

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Update in GI: WhatUpdate in GI: What’’s s New and UsefulNew and Useful
Walter J. Coyle, MD, FACP,FACGWalter J. Coyle, MD, FACP,FACG
Scripps Primary Care 2011Scripps Primary Care 2011
Movement of the TalkMovement of the Talk
Eosinophilic esophagitis: What is it and how do Eosinophilic esophagitis: What is it and how do I treat it?I treat it?
GERD: WhatGERD: What’’s New?s New?
Celiac Sprue: The epidemicCeliac Sprue: The epidemic
Hepatitis B and C: Newer RxHepatitis B and C: Newer Rx
Inflammatory Bowel Disease: Newer RxInflammatory Bowel Disease: Newer Rx
CRC screening: Follow the guidelinesCRC screening: Follow the guidelines

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Movement of the Talk Part IIMovement of the Talk Part II
Stool Transplants: The New RageStool Transplants: The New Rage
Rosacea and SIBO: New evidenceRosacea and SIBO: New evidence
Chronic nausea: a new linkChronic nausea: a new link
The Human Microbiome: Hot topicThe Human Microbiome: Hot topic Pro and Pre biotics: a rational approachPro and Pre biotics: a rational approach
C. difficileC. difficile: It will not go away!: It will not go away!
ConclusionsConclusions
Question Number 1Question Number 1
27 year old male 27 year old male presents with presents with intermittent solid food intermittent solid food dysphagia for years. He dysphagia for years. He has had 2 food has had 2 food impactions. He had impactions. He had childhood asthma. childhood asthma. The most likely The most likely diagnosis is?diagnosis is?
A.A. Peptic stricturePeptic stricture
B.B. SchatzkiSchatzki’’s rings ring
C.C. Eosinophilic esophagitisEosinophilic esophagitis
D.D. Adenocarcinoma of the Adenocarcinoma of the distal esophagusdistal esophagus
E.E. AchalasiaAchalasia

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Eosinophilic EsophagitisEosinophilic Esophagitis
Common, may be increasingCommon, may be increasing
Higher in males, younger pts with h/o atopyHigher in males, younger pts with h/o atopy
Strong association with food and aeroallergensStrong association with food and aeroallergens THE ALLERGIC ESOPHAGUSTHE ALLERGIC ESOPHAGUS
Adults: present with dysphagia, atypical GERD Adults: present with dysphagia, atypical GERD symptoms: Usually have years of symptomssymptoms: Usually have years of symptoms
Children: Failure to thrive, nausea or vomiting.Children: Failure to thrive, nausea or vomiting.
Eosinophilic EsophagitisEosinophilic Esophagitis
Linear FurrowsLinear Furrows
RingsRings
Diagnosis: Biopsy Diagnosis: Biopsy at endoscopyat endoscopy

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Eosinophilic EsophagitisEosinophilic Esophagitis
Eos. AbscessesEos. Abscesses
Long, often Long, often complex stricturescomplex strictures
Careful dilationCareful dilation
Eosinophilic EsophagitisEosinophilic Esophagitis
Mucosal tear after Mucosal tear after scope passagescope passage
Try medical Try medical treatment firsttreatment first

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Eosinophilic Esophagitis:Eosinophilic Esophagitis:TreatmentTreatment
PPIs have shown efficacy in up to 50% of ptsPPIs have shown efficacy in up to 50% of pts
Topical steroids useful but recent PC/Rand Topical steroids useful but recent PC/Rand studies have shown less efficacy then open label studies have shown less efficacy then open label studiesstudies Fluticosone or budesonide: Swallowed (not inhaled)Fluticosone or budesonide: Swallowed (not inhaled)
Allergy consultation: May be helpful in finding Allergy consultation: May be helpful in finding food or aeroallergen that is main culpritfood or aeroallergen that is main culprit
Am J Gastroenterol 2010; 105:747–756
GERD: WhatGERD: What’’s Hots Hot

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Nighttime GERD and SleepNighttime GERD and Sleep
National GERD survey:National GERD survey: GERD pts reported lower quality of life (QOL) than GERD pts reported lower quality of life (QOL) than
unaffected subjectsunaffected subjects11
Nocturnal GERD pts symptoms had lower physical and Nocturnal GERD pts symptoms had lower physical and mental QOL scores than other GERD subjects and controlsmental QOL scores than other GERD subjects and controls
Another national survey :Another national survey : 78% GERD pts have nighttime symptoms78% GERD pts have nighttime symptoms
75% noted that nighttime heartburn affected their sleep75% noted that nighttime heartburn affected their sleep
63% of those with nighttime heartburn believed it negatively 63% of those with nighttime heartburn believed it negatively influenced their ability to sleep wellinfluenced their ability to sleep well
Arch Intern Med 2009;161:45-52 Am J Gastroenterol 2003;98:1487-1493
GERD and BMI: WomenGERD and BMI: Women
N Engl J Med 2006;354:2340-2348.
An increase in BMI of 3.5 was associated with increased risk of frequent GERD symptoms, even in women with normal baseline weight
P<0.001 Multivariate odds in women with at least weekly GERD symptoms (n=2306) or no symptoms (n=3904)0
0.51
1.52
2.53
3.54
Od
ds
Rat
io
<20 20 22 25 27 30 ≥35
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
GERDGERD
PPIs are no longer viewed as innocuous medsPPIs are no longer viewed as innocuous meds Malabsorption of nutrientsMalabsorption of nutrients
Iron, calcium, Vitamin B12Iron, calcium, Vitamin B12
Increase risk for fracturesIncrease risk for fractures
Increase risk for infections including Increase risk for infections including Clostridium Clostridium difficiledifficile
Interaction with clopidogrelInteraction with clopidogrel
PPI use and Hip fracturePPI use and Hip fracture
CaseCase--control study of patients older than 50 control study of patients older than 50 years in a large UK databaseyears in a large UK database PPI users had a 4 /1000 risk for hip fx vs 1.8 /1000 in nonPPI users had a 4 /1000 risk for hip fx vs 1.8 /1000 in non--
users of acid related medsusers of acid related meds
Absolute risk still lowAbsolute risk still low
Seven case control or cohort trials have shown Seven case control or cohort trials have shown a small absolute increased risk of fracturesa small absolute increased risk of fractures
Recent metaRecent meta--analysis (DDW abs only) showed a analysis (DDW abs only) showed a slight increase in hip fx with PPI therapyslight increase in hip fx with PPI therapy
JAMA 2006;296:2947-29Calcif Tissue Int. 2008;83:251-259

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Long term PPI useLong term PPI use
AGA now recommends Calcium / Vit D in long AGA now recommends Calcium / Vit D in long term usersterm users
No guidelines for monitoring B12 or ironNo guidelines for monitoring B12 or iron Be aware, check when clinically indicatedBe aware, check when clinically indicated
Be aware of meds that absorb better with acidBe aware of meds that absorb better with acid Digoxin, amoxicillin, ketoconazole, iron, calciumDigoxin, amoxicillin, ketoconazole, iron, calcium
Organic (heme derived) iron now availableOrganic (heme derived) iron now available
PPIs and InfectionsPPIs and Infections
Studies have linked acid suppresion meds Studies have linked acid suppresion meds including PPIs with including PPIs with C. difficile C. difficile infectioninfection Higher recurrence of C diff if on PPI at time of RxHigher recurrence of C diff if on PPI at time of Rx
May increase risk for hospital acquired May increase risk for hospital acquired pneumoniapneumonia
Am J Gastro 2007;102:2047-56 CMAJ 2004;171:33-38JAMA. 2004;292:1955-60 Ann Intern Med. 2008;149:391-98Arch Intern Med 2010;170:772-8

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Arch Intern Med. 2010;170(9):772-778
42% more likely to recur if on PPIs
PPIs and clopidogrelPPIs and clopidogrel
US Food and Drug Administration: Drug Safety Information Nov 2009

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
N Engl J Med 2010;363:1909-17.
PPIs: WaltPPIs: Walt’’s Recss Recs
Right drug, right disease, right patientRight drug, right disease, right patient If your patient needs the PPI for PUD, GI bleeding, If your patient needs the PPI for PUD, GI bleeding,
BarrettBarrett’’s esophagus, then use the PPIs esophagus, then use the PPI Lowest dose that worksLowest dose that works
Use Calcium and Vit D in long term usersUse Calcium and Vit D in long term users
If it is symptomatic GERD only, other optionsIf it is symptomatic GERD only, other options Lifestyle changes, H2 blockers, antacidsLifestyle changes, H2 blockers, antacids
Informed consent to patient until final dataInformed consent to patient until final data
NB. More GI bleeding in Cogent study in nonNB. More GI bleeding in Cogent study in non--PPI PPI usersusers

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Celiac Sprue: WhatCeliac Sprue: What’’s New!s New!
Common gene: DQ2 and DQ8: Up to 25%Common gene: DQ2 and DQ8: Up to 25% Predisposes you only to CeliacPredisposes you only to Celiac
Actual disease in 1% in US: Iceberg analogyActual disease in 1% in US: Iceberg analogy
Gluten enteropathy VS Gluten intoleranceGluten enteropathy VS Gluten intolerance Gluten avoidance is in vogue!!!Gluten avoidance is in vogue!!!
Diagnosis: Gold standard remains SB biopsyDiagnosis: Gold standard remains SB biopsy
Serology: Tissue Transglutaminase and Serology: Tissue Transglutaminase and Endomysial antibody excellent sens/specificityEndomysial antibody excellent sens/specificity ALWAYS check serum IgA (IgA deficiency)ALWAYS check serum IgA (IgA deficiency)
Celiac BurdenCeliac Burden

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Celiac Issues and DilemmaCeliac Issues and Dilemma
Pt presents for Celiac testing on gluten free dietPt presents for Celiac testing on gluten free diet
Pt has negative serology (maybe even normal SB Pt has negative serology (maybe even normal SB biopsy) and insists they have celiacbiopsy) and insists they have celiac Role for genetic testingRole for genetic testing
Gluten intolerance vs Gluten enteropathyGluten intolerance vs Gluten enteropathy
Health Maintenance:Health Maintenance: Bone healthBone health
Liver diseaseLiver disease
Vitamin and mineral deficienciesVitamin and mineral deficienciesAm J Gastroenterol advance online pub, 1 March 2011
Gluten Causes Gastrointestinal Symptoms in Subjects Without Celiac Disease: A Double-Blind
Randomized Placebo-Controlled Trial
Jessica R. Biesiekierski , B Appl Sci 1 , Evan D. Newnham , MD, FRACP 1 , Peter M. Irving , MD, MRCP 1 , Jacqueline S. Barrett ,PhD, BSc, MND 1 , Melissa Haines , MD 1 , James D. Doecke , BSc, PhD 2 , Susan J. Shepherd , B Appl Sci, PhD 1 , Jane G. Muir ,PhD, PGrad Dip(Dietetics) 1 and Peter R. Gibson , MD, FRACP 1
Am J Gastroenterol advance online publication, 11 January 2011; doi: 10.1038/ajg.2010.487
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
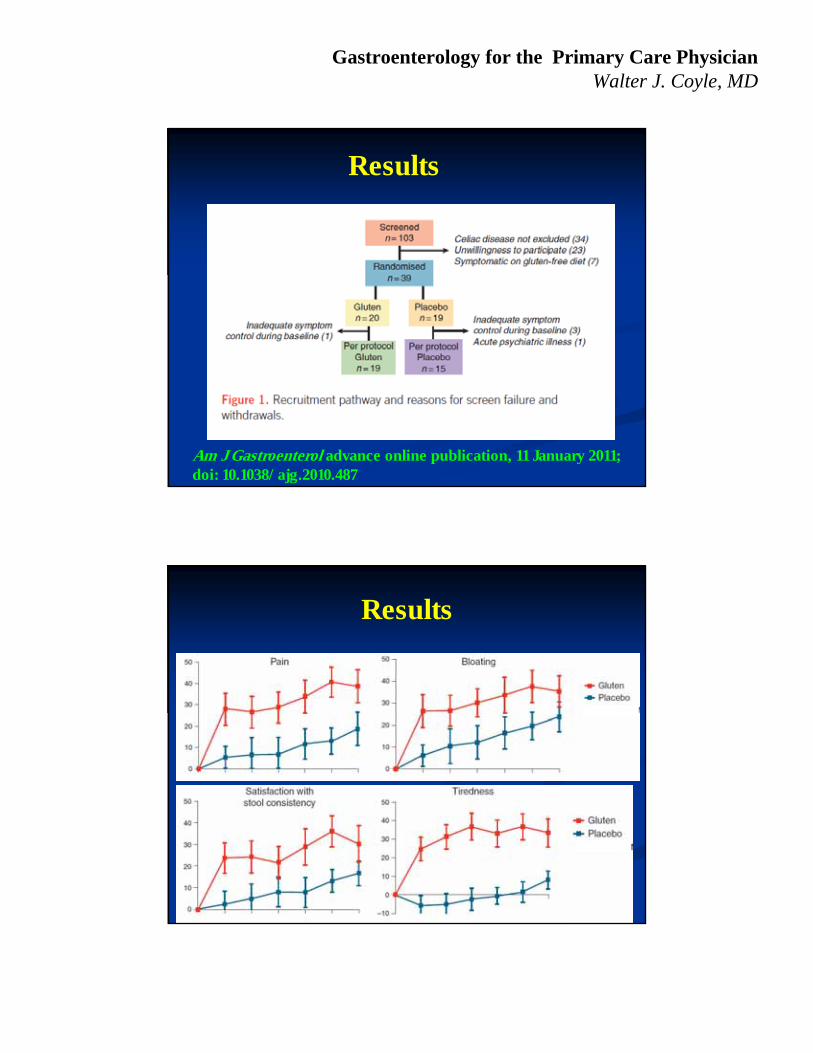
Results
Am J Gastroenterol advance online publication, 11 January 2011; doi: 10.1038/ajg.2010.487
Results

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Discussion
No prior randomized controlled trials demonstrating that the entity of “gluten intolerance” does actually exist
This study supports the existence of non-celiac gluten sensitivity based on the following symptoms: Bloating
Dissatisfaction with stool consistency
Abdominal pain
Tiredness
Future studies
Gluten may have the following deleterious effects in non-celiac patients: Increase fermentation, and thus, distension
Increase cholinergic activation, and thus, increased smooth muscle contractility
Increase enteric NS stimulation by gluten digestion creating neurally active peptides
Symptoms may not be related to gliadin proteins of gluten Carbohydrates – fructans (in wheat)

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Novak Djokavic claims his energy improved on gluten-free diet and coincided with his winning streak
“A gluten-free diet can have implications far beyond the physical, especially in tennis, which taxes the mind like few other sports.”
Hepatitis B Virus (HBV)
Image at left (10229): Courtesy of Centers for Disease Control and Prevention Public Health Image Library at: http://phil.cdc.gov/phil/home.aspImage at right adapted from Block TM, et al. Clin Liver Dis. 2007;11:685-706.
Transmission electron micrograph of HBV from blood of patient with
hepatitis B
Hepatitis B Virus
HBVDNA
pol
(–)(+)
Lipid Bilayer Envelope
CapsidCapsid
Lipid bilayer envelope

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Question Number 2
Most deaths from chronic hepatitis B are due to???
A. Portal hypertension
B. Glomerulonephritis
C. Spontaneous bacterial peritonitis
D. GI hemorrhage
E. Hepatocellular Ca
Complications of CHB
w Fibrosis• Consequence of ongoing liver
injury and repair1
w Cirrhosis• Risk of progression to cirrhosis of
untreated CHB is 2-6% per year2
w End-stage Liver Disease• Typically presents 3-5 years after
a diagnosis of CHB with cirrhosis2
w Hepatocellular Carcinoma• 70% of deaths in patients with
CHB are due to HCC, with or without cirrhosis3
1. Lim YS and Kim WR. Clin Liver Dis. 2008;12:733-746.2. Weisberg IS, et al. Clin Liver Dis. 2007;11:893-916. 3. Asian Liver Center. 2007 Physician’s Guide to Hepatitis B.
http://liver.stanford.edu/Media/publications/Handbook/2007Handbook.pdf. Accessed January 9, 2009.
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
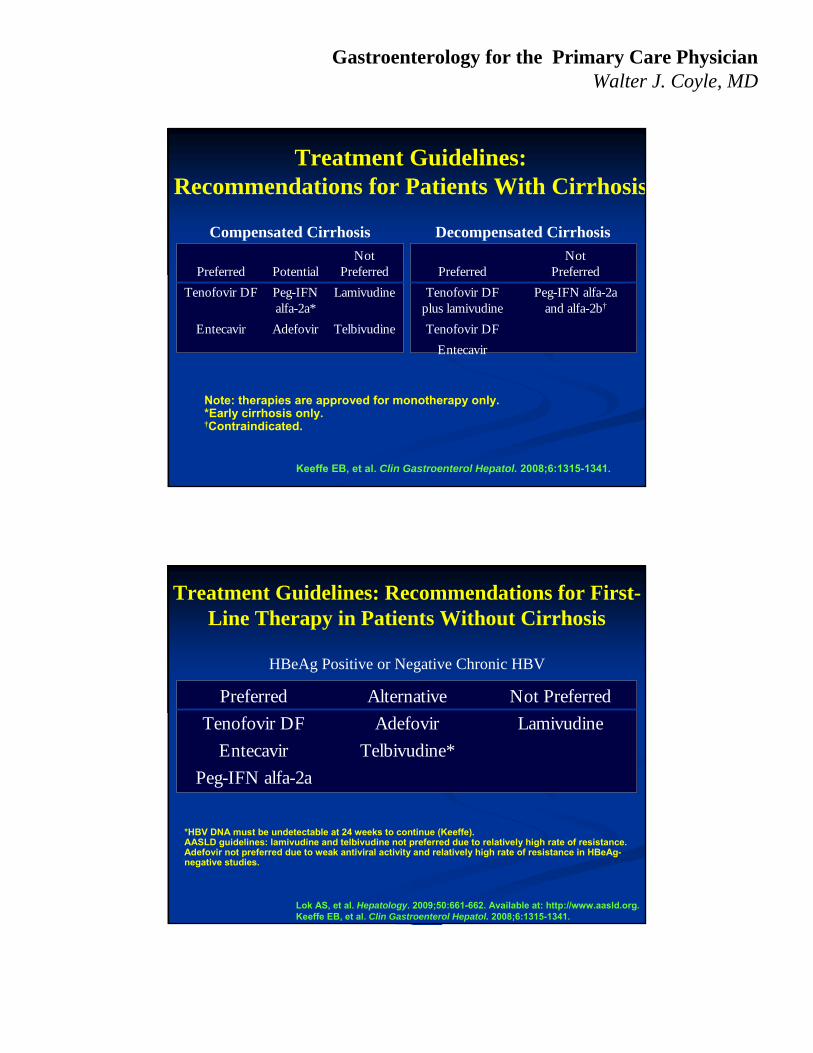
Treatment Guidelines:Recommendations for Patients With Cirrhosis
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2008;6:1315-1341.
Compensated Cirrhosis
Note: therapies are approved for monotherapy only. *Early cirrhosis only.†Contraindicated.
Preferred PotentialNot
Preferred
Tenofovir DF Peg-IFN alfa-2a*
Lamivudine
Entecavir Adefovir Telbivudine
Decompensated Cirrhosis
PreferredNot
Preferred
Tenofovir DF plus lamivudine
Peg-IFN alfa-2aand alfa-2b†
Tenofovir DF
Entecavir
Treatment Guidelines: Recommendations for First-Line Therapy in Patients Without Cirrhosis
HBeAg Positive or Negative Chronic HBV
*HBV DNA must be undetectable at 24 weeks to continue (Keeffe). AASLD guidelines: lamivudine and telbivudine not preferred due to relatively high rate of resistance. Adefovir not preferred due to weak antiviral activity and relatively high rate of resistance in HBeAg-negative studies.
Preferred Alternative Not Preferred
Tenofovir DF Adefovir Lamivudine
Entecavir Telbivudine*
Peg-IFN alfa-2a
Lok AS, et al. Hepatology. 2009;50:661-662. Available at: http://www.aasld.org.Keeffe EB, et al. Clin Gastroenterol Hepatol. 2008;6:1315-1341.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Duration of Treatment for Chronic HBV
HBeAg(+)• 6 to 12 months after HBsAg seroconversion to reduce relapse rate
HBeAg(-)• Relapse common after cessation of therapy; long-term treatment
currently recommended
Cirrhosis• Long-term therapy required
• Combination therapy commonly used
Keeffe EB. Clin Gastroenterol Hepatol. 2006;4:936-962.
Paul Pockros: The Last Great Hope

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Question Number 3
Hepatitis C is found in what percentage of US citizens???
A. 1%
B. 2%
C. 3%
D. 4%
E. 5%
Predictions for 2010-2019
• 193,000 HCV deaths– 720,700 million years of advanced liver disease– 1.83 million years of life lost
• $11 billion in direct medical care costs
• $21.3 and $54 billion societal costs from premature disability and mortality
Wong Am J Pub Health 2000
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Screening for HCV
2010 IOM Recommendation
-All patients born 1945-1964!
Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C Released: January 11, 2010 .
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
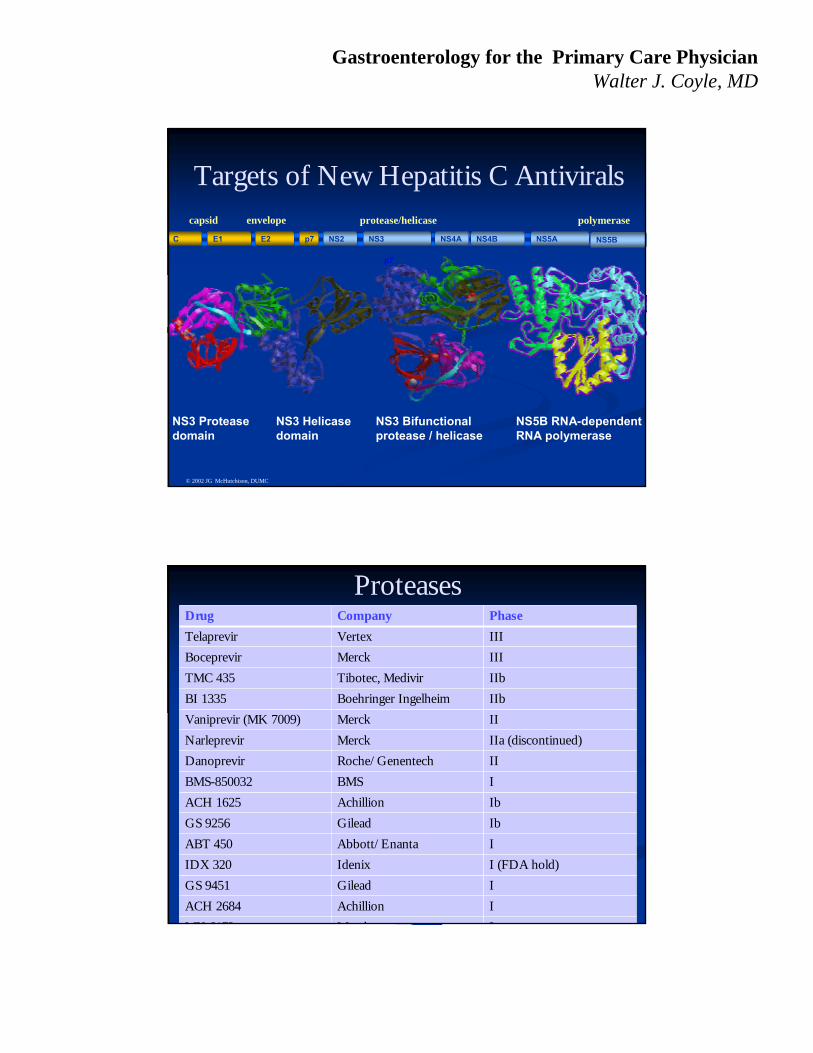
Targets of New Hepatitis C Antiviralscapsid
NS3 Protease domain
NS5B RNA-dependentRNA polymerase
C E1 E2 p7 NS2 NS3 NS4A NS4B NS5A NS5B
NS3 Helicase domain
NS3 Bifunctionalprotease / helicase
© 2002 JG McHutchison, DUMC
envelope protease/helicase polymerase
p7
ProteasesDrug Company Phase
Telaprevir Vertex III
Boceprevir Merck III
TMC 435 Tibotec, Medivir IIb
BI 1335 Boehringer Ingelheim IIb
Vaniprevir (MK 7009) Merck II
Narleprevir Merck IIa (discontinued)
Danoprevir Roche/Genentech II
BMS-850032 BMS I
ACH 1625 Achillion Ib
GS 9256 Gilead Ib
ABT 450 Abbott/Enanta I
IDX 320 Idenix I (FDA hold)
GS 9451 Gilead I
ACH 2684 Achillion I
MK 6172 M k I

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Emerging HCV Treatment Paradigm
• 2011: Peg-IFN + RBV + protease inhibitor
↓• 2014: Protease + polymerase +/or
other agents (+/or Peg-IFN +/or RBV)
Inflammatory Bowel DiseaseInflammatory Bowel Disease
Newer ConceptsNewer Concepts
TreatmentTreatment
Top down VS Step upTop down VS Step up

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
IMMUNE RESPONSE
GENETICSUSCEPTIBILITY
ENVIRONMENTALTRIGGERS & MODIFIERS
Current Model:Current Model:Pathogenesis of CrohnPathogenesis of Crohn’’s s
Disease and UCDisease and UC
Bickston SJ, et al. Curr Gastroenterol Rep. 2003;5:518.Bickston SJ, et al. Curr Gastroenterol Rep. 2003;5:518.
Environment and IBDEnvironment and IBD
Geographic distributionGeographic distribution Increase incidence in emigrants to NorthIncrease incidence in emigrants to North
SmokingSmoking
Germ free animals do not get IBDGerm free animals do not get IBD Influence of the microbiomeInfluence of the microbiome
? Infectious (? Infectious (M. paratuberculosis, E.coliM. paratuberculosis, E.coli, , Measles) Measles) –– Antibody testing Antibody testing
Diet and Diversion of fecal streamDiet and Diversion of fecal stream

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Environmental TriggersEnvironmental TriggersInflammatoryBowel Disease
Infections
NSAIDsNSAIDs
StressStressSmokingSmoking
DietDiet
AntibioticsAntibiotics
IBDIBD
Normal Intestine vs. Normal Intestine vs. Intestine With IBDIntestine With IBD
Normal bowel: controlled inflammationNormal bowel: controlled inflammation
Normally: inflammationIs down-regulatedNormally: inflammationIs down-regulated
IBD: failure todown-regulate inflammation
IBD: failure todown-regulate inflammation
Chronic uncontrolledinflammation = IBDChronic uncontrolledinflammation = IBD
Environmentaltriggers (medicationsinfections, diet?)
Environmentaltriggers (medicationsinfections, diet?)
Inflamed bowelInflamed bowel
Normal bowel:controlled inflammation
Normal bowel:controlled inflammation

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Management Goals in IBDManagement Goals in IBD
Define disease extent and severity and type Evaluate for extra-intestinal disease and
complications Induction of clinical remission
– Short term side effects balanced vs. disease severity
Maintenance of remission– Medical vs. Surgical– STEROID SPARING************************
Education and improvement of quality of life “Step up” vs “Top down therapy”
Therapeutic Options in IBDTherapeutic Options in IBD
Crohn’s Disease– 5-Aminosalicylates– Antibiotics– Corticosteroids– 6-MP/AZA– Methotrexate– Biologics (TNFs)– Tacrolimus– Probiotics?– Surgery
Ulcerative Colitis– 5-Aminosalicylates
– Corticosteroids
– 6-MP/AZA
– Cyclosporine
– Biologics (only infliximab to date)
– Probiotics?
– Surgery

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Top down vs Step up RxTop down vs Step up Rx
Should we use TNFs earlierShould we use TNFs earlier
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Summary for IBDSummary for IBD
Pathogenesis remains obscure stillPathogenesis remains obscure still Role of Microbiome keyRole of Microbiome key
Serology has limited role in diagnosisSerology has limited role in diagnosis Helpful in borderline casesHelpful in borderline cases
Treatment options have increasedTreatment options have increased Individualized therapy bestIndividualized therapy best
Top down appropriate for some patientsTop down appropriate for some patients
Question Number 3Question Number 3
Which of the following Which of the following extraextra--intestinal intestinal manifestations of IBD manifestations of IBD does not respond to does not respond to treatment of the IBD???treatment of the IBD???
A.A. Primary sclerosing Primary sclerosing cholangitischolangitis
B.B. Erythema nodosumErythema nodosum
C.C. SacroileitisSacroileitis
D.D. Acute arthritisAcute arthritis
E.E. A and CA and C
F.F. B and DB and D

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Colon Cancer ScreeningColon Cancer Screening
Review of the GuidelinesReview of the Guidelines
Question Number 3Question Number 3
What is the lifetime What is the lifetime risk for colon risk for colon cancer in the cancer in the United States?United States?
A.A. 2%2%
B.B. 4%4%
C.C. 6%6%
D.D. 8%8%
E.E. 10%10%

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Colon CancerColon Cancer
Second most common cause of cancer deathSecond most common cause of cancer death
Prototypical disease for screeningPrototypical disease for screening Intermediate probability of diseaseIntermediate probability of disease
Significant impact on public healthSignificant impact on public health
Well defined, modifiable disease progressionWell defined, modifiable disease progression
USPSTFUSPSTF ACS ACRACS ACR
USMSTFCCUSMSTFCC
ACGACG
AgeAge 5050--7575 5050 50/45 AfAm50/45 AfAm
ColonoscopyColonoscopy 10 yrs10 yrs 10 yrs10 yrs 10yrs10yrs
Flex SigFlex Sig 5 yrs5 yrs 55--10 yrs10 yrs
FS/FOBTFS/FOBT 5 yrs/ 3 yrs5 yrs/ 3 yrs
DCBEDCBE 5 yrs5 yrs
CT CT ColonographyColonography
Insuff EvidInsuff Evid 5 yrs5 yrs 5 yrs5 yrs
FOBTFOBT YearlyYearly YearlyYearly YearlyYearly
FITFIT YearlyYearly YearlyYearly Pt refusesPt refuses
Stool DNAStool DNA ??
Current Guidelines

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Average Risk Screening: Average Risk Screening: RecommendationsRecommendations
Stool cards(yearly); FIT??
Flexiblesigmoidoscopy(every 3–5 years)
Colonoscopy(every 10 years)
Barium enema(every 5 years)
OR
OR
AND
FUTURE?Stool DNACT colonographyCapsule Colonoscopy
≥50 years old
Preferred: ACG and MSGITFPreferred: ACG and MSGITF
Option: USPSTF, ACS, AGAOption: USPSTF, ACS, AGA
New Recommendations for New Recommendations for AfricanAfrican--AmericansAmericans
Younger mean age at diagnosis (60Younger mean age at diagnosis (60––66 years)66 years)
Higher incidence ratesHigher incidence rates
Higher mortality ratesHigher mortality rates
More proximal distribution of cancers and adenomasMore proximal distribution of cancers and adenomas
Recent American College of Gastroenterology Recent American College of Gastroenterology recommendations to beginrecommendations to begin averageaverage--risk screening at risk screening at age 45age 45
http://seer.cancer.gov/csr/1975http://seer.cancer.gov/csr/1975--2000. Access February 23, 2006. Agrawal S, et al. 2000. Access February 23, 2006. Agrawal S, et al. Am J Gastroenterol.Am J Gastroenterol. 2005;100:5152005;100:515––523. Ghafoor A, et al. 523. Ghafoor A, et al. CA Cancer J Clin.CA Cancer J Clin.2002;52:3262002;52:326––341.341.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Screening Compliance is LowScreening Compliance is Low
Cancer Prevention and Early Detection, Fact s and Figures 2008
Stool Transplants:Stool Transplants:Everyone is doing it!Everyone is doing it!

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Stool Transplants: How ToStool Transplants: How To
Stool transplants: Stool transplants: ““preparedprepared”” feces by feces by NGT or enema or colonoscopyNGT or enema or colonoscopy
Usually family member; 30Usually family member; 30--50 g fresh 50 g fresh stoolstool
Stool homogenized for deliveryStool homogenized for delivery
No infectious complications to dateNo infectious complications to date
Screen for Hepatitis, HIV, etcScreen for Hepatitis, HIV, etc……
7373--100% response reported in C Diff100% response reported in C Diff
Gastro 2006;130 Clin Infect Dis 2003;36
Stool Transplant: EvidenceStool Transplant: Evidence
2003 case series of refractory 2003 case series of refractory C diffC diff patients patients Stool via NG from healthy family memberStool via NG from healthy family member
15 of 18 became recurrence15 of 18 became recurrence--freefree
2009 case series of refractory 2009 case series of refractory C diff C diff patientspatients 11 of 15 became recurrence11 of 15 became recurrence--freefree
2010 case series of refractory C diff patients2010 case series of refractory C diff patientsStool via colonoscopyStool via colonoscopy
12 of 12 with immediate and sustained response12 of 12 with immediate and sustained response
Clin Infect Dis 2003;36: 540-544 QJM 2009;102:781-784 Yoon, J of Clin Gastro 2010, 44:562-66

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Colonoscopy Stool TransplantsColonoscopy Stool Transplants
Coming to your neighborhood soonComing to your neighborhood soon……..
Stool transplants done here.
Donations accepted.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
CoyleCoyle’’s Corollarys Corollary
It is better to be a stool donor
than a recipient.
Stool donor cards will be made available after this
lecture.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Stool Donor Card
Share your stool; stop C diff
Clinical Gastro Hep 2008; 759-764

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
MethodsMethods
Prosp. study; 113 pts with rosacea 60 controlsProsp. study; 113 pts with rosacea 60 controls
Derm Assessment by two docsDerm Assessment by two docs 7 point scale7 point scale
All subjects completed global scoreAll subjects completed global score
Baseline labs, Urease BT, H2 Breath testsBaseline labs, Urease BT, H2 Breath tests Lactulose BT: 1Lactulose BT: 1stst, + test if double peak seen, + test if double peak seen
Glucose BT: 2Glucose BT: 2ndnd (1 wk later), + test single peak(1 wk later), + test single peak
Hp + pts, treated then reHp + pts, treated then re--tested by H2 BTtested by H2 BT
If both Hp + and SIBO+: rx SIBO 1stIf both Hp + and SIBO+: rx SIBO 1st
Results: SIBO pos and neg ptsResults: SIBO pos and neg pts
Clinical Gastro Hep 2008; 759-764

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Rosacea and the MicrobiomeRosacea and the Microbiome
DiscussionDiscussion
SIBO common in Rosacea ptsSIBO common in Rosacea pts
Esp those with papulopustulesEsp those with papulopustules
Rx of SIBO results in dramatic improvement of rashRx of SIBO results in dramatic improvement of rash
78% resolved/17% improved (95% total)78% resolved/17% improved (95% total)
Affect is sustained (9 months); relapse can be reAffect is sustained (9 months); relapse can be re--treatedtreated
Hypothesis: SIBO increases intest absorption of Hypothesis: SIBO increases intest absorption of bacterial products, esp endotoxin, proinflam cytokinesbacterial products, esp endotoxin, proinflam cytokines
SIBO more important then colonic bacteria (SIBO SIBO more important then colonic bacteria (SIBO neg rosacea pts did not respond as well)neg rosacea pts did not respond as well)
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
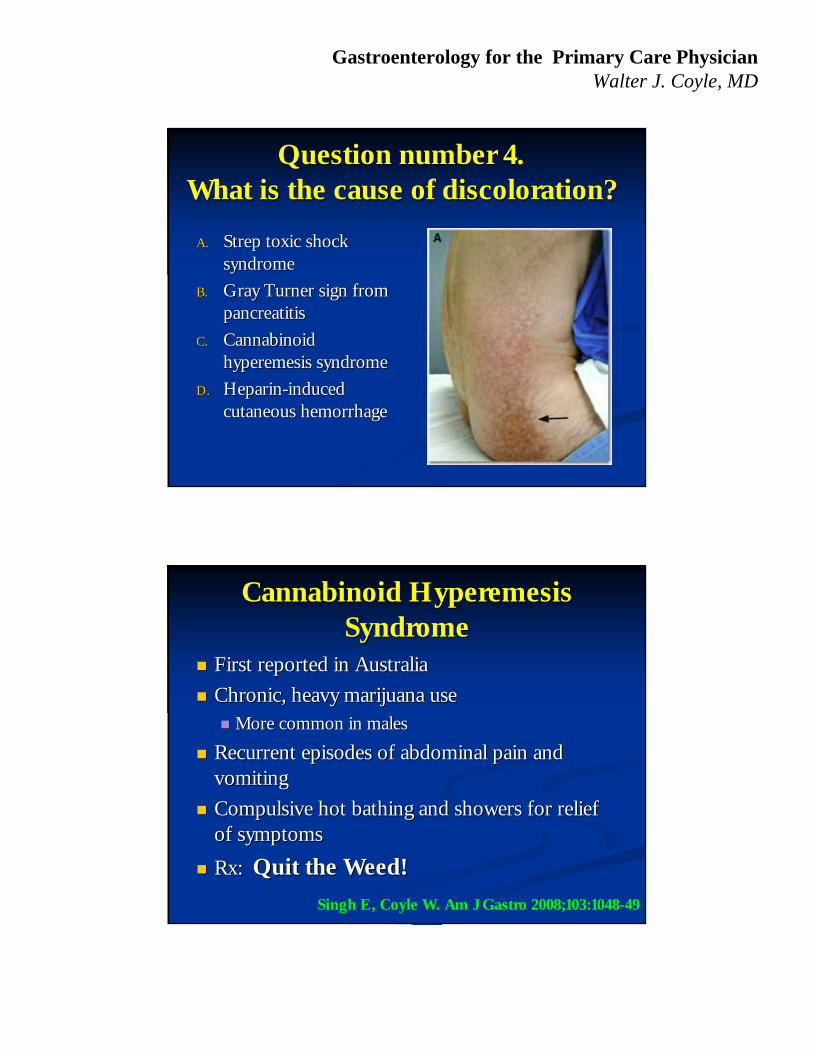
Question number 4.Question number 4.What is the cause of discoloration?What is the cause of discoloration?
A.A. Strep toxic shock Strep toxic shock syndromesyndrome
B.B. Gray Turner sign from Gray Turner sign from pancreatitispancreatitis
C.C. Cannabinoid Cannabinoid hyperemesis syndromehyperemesis syndrome
D.D. HeparinHeparin--induced induced cutaneous hemorrhagecutaneous hemorrhage
Cannabinoid Hyperemesis Cannabinoid Hyperemesis SyndromeSyndrome
First reported in AustraliaFirst reported in Australia
Chronic, heavy marijuana useChronic, heavy marijuana use More common in malesMore common in males
Recurrent episodes of abdominal pain and Recurrent episodes of abdominal pain and vomitingvomiting
Compulsive hot bathing and showers for relief Compulsive hot bathing and showers for relief of symptomsof symptoms
Rx: Rx: Quit the Weed!Quit the Weed!
Singh E, Coyle W. Am J Gastro 2008;103:1048-49

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
The Microbiome and The Microbiome and ProbioticsProbiotics
The Human MicrobiomeThe Human Microbiome
Definitions: Definitions: Microbiome: Aggregate of all gut speciesMicrobiome: Aggregate of all gut species Microbiota: Individual bacterial species in the biomeMicrobiota: Individual bacterial species in the biome
Over 100 trillion organisms (10Over 100 trillion organisms (101414)) Passengers in the mobile colonic petri dishPassengers in the mobile colonic petri dish Over 500 species identified so far (70 divisions)Over 500 species identified so far (70 divisions) 90% of the cells in our body our microbial!90% of the cells in our body our microbial!
100 fold more genes in our gut then in us100 fold more genes in our gut then in us Our flora are an integral part of our genetic Our flora are an integral part of our genetic
landscape and evolutionlandscape and evolution

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
The Human Gut Flora
DiBiase, et al. Mayo Clin Proc 2008;83:460-469
Microbes and Humans
Dethlefsen Nature 2007; 449:812-818

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Gut Flora and MetabolismGut Flora and Metabolism
Microbial genomes enhance our metabolic activityMicrobial genomes enhance our metabolic activity May indirectly or directly effect our metabolismMay indirectly or directly effect our metabolism
The colon is very active metabolicallyThe colon is very active metabolically 2020--70 gms of carbos and 570 gms of carbos and 5--20 gms of protein/day20 gms of protein/day
Over 100 kcal per day!Over 100 kcal per day!
Mass of colonic microbiome = single kidneyMass of colonic microbiome = single kidney Metabolically as active as the liverMetabolically as active as the liver
Hooper, et al. Annu Rev Nutr, 2002
ProbioticsProbiotics
Definition: Live microorganisms which when Definition: Live microorganisms which when ingested in adequate amounts confer a health ingested in adequate amounts confer a health benefit on the host. benefit on the host.
Majority of probiotics are Gram +, lactic acid Majority of probiotics are Gram +, lactic acid producers (ie. Firmacutes)producers (ie. Firmacutes) Bifidobacterial species and Bifidobacterial species and LactobacillusLactobacillus speciesspecies Survive transit through stomach and duodenumSurvive transit through stomach and duodenum
Others include: nonOthers include: non--pathogenic streptococci, pathogenic streptococci, enterococci, enterococci, E coliE coli Nissle 1917, Nissle 1917, Saccharomyces Saccharomyces boulardiiboulardii (yeast)(yeast)
Fooks, et al. Int Dairy J, 1999 Sheil, et al. In Gastrointestinal Microbiology, 2006

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Question Number 5Question Number 5
Which probiotic Which probiotic has been shown to has been shown to decrease mucosal decrease mucosal ILIL--6 levels?6 levels?
A.A. Lactobacillis acidopholusLactobacillis acidopholus
B.B. Bifidobacter infantisBifidobacter infantis
C.C. Saccharomyces boulardiiSaccharomyces boulardii
D.D. Lactobacillus rhamnosus Lactobacillus rhamnosus GGGG
ProbioticsProbiotics
VSL #3VSL #3
4 lactobacilli4 lactobacilli L. plantarum, casei, L. plantarum, casei,
acidopholus, delbrueckii acidopholus, delbrueckii sppspp
3 bidifobacteria3 bidifobacteria B. infantis, breve, longumB. infantis, breve, longum
1 streptococcus1 streptococcus Streptococcus salivarius ssp. Streptococcus salivarius ssp.
thermophilusthermophilusRand, PC studies have shown efficacy in pouchitis and IBSSome efficacy in mild/mod UC in new study

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
ProbioticsProbiotics
Digestive AdvantageDigestive Advantage Ganeden BCGaneden BC3030
Bacillus coagulansBacillus coagulans
ErythritolErythritol
CelluloseCellulose
Other minor ingredients Other minor ingredients
Some data for IBSSome data for IBS Mostly bloatingMostly bloating
Postgrad Med, Vol. 121, Issue 2, March 2009
ProbioticsProbiotics
Bifidobacterium infantisBifidobacterium infantis35624 aka Bifantis 35624 aka Bifantis
““PatentedPatented”” strain of strain of probiotic in Alignprobiotic in Align
Decreased symptoms in Decreased symptoms in two large trials in two large trials in subjects with IBS*subjects with IBS*
*Whorwell P, et al. Am J Gastro 2006; 101O’Mahoney L, et al. Gastro 2005;128

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
ProbioticsProbiotics
Saccharomyces Saccharomyces boulardiiboulardii
Other minor ingredientsOther minor ingredients
Shown in Rand / PC Shown in Rand / PC trials to help prevent trials to help prevent recurrent recurrent C. difficileC. difficileinfectioninfection
Decreases antibiotic Decreases antibiotic associated diarrheaassociated diarrhea
Am J Gastroenterol. 2006 Apr;101(4):812-22McFarland, et al. JAMA 1994;271:1913-8
Probiotics in Food (Actimel)Probiotics in Food (Actimel)
L. caseiL. casei ImmunitasImmunitas™™
Claim it is scientifically Claim it is scientifically proven to be effectiveproven to be effective
““Each bottle contains Each bottle contains 10 billion live10 billion live”” bacteria bacteria ““that survive and that survive and remain active in theremain active in the
digestive tract.digestive tract.””

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Probiotics in Food (Activia)Probiotics in Food (Activia)
Contains Contains Bifidus regularisBifidus regularis
Bifidobacterium animusBifidobacterium animus
Scientific trials show Scientific trials show increased transit time in increased transit time in adults and womenadults and women
““Helps with slow transit in Helps with slow transit in women and the elderlywomen and the elderly””
Bioscience and Microflora, 2001;20:43-48,Aliment Pharn Ther 2002;16:587-93
Probiotics for Immune SystemProbiotics for Immune System
Lactobacillus rhamnosusLactobacillus rhamnosus GG (ATCC GG (ATCC 53103)53103)
Patented by Gorbach and GoldinPatented by Gorbach and Goldin
Various studies have shown it to Various studies have shown it to be better than placebo for diarrheal be better than placebo for diarrheal illnessesillnesses
Proven to survive the stomach, Proven to survive the stomach, produces lactic acid and binds to produces lactic acid and binds to human colonocyteshuman colonocytes
BMJ 2007; 335 : 340-345

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Probiotics and prebiotics in maintenance of Probiotics and prebiotics in maintenance of remission in Crohnremission in Crohn’’s diseases disease
Study Groups Relapse Rate (%)
n Intervention Comparator Dur Intervention Comparator p
Guslandi (2000)
32 S. Bouliardii +
Mesalamine
Mesalamine 6 6 38 0.04
Campieri (2000)
40 VSL #3 Mesalamine 12 20 40 NR
Prantera (2002)
45 LGG Placebo 12 17 11 0.3
Schultz (2004)
11 LGG Placebo 6 60 67 NS
Bousvaros (2005)
75 LGG Placebo 24 31 17 0.18
Marleau (2006)
98 L. johnsonii Placebo 6 49 64 0.15
Van Gossum (2007)
70 L. johnsonii Placebo 3 15 14 0.91
Chermesh (2007)
30 Synbiotic 2000
Placebo 24 25 20 NS
Clostridium difficileClostridium difficile

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Clostridium difficile Clostridium difficile and altered and altered microbiotamicrobiota
Confirmed BI NAP1 strainConfirmed BI NAP1 strain
Gerding, et al. GASTRO 2009;136:1913–1924

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Metronidazole failuresMetronidazole failures
Leffler and Lamont in GASTRO 2009;136:1899–1912
New New C Difficile C Difficile Rx GuidelinesRx Guidelines
Infect Control Hosp Epidemiol 2010; 31(5):431-455
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
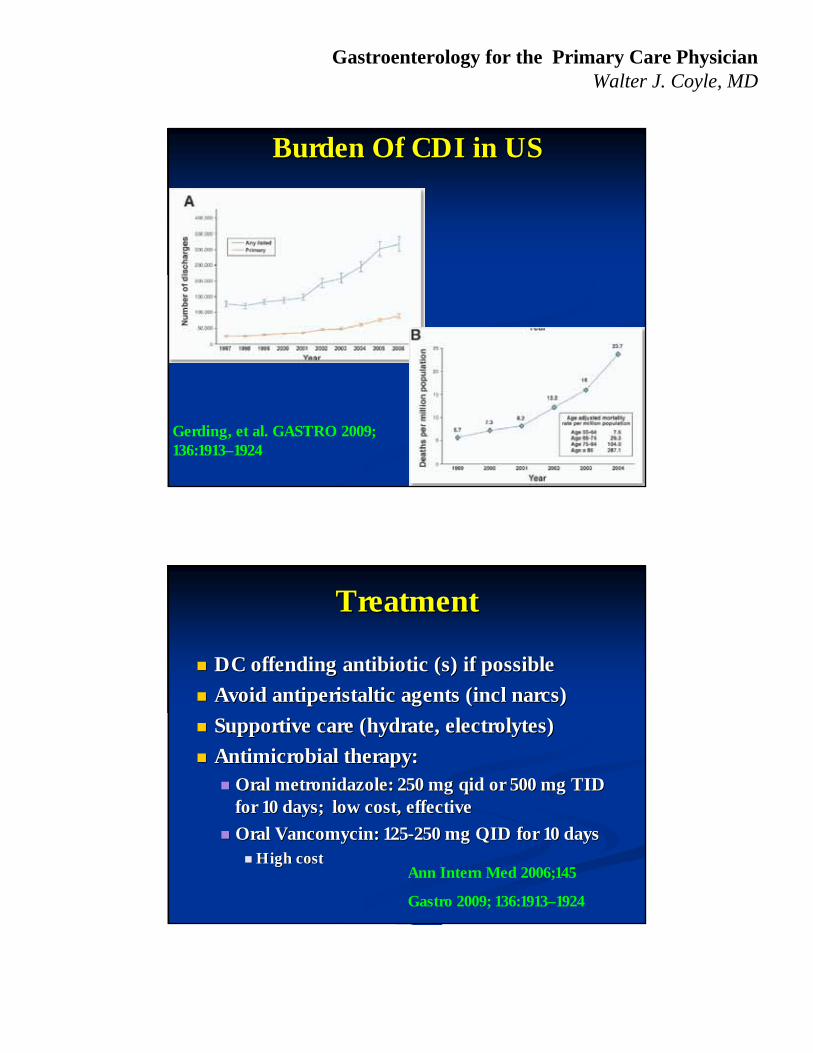
Burden Of CDI in USBurden Of CDI in US
Gerding, et al. GASTRO 2009; 136:1913–1924
TreatmentTreatment
DC offending antibiotic (s) if possibleDC offending antibiotic (s) if possible
Avoid antiperistaltic agents (incl narcs)Avoid antiperistaltic agents (incl narcs)
Supportive care (hydrate, electrolytes)Supportive care (hydrate, electrolytes)
Antimicrobial therapy:Antimicrobial therapy: Oral metronidazole: 250 mg qid or 500 mg TID Oral metronidazole: 250 mg qid or 500 mg TID
for 10 days; low cost, effectivefor 10 days; low cost, effective
Oral Vancomycin: 125Oral Vancomycin: 125--250 mg QID for 10 days250 mg QID for 10 days High costHigh cost
Ann Intern Med 2006;145
Gastro 2009; 136:1913–1924

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Recurrence: Probiotic Treatment Recurrence: Probiotic Treatment of of C difficileC difficile
ProbioticsProbiotics
Saccharomyces boulardii: 500 mg bid for 4Saccharomyces boulardii: 500 mg bid for 4--6 wks6 wks
Best evidence of all probioticsBest evidence of all probiotics
Several DB / PC trials show good efficacySeveral DB / PC trials show good efficacy
Lactobacilli: 1 g qid for 4Lactobacilli: 1 g qid for 4--6 weeks6 weeks
Evidence not as convincingEvidence not as convincing
PO nontoxicogenic C Diff: experimentalPO nontoxicogenic C Diff: experimental
Effective but only case reports to dateEffective but only case reports to date
Gastro 2006;130 Ann Intern Med 2006; 145 Am J Gastroenterol 2006; 101:812–822.
FidaxomicinFidaxomicin
Macrocyclic antibioticMacrocyclic antibiotic
Cure: 88.2% vs 85.8% vancomycinCure: 88.2% vs 85.8% vancomycin
Recurrence Rate: 15.4 % vs 25.3 % Recurrence Rate: 15.4 % vs 25.3 %
FDA approved.FDA approved.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
FidaxomicinFidaxomicin
NEJM 2011;364:422-431
FidaxomicinFidaxomicin
FDA approved May 2011FDA approved May 2011
Macrolide Ab: Aka Macrolide Ab: Aka DificidDificid
Dose: 200 mg BID for 10 daysDose: 200 mg BID for 10 days
Estimated cost: $2800 for full courseEstimated cost: $2800 for full course
WaltWalt’’s Recs Rec: : Not first line, too expensiveNot first line, too expensive Save for recurrent Save for recurrent C. difficileC. difficile infectionsinfections

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Probiotics and DiarrheaProbiotics and Diarrhea
135 hospitalized pts given antibiotics135 hospitalized pts given antibiotics
DB, PC, Rand trialDB, PC, Rand trial
Probiotic Yogurt (Actimel) or PC BIDProbiotic Yogurt (Actimel) or PC BID
Diarrhea: 34% PC vs 12% active (NNT:5)Diarrhea: 34% PC vs 12% active (NNT:5)
C DiffC Diff: Less often in Rx arm (NNT: 6): Less often in Rx arm (NNT: 6)
First rand trial to show prevention of First rand trial to show prevention of C diff C diff with with probioticsprobiotics
Hickson M, et al. BMJ, 2007:335-80
Probiotics and PancreatitisProbiotics and PancreatitisNot all good news!Not all good news!
296 hospitalized pts with acute pancreatitis given 296 hospitalized pts with acute pancreatitis given probioticsprobiotics
DB, PC, Rand trial; Given in tube feedingsDB, PC, Rand trial; Given in tube feedings
Probiotic : Ecologic 642 (Probiotic : Ecologic 642 (L. acidophilus, casei, L. acidophilus, casei, salivarius, lactis and B. bifidum, lactissalivarius, lactis and B. bifidum, lactis.).)
Morbidity: No difference in infectionsMorbidity: No difference in infections
Mortality: 24 (16%) vs 9 (6%) in PCMortality: 24 (16%) vs 9 (6%) in PC 9 pts in Rx arm developed ischemic bowel9 pts in Rx arm developed ischemic bowel
Besselink M, Gooszen H, et al Lancet 2008:371:651-659
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
PrebioticsPrebiotics
PrebioticsPrebiotics
Ingested substances that selectively stimulate the Ingested substances that selectively stimulate the proliferation and/or activity of desirable proliferation and/or activity of desirable bacterial populations present in the host bacterial populations present in the host intestinal tract.intestinal tract.
Usually target bifidobacteria and lactobacilliUsually target bifidobacteria and lactobacilli Bifidogenic or bifidus factors explored in the 50sBifidogenic or bifidus factors explored in the 50s
Usually are nonUsually are non--digestible oligosaccharides digestible oligosaccharides (NDOs)(NDOs) Lactulose, galactoLactulose, galacto--oligosaccharides, lactosucroseoligosaccharides, lactosucrose……
Crittenden and Playne. In Gastrointestinal Microbiology, 2006, pg 285-314.

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
PrebioticsPrebiotics
Inulin: plant polymers Inulin: plant polymers mainly comprising mainly comprising fructose units, use have a fructose units, use have a terminal glucoseterminal glucose
Indigestable fiberIndigestable fiber
Gut flora produce H2, Gut flora produce H2, CO2, methane gas from CO2, methane gas from inulininulin
PrebioticsPrebiotics
Inulin: plant polymers mainly Inulin: plant polymers mainly comprising fructose units, comprising fructose units, use have a terminal glucoseuse have a terminal glucose
Indigestable fiberIndigestable fiber
Gut flora produce H2, CO2, Gut flora produce H2, CO2, methane gas from inulinmethane gas from inulin
““Breakfast of FlatulanceBreakfast of Flatulance””

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
PrebioticsPrebiotics
Feed your flora!!!
PrebioticsPrebiotics
Is is possible to design a food, sugar, protein, or Is is possible to design a food, sugar, protein, or fat that would alter your gut flora to promote fat that would alter your gut flora to promote weight loss?weight loss?
More likely possibility is to give a prebiotic that More likely possibility is to give a prebiotic that decreases your decreases your ““Energy HarvestEnergy Harvest”” of colonic of colonic bacteriabacteria ie. lose weight by making your gut flora less efficient ie. lose weight by making your gut flora less efficient
at digesting your left over food at digesting your left over food

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Designing Probiotics: The Future?Designing Probiotics: The Future?
GASTROENTEROLOGY 2009;136:2015–2031
ConclusionsConclusions
Future studies must focus on the mechanisms of Future studies must focus on the mechanisms of influence of our gut flora.influence of our gut flora.
Studies must be placebo controlled and high Studies must be placebo controlled and high quality.quality.
Truly need translational science to work at the Truly need translational science to work at the levels of the petri dish, genomics, and clinical levels of the petri dish, genomics, and clinical outcomes.outcomes.
Much more to come!Much more to come!

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
GI Update: SummaryGI Update: Summary
Longstanding dysphagia: Think EoELongstanding dysphagia: Think EoE
PPIs: Use them thoughtfullyPPIs: Use them thoughtfully
Be smart about Celiac disease: Know the testsBe smart about Celiac disease: Know the tests
Many new options for Hepatitis B and CMany new options for Hepatitis B and C
TNFs will be used more often for IBDTNFs will be used more often for IBD
Colon cancer screening: DO IT!Colon cancer screening: DO IT!
GI Update: SummaryGI Update: Summary
Stool transplants: Not ready for prime timeStool transplants: Not ready for prime time
Think SIBO with RosaceaThink SIBO with Rosacea
Pot and vomiting: Ask about hot bathsPot and vomiting: Ask about hot baths
Microbiome: research will explodeMicrobiome: research will explode
C. difficileC. difficile: the pest is here to stay: the pest is here to stay
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
QuestionsQuestions
Break TimeBreak Time
THE CALLTHE CALL

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
First Rule: Never go to “check” a puppy out
The Visit
Review of Bloodline

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Rule two: Never believe that parents have anything to do with the pup
Rule Three: Never bring the puppy home

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
The InfectionThe Infection

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
The DecisionThe Decision

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
Probiotics and Probiotics and C. DifficileC. Difficile
124 Adults with 124 Adults with C difficile C difficile (Rand, PC)(Rand, PC) 64 164 1stst episode, 60 recurrent CDADepisode, 60 recurrent CDAD
Standard Ab with Standard Ab with S. boulardii S. boulardii or PBO or PBO
Outcome: Recurrence of CDADOutcome: Recurrence of CDAD 11stst Episode: 19.3% vs 24.2% (P=.86)Episode: 19.3% vs 24.2% (P=.86)
Rec CDAD: 34.6% vs 64.7% (P=.04)Rec CDAD: 34.6% vs 64.7% (P=.04)
S. boulardii S. boulardii reduces risk for recurrence in subjects reduces risk for recurrence in subjects with recurrent with recurrent C difficileC difficile
McFarland, et al. JAMA 1994;271:1913-8
Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
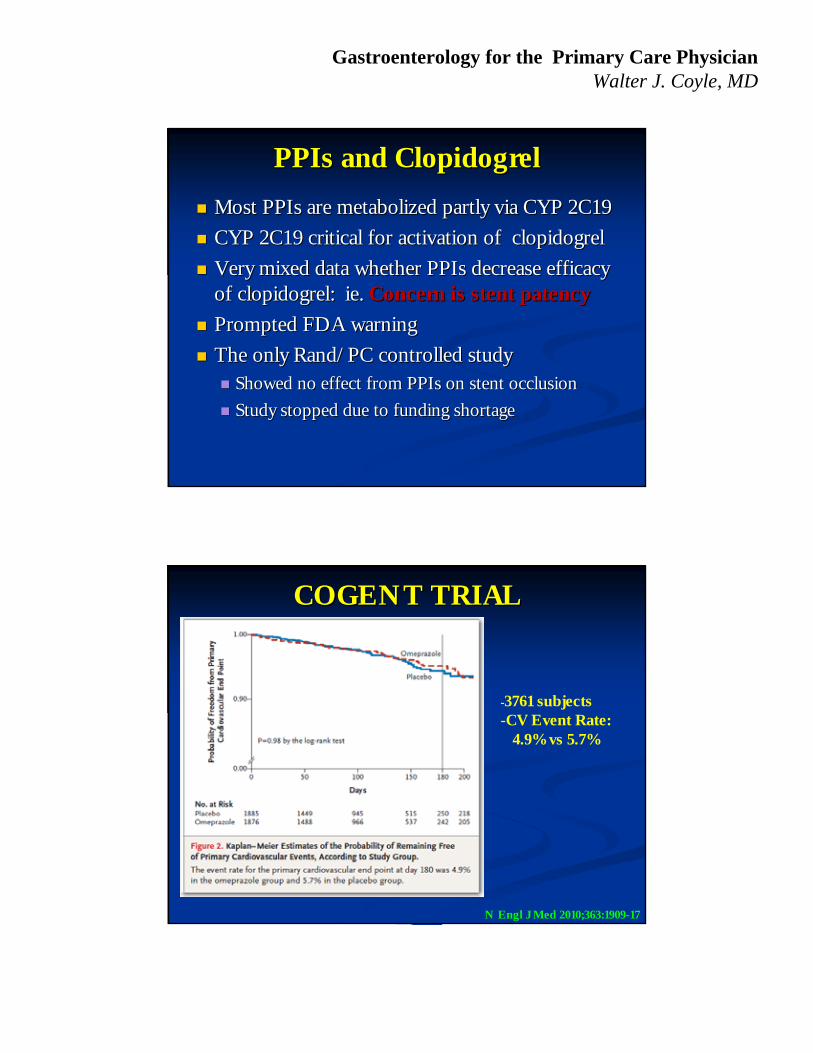
PPIs and ClopidogrelPPIs and Clopidogrel
Most PPIs are metabolized partly via CYP 2C19Most PPIs are metabolized partly via CYP 2C19
CYP 2C19 critical for activation of clopidogrelCYP 2C19 critical for activation of clopidogrel
Very mixed data whether PPIs decrease efficacy Very mixed data whether PPIs decrease efficacy of clopidogrel: ie. of clopidogrel: ie. Concern is stent patencyConcern is stent patency
Prompted FDA warningPrompted FDA warning
The only Rand/PC controlled studyThe only Rand/PC controlled study Showed no effect from PPIs on stent occlusionShowed no effect from PPIs on stent occlusion
Study stopped due to funding shortageStudy stopped due to funding shortage
COGENT TRIALCOGENT TRIAL
N Engl J Med 2010;363:1909-17
-3761 subjects-CV Event Rate:
4.9% vs 5.7%

Gastroenterology for the Primary Care Physician Walter J. Coyle, MD
COGENT TRIALCOGENT TRIAL
N Engl J Med 2010;363:1909-17
-3761 subjects-GI event rate:1.1% vs 2.9%
COGENT TrialCOGENT Trial
End point Placebo, n PPI, n p
All CV events 67 69 NS
MI 37 36 NS
Revascularization 67 69 NS
GI events 67 38 0.007
COGENT event ratesCOGENT event rates
Bhatt D. TCT 2009; Sept 24, 2009; San Francisco, CA.







