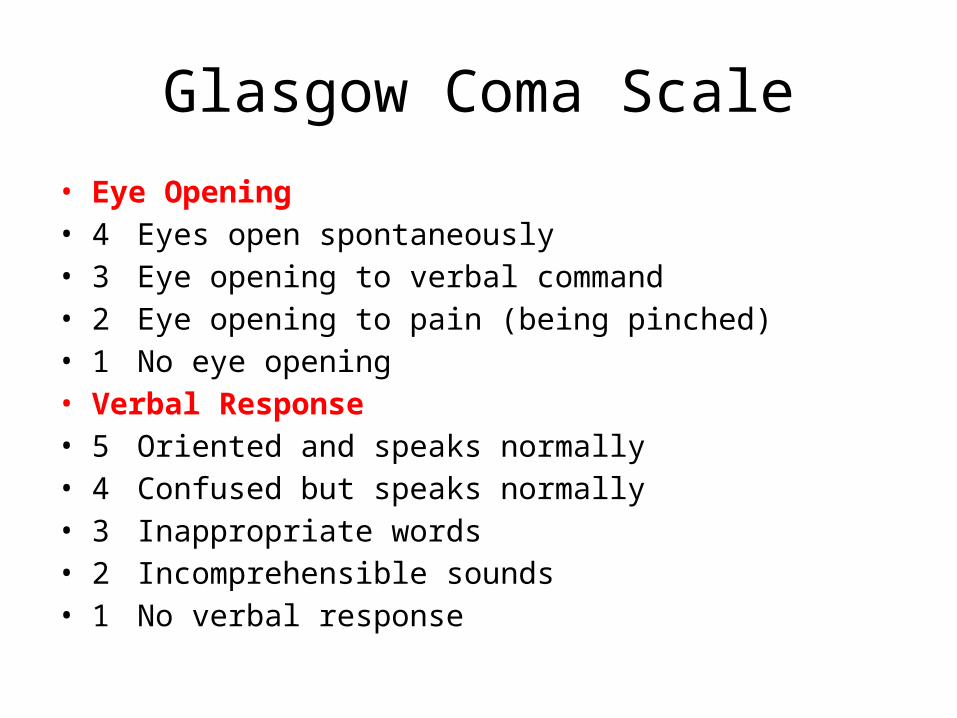
Glasgow Coma Scale
• Eye Opening• 4 Eyes open spontaneously • 3 Eye opening to verbal command • 2 Eye opening to pain (being pinched) • 1 No eye opening• Verbal Response• 5 Oriented and speaks normally• 4 Confused but speaks normally • 3 Inappropriate words • 2 Incomprehensible sounds • 1 No verbal response
TBI Assessment
• Individuals with severe brain injury may be confused, combative, or unconscious
• When did the injury occur?• Loss of consciousness? • Any change in consciousness? • Individual may be unconscious, return to a
normal state of consciousness and then decline quickly
TBI Assessment
• Nursing goals in assessing individuals with TBI are in obtaining baseline information and early detection of complications– Increased ICP (Normally, the ICP ranges from 1 to
15 mm Hg. Note: mm Hg = millimeters of mercury)– Hypoxia– Hypercapnia (increased blood levels of carbon
dioxide)– Subtle changes in neurologic status
TBI Assessment
• FIRST… airway! • Monitor chest wall movement with auscultation • Brain-stem injuries can cause changes in breathing,
such as Cheyne-Stokes respirations• Monitor BP and pulse for any changes in cerebral
blood flow which occurs secondary to impaired autoregulation r/t hypotension or hypertension
TBI Assessment
• Cushing reflex (late sign of ICP) characterized by severe HTN with widened pulse pressure and bradycardia. Increasing ICP is associated with a thready, irregular, and rapid pulse
• (Cushing’s Law) An acute increase of intracranial pressure also causes compression of the cerebral blood vessels and cerebral ischemia, producing an increase of systemic blood pressure over the vasomotor center, with simultaneous reduction in heart rate, respiratory slowing
• Cardiac dysrhythmias may occur secondary to increased ICP and brainstem pressure
TBI Assessment• Intracranial pressure, (ICP), is the pressure exerted by the cranium on the
brain tissue, cerebrospinal fluid (CSF), and the brain's circulating blood volume
• ICP is a dynamic phenomenon constantly fluctuating in response to activities such as exercise, coughing, straining, arterial pulsation, and respiratory cycle.
• ICP is measured in millimeters of mercury (mmHg) and, at rest, is normally 7–15 mmHg for a supine adult, and becomes negative (averaging −10 mmHg) in the vertical position
• Changes in ICP are attributed to volume changes in one or more of the constituents contained in the cranium.
• ICP is normally 0–10 mm Hg; at 20–25 mm Hg, the upper limit of normal, treatment to reduce ICP is needed
TBI Assessment
• Signs of increasing ICP include – Severe headache (response to the injury*)– Nausea– Vomiting– Seizures (response to the injury*)– Papilledema (optic disk swelling secondary to ICP)
Always a sign of ICP
TBI Assessment: Neurologic
• The most important assessment when using the Glasgow Coma Scale is the LOC
• Early changes in LOC may include restlessness or irritability
• Decreased LOC is the first sign of a worsening neurologic status
TBI Assessment: Neurologic
• In a conscious and cooperative individual, a full neurologic assessment is conducted
• CNs I, V, VII, IX and X • Damage to CN I results in a loss of ability to
smell (anosmia)• CNs V, VII, IX and X are involved in chewing
and swallowing and in phonation
TBI Assessment: Neurologic
• Watch ears and nose for CSF leakage (secondary to basilar skull fx)
• CSF on white absorbent background can be differentiated from other fluids due to its “halo” effect (i.e., yellowish stain and surrounding bloody drainage)
• Dipstix used to test for glucose, but not always diagnostic for the purpose of checking for CSF
TBI Assessment: Neurologic
• Nuchal rigidity (neck stiffness) may suggest infection or blood in the CSF
• Not checked until SCI is ruled out. Why?
TBI Assessment: Eyes
• Change in pupil size, shape or reactivity may suggest an increase in ICP
• Ovoid pupils (between a normal-sized pupil and dilated pupil) is indicative of increasing ICP
• Fixed, dilated pupils occur with significant increase in ICP and are associated with a poor prognosis
(Ovoid Pupil)
TBI Assessment: Motor
• Motor loss is generally contralateral to the location of the lesion/injury (i.e., left-sided hemiparesis is characteristic of right-sided cerebral hemisphere injury)
• Other motor signs of ICP include loss of motor function, abnormal posturing, or flaccidity.
Psychosocial Aspects of TBI
• An individual who suffers a severe or moderate brain injury is never recovered to the extent prior to the injury
• Personality changes including increased temper, risk-taking behaviors, depression and lack of acknowledging disability occur
• Recent and short-term memory may be affected
Psychosocial Aspects of TBI
• Individuals who sustained mild TBI may exhibit symptoms of disability for one year post injury
• Changes occur within the family. What changes would be anticipated?
• Think about your patient in rehab. What changes are occurring, or have occurred r/t injury or disability?
TBI and Nursing Interventions
• Preventing or detecting any increase in ICP• Fluid and electrolyte balance (significant
electrolyte imbalances can be r/t secondary injury as well as increase the risk of seizures
• Assess for fever (hypothalamic damage can cause fever)
TBI and Nursing Interventions
• Avoid extreme flexion or extension of the neck• Head should be maintained in a midline,
neutral position• Head of bed elevated at 30 degrees* Why? Hint… helps to decrease ICP
TBI and Drug Therapy• Mannitol (Osmitrol), an osmotic diuretic, is used to treat cerebral edema by
drawing water from the extracellular space (osmotic diuretics increase excretion of water and electrolytes, i.e., urinary excretion)
• Furosemide (Lasix), a loop diuretic, reduces edema and blood volume, decreases the production of CSF (loop diuretics increase salt excretion)
• Dilantin (phenytoin) – can cause visual changes (diplopia & photophobia) which could be confused w/ brain injury sypmtoms. Can also cause slurred speech as well.
• Opiod: to calm them, decrease BP, decreases anxiety & agitation…, may be used even if they are having pain. Also is a vasodialator
• May even give them a paralyzing agent to put them in a coma… (vancreonium, sp???)
• These pts can also develop hydrocephalus… may need a shunt….• Also maybe a brain herniation… cerebral portion of brain can shift down into the
midbrain (life threatening) or could shift into either of the the temporal lobes) dramatic CN effects, unreactive pupils… Usually not treatable.
Brain Tumors
Spring 2009
Brain Tumors
• Primary tumors occur within the CNS• Secondary tumors are generally metastatic lesions
(lungs, breast, kidney, GI tract)• Consequences of brain tumors include
– Edema and inflammation of the brain– Increased ICP– Obstruction in the flow of CSF– Pituitary dysfunction– Neurologic deficits
Brain Tumors: Malignant Types
• Gliomas – Defined as any tumor of non-nervous cells in the nervous
system (low grade or high grade)– 60% of all brain tumors in adults – Peak in adults 40 to 60 years of age
Metastatic tumors- 30% of brain tumors- Metastatic lesion from lungs, breast, colon, pancreas and
kidney- Cells travel via the lymphatic and blood systems
Brain Tumors: Benign Type
• Pituitary adenoma– 10% to 25% of brain tumors– Presenting symptoms may be visual disturbances– Produce loss of hair; headaches; diabetes; sterility; visual
deficiencies Acoustic Neuroma- Arise from cranial nerve VIII (the acoustic nerve)- Compress brain tissue making removal difficult- Affect females more than males- Symptoms include hearing loss; tinnitus (ringing in the
ears) and dizziness or vertigo
Brain Tumors: Symptoms
• Headaches (more severe in the morning)• Nausea and vomiting• Visual symptoms• Seizures*• Changes in personality• Papilledema (swelling of the optic disk)
Brain Tumors: Management• Non-surgical
– May include radiation and chemotherapy• Radiation therapy
– Post-op; Treatment injected via catheter directly into the surgical cavity (seeds or pellets) – to slow tumor growth
• Chemotherapy– Used alone or in combination with radiation therapy and/or surgery
• Gamma knife– Uses high-dose, targeted radiation to destroy intracranial lesions
while leaving surrounding tissue intact• Surgical
– Craniotomy most common type
Brain Tumor: Nursing Care
• Postoperative care is directed toward identifying changes; ICP in particular
• Possible complications include – Decreased level of consciousness– Motor weakness or paralysis – Visual changes– Changes in personality– Perioribital edema
Assessment and Evaluation
• Full consciousness• Confused• Lethargy• Stupor• Light Coma• Deep Coma
Coma
Spring 2009
Coma
• A profound state of unconsciousness • Result of bilateral, diffuse, cerebral
hemispheric dysfunction or involvement of the brainstem, or both
• Not a disease, but a condition of an underlying process– CNS problems – Metabolic problems
Coma: Metabolic /Systemic Conditions
• Hypoxia• Diseases of other organs
– Liver– Kidney– Lungs – Pancreas Pharmacologic agents (insulin)
Metabolic vs CNS Comas
Metabolic• Diffuse abnormal motor
signs• Coma precedes motor
abnormalities• Pupils bilaterally reactive• Partial dysfunction of many
areas of CNS
CNS• Focal abnormalities,
unilateral• Coma follows motor
abnormalities• Pupils non-reactive• Orderly progression of CNS
dysfunction
States of Altered Consciousness
• Persistent vegetative state (PVS)– Coma has progressed to a stage of wakefulness
without awareness– Retain non-cognitive function and sleep pattern
• Locked-in syndrome– Awake and aware, but cannot communicate or move
(usually related to brain mass or hemmorrhage that is severe… follow w/ eyes & may follow some commands, can follow some commands… some of these things are reflexes)
• Brain death – Legal death
Rancho Los Amigos Scale
• Measures cognitive function– Levels I – XIII– Lower number = lower cognitive function– Used to assess the level of recovery from brain
injury in individuals recovering from coma– Children scale is opposite
• Lower number = higher cognitive function
Rancho Los Amigos Scale
• Level I No response• Level II Generalized response• Level III Localized response• Level IV Confused, agitated • Level V Confused, inappropriate,
non-agitated response• Level VI Confused, appropriate• Level VII Automatic, appropriate• Level VIII Purposeful, appropriate
Children’s Ranch Scale
• Lower number = higher cognitive function• I Oriented to self and surroundings• II Responsive to environment• III Localized response to sensory
stimulation• IV Generalized response to sensory
stimulation• V No response to sensory
stimulation
Stroke
Spring 2009
Stroke (Brain Attack)
• Stroke (CVA no longer acceptable term) consists of an interruption in cerebral blood flow; linked to ischemia, hemorrhage, or embolism (Parsons, 2006, cited in Wissman (Ed.), 2006)
• Syndrome of rapid onset characterized by neurologic deficits lasting 24 hours or more, that fit a known cerebrovascular territory and result in impaired brain circulation
Stroke Risk Factors
• Hypertension ×Diabetes mellitus • Obesity ×Atrial fibrillation • Oral contraceptive use• Physical inactivity ×Arteriovenous • Sickle cell disease malformation• Smoking ×Atherosclerosis • Hyperlipidemia• (the 3 in bold are the “trifecta”… most likely to dispose you to
stroke)
Types of Stroke
• Obstructive or hemmoragic (not ischemic) – 80%– Blood clot in artery in the brain
• Hemorrhagic – 20% – Rupture of vessel in the brain with subsequent
bleeding into the brain
Types of Stroke
• Ischemic strokes (80%)– Classifications
• Cerebral thrombus• Cerebral embolism• Lacunar infarct • Transient ischemic attack (TIA) What about this?• Reversible ischemic neurologic deficit• Systemic hypoperfusion (ischemic-anoxic
encephalopathy)
Cerebral Thrombus
• Description – Vessels become occluded, resulting in ischemia
and infarction– Often preceded by TIAs– Patient awakes with symptoms or is sedentary
when it happens What symptoms?– Cerebral edema occurs in 2-5 days
Cerebral Embolus
• Description– Seen in younger individuals, awake and active– Most common cause is microembolus from atrial
fibrillation– What is “atrial fibrillation” and why does
microembolus result? – Develops quickly, middle cerebral artery most
often affected
Hemorrhagic Stroke
• Intracerebral– Spontaneous hemorrhage r/t HTN, usually occurs in an
older individual, active, no previous symptoms– Decreasing LOC, hemiplegia (paralysis of one-half of
patient’s body)– Aneurysm or arteriovenous malformation (AVM)
• Subarachnoid– Result of a ruptured aneurysm or AVM; immediate decreasing LOC– Anterior cerebral artery
• Neurologic impairment is sudden and severe
Warning Signs of Stroke
• Sudden numbness or weakness of the face, arm, or leg (especially on one side)
• Sudden confusion, trouble speaking or understanding speech
• Sudden trouble seeing in one eye or both eyes• Sudden severe headache
Stroke Signs and SymptomsIs Based on the Area of the Brain Affected
• Left cerebral hemisphere responsible for language, mathematic skills, and analytic thinking– Aphasia (language use or comprehension difficulty)– Alexia (reading difficulty)– Agraphic (writing difficulty)– Right hemiplegia or hemiparesis (paralysis of one side of the
body) – Slow, cautious behavior– Depression and quick frustration– Visual changes, such as hemianopsia (absence of half of the
normal field of vision) (Parsons, 2006, cited in Wissman (Ed.), 2006)
Stroke Signs and SymptomsIs Based on the Area of the Brain Affected
• Right cerebral hemisphere is responsible for visual and spatial awareness and proprioception (coordinated muscular activity)– Unawareness of deficits (neglect syndrome, overestimation of
abilities)– Loss of depth perception– Disorientation– Impulse-control difficulty– Poor judgment – Left hemiplegia or hemiparesis (paralysis of one side of the body)– Visual changes, such as hemianopsia (absence of half the normal field
of vision) (Parsons, 2006, cited in Wissman (Ed.), 2006)
Immediate Care of ANY Stroke
• 9-1-1 and immediate transport to stroke center
• Inform family members• Notify primary care physician
Strokes and the Elderly
• Arteriosclerosis in older adults greatly increases the incidence of stroke
• Resulting neurologic deficits increase the risk for falls
• Neurologic deficits r/t impaired swallowing place these individuals at an increased risk for malnutrition
• Behavioral changes are common – depression
Ischemic Stroke
• Immediate care– MRI to rule out hemorrhage– Activase® - Tissue Plasminogen Activator, better
known as TPA if within 3 hours of onset of symptoms
– Surgical intervention – Anticoagulation – Hemodynamic stabilization – Monitor for increasing cerebral edema
Ischemic Stroke: Anticoagulants/Antiplatelets/Antiepileptics
• Anticoagulants – Sodium heparin, warfarin (Coumadin)– Appropriate therapy for all strokes?
• Antiplatelets– Ticlopidine (Ticlid), clopidogrel (Plavix)
• Antiepileptics – Phenytoin (Dilantin), gabapentin (Neurontin)
Hemorrhagic Stroke
• Immediate care– Control of increasing intracranial pressure– Control of hypertension– Surgical intervention
• Coiling (catheter inserted through the arm or the groin - placement causes blood in the aneurysm to clot)
• Hematoma evacuation (beneficial for lowering intra-cranial pressure; re-establishing blood flow)
Following Immediate Care
• Assessment and ongoing monitoring for even subtle changes
• Prevention of secondary brain injury• Prevention, early recognition and nursing
management of multi-system problems• Early rehabilitation
Risk for Aspiration / Impaired Swallowing
• Monitor for dysphagia or aspiration • Videofluroscopic swallow study (VSS)• Chair or straight up in bed for meals/meds• Head and neck flexed and slightly forward• Soft vs. thin liquids or table food• Pocketing
Impaired Physical Mobility
• Positioning and ROM with joint support• Use general principles of normalizing muscle
tone, integration vs. compensation, meaningful activities vs. simulated activities, cross-over neurodevelopmental techniques
• Shoes to prevent foot drop (r/t muscle weakness)
Risk for Falls
• More than one-third of falls in stroke patients occur while rising or sitting down
• Left-hemisphere stroke (right-sided deficits, aphasias in 15%) tend to recover more quickly; nurses tend to under-estimate their abilities
• Right-sided strokes (left-sided deficits, chatty and impulsive) at risk for falls/high risk behaviors; nurses over-estimate their abilities
Nursing Management
• Ineffective airway clearance• Swallowing deficit• Fluid volume deficit• Inadequate nutrition• Impaired skin integrity (actual, potential)• Altered bladder elimination• Altered bowel elimination• Sleep/rest disturbance• Impaired vision• Altered ADLs
Rehab in Acute Care
• Physiological functions stabilized, usually 24 – 36 hours after admission
• Prevention of complications that interfere with rehab• Primarily involves positioning and ROM• Focus no longer only on unaffected side, but on affected side
to facilitate bilateral function • Over-learn functional movements and automatic posture
reactions (procedural memory) to regain normal muscle tone, posture, movement and function
Rehab – Brain Plasticity
• The brain can be retrained to transfer function to different areas, accomplished through specific positioning and patterned exercise of normal automatic postural reactions, stimulating basic motions
• Once basic motions are restored (bed posture), they can be used to support the next level of functioning/improvement
Brain Plasticity
• When cells die, remaining cells function more efficiently
• When neural connections are impaired, degeneration of inhibitors that had previously masked unused connections present in embryonic stage, which provides avenues for impulses
• Previously unconnected axons develop attachments to dendrites of still functioning cells, providing new input or collateral sprouting
Inflammatory Conditions of the Brain
Spring 2009
Meningitis
• Meningitis is an inflammation of the protective membrane covering the brain and spinal cord – the meninges
• Bacterial meningitis• Viral meningitis
Meningitis Signs and Symptoms
• Headache, excruciating and unrelenting • Fever and chills• Photophobia • Nausea and vomiting• Altered level of consciousness • Nuchal rigidity (neck stiffness that prevents flexion) • Positive Kernig’s sign (resistance to extension of the patient’s leg from a
flexed position)• Positive Brudzinski’s sign (flexion of extremities occurring with deliberate
flexion of the patient’s neck)• Tachycardia • Seizures• Red macular rash (meningococcal meningitis)
MeningitisSigns and Symptoms
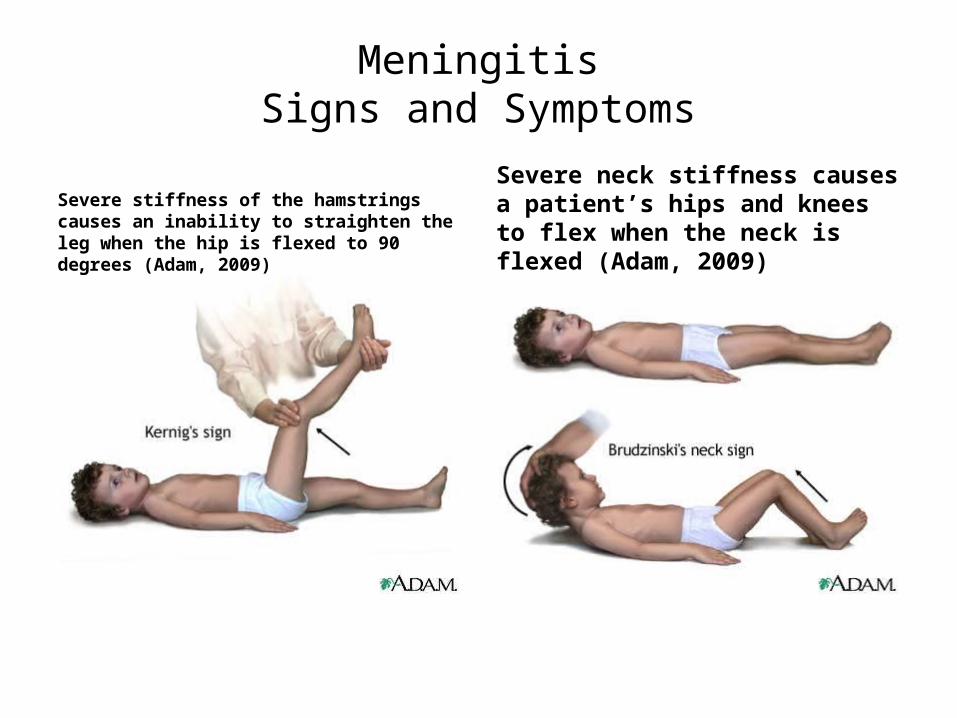
Severe stiffness of the hamstrings causes an inability to straighten the leg when the hip is flexed to 90 degrees (Adam, 2009)
Severe neck stiffness causes a patient’s hips and knees to flex when the neck is flexed (Adam, 2009)
Bacterial Meningitis Pathophysiology
• A medical emergency with a high mortality rate if untreated
• (Viral meningitis occurs most often and usually resolves without treatment)
• Responsible organisms enter CNS through the bloodstream at the blood-brain barrier
• Organisms distribute throughout the CNS through the subarachnoid space resulting in the inflammatory response
Bacterial Meningitis Risk Factors
• Risk Factors– Bacterial infections such as upper respiratory
infections, i.e., otitis media, pneumonia, sinusitis) – Immunosuppression– Invasive procedures, skull fracture, or penetrating
head injury (direct access to cerebrospinal fluid)– Overcrowded living conditions
Viral MeningitisRisk Factors
• Most common type• Risk factors:
– May occur secondary to viral illnesses, including measles, mumps, herpes simplex and herpes zoster
• Frequently resolves without treatment• Exudate does not occur
Clinical Presentation of Meningitis , other
• Decreased (or change in) LOC• Disoriented to person, place and year• Pupil reaction and eye movements
– Photophobia– Nystagmus– Abnormal eye movements
• Motor response– Normal early in disease process – Hemiparesis, hemiplegia, and decreased muscle tone
possible later– Cranial nerve dysfunction, esp. CN III, IV, VI, VII, VIII
Clinical Presentation of Meningitis , other
• Memory changes• Severe, unrelenting headaches• Generalized muscle aches and pain• Nausea and vomiting• Fever and Chills• Tachycardia• Red macular rash (meningococcal meningitis)
(Chart 45-8 of Ignatavicius and Workman, 2006)
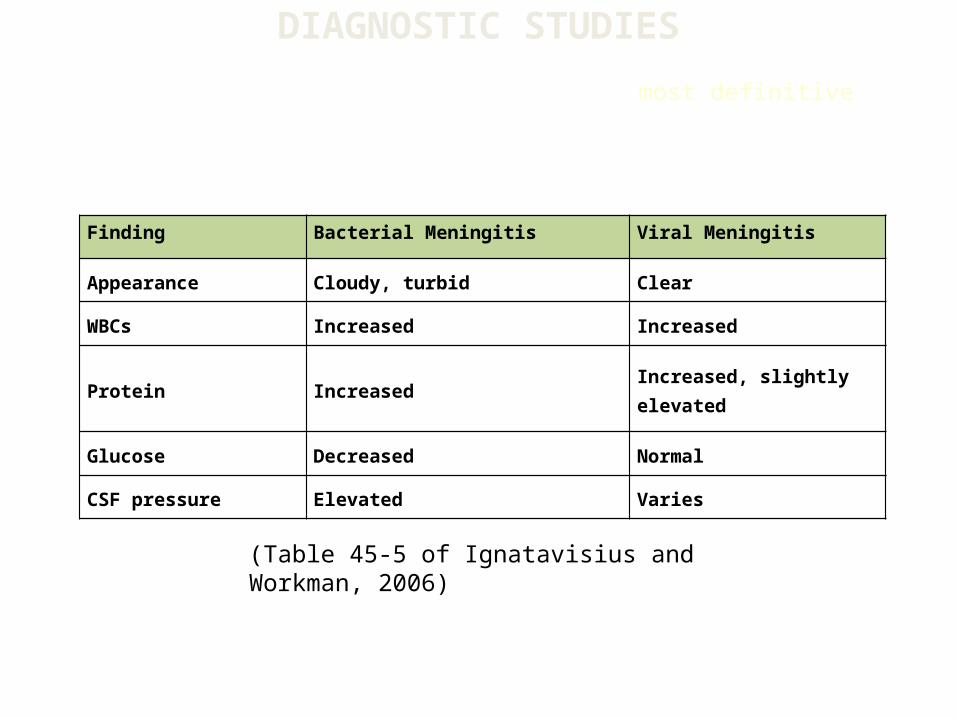
Finding Bacterial Meningitis Viral Meningitis
Appearance Cloudy, turbid Clear
WBCs Increased Increased
Protein Increased Increased, slightly elevated
Glucose Decreased Normal
CSF pressure Elevated Varies
(Table 45-5 of Ignatavisius and Workman, 2006)
DIAGNOSTIC STUDIES
Cerebrospinal fluid analysis is the most definitive diagnostic procedure
Collaborative Care
• Monitor airway, breathing, circulation • Neuro checks and vital signs 2-4 hours• Watch for motor changes• Assess CNs, esp III, IV, VI, VII and VIII• Meds as ordered• I &Os• Decrease environmental stimuli• Isolation precautions
Collaborative Care, continued
• Monitor for and prevent complications– Increased ICP– Vascular dysfunction– Seizures– Shock– Fluid and electrolyte imbalance







