

Urgent need to strengthen active tracing of lost to follow up cases: a prospective cohort study of newly diagnosed HIV clients in rural districts, Zambia
Paul Nambala1, Shinsuke Miyano2, Kenichi Komada2,3, Francis Hadunka1, Vincent Chipeta4, Kenneth Chibwe4, Albert Mwango5
1 Kazungula District Community Medical Office, Zambia2 National Center for Global Health and Medicine, Japan3 SHIMA project, JICA, Lusaka, Zambia4 Kalomo District Community Medical Office, Zambia5 Ministry of Health, Lusaka, Zambia

Background: HIV in Zambia• Zambia has a population of 13.2
million (2010)
• New infection rate in 2011 - 0.96% among males - 1.25% among females
• HIV Prevalence in adults: 14.3% (2007 ZDHS)
- Rural 10.3 % - Urban 19.7%

Kazungula and Kalomo District
• 480 & 360km south west of Lusaka (Capital city)
• Share borders with Zimbabwe, Namibia, Botswana by the Zambezi river.
• Total population: 396,390 (2013)
• Area: 30,000 km2
• The mainstay is agriculture and animal husbandly with few industry.

HIV in Kazungula/Kalomo • Adult HIV prevalence rate -13.4%.
• ART services started in a few selected health facilities in 2005 and have been scaling up.
• Number of HIV infected adults on ARVs – 8200.

Objectives
• To assess the retention among HIV testing, care and treatment.
• To evaluate active tracing for lost to follow up cases in rural districts in Zambia.

Methods• A Prospective Cohort Study
• Newly diagnosed HIV clients from April 2012 to March 2013 in 8 health facilities in Kazungula and Kalomo has been enrolled.
• The data have been collected through clients’ records and interviews
• Assessed at June 2013
• The retention rates were estimated by Kaplan-Meier method
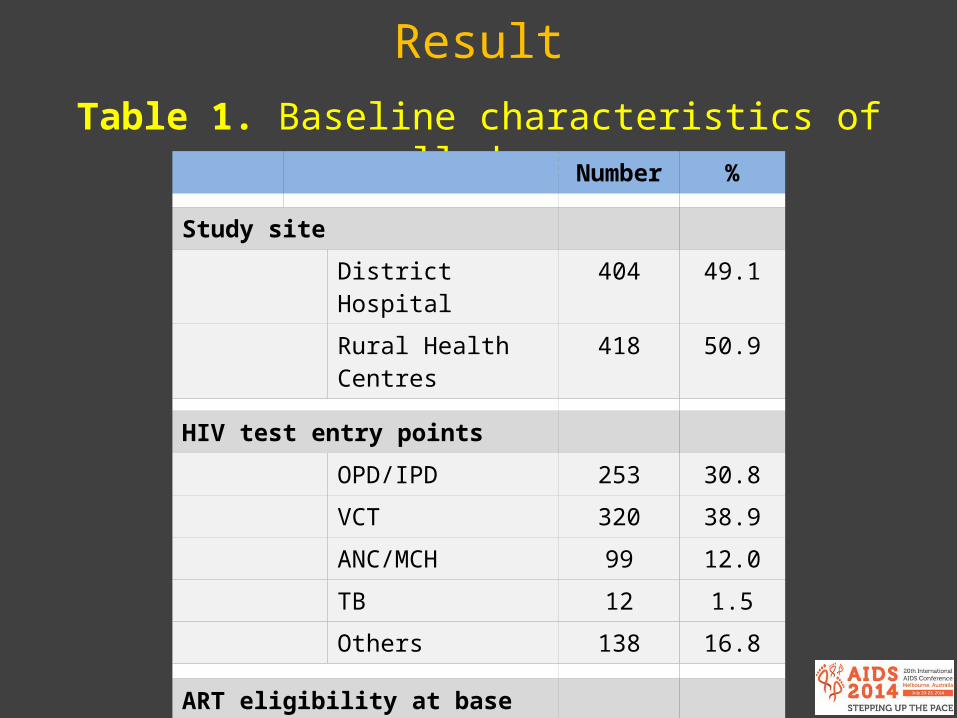
ResultTable 1. Baseline characteristics of enrolled cases
Number %
Study site
District Hospital 404 49.1
Rural Health Centres 418 50.9
HIV test entry points
OPD/IPD 253 30.8
VCT 320 38.9
ANC/MCH 99 12.0
TB 12 1.5
Others 138 16.8
ART eligibility at base line
Eligible (ART) 414 63.3
Not eligible (Pre-ART) 240 36.7

Number %
Gender
Male 309 41.1
Female 442 58.9
WHO stage
Stage Ⅰ 422 65.8
Stage Ⅱ 127 19.8
Stage Ⅲ 86 13.4
Stage Ⅳ 6 1.0
Discordant couples
Known as discordant 69 8.4
Median IQR
Age (years) 33 26 - 40
CD4 cell count (cells/mm3) 286 158 - 444
Table 1. Baseline characteristics of enrolled cases (cont’d)

Result
Figure 1. Continuum of HIV care in enrolled cases
Pre-ART240 clients
(36.7%)
ART 414 clients
(63.3%)
No access to HIV care168 / 822 clients
(20.4%)
LTFU at 12 months139 / 654 clients
(21.3%)
HIV Positive
Total 822 clients
OPD/IPD 253
VCT 320
ANC/MCH 99
TB 12
Others 138
Enrolled in HIV CareTotal 654 clients (79.6%)
OPD/IPD 221 (87.4%)
VCT 266 (83.1%)
ANC/MCH 74 (74.7%)
TB 12 (100%)
Others 81 (58.7%)

Result
Figure 2. Pre-ART and ART retention rate (Kaplan-Meier estimates)
12 months retentionART 75.4% Pre-ART 75.9%

Result
Figure 3. The LTFU cases traced by phone
Lost to Follow up at 12 months n = 139
Have phone number 53 / 139 ( 38.1%)
No phone number 86 / 139 ( 61.9%)

Figure 3. The LTFU cases traced by phone
Lost to Follow up at 12 months n = 139
Have phone number 53 / 139 ( 38.1%)
No phone number 86 / 139 ( 61.9%)
Reachable to Clients17 / 53 (32.1%)
Not Reachable14 / 53 (26.4%)
Invalid/Wrong number22 / 53 (41.5%)
Result

Figure 3. The LTFU cases traced by phone
Lost to Follow up at 12 months n = 139
Have phone number 53 / 139 ( 38.1%)
No phone number 86 / 139 ( 61.9%)
Reachable to Clients17 / 53 (32.1%)
Not Reachable14 / 53 (26.4%)
Invalid/Wrong number22 / 53 (41.5%)
Returned to the original facility3 / 17 (17.6%)
Self transfer out to other facility
4 / 17 (23.5%)
Not returned on the care
10 /17 (58.9%)
Result

Figure 3. The LTFU cases traced by phone
Lost to Follow up at 12 months n = 139
Have phone number 53 / 139 ( 38.1%)
No phone number 86 / 139 ( 61.9%)
Reachable to Clients17 / 53 (32.1%)
Not Reachable14 / 53 (26.4%)
Invalid/Wrong number22 / 53 (41.5%)
Returned to the original facility3 / 17 (17.6%)
Self transfer out to other facility
4 / 17 (23.5%)
Not returned on the care
10 /17 (58.9%)
122 / 139 (87.8%) needphysical follow-up
Result

Discussions (1)• The reasons for Many LTFU cases were maybe; - long distances to access ART services. - bad road condition in the rainy season. - not enough attention by staff and supporters. - still have some stigma among HIV clients. - many seasonal migrants (fishermen) in some sites.
• The linkage between diagnosis and care should be strengthened.
• There is need to conduct adequate counseling soon after HIV diagnosis

Discussions (2)• Tracing LTFU case by phone is not feasible in rural area of
Zambia because, - most clients do not have Mobile phones - some clients give wrong phone numbers - poor accessibility of phone networks in rural area
• Adherence counseling at every visit and physical tracing should be strengthened.
• Need to consider how to motivate treatment supporters.

Conclusions
• Despite having successful scaled up HIV services to many rural health facilities, we still have a big number of LTFU cases.
• There is urgent need to strengthen active tracing of LTFU cases.

Acknowledgement
• Our patients• Treatment supporters• District Community Medical Offices• JICA-SHIMA project• NCGM• MCDMCH- Zambia• MOH- Zambia







