

Ultrasound in Abdominal
EmergenciesDr/Ahmed Bahnassy
Consultant RadiologistRiyadh Military Hospital

The acute abdomen
The acute abdomen is a medical term used to describe a patient who presents with sudden onset of severe abdominal pain sometimes accompanied by nausea, vomiting, diarrhea, abdominal distension, and even hypotension or shock.

Ultrasound is a well-established imaging modality for evaluating the abdomen, as it is noninvasive, portable, readily obtainable, relatively inexpensive, and without the risks of ionizing radiation or iodinated intravenous contrast. In addition, ultrasound has extremely high diagnostic accuracy in many clinical scenarios equivalent or even superior to CT .


The biliary tract
The most common cause of acute right upper quadrant (RUQ) pain in adults is acute cholecystitis. Ultrasound largely has replaced scintigraphy (HIDA scan) as the initial imaging modality of choice for evaluating patients with clinical suspicion of acute cholecystitis,
Furthermore, ultrasound has the additional advantages of being able to demonstrate potential complications of acute cholecystitis, such as perforation and gangrene, and the potential to identify nonbiliary causes of RUQ pain.

The two most important diagnostic criteria for the diagnosis of acute cholecystitis on ultrasound examination are the presence of gallstones and a positive sonographic Murphy's sign. In combination, these two findings have been shown by Ralls and colleagues to have a positive predictive value of 92% .
Acute Cholecystitis

gall stones Dx
sitting position
decubitus
duodenal gas

Tissue Harmonic imaging THI

Complicated cholecystitis
perforated cholecystitis

Gangrenous cholecystitis
sloughed membranes

HIV cholangiopathy.
hepatitis
Thickening of the gallbladder wall and the presence of peri-cholecystic fluid are secondary findings of acute cholecystitis
on ultrasound examination, but are neither sensitive nor specific

Perforated DU +abnormal GB

As acute cholecystitis is an obstructive process, the gallbladder also typically is distended.
Hence, a careful search should be made for an obstructing stone in either the cystic duct or the neck of the gallbladder

Acalculous Cholecystitis
Emphysematous cholecystitis

Emphysematous cholecystitis

XanthogranulomatousCholecystitis

Choledocholithiasis
Biliary colic should be suspected in patients with acute RUQ pain who are found to have small-to-tiny gallstones in a nondistended gallbladder but no sonographic Murphy's sign, gallbladder wall thickening, or peri-cholecystic fluid

The sensitivity of ultrasound in detecting choledocholithiasis has been reported to range from 70% to 89% in experienced hands .
Images should be obtained in supine, semierect, left posterior oblique (LPO) and right posterior oblique (RPO) positions using multiple scanning planes .


Decubitus or right posterior oblique views can be very helpful in evaluating the distal common bile duct. Note obstructing echogenic
stone (arrow) in the dilated (1.5 cm) distal common bile duct (calipers).

Liver abscess
• On ultrasound, a liver abscess most commonly appears as a complex cystic mass with an irregular, shaggy border that demonstrates increased through transmission
use tissue harmonic imaging

hepatitis stage can manifestonly by
decreased echogenicity

Gray scale image demonstrating a complex hypoechoic cystic lesion in the liver (calipers). Echogenic material with
dirty distal shadowing represents air in the abscess
look indifferent anglesto avoid impedance from gas

Focal liver lesions
• Occasionally patients who have metastatic liver disease may present with acute RUQ pain.
• In patients who have diffuse metastatic disease, the pain likely is caused by swelling of the liver and stretching of the liver capsule .
• Hemorrhage into a liver mass or metastasis, however, also may cause acute RUQ pain. Subcapsular hematomas or free intraperitoneal hemorrhage also may occur following rupture a liver mass.

Mets
• Hepatic adenomas, hepatocellular carcinomas (HCCs), and vascular metastases are the liver masses most prone to hemorrhage.
• The risk of rupture is related to size and location, with larger size and subcapsular location being risk factors.
• subcapsular hematoma will appear as a crescentic-shaped area The mass is typically heterogenous in echotexture.

Hepatic subcapsular haematoma

• Spontaneous hemorrhage or rupture has been estimated to occur in up to 10% of HCCs .
• An echogenic rind surrounding the liver has been described as a common finding in this clinical scenario, representing either acute hemoperitoneum or subcapsular hematoma .

Ruptured HCC


Pancreas
• It may be difficult to visualize the pancreas in the setting of acute pancreatitis because of shadowing from overlying bowel gas and guarding on examination. In addition, such patients are typically NPO, and therefore, the stomach cannot be filled with fluid to provide an improved acoustic window. Placing the patient in the RPO or right decubitus position often will improve visualization of the pancreas, as air in the duodenum and antrum of the stomach will rise to the fundus on the left, and the antrum and duodenum will fill with fluid, providing a better acoustic window.
tech.hint

Acute pancreatitis
swollen hypoechoic pancreas
normal size

Oblique view through the right flank in a patient with upper abdominal pain reveals fluid in the peri-renal space and para-renal space. Note
hypoechoic, thickened para-renal fat linear, hypoechoic plane between the pancreas (P) and splenic vein/portal confluence .

peripancreatic/perirenal fluid
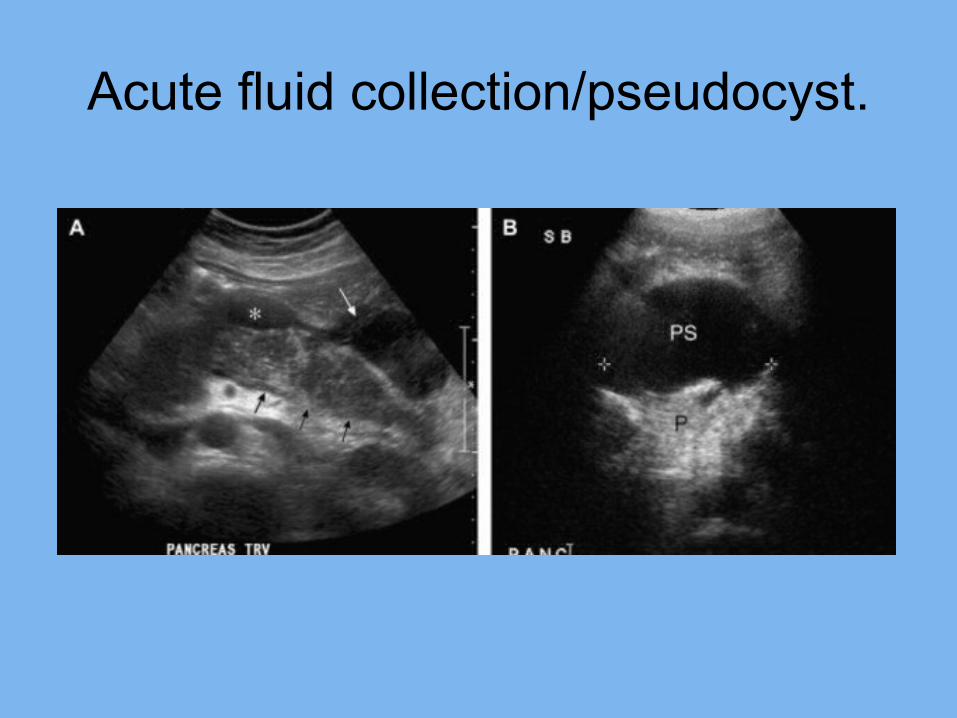
Acute fluid collection/pseudocyst.


Value of twinkle artefact

value of ureteric jet

Renal colic
calculus and hydronephrosis

UV junction stone with hydronephrosis

Pyonephrosis

Acute pyelonephritis
size
parenchymathickness

Pyelonephritis+GB wall thickening
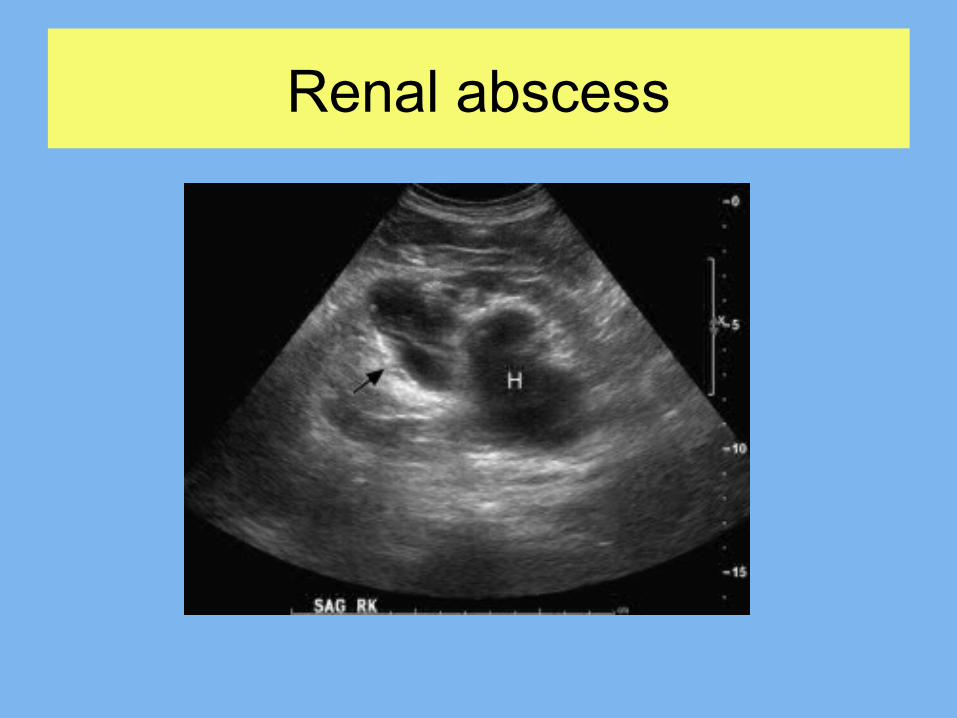
Renal abscess

Emphysmatous pyelonephritis
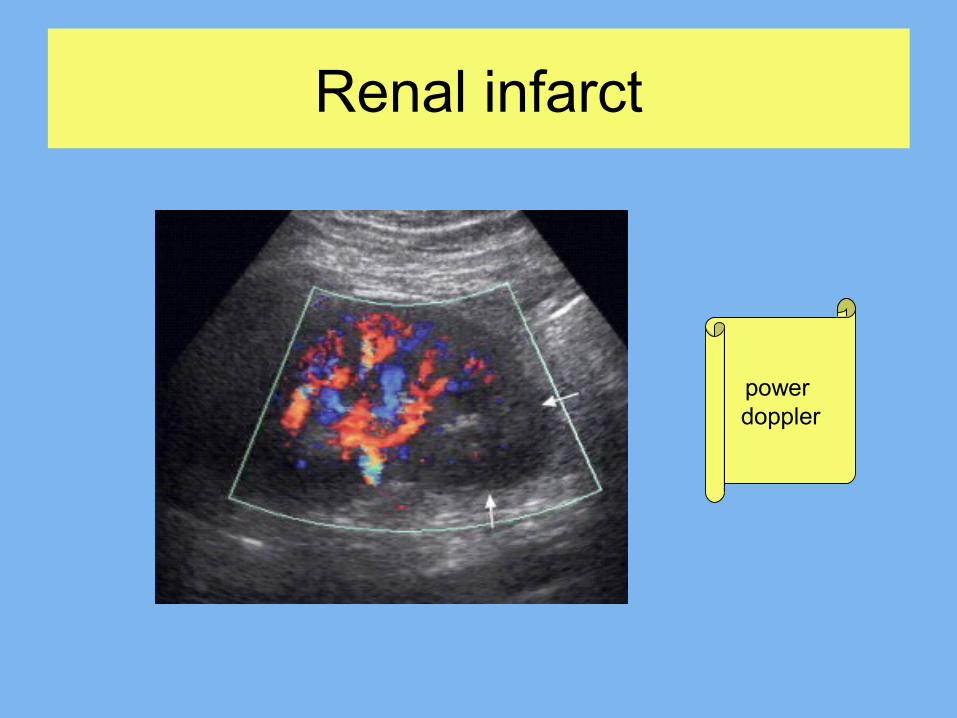
Renal infarct
power doppler

haemorrhage on AML/RCC

Perinephric haematoma

Adrenal haemorrhage

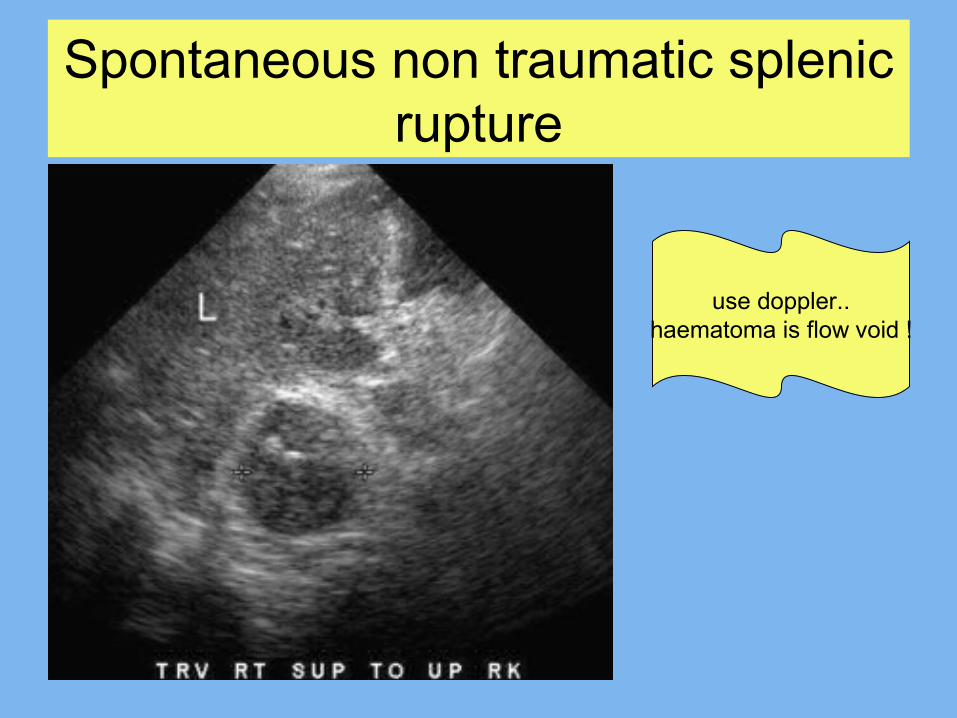
Spontaneous non traumatic splenic rupture
use doppler..haematoma is flow void !

Splenic infarction

Splenic abscess


Ruptured AAA

Abdominal aortic dissection
intimalflap


Acute appendicitis
dilated,uncompressible,aperistaltic,blind ended bowel loop>6mm

Appendicolith


Perforated appendicitis
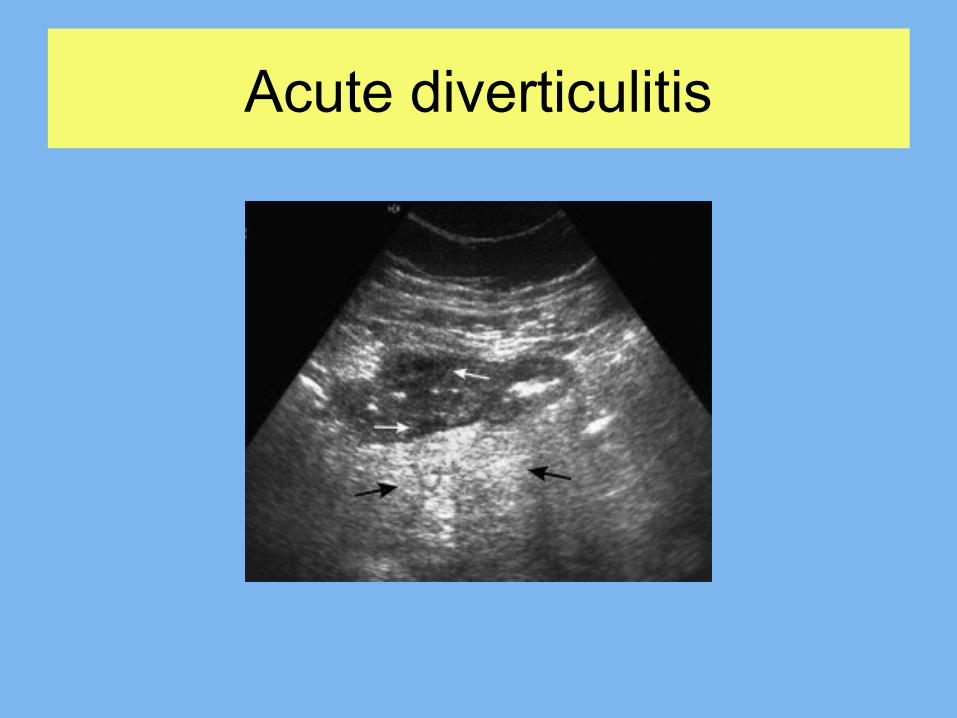
Acute diverticulitis

Typhlitis/ascending colitis

Pseudomembranous colitis

Small bowel obstruction

Intussusception

Free air

Ectopic pregnancy pillars of diagnosis

Ectopic pregnancy variability

Interstitial ectopic

Haemorrhagic corpus luteal cyst

Haemorrhagic corpus luteal cyst

Pelvic inflammatory disease
Fitz-Hugh-Curtis syndrome

Ovarian torsion


Rectus shealth haematoma
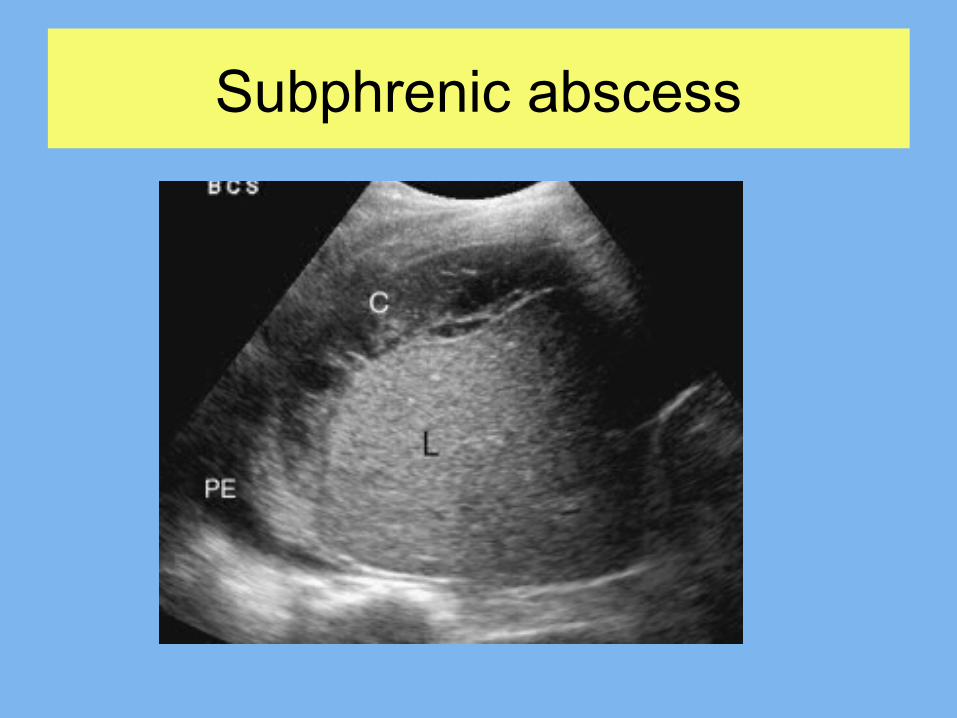
Subphrenic abscess

Pneumonia
air bronchogram








