

2017 CONFERENCE
Value Based Healthcare
Speakers:Dr Paul Buss Executive Medical Director/
Deputy CEO, Aneurin Bevan UHBDr Sally Lewis Deputy Medical Director
Aneurin Bevan UHBSir Muir Gray Chair, Health and Social Care
Digital Service
Building a value delivery-system for
health_______________________
Dr Paul Buss Executive Medical Director/Deputy CEO Aneurin Bevan University Health Board
© ABUHB VBHC
Value-Based Health Care
Organising for value across a whole system
© ABUHB VBHC

Doing the right things with resource?
Aneurin Bevan: “too many drugs are consumed in too largequantities –whilst few doctors would disagree with thisstatement the fault lies primarily with them” Note 20 Chapter5 – In Place of Fear -1952
© ABUHB VBHC

We spend a great deal of money!!
Aneurin Bevan: “the cost of looking after the visitorwho falls ill cannot amount to more than a negliblefraction of £4m – the total cost of the NHS” A free
health service – In Place of Fear -1952
© ABUHB VBHC
Clinical Responsibility and Resource
Patients help us make lower
cost clinical decisions (Prof Don
Increasing evidence - better
results at lower cost
Better outcomes often COSTS
LESS!!
Rising costs - sign of concern?
Rising unit cost per unit
outcome…..an early indicator!!George Akerlof: “when returns for goodquality accrue mainly to the entire groupthe incentive to differentiate goods on theside of better quality reduces”- “TheMarket for Lemons – An EconomistTheorists Book of Tales” -1984
© ABUHB VBHC
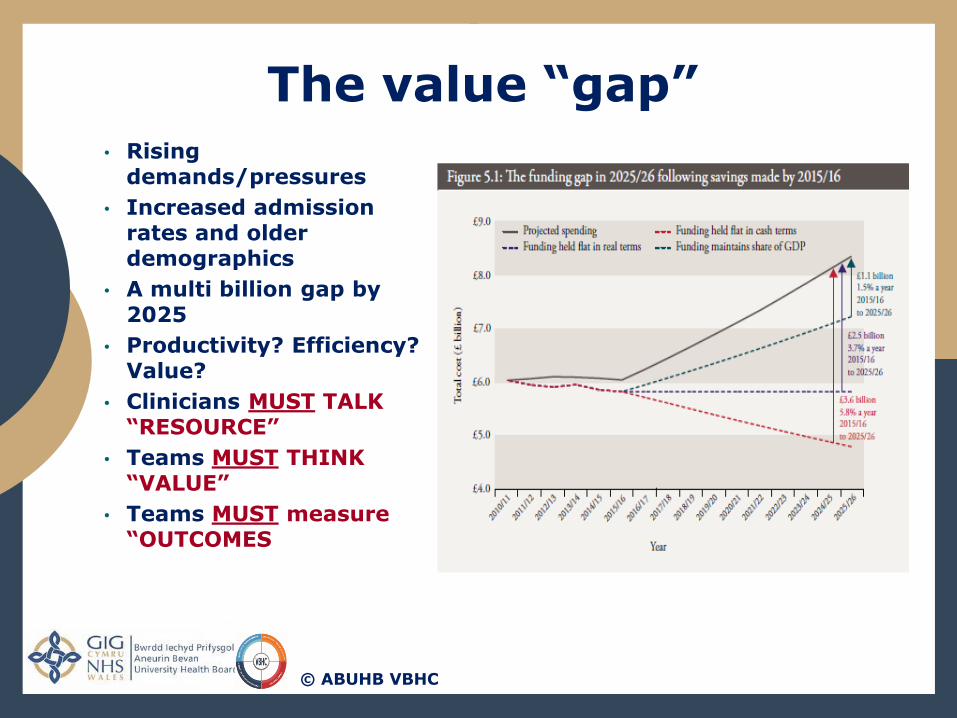
The value “gap”• Rising
demands/pressures
• Increased admission rates and older demographics
• A multi billion gap by 2025
• Productivity? Efficiency? Value?
• Clinicians MUST TALK “RESOURCE”
• Teams MUST THINK “VALUE”
• Teams MUST measure “OUTCOMES
© ABUHB VBHC

Influencing Clinical
Behaviour• Understanding the
“Porter standard”
• Actively measuring clinical outcomes
• Using International Datasets (ICHOM)
• TDABC/PLics - tools forvalue-delivery
• Clinical costs as a non-clinical marker
• Changing the culture from…………………...
Why don’t we correlate
clinical outcomes and costs routinely?
What is clinical value - what
does it mean in my practice?
To…………….…
© ABUHB VBHC

The COSTING CHALLENGE
• Costing that influences clinical behaviour
• Costs - as an economic “signal”
• Costing to close the Value Gap.
• Costing mechanism that accurately portrays clinical behaviour
Clinical decisions
Impact of clinical behaviours
ClinicalLeadership
Culture
Richard Thaler: “Prospect theory broke from the traditional theory that human behaviour can be normative and descriptive” Misbehaving – Making Behavioural Economics 2015
Do we understand our Costs?
© ABUHB VBHC
ABUHB-Strategic Partnership with ICHOM : support to
deliver our strategic outlook & vision
Scaling Implementation Support & Training inMethodology: Move towards measuring globalconsensus sets of outcomes
Supporting the provision of a Value Based Health CareCourse 04/05th October, Life Sciences Hub Cardiff.
Support delivery of Standard Set Workshops
© ABUHB VBHC
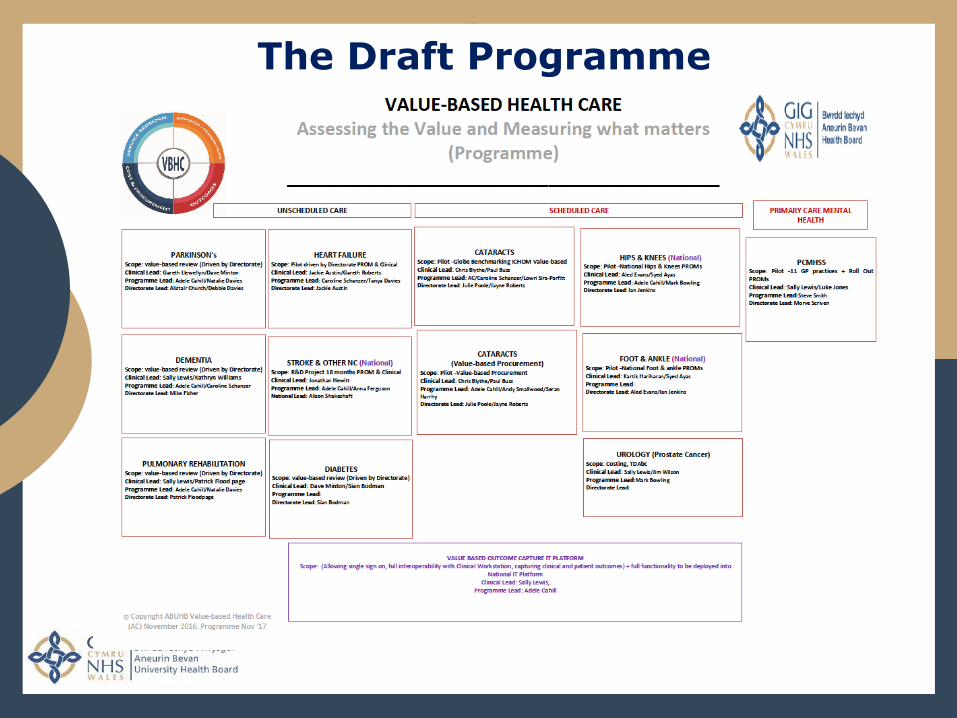
The Draft Programme

Impact of Care on QOL and Cost
Renal disease and EQ5D: Real-Life Costs of Care
0
1
2
3
4
5mobility
self care
activitiesPain
Anxiety
0102030405060708090
Nochange
Better Worse
6 months post
0
20
40
60
80
Nochange
Better Worse
6 months post
Dr Gareth Roberts clinical Business lead ABUHB
© ABUHB VBHC
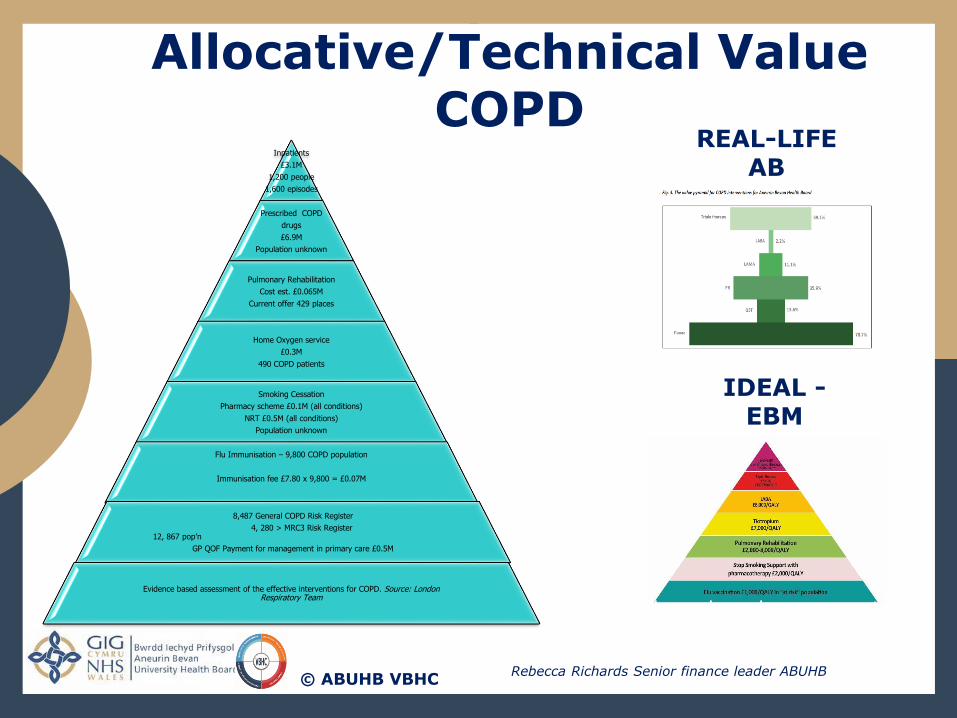
Inpatients
£3.1M
1,200 people
1,600 episodes
Prescribed COPD
drugs
£6.9M
Population unknown
Pulmonary Rehabilitation
Cost est. £0.065M
Current offer 429 places
Home Oxygen service
£0.3M
490 COPD patients
Smoking Cessation
Pharmacy scheme £0.1M (all conditions)
NRT £0.5M (all conditions)
Population unknown
Flu Immunisation – 9,800 COPD population
Immunisation fee £7.80 x 9,800 = £0.07M
8,487 General COPD Risk Register
4, 280 > MRC3 Risk Register 12, 867 pop’n
GP QOF Payment for management in primary care £0.5M
Evidence based assessment of the effective interventions for COPD. Source: London Respiratory Team
Evidence based assessment of the effective interventions for COPD. Source: London Respiratory Team
REAL-LIFE AB
Allocative/Technical Value COPD
IDEAL -EBM
Rebecca Richards Senior finance leader ABUHB© ABUHB VBHC
A blended way at ABUHB - the best of bothworlds:
• Examine and / or improve existing cost data where fit forpurpose employing PLICS
• TDABC as first choice for specific occasions or to fillpathway gaps in traditional data
To produce clinically meaningful costingdata:
• the resultant data gives a fair and useful reflection ofthe real (or improved) world
• providing the best chance of assessing value across agiven condition or pathway
© ABUHB VBHC
TDABC or Traditional Costing 4 VALUE

• Value Based Management
• Coordinated value based approach
• Clinical Cost Leadership
• Education –“importance of value”
• Clinical Value Analysis and Delivery
• Value weighting/indices for costing
Elinor Ostrom: “Local appropriators of resource have too little motivation to contribute to sustainability” – Governing the Commons
Outcome measures
Clinical Costing
ClinicalValue Analysis
The Clinical Leadership Challenge
© ABUHB VBHC
Thank you for listening: [email protected]
2017 CONFERENCE
Dr Sally LewisAssistant Medical Director
Aneurin Bevan Health Board

A Value Delivery System for Health: ‘In Practice’
Dr Sally Lewis
Assistant Medical Director
Value-Based Health Care
___________________________
Email: [email protected]
© Value Based Health Care Team; Aneurin Bevan University Health Board

Example 1: Implementing Outcomes Capture in Parkinson’s Disease (Personal Value)
Aim: Test use of standard set ICHOM
by Patient & Clinician / Understand IT solutions/
challenges NOT linked to cost TDABC at this stage
Testing methodologies and approach, i.e. process mapping
Findings/Observations:
1. Clinical Engagement is key to its success - we hadtotal buy in
2. IT Support fundamental – we had total buy in3. ICHOM expertise – required first time4. Dedicated capacity to support the work
1. The Clinical Environment2. The Clinic Flow3. Staffing4. Relationships and Awareness
•Patients entering their patient reportedoutcomes via tablet form in a clinicenvironment
•Clinicians reviewing ‘the things thatmatter to patients’ in clinic, focusing theconsultation
AT THIS STAGE THE PROGRAMME HAS
Highlighted the increasing importance ofclose collaboration between clinicians,managers, finance and fundamentally thepatients/carers/relatives in designing anddelivering healthcare in such a way thatpatients have the best possible experienceand outcomes with a high degree of VALUEin the system.
© Value Based Health Care Team; Aneurin Bevan University Health Board
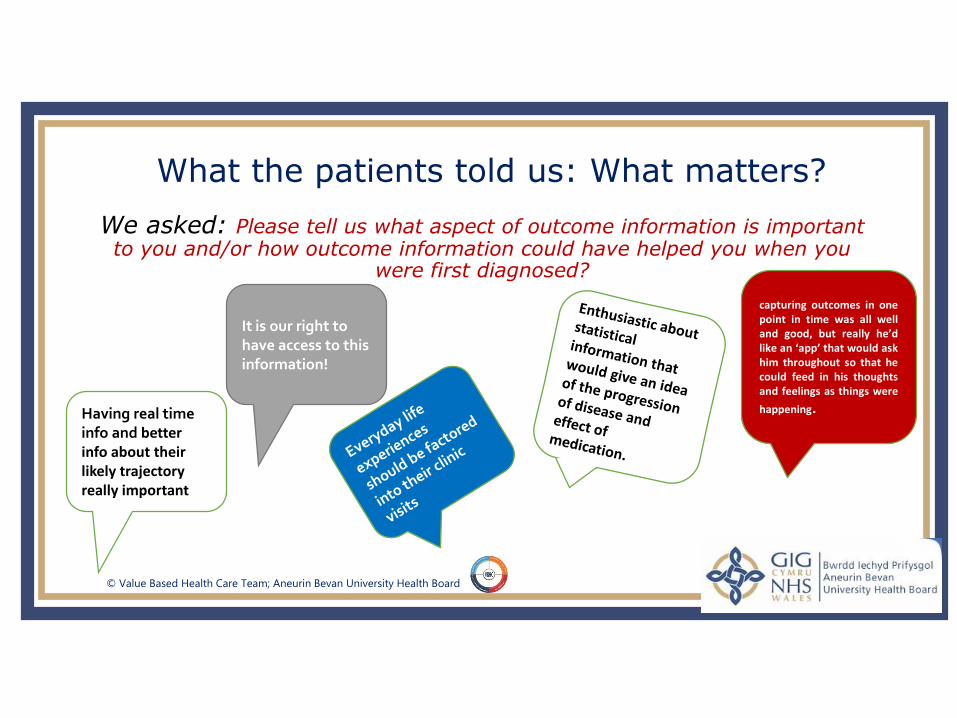
We asked: Please tell us what aspect of outcome information is important to you and/or how outcome information could have helped you when you
were first diagnosed?
What the patients told us: What matters?
Having real time info and better info about their likely trajectory really important
It is our right to have access to this information!
capturing outcomes in onepoint in time was all welland good, but really he’dlike an ‘app’ that would askhim throughout so that hecould feed in his thoughtsand feelings as things were
happening.
© Value Based Health Care Team; Aneurin Bevan University Health Board
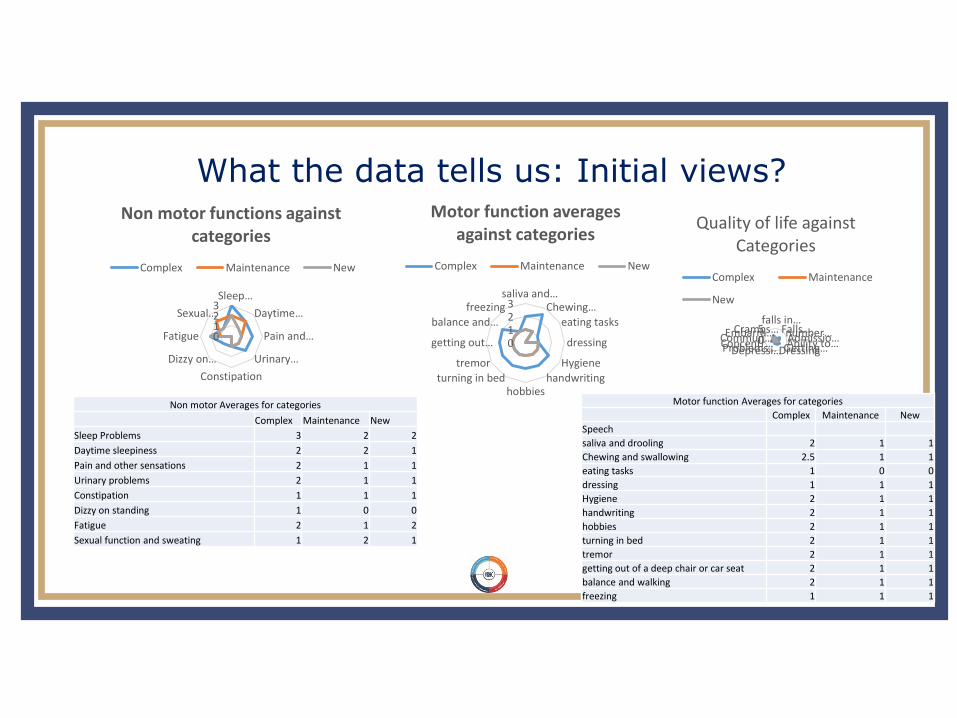
What the data tells us: Initial views?
0123Sleep…
Daytime…
Pain and…
Urinary…
Constipation
Dizzy on…
Fatigue
Sexual…
Non motor functions against categories
Complex Maintenance New
Non motor Averages for categories
Complex Maintenance New
Sleep Problems 3 2 2
Daytime sleepiness 2 2 1
Pain and other sensations 2 1 1
Urinary problems 2 1 1
Constipation 1 1 1
Dizzy on standing 1 0 0
Fatigue 2 1 2
Sexual function and sweating 1 2 1
Motor function Averages for categories
Complex Maintenance New
Speech
saliva and drooling 2 1 1
Chewing and swallowing 2.5 1 1
eating tasks 1 0 0
dressing 1 1 1
Hygiene 2 1 1
handwriting 2 1 1
hobbies 2 1 1
turning in bed 2 1 1
tremor 2 1 1
getting out of a deep chair or car seat 2 1 1
balance and walking 2 1 1
freezing 1 1 1
0123
saliva and…Chewing…
eating tasks
dressing
Hygiene
handwritinghobbies
turning in bed
tremor
getting out…
balance and…
freezing
Motor function averages against categories
Complex Maintenance New
05 falls in…
Falls…number…Admissio…Ability to…Getting…DressingDepressi…Problems…Concentr…Commun…Embarra…Cramps…
Quality of life against Categories
Complex Maintenance
New
Example 2:
Implementing Allocative/Technical value in COPD
© Value Based Health Care Team; Aneurin Bevan University Health Board

Inpatients
£3.1M
1,200 people
1,600 episodesPrescribed COPD
drugs
£6.9M
Population unknown
Pulmonary Rehabilitation
Cost est. £0.065M
Current offer 429 places
Home Oxygen service
£0.3M
490 COPD patientsSmoking Cessation
Pharmacy scheme £0.1M (all conditions)
NRT £0.5M (all conditions)
Population unknownFlu Immunisation – 9,800 COPD population
Immunisation fee £7.80 x 9,800 = £0.07M
8,487 General COPD Risk Register
4, 280 > MRC3 Risk Register
12, 867 pop’n GP QOF Payment for management in primary care £0.5M
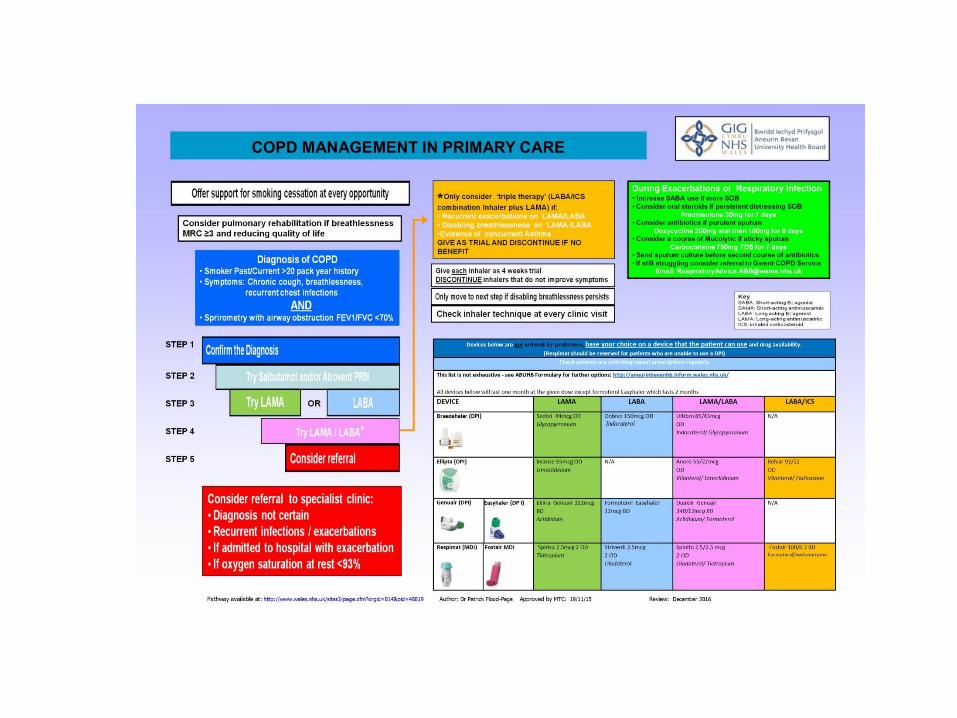
• Disinvestment in low value activity led by clinicians who havesubsequently influenced decision making around high valuereinvestment, thereby improving outcomes and reducing costssimultaneously.
• Example: Respiratory Care involving a collaboration of primary care,secondary care, pharmacy, finance and patient representative.Rationalise inhaler prescribing which was not of benefit to patients withchronic obstructive pulmonary disease.
• Savings for 2015/6 were £204K recurrently and work is expanding.
• Re-investment: proportion of saving in PR, providing equitable timelyaccess , improving quality of life
• Reduce hospital admissions due to exacerbations.
• be highly cost-effective – it is substantially below the NICE thresholdfor cost-effectiveness, at only £2,000 - £8,000 per QALY
• Pulmonary Rehabilitation is a cost effective intervention. Estimates ofsavings range from £890 per person per course (Griffith et al: Thorax2001) to £1835 per person per year (Chakravorti et al : ISRNPulmonology 2011)
• They will be doubling the number of places to 900 from 429. Thereforecan see the economic benefit as well as the personal value
© Value Based Health Care Team; Aneurin Bevan University Health Board

Example 3:
Implementing Costing and Outcomes Capture in Cataract
Surgery i.e. Outcomes/Cost = Value
Globe Benchmarking
© Value Based Health Care Team; Aneurin Bevan University Health Board
Cataract Pathway IntroductionStarted with Costing
Planned Care Programme:Evidence based pathway redesign and standardisation across Wales
Measuring patient outcome, experience and value for moneyApproached Directors of Finance to advise on best approach to the latter
From initial work on cataract pathway they knew the number of steps in pathways around Wales varied but ‘so what’
Mark Bowling, Finance BPA and BI Lead© Value Based Health Care Team; Aneurin Bevan University Health Board
Cataract Pathway Methodology_____________________________
From previous experiences ABUHB approached to pilot. Once internal version complete:
Mark Bowling, Finance BPA and BI Lead© Value Based Health Care Team; Aneurin Bevan University Health Board
1. Presented to other Welsh Health Boards –sharing tools, templates and models
2. Regularly meeting to manage issues3. Key consistency – apples with apples4. Key decision – the real cost of getting one patient through a
cataract operation5. Therefore capturing and segregating under-utilisation /
wastage6. Additional levels of analysis to allow deeper benchmarking
and variation7. Feedback sessions locally and nationally8. Comparison with traditional costing
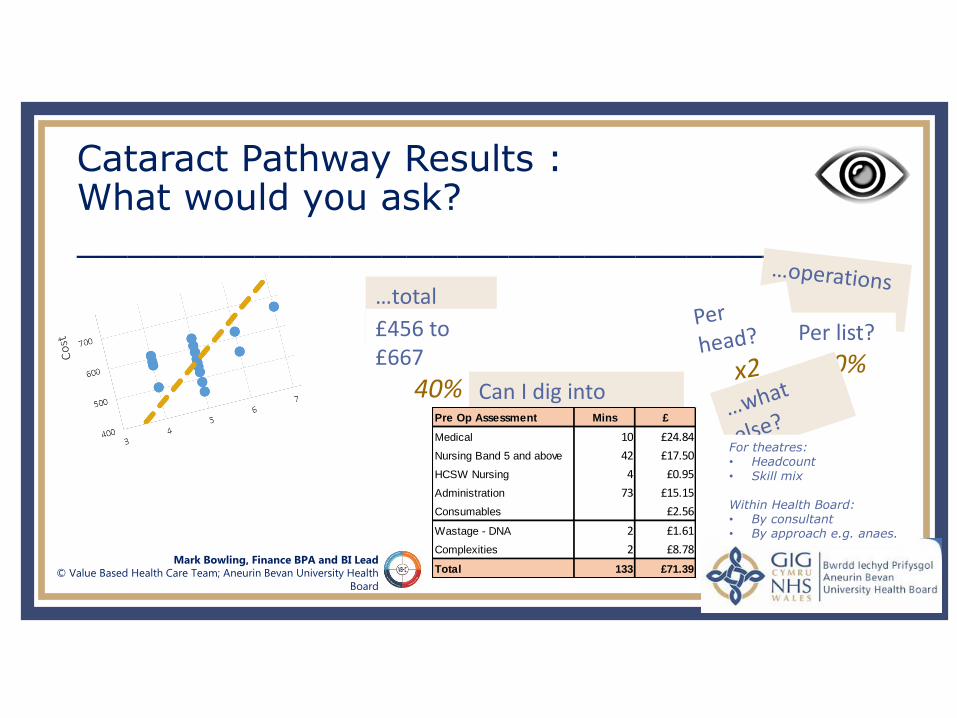
Cataract Pathway Results :What would you ask?_____________________________
Mark Bowling, Finance BPA and BI Lead© Value Based Health Care Team; Aneurin Bevan University Health
Board
…total cost?£456 to £667
40%
Per list?
60%Can I dig into results?Pre Op Assessment Mins £
Medical 10 £24.84
Nursing Band 5 and above 42 £17.50
HCSW Nursing 4 £0.95
Administration 73 £15.15
Consumables £2.56
Wastage - DNA 2 £1.61
Complexities 2 £8.78
Total 133 £71.39
For theatres:• Headcount• Skill mix
Within Health Board:• By consultant• By approach e.g. anaes.
Cataract Globe Benchmarking
© Value Based Health Care Team; Aneurin Bevan University Health Board
Pre- & post-op patient questionnaires plus intra-op data.
Completed:• Clinical Engagement• Gap Analysis• Started Data Collection
Still to do:• Data validation• Complete data collection• Feed back

Questions ?
© Value Based Health Care Team; Aneurin Bevan University Health Board

2017 CONFERENCE
Sir Muir GrayChair
Health and Social CareDigital Service

2017 CONFERENCE
Value Based Healthcare
THANK YOU

2017 CONFERENCE
Lower Hall
Ground Floor







