

Update on Reproductive Update on Reproductive SurgerySurgery
Prof T C LIProf T C LIProfessor of Reproductive Medicine & SurgeryProfessor of Reproductive Medicine & Surgery
Sheffield, EnglandSheffield, England
Shenzhen, May 2013
Areas to be coveredAreas to be covered
Management of distal tubal diseaseManagement of distal tubal disease
Ovarian surgery revisitedOvarian surgery revisited
Haemostatic agent Haemostatic agent

Management of distal tubal Management of distal tubal diseasedisease
Salpingostomy
Salpingectomy
IVF?
Management of distal tubal Management of distal tubal diseasedisease
Salpingostomy
Salpingectomy
IVF?
Answer: it depends
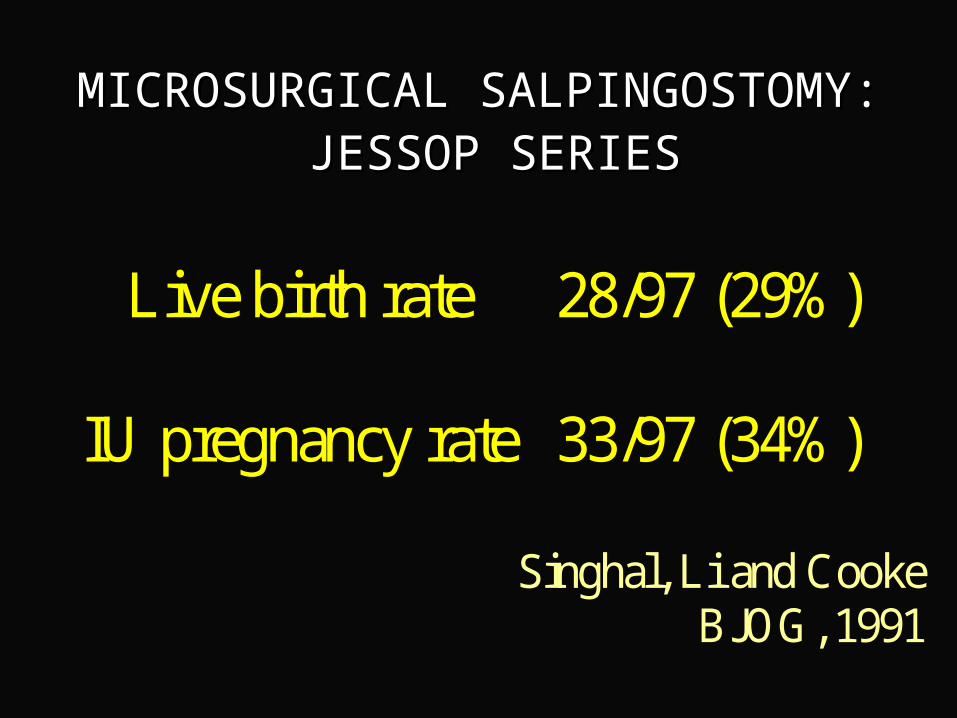
MICROSURGICAL SALPINGOSTOMY:MICROSURGICAL SALPINGOSTOMY: JESSOP SERIESJESSOP SERIES
Live birth rate
28/97 (29%)
IU pregnancy rate
33/97 (34%)
Singhal, Li and Cooke
BJOG, 1991

MICROSURGICAL SALPINGOSTOMY
Tubal score Term pregnancy
Stage I 22/56 (39%)
Stage II 20/99 (20%)
Stage III/IV 6/75 (8%)
Winston and Magara BJOG 1991
SALPINGOSTOMY: SALPINGOSTOMY: GOOD PROGNOSTIC GOOD PROGNOSTIC
FEATURESFEATURES
small hydrosalpinxsmall hydrosalpinx
no/minimal peri-tubal adhesionsno/minimal peri-tubal adhesions
normal mucosanormal mucosa
normal/thin wallnormal/thin wall
partial occlusionpartial occlusion
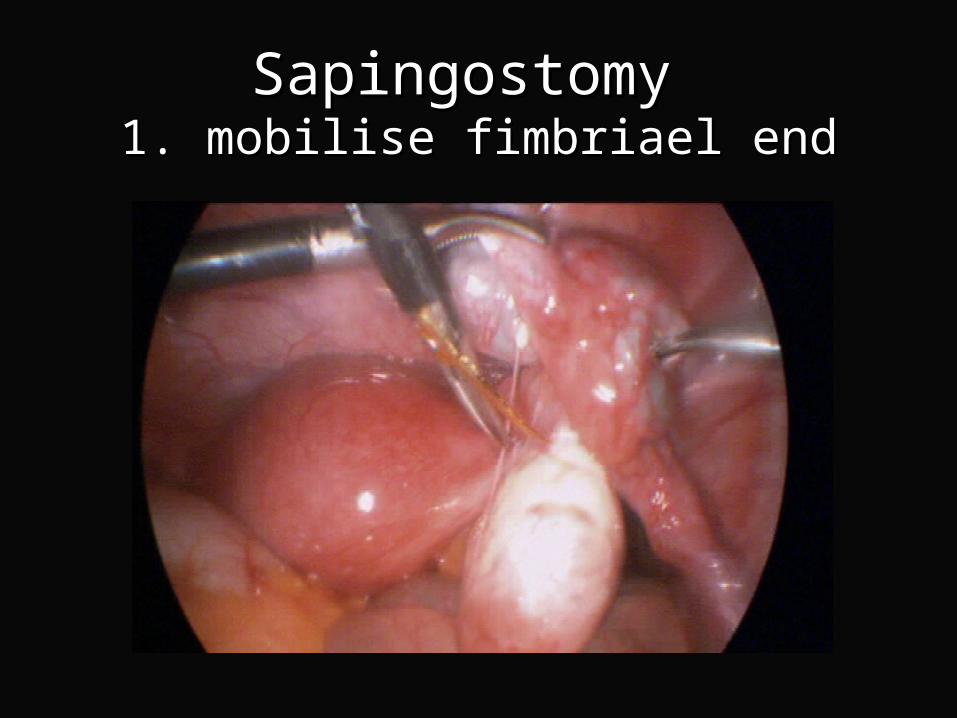
Sapingostomy Sapingostomy 1. mobilise fimbriael end1. mobilise fimbriael end

Sapingostomy Sapingostomy 1. mobilise fimbriael end1. mobilise fimbriael end

Sapingostomy Sapingostomy 1. mobilise fimbriael end1. mobilise fimbriael end

Sapingostomy Sapingostomy 2.locate blocked ostium2.locate blocked ostium

Sapingostomy Sapingostomy 3. incise blocked ostium 3. incise blocked ostium

Sapingostomy Sapingostomy 4. inspect lumen 4. inspect lumen
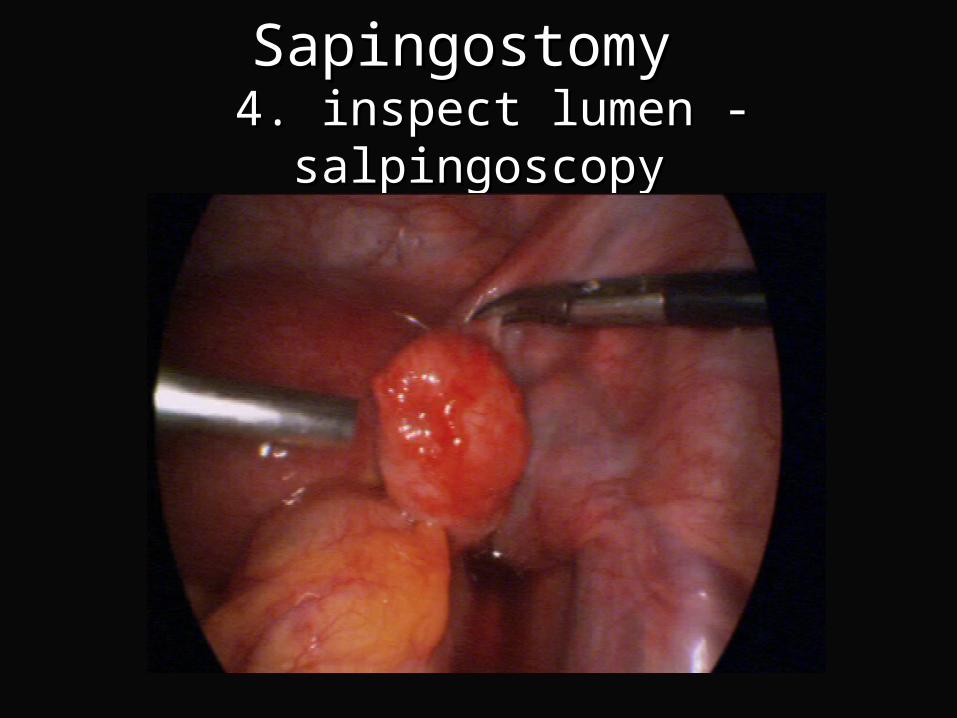
Sapingostomy Sapingostomy 4. inspect lumen - salpingoscopy 4. inspect lumen - salpingoscopy
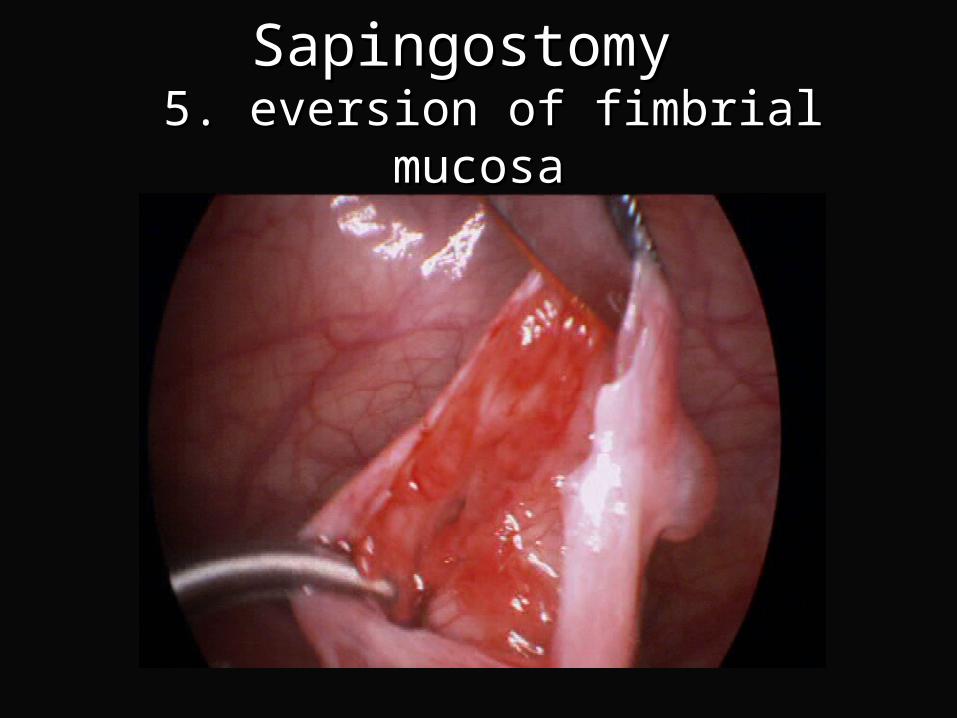
Sapingostomy Sapingostomy 5. eversion of fimbrial mucosa 5. eversion of fimbrial mucosa

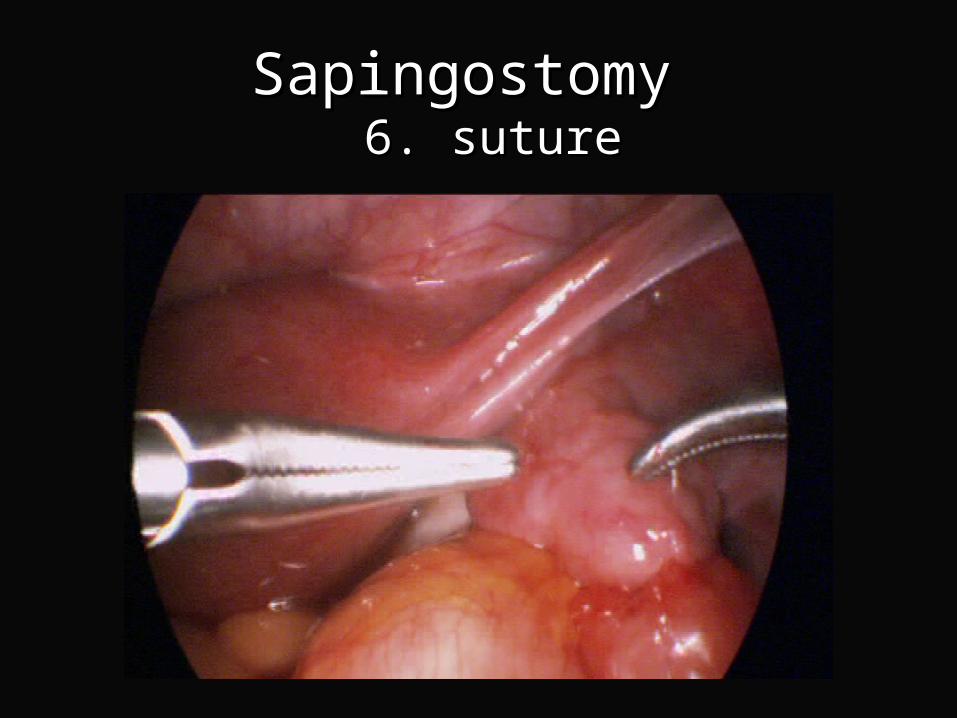
Sapingostomy Sapingostomy 6. suture 6. suture
Sapingostomy Sapingostomy 6. suture 6. suture

MICROSURGICAL SALPINGOSTOMY
Tubal score Term pregnancy
Stage I 22/56 (39%)
Stage II 20/99 (20%)
Stage III/IV 6/75 (8%)
Winston and Magara BJOG 1991
Salpingoscopy Salpingoscopy Abnormal MucosaAbnormal Mucosa

Management of distal tubal Management of distal tubal diseasedisease
Salpingostomy
Salpingectomy
IVF?

Hydrosalpinges and IVFHydrosalpinges and IVF
The live birth rate of patients with The live birth rate of patients with hydrosalpinges undergoing IVF is hydrosalpinges undergoing IVF is only one-half that of women who do only one-half that of women who do not have hydrosalpinges not have hydrosalpinges
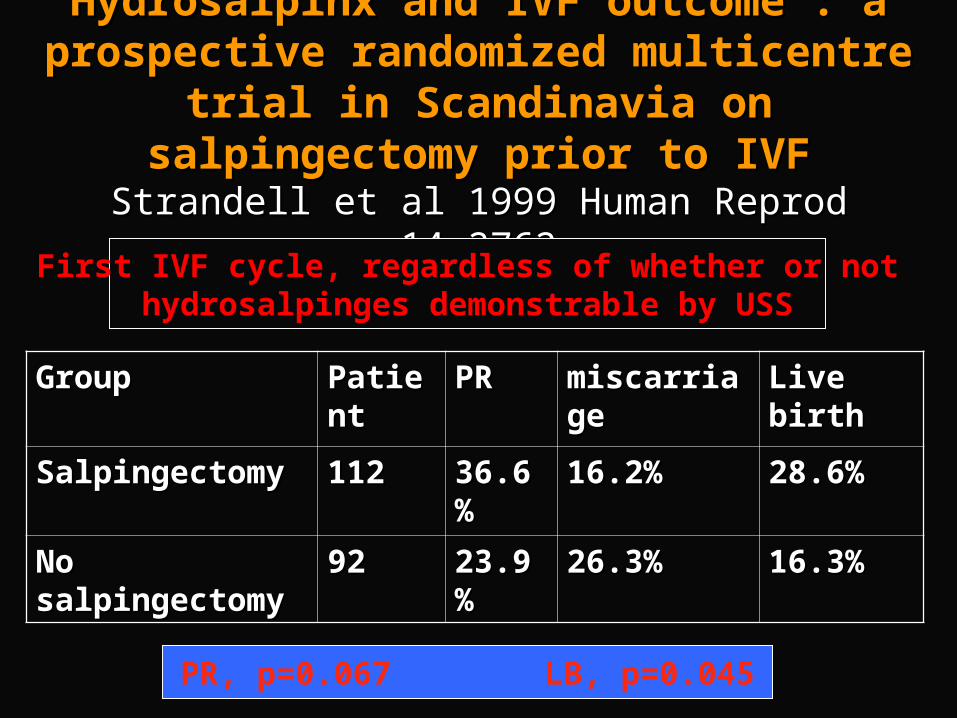
Hydrosalpinx and IVF outcome : a Hydrosalpinx and IVF outcome : a prospective randomized multicentre trial in prospective randomized multicentre trial in Scandinavia on salpingectomy prior to IVFScandinavia on salpingectomy prior to IVF
Strandell et al 1999 Human Reprod 14:2762Strandell et al 1999 Human Reprod 14:2762
GroupGroup PatientPatient PR PR miscarriagemiscarriage Live birthLive birth
SalpingectomySalpingectomy 112112 36.6%36.6% 16.2%16.2% 28.6%28.6%
No No salpingectomysalpingectomy
9292 23.9%23.9% 26.3%26.3% 16.3%16.3%
First IVF cycle, regardless of whether or nothydrosalpinges demonstrable by USS
PR, p=0.067 LB, p=0.045
Hydrosalpinges and IVFHydrosalpinges and IVF
Salpingectomy prior to IVF in women Salpingectomy prior to IVF in women with hydrosalpinges improves with hydrosalpinges improves pregnancy, implantation and live birth pregnancy, implantation and live birth rates rates
1. Is it 1. Is it cost-effective to to routinely remove routinely remove
all hydrosalpinges all hydrosalpinges prior to IVF ?prior to IVF ?
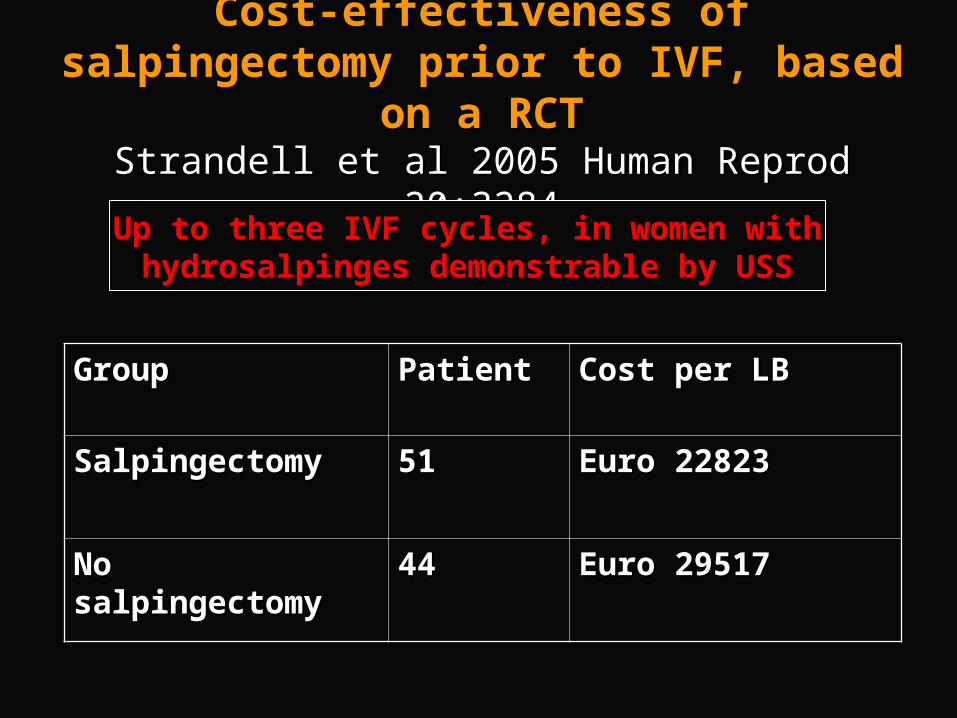
Cost-effectiveness of salpingectomy prior Cost-effectiveness of salpingectomy prior to IVF, based on a RCTto IVF, based on a RCT
Strandell et al 2005 Human Reprod 20:3284Strandell et al 2005 Human Reprod 20:3284
GroupGroup PatientPatient Cost per LBCost per LB
SalpingectomySalpingectomy 5151 Euro 22823Euro 22823
No salpingectomyNo salpingectomy 4444 Euro 29517Euro 29517
Up to three IVF cycles, in women withhydrosalpinges demonstrable by USS
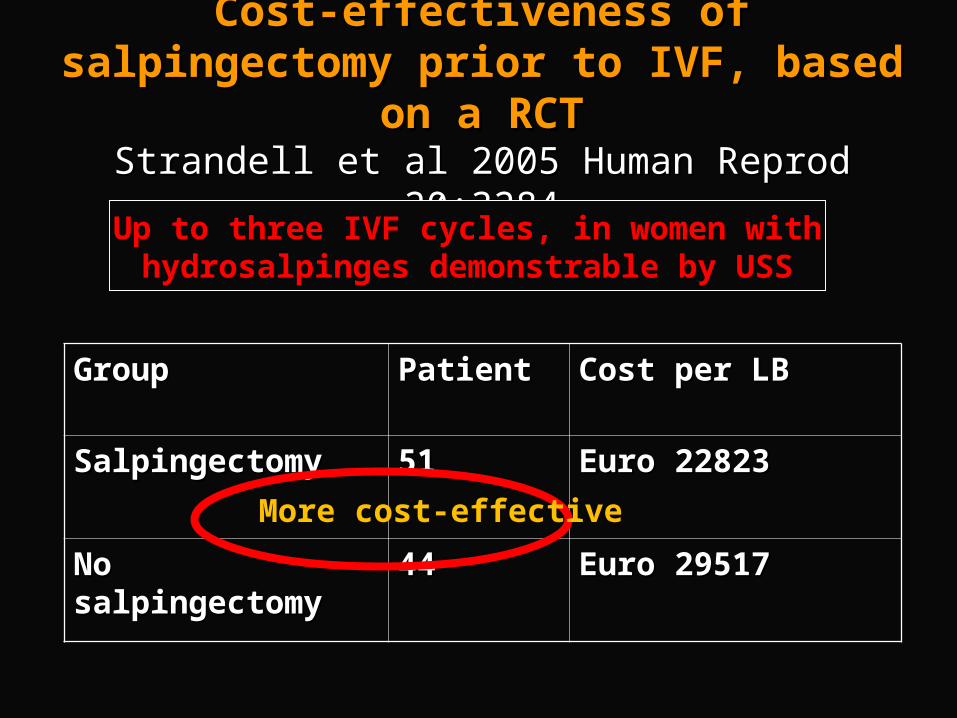
Cost-effectiveness of salpingectomy prior Cost-effectiveness of salpingectomy prior to IVF, based on a RCTto IVF, based on a RCT
Strandell et al 2005 Human Reprod 20:3284Strandell et al 2005 Human Reprod 20:3284
GroupGroup PatientPatient Cost per LBCost per LB
SalpingectomySalpingectomy 5151 Euro 22823Euro 22823
No salpingectomyNo salpingectomy 4444 Euro 29517Euro 29517
Up to three IVF cycles, in women withhydrosalpinges demonstrable by USS
More cost-effective
1. Is it 1. Is it cost-effective to to routinely remove routinely remove
all hydrosalpinges all hydrosalpinges prior to IVF ?prior to IVF ?
YesYes
2. Should proximal tubal 2. Should proximal tubal occlusion replace occlusion replace salpingectomy?salpingectomy?

Complications of salpingectomyComplications of salpingectomy
Impairment of ovarian blood supply, Impairment of ovarian blood supply, leading to reduced ovarian response to leading to reduced ovarian response to ovarian stimulation in IVFovarian stimulation in IVF
Bowel injuryBowel injury
A case of salpingectomyA case of salpingectomy
Large hydrosalpinx visible on ultrasoundLarge hydrosalpinx visible on ultrasound
One failed IVF treatmentOne failed IVF treatment
Laparoscopic surgery Laparoscopic surgery
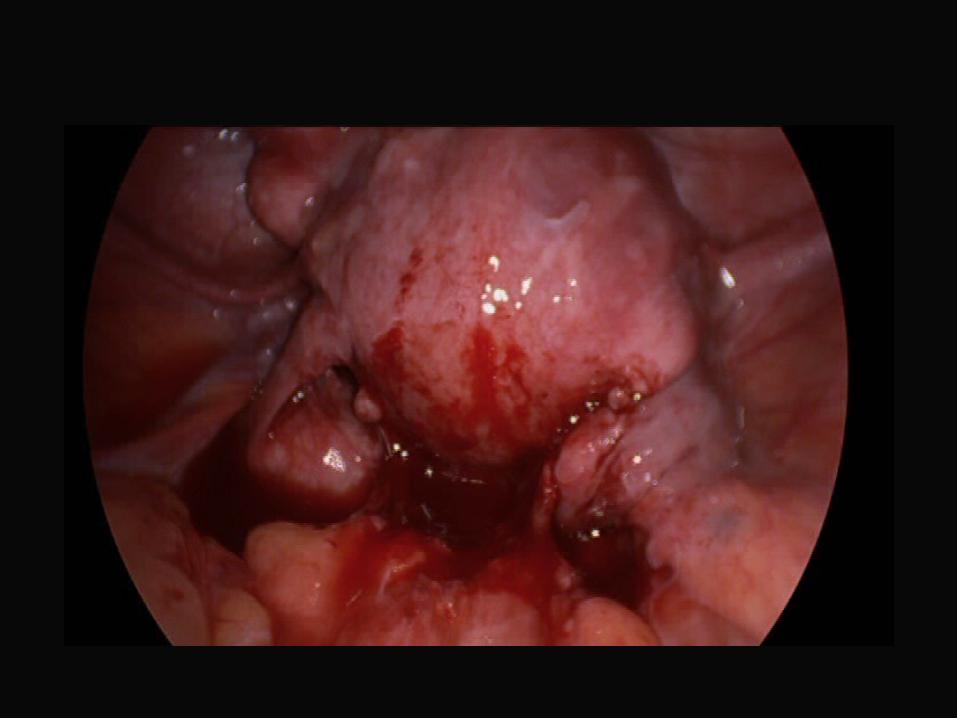
Dense adhesions between L tube and Dense adhesions between L tube and bowel and pelvic side wallbowel and pelvic side wall
2 hour operation, salpingectomy2 hour operation, salpingectomy
Day 3, sepsis, bowel leakDay 3, sepsis, bowel leak
Colostomy, ITU for 1 weeksColostomy, ITU for 1 weeks

Complications of salpingectomyComplications of salpingectomy
Impairment of ovarian blood supply, Impairment of ovarian blood supply, leading to reduced ovarian response to leading to reduced ovarian response to ovarian stimulation in IVFovarian stimulation in IVF
Bowel injuryBowel injury
More likely if there were severe adhesions

Disadvantages of proximal tubal Disadvantages of proximal tubal occlusionocclusion
Pain may get worsePain may get worseRisk of recurrent infection and pyosalpinx Risk of recurrent infection and pyosalpinx May require further surgery to remove the May require further surgery to remove the diseased tube at a later datediseased tube at a later dateThe data on possible benefit is not as robust The data on possible benefit is not as robust as that of salpingectomyas that of salpingectomy
2. Should proximal tubal 2. Should proximal tubal occlusion replace occlusion replace salpingectomy?salpingectomy?
Only if there are severe adhesions
3. Should hysteroscopic tubal 3. Should hysteroscopic tubal occlusion replace occlusion replace salpingectomy?salpingectomy?
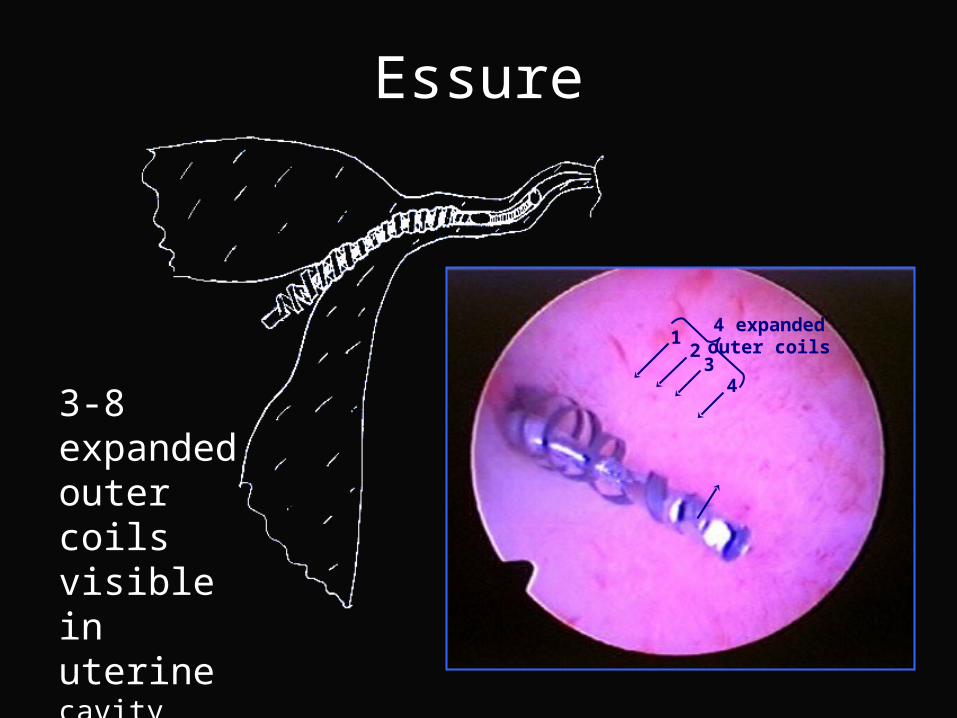
Essure
3-8 expanded outer coils visible in uterinecavity
43
21
4 expandedouter coils
3. Should hysteroscopic tubal 3. Should hysteroscopic tubal occlusion replace occlusion replace salpingectomy?salpingectomy?
No, there are concerns about implantation and premature
labour

4. Is aspiration of 4. Is aspiration of hydrosalpinges fluid as effective hydrosalpinges fluid as effective
as salpingectomy?as salpingectomy?

Ultrasound-guided hydrosalpinx aspiration, RCT
Hammadien et al, Human Reprod 2008 Hammadien et al, Human Reprod 2008
Aspiration No aspiration
P value
Biochemical pregnancy
14/32 (43.8%)
7/34 (20.6%)
0.04
Clinical pregnancy
10/32 (31.3%)
6/34 (17.6%)
0.2
4. Is aspiration of 4. Is aspiration of hydrosalpinges fluid as effective hydrosalpinges fluid as effective
as salpingectomy?as salpingectomy?
No No

5. 5. If the hydrosalpinx is small and If the hydrosalpinx is small and not visible on ultrasound, is it still not visible on ultrasound, is it still
necessary to perform necessary to perform salpingectomy?salpingectomy?

Hydrosalpinx and IVF outcome : a Hydrosalpinx and IVF outcome : a prospective randomized multicentre trial in prospective randomized multicentre trial in Scandinavia on salpingectomy prior to IVFScandinavia on salpingectomy prior to IVF
Strandell et al 1999 Human Reprod 14:2762Strandell et al 1999 Human Reprod 14:2762
GroupGroup PatientPatient PR PR miscarriagemiscarriage Live birthLive birth
SalpingectomySalpingectomy 112112 36.6%36.6% 16.2%16.2% 28.6%28.6%
No No salpingectomysalpingectomy
9292 23.9%23.9% 26.3%26.3% 16.3%16.3%
First IVF cycle, regardless of whether or nothydrosalpinges demonstrable by USS
PR, p=0.067 LB, p=0.045
5. 5. If the hydrosalpinx is small and If the hydrosalpinx is small and not visible on ultrasound, is it still not visible on ultrasound, is it still
necessary to perform necessary to perform salpingectomy?salpingectomy?
YesYes
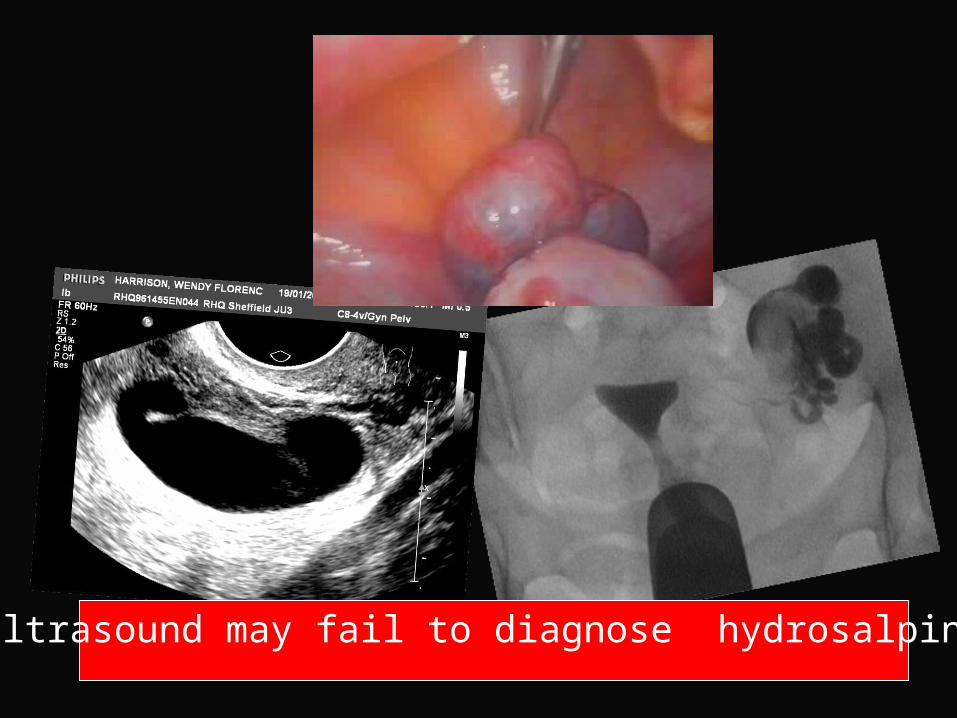
Ultrasound may fail to diagnose hydrosalpinx

6. 6. UNILATERAL TUBAL UNILATERAL TUBAL DISEASEDISEASE
Is surgery still worthwhile?Is surgery still worthwhile?
Unilateral Hydrosalpinx with a Contra-lateral Patent Tube
McComb & Taylor 2001 Fertil Steril 76:1279 McComb & Taylor 2001 Fertil Steril 76:1279
23 women with unilateral hydrosalpinx 23 women with unilateral hydrosalpinx underwent salpingostomyunderwent salpingostomy
IU pregnancy rate 43.5%IU pregnancy rate 43.5%
Conclusion – unilateral salpingostomy in Conclusion – unilateral salpingostomy in women with a contra-lateral patent tube women with a contra-lateral patent tube improves fertilityimproves fertility

Case HistoryCase History33 year old woman33 year old woman
one one miscarriagemiscarriage at 7 weeks at 7 weeks
Infertility for 15 monthsInfertility for 15 months
Conceived spontaneously, but Conceived spontaneously, but miscarriedmiscarried again at 8 week gestationagain at 8 week gestation
Investigation – L tube normal. R hydrosalpinx, Investigation – L tube normal. R hydrosalpinx, grossly dilated, intraluminal adhesions, grossly dilated, intraluminal adhesions, salpingectomy. salpingectomy.
Three months later, spontaneouslyThree months later, spontaneously conception, conception, term deliveryterm delivery

6. 6. UNILATERAL TUBAL UNILATERAL TUBAL DISEASEDISEASE
Is surgery still worthwhile?Is surgery still worthwhile?
YesYes

77. How to do salpingectomy . How to do salpingectomy properly?properly?
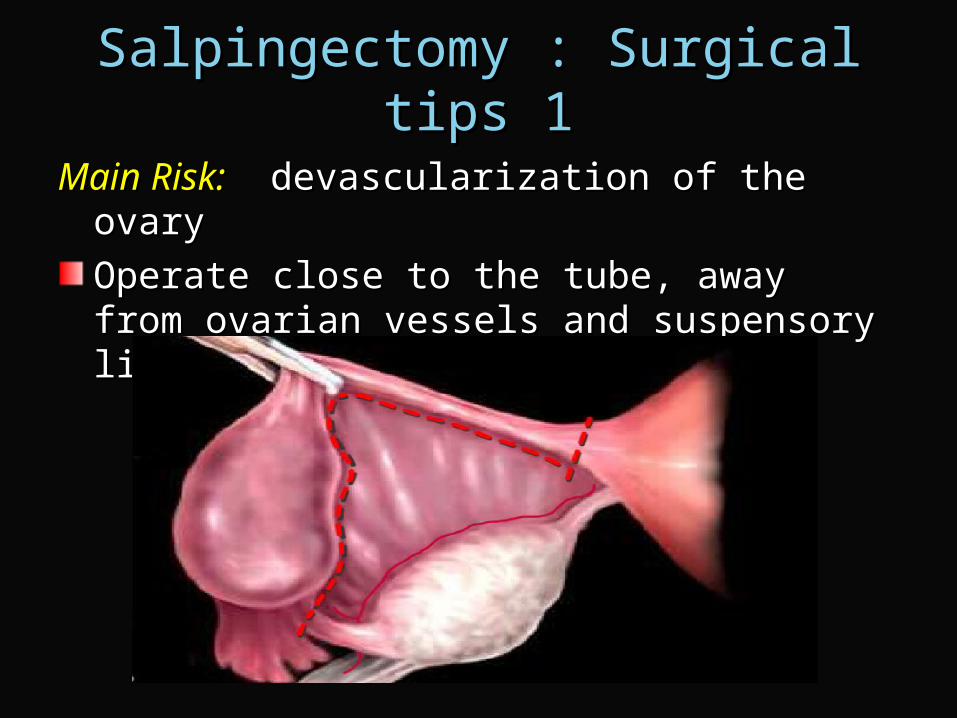
Salpingectomy : Surgical tips 1Salpingectomy : Surgical tips 1
Main Risk:Main Risk: devascularization of the ovary devascularization of the ovary
Operate close to the tube, away from ovarian Operate close to the tube, away from ovarian vessels and suspensory ligamentvessels and suspensory ligament


Salpingectomy : surgical tips 2 Salpingectomy : surgical tips 2
Other Risk:Other Risk: incomplete removal, with development incomplete removal, with development of ectopic pregnancy following ARTof ectopic pregnancy following ART
Do a complete salpingectomy !Do a complete salpingectomy !

Areas to be coveredAreas to be covered
Management of distal tubal diseaseManagement of distal tubal disease
Ovarian diathermy for PCOSOvarian diathermy for PCOS
Haemostatic agent Haemostatic agent

PCOS & Ovarian DiathermyPCOS & Ovarian Diathermy
Why bother doing laparoscopic Why bother doing laparoscopic diathermy or drilling of the ovaries?diathermy or drilling of the ovaries?
How should it be done?How should it be done?
LOD vs GONADOTROPHINLOD vs GONADOTROPHINCOCHRANE DATABASECOCHRANE DATABASE
3 RCTS3 RCTS
Vegetti et al 1998Vegetti et al 1998
Farquhar et al 2002Farquhar et al 2002
Bayram et al 2004Bayram et al 2004
CCR 6-12 month after LOD is similar to 3-CCR 6-12 month after LOD is similar to 3-6 cycles of gonadotrophin therapy 6 cycles of gonadotrophin therapy

LOD versus FSHLOD versus FSH
Bayram et al, 2004Bayram et al, 2004
Treatment RegimenTreatment Regimen No of No of womenwomen
PregnantPregnant
(%)(%)
MiscarryMiscarry MultipleMultiple LBLB
(%)(%)
LOD strategyLOD strategy
LODLOD 83 (100)83 (100) 31 (37)31 (37) 33 -- 28 (34)28 (34)
LOD + CCLOD + CC 45 (54)45 (54) 14 (31)14 (31) 11 -- 13 (29)13 (29)
LOD + CC + FSHLOD + CC + FSH 23 (28)23 (28) 18 (78)18 (78) 33 11 12 (52)12 (52)
LOD strategy totalLOD strategy total 8383 63 (76)63 (76) 77 11 53 (64)53 (64)
FSHFSH 8585 64 (75)64 (75) 77 99 51 (60)51 (60)
Conclusions of studyConclusions of study
An electrocautery strategy and An electrocautery strategy and ovulation induction with recombinant ovulation induction with recombinant follicle stimulating hormone are follicle stimulating hormone are similarly effective in inducing ovulationsimilarly effective in inducing ovulation
Multiple pregnancies can largely be Multiple pregnancies can largely be avoided by electrocautery and avoided by electrocautery and clomifene citrate before rFSHclomifene citrate before rFSH

LOD vs GONADOTROPHINLOD vs GONADOTROPHINECONOMIC CONSIDERATIONS ECONOMIC CONSIDERATIONS LOD Gonadotrophins
Pregnancy rate
50% in 12
months
Up to 20% per
cycle Cost per maternity
~ £2000
~ £4000
Multiple pregnancy
< 2%
> 20%
Li et al 1998, BJOG
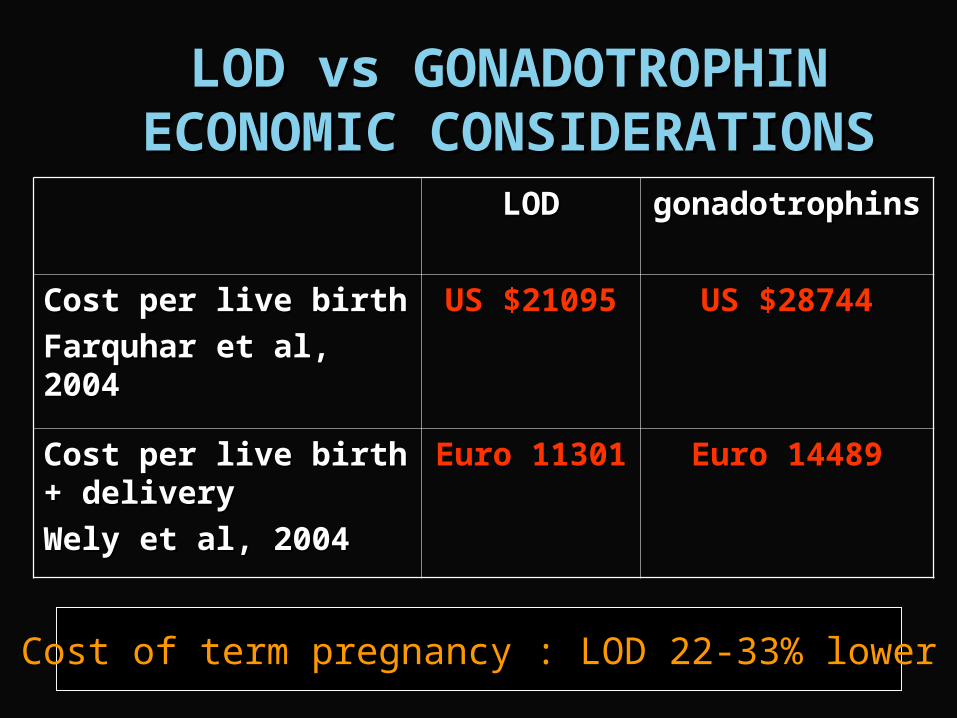
LOD vs GONADOTROPHINLOD vs GONADOTROPHINECONOMIC CONSIDERATIONSECONOMIC CONSIDERATIONS
LODLOD gonadotrophinsgonadotrophins
Cost per live birthCost per live birth
Farquhar et al, 2004Farquhar et al, 2004
US $21095US $21095 US $28744US $28744
Cost per live birth + Cost per live birth + delivery delivery
Wely et al, 2004Wely et al, 2004
Euro 11301Euro 11301 Euro 14489Euro 14489
Cost of term pregnancy : LOD 22-33% lower
NICE Guidelines NICE Guidelines
Ovarian drillingOvarian drilling
Women with PCOS who have not Women with PCOS who have not responded to CC should be offered responded to CC should be offered laparoscopic ovarian drilling because it is laparoscopic ovarian drilling because it is as effective as gonadotrophin treatment as effective as gonadotrophin treatment and is not associated with an increased and is not associated with an increased risk of multiple pregnancyrisk of multiple pregnancy

ADVANTAGES OF LODADVANTAGES OF LOD
1.1. Avoids risk of multiple pregnancyAvoids risk of multiple pregnancy
2.2. Less costlyLess costly
3.3. Long term beneficial effects including Long term beneficial effects including menstrual regularity, sustained reduction menstrual regularity, sustained reduction of FAI, sustained restoration of ovulation of FAI, sustained restoration of ovulation and further chances spontaneous and further chances spontaneous conception in over 50% of subjects conception in over 50% of subjects compared with subjects who did not compared with subjects who did not undergo LOD undergo LOD (Amer et al, Human Reprod 2002, (Amer et al, Human Reprod 2002, 17:2035; Amer et al, Human Reprod 2002, 17:2851)17:2035; Amer et al, Human Reprod 2002, 17:2851)

PCOS & Ovarian DiathermyPCOS & Ovarian Diathermy
Why bother doing laparoscopic Why bother doing laparoscopic diathermy or drilling of the ovaries?diathermy or drilling of the ovaries?
How should it be done?How should it be done?
How many punctures should How many punctures should one make?one make?
The number of puncture is only one of The number of puncture is only one of several variables which determines the several variables which determines the amount of electrical energy delivered to amount of electrical energy delivered to
the ovarythe ovary
The amount of energy (J) used is The amount of energy (J) used is calculated as: calculated as: power (w) x duration power (w) x duration
(sec) x No of punctures(sec) x No of punctures
Laparoscopic Ovarian Laparoscopic Ovarian Diathermy Diathermy
How much electrical energy How much electrical energy
is required to produce is required to produce optimal results?optimal results?

The amount thermal energy The amount thermal energy used in LODused in LOD
Gjonnaess (1984): 250 w x 3 sec x > Gjonnaess (1984): 250 w x 3 sec x > 5 5 = > 3750 joules = > 3750 joules Armar et al (1990): 40 w x 4 sec x 4 = Armar et al (1990): 40 w x 4 sec x 4 = 640 joules 640 joules Dabirashrafi (1989): Severe ovarian Dabirashrafi (1989): Severe ovarian atrophy with 8 holes x 400w x 5 sec atrophy with 8 holes x 400w x 5 sec = 16,000 Joules = 16,000 Joules

The Sheffield Prospective Dose The Sheffield Prospective Dose Finding Study Finding Study Amer, Li & Cooke, 2003Amer, Li & Cooke, 2003
30 women divided into ten groups, each group with 3 women30 women divided into ten groups, each group with 3 women
Dose in each group to be determined by the response of Dose in each group to be determined by the response of
previous groupprevious group
Energy utilised for each puncture is standardised Energy utilised for each puncture is standardised
The modified Monte Carlo Up-and-Down design
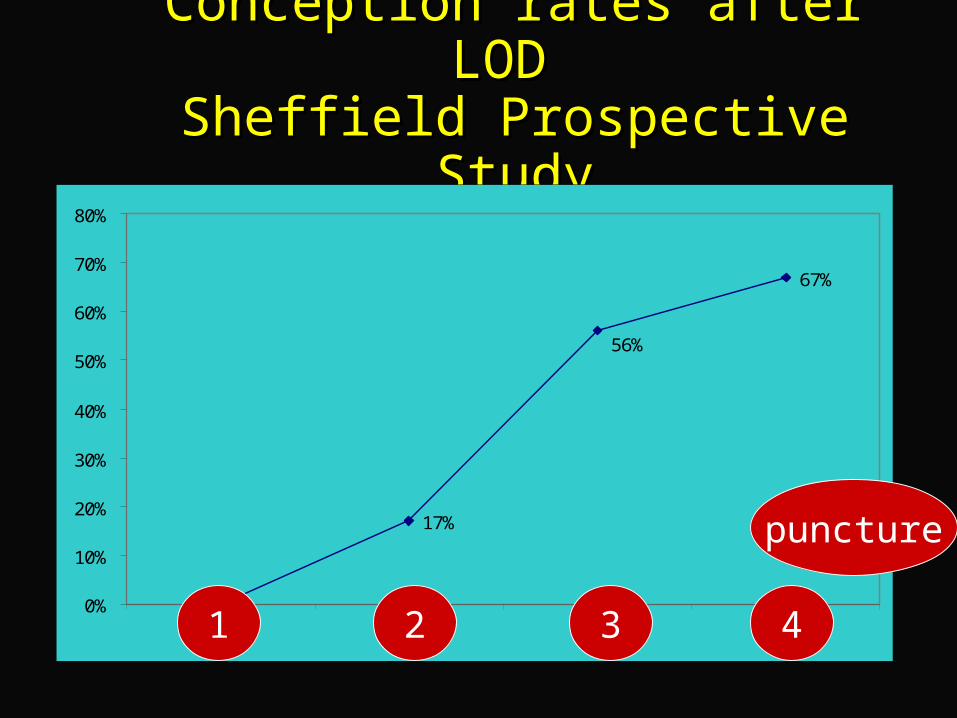
Conception rates after LOD Conception rates after LOD Sheffield Prospective StudySheffield Prospective Study
17%
67%
56%
0%
10%
20%
30%
40%
50%
60%
70%
80%
1 2 3 41
puncture
2 3 4
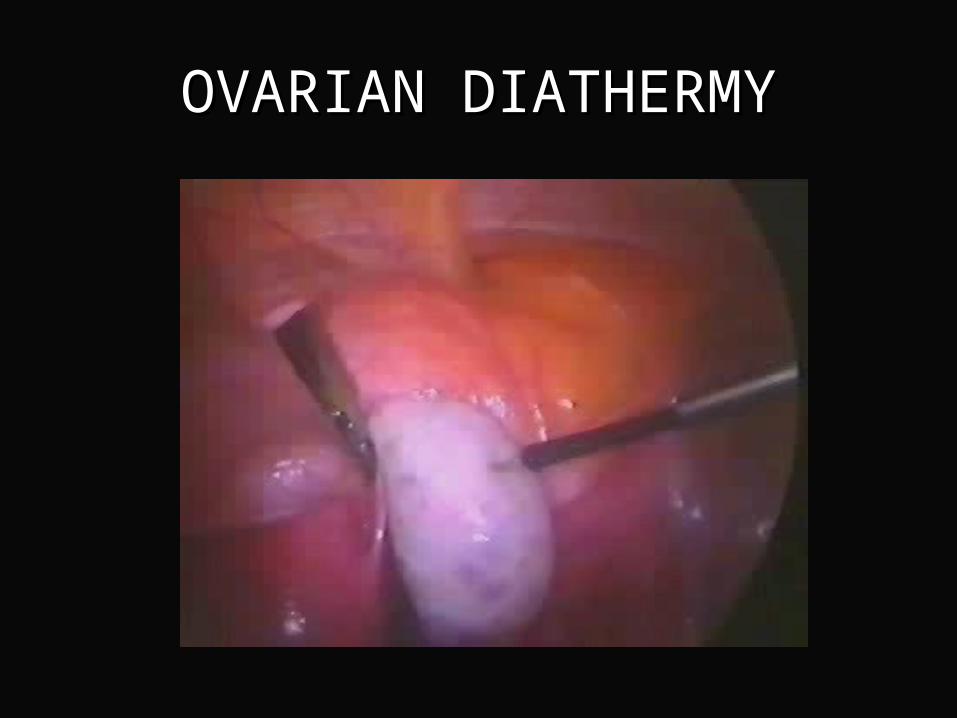
OVARIAN DIATHERMYOVARIAN DIATHERMY

ELECTRICAL ENERGYELECTRICAL ENERGY
Rockett of London diathermy needleRockett of London diathermy needle
needle 8 mm long, 2 mm diameterneedle 8 mm long, 2 mm diameter
monopolar coagulationmonopolar coagulation
power - 30 Wpower - 30 W
puncturepuncture– number 4number 4– duration 5 secondsduration 5 seconds
With the use of proper With the use of proper techniques, laparoscopic techniques, laparoscopic
ovarian diathermy is ovarian diathermy is very safevery safe
Sheffield series :Sheffield series :Adhesions – often minimalAdhesions – often minimal
ovarian failure – 0/250casesovarian failure – 0/250cases
Management of distal tubal diseaseManagement of distal tubal disease
Ovarian surgery revisitedOvarian surgery revisited
Haemostatic Agent Haemostatic Agent

Floseal Haemostatic MatrixFloseal Haemostatic Matrix(Baxter)(Baxter)
FLOSEAL is indicated in surgical FLOSEAL is indicated in surgical procedures (other than ophthalmic) as an procedures (other than ophthalmic) as an adjunct to haemostasis when control of adjunct to haemostasis when control of bleeding by ligature or conventional bleeding by ligature or conventional procedures is ineffective or impractical. procedures is ineffective or impractical.
What is Floseal?What is Floseal?
FLOSEAL provides a combination of two FLOSEAL provides a combination of two independent hemostasis promoting independent hemostasis promoting agents. agents. – The gelatin granules swell to produce a The gelatin granules swell to produce a
tamponade effecttamponade effect– High concentrations of human thrombin High concentrations of human thrombin
convert fibrinogen into fibrin monomers convert fibrinogen into fibrin monomers accelerating clot formationaccelerating clot formation
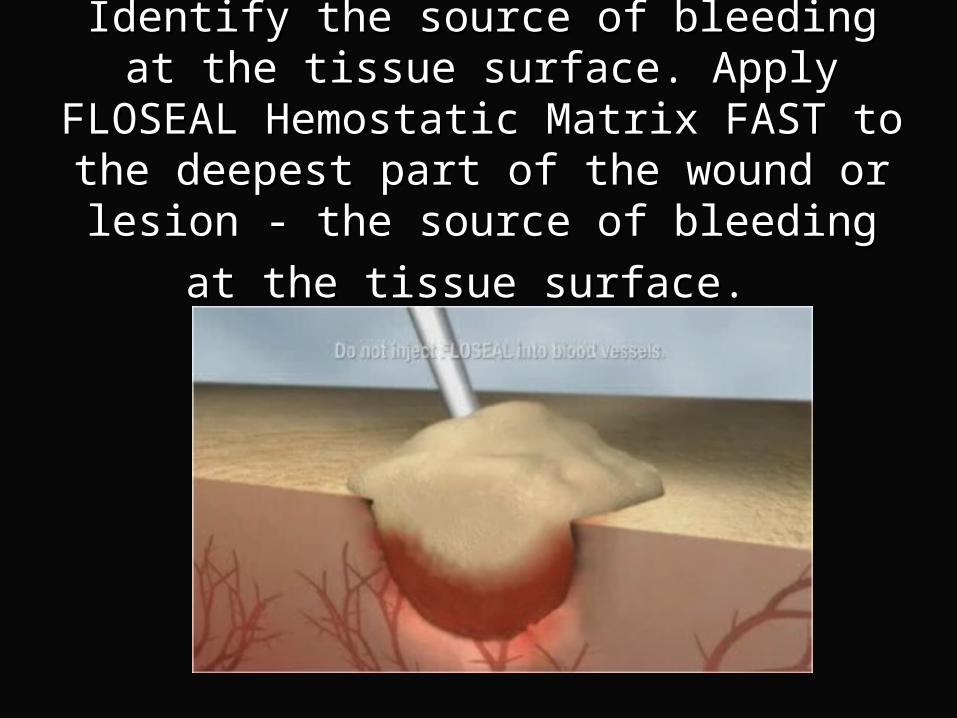
Identify the source of bleeding at the tissue Identify the source of bleeding at the tissue surface. Apply FLOSEAL Hemostatic Matrix surface. Apply FLOSEAL Hemostatic Matrix FAST to the deepest part of the wound or FAST to the deepest part of the wound or
lesion - the source of bleeding at the tissue lesion - the source of bleeding at the tissue
surface.surface.

FLOSEAL granules allow high concentrations of FLOSEAL granules allow high concentrations of thrombin to react rapidly with the patient's thrombin to react rapidly with the patient's
fibrinogen and form a mechanically stable clot.fibrinogen and form a mechanically stable clot.

FLOSEAL can be reapplied, if necessary. FLOSEAL can be reapplied, if necessary. Once haemostasis is achieved, gentle Once haemostasis is achieved, gentle irrigation should always occur to remove irrigation should always occur to remove excess product that has not been excess product that has not been incorporated into the clot. incorporated into the clot. Do not disrupt the clot by physical Do not disrupt the clot by physical manipulation or suction.manipulation or suction.
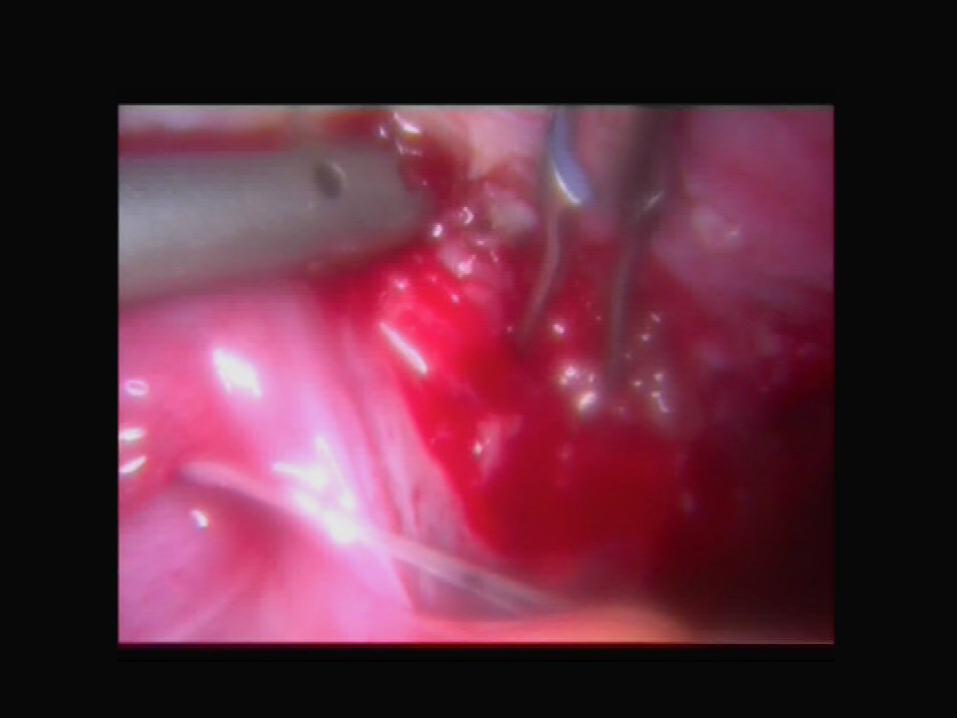
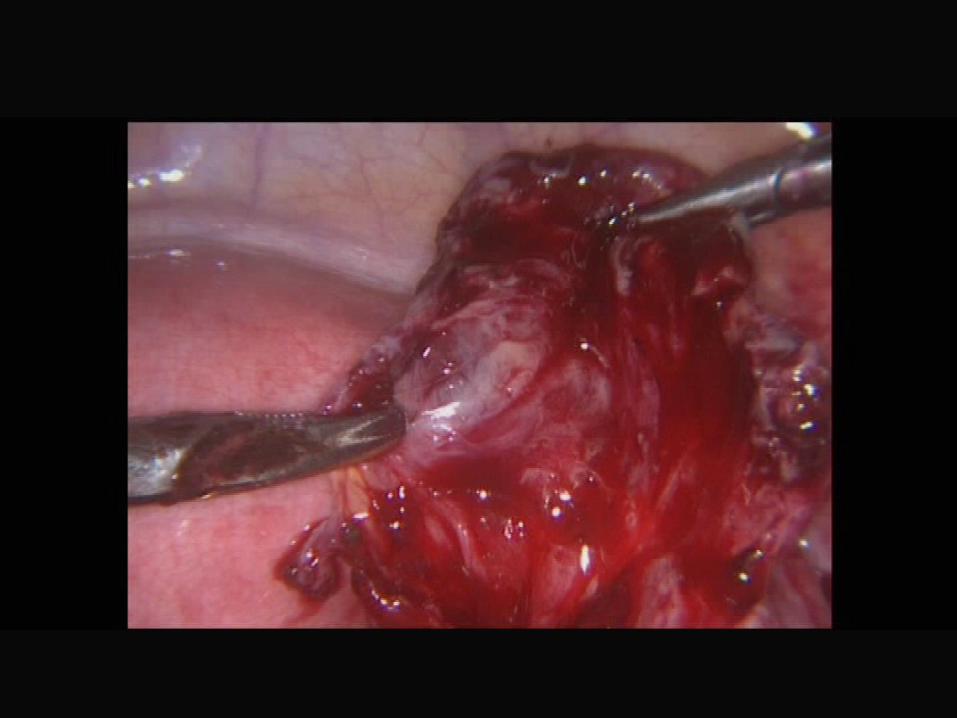
When is it useful?When is it useful?
Pelvic side wallPelvic side wall
Rectovaginal spaceRectovaginal space
Ovarian cyst wall Ovarian cyst wall
THANK YOUTHANK YOU







