

DOI: 10.1161/CIRCULATIONAHA.113.004777
1
Warfarin Use and the Risk for Stroke and Bleeding in Patients with Atrial
Fibrillation Undergoing Dialysis
Running title: Shah et al.; Warfarin Use in AF Patients Undergoing Dialysis
Mitesh Shah, MBBS, MSc1; Meytal Avgil Tsadok, PhD1; Cynthia A. Jackevicius, PharmD,
MSc2; Vidal Essebag, MD, PhD3; Mark J. Eisenberg, MD, MPH4; Elham Rahme, PhD1;
Karin H. Humphries, DSc5; Jack V. Tu, MD, PhD6; Hassan Behlouli, PhD1; Helen Guo, MSc7;
Louise Pilote, MD, PhD1
1Divisions of Clinical Epidemiology and General Internal Medicine, McGill University Health Center, Montreal, Quebec, Canada; 2Dept of Pharmacy Practice and Administration, College of
Pharmacy, Western University of Health Sciences, Pomona, CA; 3Division of Cardiology, McGill University Health Center, Montreal, Quebec; 4Divisions of Cardiology and Clinical Epidemiology, Jewish General Hospital/McGill University, Montreal, Quebec; 5Division of
Cardiology, University of British Columbia, Vancouver, British Columbia; 6Institute for Clinical Evaluative Sciences, Toronto, Ontario; Institute of Health Policy, Management and Evaluation, Faculty of Medicine, University of Toronto, Toronto; Division of Cardiology, Schulich Heart
Centre, Sunnybrook Health Sciences Centre, University of Toronto, Toronto; 7Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada
Address for Correspondence:
Louise Pilote, MD, MPH, PhD
McGill University Health Centr
687 Pine Avenue West, V Building
Montreal, Quebec, H3A 1A1 Canada
Tel: 514-934-1934 ext. 44722
Fax: 514-934-8293
E-mail: [email protected]
Journal Subject Codes: Etiology:[5] Arrhythmias, clinical electrophysiology, drugs, Etiology:[8] Epidemiology, Anticoagulants:[184] Coumarins, Stroke treatment - medical:[70] Anticoagulants, Treatment:[118] Cardiovascular pharmacology
1Divisions of Clinical Epidemiology and General Internal Medicine, McGill UnUnnivivivererersisisitytyty HHHeaeaealtltlthh Center, Montreal, Quebec, Canada; 2Dept of Pharmacy Practice and Administration, College of
Pharmacy, Western University of Health Sciences, Pomona, CA; f 3Division of Cardiology,McMccGiGiGillllll UUUninn veveersrsrsitity Health Center, Montreal, QQQueueuebec; 4Divisions off CCCaraa diology and Clinical EpEpEpididemmioioolloogyy, JeJewiwishsh GGenere ala HHosspitatal/McGcGilill UUnivverersis ty, MoMoMontrerealal, , Quebebece ; ; 5DiD viv siion of
CCCarrdrdiologyy, UnUnUniviviveeersisisitytty oooff f BrBrBritititisisish hh CoCoColululumbmbm iaiaia, VaVaV nnccooouveveer,r,r, BBBririrititishshsh CCCololo umumumbbbia;; 66InInInstststitititututu e e e fofofor r r ClClClinninici alEvEvEvala uative Scieenccces, TTooronnntooo, OnOntataririo;o; Insttittuute oofff Heealalalththth PPoolicccyy,, Maannaaageememeent ananndd d EEEvaaaluaattiooon, FaFaFacucuc ltlty ofoff MMMededdicccinineee, UUUniivveversrsrsitity y ofofo TTToorrononttto,, ToTororoontntoo;o; DDivivvisssioionnn ooof Caaardddioiollol ggygy,, SScchhhulliichhh HHeaeaeart
CeCeCentntntrerere, , SSuSunnnnnnybybybrororookokok HHHeae ltltthh h ScScScieieiencnceseses CCCenenentttrrere,, UnUnUnivivi ererersisisitytyty ooof ff ToToorororontntnto,oo, TTTororononntototo; ;; 777IInInstststitititutututeee fofoforrr ClClClinininicicicalalal EEEvavavalululuatatativiviveee ScScScieieiennncececesss, TTTorororononontototo, OnOnOntatatariririooo, CCCanananadadadaaa
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
2
Abstract
Background—Current observational studies on warfarin use and the risk for stroke and bleeding
in patients with atrial fibrillation (AF) undergoing dialysis found conflicting results.
Methods and Results—We conducted a population-based retrospective cohort study of patients
aged 65 years and older admitted to a hospital with a primary or secondary diagnosis of AF, in
Quebec and Ontario, Canada from 1998 to 2007. The AF cohort was grouped into dialysis
(hemodialysis and peritoneal dialysis) and non-dialysis patients and into warfarin and no-
warfarin users according to the first prescription filled for warfarin within 30 days after AF
hospital discharge. We determined the association between warfarin use and the risk for stroke
and bleeding in dialysis and non-dialysis patients. The cohort was comprised of 1,626 dialysis
patients and 204,210 non-dialysis patients. Among dialysis patients, 46% (756/1,626) patients
were prescribed warfarin. Among dialysis patients, warfarin users had more congestive heart
failure and diabetes but less prior bleeding event compared to the no-warfarin users. Among
dialysis patients, warfarin use, compared to no-warfarin use, was not associated with a lower risk
for stroke (adjusted hazard ratio (HR): 1.14, 95% confidence interval (CI): 0.78 to 1.67) but was
associated with a 44% higher risk for bleeding (adjusted HR: 1.44, 95% CI: 1.13 to 1.85) after
adjusting for potential confounders. Propensity score adjusted analyses yielded similar results.
Conclusions—Our results suggest that warfarin use is not beneficial in reducing stroke risk but
is associated with a higher bleeding risk in patients with AF undergoing dialysis.
Key words: atrial fibrillation, dialysis, warfarin, stroke, bleeding
hospital discharge. We determined the association between warfarin use and thee rrrisskk k fofofor r stststrororokekke
and bleeding in dialysis and non-dialysis patients. The cohort was comprised of 1,626 dialysis
paatitiienenentststs aandndnd 222044,22,21010 non-dialysis patients. Amononong dialysis patientntn s, 446%6%6% (756/1,626) patients
wwerrere prescribeed dd wawarfrffaaarininn. AmAmAmoonong gg dididialalysyssis ppattiienttss,, waaarfrffarariinn uusesersrs hhadadd mmmororeee ccocongnggesese titit vevee hhheaearrtr
faailililururureee anandd d dididiababeeteteeses bbuuut llesess prprp ioioiorrr blblbleeeedidid ngngng eeevenenent t cococompmpmpararrededed to oo ththt ee nonono-w-wwararrfafariririn n ususu ererersss. AAAmmomongngg
dialysis patieentntnts,s,s, wwwarara fafafaririr n ususu e,ee cococompmpmpararededed tttooo nonono-w-wwararrfafafarir n n n usususe,e,e, wwwasasas nnototo aaassssssococociaiai teteed d d wiwiwiththth aa lower riskkk
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
3
Introduction
Patients with atrial fibrillation (AF) suffering from severe chronic kidney disease (CKD) have a
higher risk for stroke and bleeding.1, 2 AF is the most common cardiac arrhythmia and is an
independent risk factor for a new stroke.3, 4 Patients with AF suffering from severe CKD, which
requires treatment with dialysis, have a five-fold higher risk for a new stroke.3, 4 AF is becoming
increasingly prevalent among patients with severe CKD predisposing a patient to a much higher
risk for a new stroke.1, 5, 6 Historically, warfarin, a vitamin K antagonist, has been considered the
preferred anticoagulant for reducing the risk of stroke in most patients with AF.7 However,
warfarin use has been shown to accelerate vascular calcification in CKD patients, which
eventually may further increase the risk for ischemic stroke.5, 8-10 Therefore, uncertainty still
exists regarding whether warfarin confers similar protection to reduce the risk for stroke in
patients with AF suffering from severe CKD.11-14
CKD is also considered as an independent risk factor for bleeding and therefore, warfarin
use in patients suffering from severe CKD could increase the risk for bleeding.2 Moreover, in
patients with AF undergoing hemodialysis, it is routine practice to administer heparin which
could also increase the risk for bleeding.15
Current observational studies on warfarin use and the risk for stroke and bleeding in
patients with AF undergoing dialysis present conflicting results.1, 8, 16, 17 Globally, due to lack of
evidence from randomized controlled trials (RCTs), AF management guidelines have yet to
make strong recommendations regarding anticoagulation management for patients with AF
undergoing dialysis.18-23 Due to recognized limitations of warfarin use such as frequent blood
monitoring for a therapeutic international normalized ratio (INR), numerous food and drug
interactions, uncertainly regarding benefit for reducing stroke risk, and possible augmentation of
eventually may further increase the risk for ischemic stroke.5, 8-10 Therefore, unceceertrtaiaia nntty y y stststililillll
exists regarding whether warfarin confers similar protection to reduce the risk for stroke in
paatitiienenentststs wwwititithhh AFAF sssuufuffering from severe CKD.11-141414
CKD isis aaalsso cocoonsnssidididerererededed aas ss ananan iindnddepeeendddenttt rriiskk ffaacactotoor fofor r bblleeeedididinggg aandndnd ttheheererer fofoforeree, wwawarfrr aaarinkk
ususe ee ininn pppatatieieentntnts s susuufffffererininng g frfromomm ssevevevererereee CCCKDKDKD cccouuuldldl iiinnccreeeasasseee thththe e ririr skskk fffororo bbbleeeededinining.g.g 22 MMMoooreoooveveer,r, iiinn
patients with h AFAFAF uuundndndererergogog ininng g g hehehemomom dididiallysysy isisis,, ititit iis s s rororoutututinini e e prprpracacactitt cecece tott aaadmdmdminininisisistetet r r hehehepapapariririn nn which
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
4
bleeding risk, clinicians often raise concern about warfarin’s safety and effectiveness in patients
with AF undergoing dialysis.7, 11-15
To enhance knowledge on this issue, we determined the association between warfarin use
and the risk for stroke and bleeding in patients with AF undergoing dialysis in Quebec and
Ontario, Canada.
Methods
Study design
We conducted a population-based retrospective cohort study of patients aged 65 years and older
admitted to a hospital with a primary or secondary diagnosis of AF from 1998 to 2007, in
Quebec and Ontario, Canada. Residents in Quebec and Ontario have universal access to hospital
care and physician services and those 65 years of age and older have universal prescription drug
coverage. For this study, we obtained institutional review board approval from McGill
University Faculty of Medicine, Montreal (Quebec) and from Sunnybrook Health Sciences
Centre, Toronto (Ontario).
Study Population and Data Sources
Cohort formation has been described in detail elsewhere.24, 25 In brief, we identified patients with
a primary or secondary diagnosis of AF according to the International Classification of Diseases
– 9th/10th revision codes (427.3, 427.31, or 427.32 / I48) using the following hospital discharge
abstract databases in Quebec and Ontario: Maintenance et Exploitation des Données pour l’Étude
de la Clientèle Hospitalière and the Canadian Institute for Health Information Discharge Abstract
Database, respectively. The primary (principal) diagnosis code is the main condition treated or
investigated during the admission. However, up to seven diagnosis codes may be recorded by the
admitted to a hospital with a primary or secondary diagnosis of AF from 1998 too 2020007077,, ininn
Quebec and Ontario, Canada. Residents in Quebec and Ontario have universal access to hospital
caareree aaandndnd ppphyhyhysssiciiananan sservices and those 65 years oooff f aagge and older hahaave uunininivversal prescription drug
coovveverage. For r ththhisi stutudydydy, wewe ooobbtbtaiaiinenened d ininsstituuutiioonaall rrreviiieweww bbboaaardrd appppprorovvavall frfrromomom MMMcGcGcGililill ll
UnUnnivivivererersisitytyy FFFaacacululltytyy oof f MeMMedid ciciinene, MoMoMontntrerer alalal (Q(Q(Queueuebebeec)c)) andndnd fffrororom mm SuSuunnnnnybyby rrroookok HHHeaeaaltlthh h SScScieeenccceses
Centre, Toroontntnto o o (O(OOntntn arara ioioi )..
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
5
hospital. The remaining diagnoses (secondary) are considered to be the subsidiary diagnoses. For
patients with more than one eligible admission with an AF diagnosis, the date of the first
admission with an AF diagnosis was considered the index date of entry into the study cohort. We
determined patients’ baseline characteristics, outcome data, and drug prescriptions from linkage
between hospital discharge, physician claims, prescription drug claims, and vital status databases
in Quebec and Ontario (Supplemental Table 1). For the stroke and bleeding outcomes, we used
data from emergency room (ER) visits in addition to the information from the hospital discharge
databases. We used validated database codes (whenever possible) to determine stroke and
bleeding outcomes.26-30
We used the physician claims databases maintained by la Régie de l’assurance maladie
du Québec (RAMQ) and the Ontario Health Insurance Plan, which contain information on in-
and out-patient diagnostic and therapeutic procedures. We also used the RAMQ and the Ontario
Drug Benefit Plan drug claims databases, which contain information on dispensed outpatient
medications for patients aged 65 years and older. Drug prescriptions were identified from these
databases using drug identification numbers. These prescription claims databases provide highly
accurate information on dispensed outpatient medications.31-33
We grouped the selected AF cohort into dialysis and non-dialysis patients according to
the presence of three or more dialysis procedural codes (same or different codes for hemodialysis
and peritoneal dialysis) within 12 months prior to AF hospitalization (database codes in
Supplemental Table 2). Our three-code rule attempted to select patients undergoing maintenance
dialysis. For all patients, we assessed demographic characteristics and comorbidities at and
within one year prior to AF hospitalization using validated codes, whenever possible. We
obtained information on the first prescription filled for warfarin, rate control drugs ( -blockers,
We used the physician claims databases maintained by la Régie de l’assururrannncece mmmalalaladadadieie
du Québec (RAMQ) and the Ontario Health Insurance Plan, which contain information on in-
annd d d ouououtt-t-papaatititiennt dididiaagagnostic and therapeutic proceeeddudurrres. We also uuseses d ththhee e RRAMQ and the Ontario
DDruugug Benefit PPlalalann drdruuug ccclalalaimimimsss dadatatat babab ssesess, wwhihich ccoconntaiaiinn n ininfofof rmrmaaatiioon n oonn ddisispepepensnsededd oooututppapatititienennt
memeedididicacacatitiononnss s ffofor r papapatitienenntss aagged dd 656565 yyyeaeearsrs aandndnd ooolddderere .. DDrrugugg ppprereresscriririptptptioionsnsns wwwerrree ididdenenntitifififiededd ffrrorommm ththhessee
databases ussininnggg drdrrugugug iiidededentttififificicicatttioioionnn nunun mbmbm erere s.s.s TTThehehesse ee prprp esesscrcrcripipiptitit ononon cclaaaimimims s s dadadatatatababaaseseses s s prprprovovo ide highlyyy
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
6
calcium channel blockers, and digoxin), rhythm control drugs (class Ia, Ic, and III
antiarrhythmics), aspirin, clopidogrel, and NSAIDs (non-steroidal anti-inflammatory drugs)
within 30 days after AF hospital discharge.
We grouped dialysis and non-dialysis patients into warfarin and no-warfarin users. We
selected a 30-day period to capture the majority of patients with the first prescription for warfarin
after AF hospital discharge, while minimizing the potential for survival bias.34 Our follow-up
period was started 30 days after AF hospital discharge (from the first day after the 30-day
period). The outcomes of interest were the first hospital admission or ER visit for (i) stroke; or
(ii) bleeding, at any point during follow-up period. We defined stroke as ischemic
cerebrovascular disease including transient ischemic attack (TIA) and retinal infarct. We did not
include intracerebral hemorrhages in the stroke outcome because intracerebral hemorrhages
could be a complication of warfarin use. We defined bleeding as intracerebral bleeding,
gastrointestinal bleeding, intraocular bleeding, hematuria, and unspecified location of bleeding.
We calculated CHADS2 score by assigning one point each for congestive heart failure,
hypertension, age 75 years, and diabetes, and two points for history of stroke/TIA; the
CHADS2 scores ranged between 0-6.35 The CHADS2 score is a widely used clinical prediction
score for estimating the risk for stroke and serves to guide clinicians in determining suitable
usage of warfarin in AF.35 We also calculated the HAS-BLED risk stratification score, the
clinical prediction score for estimating the risk for bleeding.36, 37 The HAS-BLED score is
calculated assigning one point each for hypertension, abnormal renal function, abnormal liver
function, history of stroke/TIA, history of bleeding, labile INR, age 65 years, drug therapy
(antiplatelet agents, NSAIDs), and alcohol intake.36, 37 Since our databases do not provide
information on labile INR and alcohol intake, we calculated a modified HAS-BLED score, with
cerebrovascular disease including transient ischemic attack (TIA) and retinal infafaarcct.t.t WWWe ee dididid d d non t
nclude intracerebral hemorrhages in the stroke outcome because intracerebral hemorrhages
cooulululdd d bebebe aaa cccoommplpllicicicata ion of warfarin use. We defffininineedd bleeding as iiintn raacececerrerebral bleeding,
ggastttror intestinalal bbbleeeedddinini gg,g, iiintntntrararaoocucuulalalarr bbbleeedinngng, heemmatuuuriria,a, aaanndd uunnsnspepeciciifif eeded lllocococatatioioon nn ofofof bbbleee dededinini ggg.
WeWee cccalalcucuulaaatetedd CCHHADADDSS22 scscscorororee bybyby aaassssssigggninin nngng oonenee pppoioioinnnt eeeacacch h fofoforr ccoconngngesesestitiivevev hhheeearttt faaiailulurrre,,
hypertensionn,, agagage e 77555 yeyey ararars,s,s, andndnd ddiaiaiabeeetetetes,s,s aaandndnd ttwowowo pppoiointntnts s s fofofor r r hihihists ororory y y ofofof ssstrtrtrokokoke/e/e/TITITIA;A;A; tthe
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
7
a maximum score of seven rather than nine.36, 37
Statistical Analyses
Descriptive analyses were used to compare demographic characteristics, comorbidities, and
prescription for medications between warfarin and no-warfarin users in the group of dialysis and
non-dialysis patients. We presented continuous variables as mean ± standard deviation and
dichotomous variables as number (%). We calculated crude stroke and bleeding incidence rate
(per 100 person-years) for the group of dialysis and non-dialysis patients. We also stratified
crude stroke and bleeding incidence according to warfarin use, CHADS2 score (for stroke
incidence rate), and HAS-BLED score (for bleeding incidence rate). Due to restrictions to access
and merge databases, we did separate analyses in Quebec and Ontario, and then combined study
results from both the provinces. Results for descriptive analyses and incidence rate are weighted
averages for results from Quebec and Ontario.
To determine association between dialysis status and warfarin filled prescription, we
conducted a multivariable logistic regression analysis. To determine association between
warfarin use and the risk for stroke and bleeding in the group of dialysis and non-dialysis
patients, we conducted multivariable Cox proportional regression analyses. In multivariable Cox
proportional hazards models, we considered warfarin use vs. no-warfarin use as a time-fixed
binary variable, where we assumed that patients who were prescribed warfarin within 30 days
after AF hospital discharge remained on the same prescription throughout the follow up period.
This approach is akin to an intention to treat analysis in RCTs.38
To account for the effect of potential confounders in the warfarin and stroke risk
analyses, we adjusted for age (years), sex, and specific components of CHADS2 score
(congestive heart failure, hypertension, diabetes, and history of stroke/TIA). In the warfarin and
and merge databases, we did separate analyses in Quebec and Ontario, and then cccommmbbibinenened dd stststududy y
esults from both the provinces. Results for descriptive analyses and incidence rate are weighted
avverereragagageeses fffororo rrresulululttsts from Quebec and Ontario.
To detterermimiminee aaassssococciaiaiatititionon bbbetetetwweeeeen ddiiai lllysisss sstatususus aandnnd wwaarrfafaaririn n fiff llllededd ppprerescsccririr pptptioioion,,, wweee
coondndnducucuctetedd a aa mmumullttivvvarariiaabblble e loogigig stststicicic rrregegrreressssssioioionn n anananalallysyssis.. ToToTo dddettterere mmiminenene aassssoocociaiaatitit onono bbbetetetweeeennn
warfarin usee aaandndnd ttthehehe rrisisi k kk fofoorr r stss rorookekek aaandndd bbleleleedededinining g g ininn ttthehh gggrororoupupup ooof f f did alalalysysysisisis aaandndnd nnnononon-d-ddiaiaialylysis
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
8
bleeding risk analyses, we adjusted for age (years), sex, and specific components of HAS-BLED
score (liver disease, hypertension, history of stroke/TIA, history of bleeding, and use of aspirin,
clopidogrel, or NSAIDs). For each patient in the warfarin or no-warfarin users, we derived a
propensity score for receiving warfarin treatment from the following variables: age 75 (years),
sex, type of AF admission (primary diagnosis vs. secondary diagnosis), CHADS2 scores (1 and
2), liver disease, congestive heart failure, hypertension, diabetes, history of stroke/TIA, history of
bleeding, use of rate control drug, rhythm control drug, aspirin, clopidogrel, and NSAIDs. To
verify the results of stroke and bleeding risk analyses, we performed Cox proportional regression
analyses adjusted for a propensity score covariate.39 The propensity score is a good alternative to
reduce bias when there is a risk of statistical overfitting due to a low number of events per
potential confounder (i.e. a low number of stroke and bleeding events in the dialysis group).40
The propensity score indicated the likelihood of receiving warfarin given that a particular patient
related characteristic is present.39 We used multivariable logistic regression models to derive
individual propensity scores for the group of dialysis and non-dialysis patients, respectively.
Results are expressed as odds ratio (OR) for logistic regression analysis or hazard ratios
(HRs) for Cox regression analyses with 95% confidence intervals (CIs). To combine results from
Quebec and Ontario, we pooled the OR (or HR) for each predictor using a fixed-effects model,
weighted for the inverse of the variance of the province-specific parameter estimate, ln (OR) [or
ln (HR)].41 We performed all statistical analyses using SAS 9.2 (SAS Institute, Cary, NC, USA).
Results
Baseline Characteristics
The AF cohort includes 1,626 dialysis patients and 204,210 non-dialysis patients. Dialysis
educe bias when there is a risk of statistical overfk itting due to a low number of eevevenenntsss pppererer ff
potential confounder (i.e. a low number of stroke and bleeding events in the dialysis group).40
Thhe e e prprproopopenenensisitty sscococorer indicated the likelihood of ff rerer ccceiving warfarrininin giivevevenn n that a particular patient
eelaaateted characcteterrir stticc iiis s pprpresesesenenentt.t.39399 WWWe e ususeed mmmuuultivvvarrriabbblelee lloogogiisstiticcc rreegrg eesssiiononn mmmododelelelss totot dderereriiviveee
nndididivivividudud alal ppprorropepeensnssitity y scscororese fffororr thththe e e grgrouououppp oofof dddiaiai lylylyssiis anana ddd nnonon-n-n-didiialalysysysisis paatatieientntn s,s,s, rresesesppepectcttivvvelelyy.y.
Resuultlttsss arara ee e exexe prprpresee sesesed d d asass ooodddddds ss raraatitit oo o (O(O(OR)R)R) fffororo lllogogisisistitiic cc rereregrgrgresee sisisiononon aaanananalylylyssisisi ooor rr hahahazaz rd ratios
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
9
patients were younger, more likely to be men, and had more congestive heart failure,
hypertension, diabetes, coronary artery disease, and past history of bleeding event, compared to
non-dialysis patients (Table 1). A larger proportion of dialysis patients, compared to non-dialysis
patients, had high risk score for stroke (CHADS2 score 2: 72% (1,176/1,626) vs. 55%
(112,049/204,210)) and bleeding (HAS-BLED score 3: 85% (1,381/1,626) vs. 25%
(50,203/204,210)).
Prescription Pattern of Warfarin
Comparable proportions of the dialysis patients and the non-dialysis patients filled a prescription
for warfarin within 30 days after AF hospital discharge (46% (756/1,626) vs. 51%
(103,473/204,210)). In the multivariable logistic regression model, dialysis status was associated
with a lower proportion of filled prescriptions for warfarin (adjusted OR: 0.83, 95% CI: 0.74 to
0.92).
Among dialysis patients, those who filled a prescription for warfarin had more congestive
heart failure and diabetes but less prior bleeding event compared to the no-warfarin users.
Patients who filled a prescription for warfarin had higher proportion of patients with the high risk
score for stroke (CHADS2 2: 77% (580/756) vs. 69% (596/870)) compared to the no-warfarin
users but the proportion of high risk score for bleeding (HAS-BLED 3: 84% (637/756) vs. 86%
(744/870)) was similar between both the groups.
Stroke Outcome
Among dialysis patients, warfarin users did not have a lower crude incidence rate for stroke
compared to the no-warfarin users (unadjusted incidence rate: 3.37 vs. 2.91 / 100 person-years; P
= .44) (Table 2). On the contrary, among the non-dialysis patients, warfarin users did exhibit a
lower crude incidence rate for stroke compared to the no-warfarin users (unadjusted incidence
103,473/204,210)). In the multivariable logistic regression model, dialysis statuusss waww ss asasassososociciciatated
with a lower proportion of filled prescriptions for warfarin (adjusted OR: 0.83, 95% CI: 0.74 to
0..92922).).).
Amonng g ddid aaalysysisi pppatatatieieientntnts,s, tthohohosese wwwho ffilllled a ppreesesccrcripipptiionon ffoorr wwaarrffaaririnn n hhahad d momomorere coonongegeeststtive
heheararart t fafafaililururreee anandd didiiababeeeteeses bbututt leessssss ppprririororr bbbleleleeededininng g g eeveveentt t cocoompmpmparararededd ttooo ththt eee nnono-w-wwararrfafariririnn n usserers.s.s
Patients whoo fffililillelel dd d aa a prprp esee crcrripipiptitt ononon ffororor wwwarara fafafariririn n n hahah d d d hihihighghg ererer ppprororopopoportrtrtioionn n ofofof pppatatatieieientnttss wiwiw ththth tthe high risskk
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
10
rate: 2.19 vs. 2.51 / 100 person-years; P < .001).
After adjusting for potential confounders, warfarin use, compared to no-warfarin use, was
not associated with a lower risk for stroke in dialysis patients (adjusted HR: 1.14, 95% CI: 0.78
to 1.67), however, it was associated with a 13% lower risk for stroke in non-dialysis patients
(adjusted HR: 0.87, 95% CI: 0.85 to 0.90) (Table 3). We observed similar results when we
performed propensity score adjusted Cox proportional regression analyses (dialysis patients –
adjusted HR: 1.17, 95% CI: 0.79 to 1.75; non-dialysis patients – adjusted HR: 0.89, 95% CI:
0.87 to 0.92).
Bleeding Outcome
Among dialysis patients, warfarin users had a higher crude incidence rate for bleeding event
compared to the no-warfarin users (unadjusted incidence rate: 10.88 vs. 7.31 / 100 person-years;
P < .001) (Table 2). Similarly, among non-dialysis patients, warfarin users had a higher crude
incidence rate for bleeding event compared to the no-warfarin users (unadjusted incidence rate:
4.64 vs. 4.00 / 100 person-years; P < .001).
After adjusting for potential confounders, warfarin use, compared to no-warfarin use, was
associated with a 44% and a 19% higher risk for bleeding event in dialysis patients (adjusted HR:
1.44, 95% CI: 1.13 to 1.85) and non-dialysis patients (adjusted HR: 1.19, 95% CI: 1.16 to 1.22),
respectively (Table 3). We observed similar results when we performed propensity score
adjusted Cox proportional regression analyses (dialysis patients – adjusted HR: 1.41, 95% CI:
1.09 to 1.81; non-dialysis patients – adjusted HR: 1.20, 95% CI: 1.17 to 1.23).
Discussion
Our study indicates that in dialysis patients with AF, warfarin use, compared to no-warfarin use,
Among dialysis patients, warfarin users had a higher crude incidence rate for bleeeeedidiingngg eeveveventntnt
compared to the no-warfarin users (unadjusted incidence rate: 10.88 vs. 7.31 / 100 person-years;
PP << .0000001)1)1) (((TaTaTable e 22)2).. Similarly, among non-dialyyyssisis PP ppatients, warffarara in uuusesesersr had a higher crude
nnciiiddence ratee fffoor bbbleeedede inining gg eveveveenent t cococompmpmpaarred ttoo thee nno-wwwaararfafaaririnn n uusseerrs (u(unananadjdjuusustteted d ininincicicidededencccee raraatetee:
4..646464 vvvs.s.s 44.0.000 0 0 // 1010000 peperrrsoonon--yeeaearsrss;;; PPP <<< ..0000001)1)1).. PPP
After r adadadjujujustststinini g g g foff r r popopotett ntntntiaiai l l cococ nfnfn ouououndndndererers,s,s, wwwarara faaariririnnn uuusesese,, cococ mpmpmparararededed ttto oo nonoo-w-wwarararfafafarin use, waaasnnn
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
11
did not reduce the risk for stroke but was associated with a 44% higher risk for bleeding event,
while warfarin use in non-dialysis patients with AF was associated with a 13% lower risk for
stroke and only a 19% higher risk for bleeding event. Thus, the risk-benefit profile does not
appear to be favourable to support a recommendation of routine warfarin use for stroke reduction
in dialysis patients with AF.
Dialysis patients have several platelet and coagulation abnormalities and also have
associated comorbidities such as uncontrolled hypertension and diabetes, which all contribute to
an increase in the risk for stroke and bleeding.8, 42 Further, dialysis patients routinely receive
heparin during dialysis procedure, which also increases the risk for bleeding.8, 42 Moreover,
warfarin use in dialysis patients, through the inhibition of Matrix Gla protein and Gas-6, can
accelerate vascular calcification, which eventually might increase the risk for ischemic stroke.5, 8-
10 These factors could explain why, in our study, warfarin was not associated with a lower risk
for ischemic stroke in dialysis patients, but was rather associated with an increased risk for
bleeding.
We summarized the results of our current study and evidence from previous published
studies of warfarin use and the risk for stroke and bleeding in patients with AF undergoing
dialysis in Figure 1 and Figure 2, respectively. In a retrospective cohort study of 1,671 AF
patients undergoing haemodialysis, Chan et al. observed a 1.9 fold higher risk for the composite
stroke/death outcome with warfarin use.8 In another observational study analysing data from the
international Dialysis Outcomes and Practice Patterns Study (DOPPS), Wizemann et al.
stratified patients with AF undergoing haemodialysis according to age categories, 65, 65-75,
and > 75 years.17 The authors reported that warfarin use in patients > 75 years (n=1,107) was
associated with a 2.2 fold higher risk for the composite stroke/death outcome.17 In the younger
warfarin use in dialysis patients, through the inhibition of Matrix Gla protein andndd GGGasa -6-6-6, ,, cacacan n n
accelerate vascular calcification, which eventually might increase the risk for ischemic stroke.5, 8
0 TTThehehessese fffacacactototors cccoouould explain why, in our studyyy,, wwaarfarin was notott asssococociiaiated with a lower risk
ffoor isischemic sstrtrokoo eee inin ddiaiaiallylysisiis s s papatititienenntsts, bbbut wawawas raaathhher aasssssococciaiaateteddd wwiwiththh aannn ininncrcrcreaeaseseed d d riririsksksk fffooror
blleeeeeedididingngng..
We ssumumummamamariririzezeed d d thheee rereresuuultltltss ofofo oooururur cccurururrererentntnt ssstutuudydy aaandndnd eeevivividededencncce e e frfrfromomom ppprereeviviviouououss s pupup blished
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
12
age groups, the authors noticed that warfarin use did not reduce the risk for the composite
stroke/death outcome.17 Winkelmayer et al. conducted a retrospective cohort study in
hemodialysis patients with incidental AF and performed propensity score matched analyses
(warfarin user: 237; matched nonusers: 948).16 The authors found that warfarin use did not
reduce the risk for ischemic stroke but was associated with a 2.4 fold higher risk for hemorrhagic
stroke.16 Olesen et al., in 901 dialysis patients, was the only one to observe that warfarin use was
associated with a 56% decrease in the risk for the composite stroke/death outcome.1 However,
there were several limitations to this study.1, 43-45 A larger proportion of dialysis patients had
unusually low HAS-BLED score (HAS-BLED score: 2 – 35% (312/901); 0 or 1 – 43%
(390/901)).1, 44 Contrary to our study and DOPPS, dialysis patients had low prevalence of
diabetes (14% (129/901)) and hypertension (54% (486/901)).1, 43 It is possible that a selection
bias of healthier patients undergoing dialysis could explain the reason for the decreased risk of
stroke with warfarin use in the study by Olesen et al.1, 43
Contrary to our results of increased bleeding risk in dialysis patients, Winkelmayer et al.
and Olesen et al. observed no association between warfarin use and the risk for gastrointestinal
bleeding and the composite bleeding/death outcome, respectively.1, 16
A major consideration when comparing our study results for stroke and bleeding risk
with previous studies is the heterogeneity in stroke and bleeding definitions across the different
studies.1, 8, 16, 17 In our study, we included ischemic stroke, TIA, and retinal infarct in stroke
definition and excluded intracerebral hemorrhages. Contrary to the composite stroke/death and
bleeding/death outcomes in previous studies,1, 8, 17 we did not include death in our stroke and
bleeding definitions.
Our study has a number of strengths. Our large sample size allowed us to study the
390/901)).1, 44 Contrary to our study and DOPPS, dialysis patients had low prevvaaalenenncee ooof f f
diabetes (14% (129/901)) and hypertension (54% (486/901)).1, 43 It is possible that a selection
biiasass ooofff hehehealalalthththier r papapatit ents undergoing dialysis coouululdd explain the reaeaason n fofoforr the decreased risk of
ttroookke with waarfrfrfararinin uuusesee iiin nn ththheee ststudududyy y bbyy Oleeseeen ettt aaal.1, 44343
CoContntntrrararyryy too o ououurr rreressultlttss ofofof iiincncncrereasasasededed bbbleeeedede iiinggg rriisi k kk ininin ddiaiaialylyysiiisss papapattieenentstss,, WWiWinknknkeelelmmamayyeyer r eeet aaal.l
and Olesen etet aaalll.. obobobseseservrvrveddd nnno o o asasssososociciciata ioioion n n bebebetwtwweeeeeen n n wawaw rfffarararininin usususe e e anaa d d d ththhe e e riririsksksk ffororo gggasasastrtrroio ntestinal
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
13
association between warfarin use and the risk for stroke and bleeding in the AF cohort. Unlike
other studies, we attempted to reduce concerns about statistical overfitting46 and included only
the most relevant covariates in the adjusted analyses. Finally, the information available within
the large Quebec and Ontario health care databases reflects routine clinical practice in Canada,
and may be less prone to participation biases that can arise in other types of studies.47
There are some limitations to our study. First, biases due to residual confounding from
unknown or unmeasured confounders and also confounding by indication are well described in
observational studies on drug effects.48, 49 To overcome confounding bias, we adjusted for most
appropriate covariates that may confound the association between warfarin use and the study
outcomes, and also performed sensitivity analyses using the propensity score approach.39, 50
However, we still cannot rule out residual confounding.48 Second, our health administrative
databases do not contain information on INR levels or heparin use during dialysis procedure and
therefore we could not account for these variables in the adjusted analyses. Third, the accuracy
of database codes for patients’ related health information is a known concern in observational
studies based on health administrative databases. In attempt to limit this concern, we used
database codes with the best validation whenever possible.
In summary, current and previous observational studies on warfarin use and the risk for
stroke and bleeding in patients with AF undergoing dialysis failed to provide much evidence in
favor of warfarin use, yet there was a signal for an increased bleeding risk.1, 8, 16, 17 Recently, the
Canadian Cardiovascular Society (CCS) AF guidelines (2012) made conditional
recommendation (on low quality of evidence) that patients with AF undergoing dialysis should
not routinely receive anticoagulation treatment for primary prevention of stroke.23 This is
consistent with the recommendation from the Kidney Disease: Improving Global Outcomes
outcomes, and also performed sensitivity analyses using the propensity score appprproaoaachhh.39,39,39, 505050
However, we still cannot rule out residual confounding.48 Second, our health administrative
daatataabababasseses s dododo nnott cccoonontain information on INR levevevelss or heparin ussee e duuririingngng dialysis procedure and
hhherrrefe ore we ccououulddd nnotot aaacccccououountntnt ffororr ttthehesese varrriaaablesss iinn thehehe aadjddjuusustetedd ananalallyyyseses.. ThThThirird,d,d tthehehe aaacccccururaacacyy y
offf dddatatatababa asaseee coccodedes fofof r r papaatitieentststs’ rrrelelelatatateeded hheaeaealtltlthhh ininnfoformrmrmatatioionnn isisis aaa kkknnoownwnwn cconononcecernrnrn iiin nn obobobssservvvatttioionnanal
tudies based d ononon hhheaeaealtlth hh adadmimimininn stststrararatitiivevv dddatattabababasasasesese . IIn nn atata teeempmpmpt t tototo lllimimimititit tthihih s s s cococoncncn erere n,n,n wwwe e e usu ed
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
14
(KDIGO).22 Nevertheless, with no evidence from RCTs, there is a lack of strong
recommendations for anticoagulation management guidelines for this patient population.18-23
Due to the observational nature of our and previous studies, the study results may not be
conclusive. We propose that a large multi-centre RCT should be undertaken to clarify this issue
and to guide AF management guideline bodies around the world.
Acknowledgments: Dr. Pilote had full access to all of the data in Quebec and Dr. Jackevicius
had full access to all of the data in Ontario and take responsibility for the integrity of the data and
the accuracy of the data analysis. The opinions, results, and conclusions reported in this paper are
those of the authors and are independent from the funding sources. No endorsement by Canadian
Institutes of Health Research (CIHR), Institute for Clinical Evaluative Sciences (ICES), or the
Ontario Ministry of Health and Long-term Care (MOHLTC) is intended or should be inferred.
We thank la Régie de l’assurance maladie du Québec (RAMQ) and Brogan Inc., Ottawa for use
of its Drug Product and Therapeutic Class Database.
Funding Sources: This study was supported by the CIHR operating grant MOP-84304.
Conflict of Interest Disclosures: All the authors declare no competing interest. Dr. Shah
reported receiving a fellowship award from FRQS (Fonds de recherche du Québec - Santé). Dr.
Avgil Tsadok reported receiving a fellowship award from the CIHR. Dr. Essebag is the recipient
of a Clinician Scientist award from the CIHR. Dr. Pilote reported serving as a James McGill
Chair at McGill University and receiving a national investigator award from the Fonds de
recherche en sante´ du Québec.
References: 1. Olesen JB, Lip GY, Kamper AL, Hommel K, Kober L, Lane DA, Lindhardsen J, Gislason GH, Torp-Pedersen C. Stroke and bleeding in atrial fibrillation with chronic kidney disease. NEngl J Med. 2012;367:625-635. 2. Poli D, Antonucci E, Zanazzi M, Grifoni E, Testa S, Ageno W, Palareti G. Impact of glomerular filtration estimate on bleeding risk in very old patients treated with vitamin K
nstitutes of Health Research (CIHR), Institute for Clinical Evaluative Sciences (I(IICECECES)S)S),, ororor ttthehehe
Ontario Ministry of Health and Long-term Care (MOHLTC) is intended or shoululd dd bebebe iinfnfnferererreereddd.
We thank la Régie de l’assurance maladie du Québec (RAMQ) and Brogan Inc., Ottawa for use
off iiitststs DDDrurug gg PrPrProdducucuctt and Therapeutic Class Databababaseee.
FFuFunndnding Soouru ceees:: Thhiis stuuddydy wasa sssupupu popoorteddd bbby thhheee CICIIHRHRHR ooppperaaatinng grrranntnt MMMOPOP-8884343304044.
Conflict of InIntetererestst DDissclososuru eses:: AlAlA l thththeee auauauththhororo s ss dededeclclc ararreee nonono cccomomompepeetitit ngngng iiintntnterere esesesttt. DrDr.. ShS ah
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
15
antagonists. Results of EPICA study on the behalf of FCSA (Italian Federation of Anticoagulation Clinics). Thromb Haemost. 2012;107:1100-1106. 3. Seliger SL, Gillen DL, Tirschwell D, Wasse H, Kestenbaum BR, Stehman-Breen CO. Risk factors for incident stroke among patients with end-stage renal disease. J Am Soc Nephrol. 2003;14:2623-2631.
4. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983-988. 5. Clase CM, Holden RM, Sood MM, Rigatto C, Moist LM, Thomson BK, Mann JF, Zimmerman DL. Should patients with advanced chronic kidney disease and atrial fibrillation receive chronic anticoagulation? Nephrol Dial Transplant. 2012;27:3719-3724.
6. Wetmore JB, Ellerbeck EF, Mahnken JD, Phadnis M, Rigler SK, Mukhopadhyay P, Spertus JA, Zhou X, Hou Q, Shireman TI. Atrial fibrillation and risk of stroke in dialysis patients. AnnEpidemiol. 2013;23:112-118. 7. Mega JL. A new era for anticoagulation in atrial fibrillation. N Engl J Med. 2011;365:1052-1054. 8. Chan KE, Lazarus JM, Thadhani R, Hakim RM. Warfarin use associates with increased risk for stroke in hemodialysis patients with atrial fibrillation. J Am Soc Nephrol. 2009;20:2223-2233. 9. Chan KE, Lazarus JM, Thadhani R, Hakim RM. Anticoagulant and antiplatelet usage associates with mortality among hemodialysis patients. J Am Soc Nephrol. 2009;20:872-881. 10. Reynolds JL, Joannides AJ, Skepper JN, McNair R, Schurgers LJ, Proudfoot D, Jahnen-Dechent W, Weissberg PL, Shanahan CM. Human vascular smooth muscle cells undergo vesicle-mediated calcification in response to changes in extracellular calcium and phosphate concentrations: a potential mechanism for accelerated vascular calcification in ESRD. J Am Soc Nephrol. 2004;15:2857-2867. 11. Ng KP, Edwards NC, Lip GY, Townend JN, Ferro CJ. Atrial Fibrillation in CKD: Balancing the Risks and Benefits of Anticoagulation. Am J Kidney Dis. 2013;62:615-632. 12. Reinecke H, Brand E, Mesters R, Schabitz WR, Fisher M, Pavenstadt H, Breithardt G. Dilemmas in the management of atrial fibrillation in chronic kidney disease. J Am Soc Nephrol. 2009;20:705-711. 13. Shen JI, Turakhia MP, Winkelmayer WC. Anticoagulation for atrial fibrillation in patients on dialysis: are the benefits worth the risks? Curr Opin Nephrol Hypertens. 2012;21:600-606. 14. Sood MM, Komenda P, Sood AR, Rigatto C, Bueti J. The intersection of risk and benefit: is warfarin anticoagulation suitable for atrial fibrillation in patients on hemodialysis? Chest.
7. Mega JL. A new era for anticoagulation in atrial fibrillation. N Engl J Med. 200111;1;;363665:5:5 101010525252--1054.
8. Chan KE,, Lazarus JM, Thadhani R, Hakim RM. Warfarin use associates with increased risk foor r stststrororokekeke iiin nn hhhemomomodidialysis patients with atrial fibbbrrir lllation. J Am SSococo NNepepephhrhrol. 2009;20:2223-2222233333.
9.9.. CCChah n KE,, LaL zzazarrrus JMJMJM, ThThhaaddhaanii RR,, HHHakiim m RMMM. AnAnntititicococoaagaguuulannnt and annntitippplaatatele et ussasaggge asssososociciciatata eses wwwititith h momomortrtalallitityy y amamonono ggg hehehemomomodididialalalysysysisss pppatattieeentn ss.s JJJ AAmAm SSSococc NNNepepe hhhroolol. 222000009;9;;202020::87772--8-881811.
10. Reynoldss JJJL,L,L, JJJoaoaoannnnnnidii esess AAAJ,, SSSkekekeppppp ererer JJJN,N,N, MMMccNaNaNairirr RR,, ScScSchuhuhurgrgrgerere s LJLJLJ, , PrPrProuououdfdfoooooot t t D,D,D, JJJaha nen-DeDechchenentt WW WWeieissssbebergrg PPLL SShahananahahann CMCM HuHumamann vavascsculularar ssmomootothh mumuscsclele ccelellsls uundnderergogo
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
16
2009;136:1128-1133.
15. To AC, Yehia M, Collins JF. Atrial fibrillation in haemodialysis patients: do the guidelines for anticoagulation apply? Nephrology (Carlton). 2007;12:441-447. 16. Winkelmayer WC, Liu J, Setoguchi S, Choudhry NK. Effectiveness and safety of warfarin initiation in older hemodialysis patients with incident atrial fibrillation. Clin J Am Soc Nephrol. 2011;6:2662-2668. 17. Wizemann V, Tong L, Satayathum S, Disney A, Akiba T, Fissell RB, Kerr PG, Young EW, Robinson BM. Atrial fibrillation in hemodialysis patients: clinical features and associations with anticoagulant therapy. Kidney Int. 2010;77:1098-1106. 18. Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, Demets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Wann LS, Curtis AB, Ellenbogen KA, Estes NA, III, Ezekowitz MD, Jackman WM, January CT, Lowe JE, Page RL, Slotwiner DJ, Stevenson WG, Tracy CM, Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Le Heuzey JY, Kay GN, Olsson SB, Prystowsky EN, Tamargo JL, Wann S. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:1935-1944. 19. Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De CR, De SJ, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace. 2010;12:1360-1420. 20. Camm AJ, Lip GY, De CR, Savelieva I, Atar D, Hohnloser SH, Hindricks G, Kirchhof P. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation--developed with the special contribution of the European Heart Rhythm Association. Europace. 2012;14:1385-1413. 21. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC, Jr., Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e257-e354.
Curtis AB, Ellenbogen KA, Le Heuzey JY, Kay GN, Olsson SB, Prystowsky EN, , TaTaTamamargrggoo JLJL, Wann S. Management of patients with atrial fibrillation (compilation of 2006 AACCCCCF/FF AHAHAHA/A/A/ESEESCand 2011 ACCF/AHA/HRS recommendations): a report of the American Collegege ooofff Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol.2013;6;61:1935-1949 4.
19199. CCaCamm AAAJJJ, KKiririrchchhohoof f f P,P,P, LLipipp GGGY,Y,Y SSchchotottetenn U,U, SSSaavveliievevevaaa I,I,I, EErnrnrnststt SS, VaVaVan n GeGeldldldererer IIC,C, AAAl-l-l AtAtAttatatar r NHHinndndricks G, PPrereenddderergggastsst BBB, , HeHeH ididdbububuchchhell H, AAAlfierrri O, AAAngnggelele inini ii AA,A, AAtataarr DD,D, CCCoololononnanan PP,, DeDeDe CCCRR,, DDDe SSSJ, Goettttee A, GGGoreeeneek BBB, HHHeldl alall MMM, Hohhhloooserrr SSSH,H, KKKolololh hh PPP, LLLe HHeuuzzeeyey JJJYY,Y, PPonnnikkkowowwsskki PPP, RuRuuttttt enenen FFH.H.. GGGuiuiddedellilineness ffofor r thhheee mamamanananagegememementntnt oof ff atata ririialall fibibbriririllllllataatiooon:n:n tthehehe TTTaaaskk k FoFoorcrcrceee fofoor r tthee e Maananageg mementn oof f Attririalal Fibibrrilllatatioion n of thee EuEuroropeeana SSococieietyty oof f CaCardrdioiolologyy ((ESESC)C). Euuroropaacece.2010;12:1360600-1-11424220.0.0.
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
17
22. Herzog CA, Asinger RW, Berger AK, Charytan DM, Diez J, Hart RG, Eckardt KU, Kasiske BL, McCullough PA, Passman RS, DeLoach SS, Pun PH, Ritz E. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011;80:572-586. 23. Skanes AC, Healey JS, Cairns JA, Dorian P, Gillis AM, McMurtry MS, Mitchell LB, Verma A, Nattel S. Focused 2012 update of the Canadian Cardiovascular Society atrial fibrillation guidelines: recommendations for stroke prevention and rate/rhythm control. Can J Cardiol. 2012;28:125-136. 24. Avgil TM, Jackevicius CA, Rahme E, Humphries KH, Behlouli H, Pilote L. Sex differences in stroke risk among older patients with recently diagnosed atrial fibrillation. JAMA. 2012;307:1952-1958. 25. Pilote L, Eisenberg MJ, Essebag V, Tu JV, Humphries KH, Leung Yinko SS, Behlouli H, Guo H, Jackevicius CA. Temporal Trends in Medication Use and Outcomes in Atrial Fibrillation. Can J Cardiol. 2013;29:1241-1248. 26. Cattaruzzi C, Troncon MG, Agostinis L, Garcia Rodriguez LA. Positive predictive value of ICD-9th codes for upper gastrointestinal bleeding and perforation in the Sistema Informativo Sanitario Regionale database. J Clin Epidemiol. 1999;52:499-502. 27. Goldstein LB. Accuracy of ICD-9-CM coding for the identification of patients with acute ischemic stroke: effect of modifier codes. Stroke. 1998;29:1602-1604. 28. Henderson T, Shepheard J, Sundararajan V. Quality of diagnosis and procedure coding in ICD-10 administrative data. Med Care. 2006;44:1011-1019. 29. Kirkman MA, Mahattanakul W, Gregson BA, Mendelow AD. The accuracy of hospital discharge coding for hemorrhagic stroke. Acta Neurol Belg. 2009;109:114-119. 30. Liu L, Reeder B, Shuaib A, Mazagri R. Validity of stroke diagnosis on hospital discharge records in Saskatchewan, Canada: implications for stroke surveillance. Cerebrovasc Dis. 1999;9:224-230. 31. Jackevicius CA, Paterson JM, Naglie G. Concordance between discharge prescriptions and insurance claims in post-myocardial infarction patients. Pharmacoepidemiol Drug Saf. 2007;16:207-215. 32. Levy AR, O'Brien BJ, Sellors C, Grootendorst P, Willison D. Coding accuracy of administrative drug claims in the Ontario Drug Benefit database. Can J Clin Pharmacol. 2003;10:67-71. 33. Tamblyn R, Lavoie G, Petrella L, Monette J. The use of prescription claims databases in pharmacoepidemiological research: the accuracy and comprehensiveness of the prescription claims database in Quebec. J Clin Epidemiol. 1995;48:999-1009.
26. Cattaruzzi C, Troncon MG, Agostinis L, Garcia Rodriguez LA. Positive prededdiciictititiveee vvalalalueueue oof CD-9th codes for upper gastrointestinal bleeding and perforation in the Sistema a InInnfofoformrmmatatativiivoo
Sanitario Regionale database. J Clin Epidemiol. 1999;52:499-502.
277. . GoGoGoldldldstststeieieinnn LBBB.. AAccuracy of ICD-9-CM codinnng gg fffor the identifiicacc tiononn ooof f patients with acute sschchcheemic strtrokokoke:e: eeefffff ecect t ofofof mmmododififfieieier r r cocodedes.s. StStrorokeke. 19998;8;;292929:1:1:1606 2-2-2-16161 0404.
28288. HHeH ndersoson n TT,T, SSShephphheardrdd JJJ, , SuSundnddararrarrrajannn VVV. QQuQualalititty yy ofofof diiagnnnoossis aandndnd pprrorocecec durrre ccooddiinng iiin CCCD-D-D-101010 aadmdmminiinisistttraatativiveee ddadatata. MeMeMeddd CaCaCareree.. 2220000006;6;444444:1:1100111--10100191919.
29. Kirkman n MAMAMA, , MaMaM hahahattanananakakakululul WWW,, GrGrregegegsososon n n BABABA,, MeMeM ndnddelelelowowow AAAD.DD TTThehehe aaaccccccururu acaccy y y ofofof hhhoso pital didiscschahargrgee cocodidingng fforor hhememororrhrhagagicic sstrtrokokee AcActata NNeueuroroll BeBelglg 2200009;9;10109:9:111144-111199
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
18
34. Zhou Z, Rahme E, Abrahamowicz M, Pilote L. Survival bias associated with time-to-treatment initiation in drug effectiveness evaluation: a comparison of methods. Am J Epidemiol. 2005;162:1016-1023. 35. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864-2870. 36. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33:1500-1510. 37. Olesen JB, Lip GY, Hansen PR, Lindhardsen J, Ahlehoff O, Andersson C, Weeke P, Hansen ML, Gislason GH, Torp-Pedersen C. Bleeding risk in 'real world' patients with atrial fibrillation: comparison of two established bleeding prediction schemes in a nationwide cohort. J Thromb Haemost. 2011;9:1460-1467. 38. Newell DJ. Intention-to-Treat Analysis: Implications for Quantitative and Qualitative Research. Int J Epidemiol. 1992;21:837-841. 39. D'Agostino RB, Jr. Propensity scores in cardiovascular research. Circulation. 2007;115:2340-2343. 40. Cepeda MS, Boston R, Farrar JT, Strom BL. Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. Am J Epidemiol. 2003;158:280-287. 41. Deeks JJ, Altman DG, Bradburn MJ. Statistical Methods for Examining Heterogeneity and Combining Results from Several Studies in Meta-Analysis. Systematic Reviews in Health Care. BMJ Publishing Group; 2001:285-312. 42. Marinigh R, Lane DA, Lip GY. Severe renal impairment and stroke prevention in atrial fibrillation: implications for thromboprophylaxis and bleeding risk. J Am Coll Cardiol. 2011;57:1339-1348. 43. Baumann M, Seifert CL, Poppert H. Atrial fibrillation and chronic kidney disease. N Engl J Med. 2012;367:2157-2158. 44. Schlieper G, Kruger T, Floege J. Atrial fibrillation and chronic kidney disease. N Engl J Med. 2012;367:2157-2159. 45. Sood MM, Tangri N. Atrial fibrillation and chronic kidney disease. N Engl J Med. 2012;367:2158-2159. 46. Babyak MA. What you see may not be what you get: a brief, nontechnical introduction to overfitting in regression-type models. Psychosom Med. 2004;66:411-421.
38. Newell DJ. Intention-to-Treat Analysis: Implications for Quantitative and Qualalitititatata iviveemResearch. Int J Epidemiol. 1992;21:837-841.
39. D'Agostino RB, Jr. Propensity scores in cardiovascular research. Circulation.2007;1; 15:2340-2343.
40400. CCeCepeda MMMS,S, BBBosostoton nn R,R,R, FFararrarararrr JTJT, , , StStrorom m BLBL. CoCoCompparararisisisonono ooff f lolologigig ststicicc rreggreressssssioioion n veversrssususu propppensity scoorere wwwhehennn ththhe ee nununumbmmbererr ooof f eeveveentsss iss lowww anddd tththererre arareee mmumultltipipipllee cconononfofoununndededersrs. AmAmAm JJJ EpEpEpidddemiol. 22000 3;;158:28280-2828877.7.
41. DeDe kekss JJJ , AlAltmmanan DG,G, Braradbdbuurn MJJ. StStatatisistiticac l MeMeththodods s fofor ExExamamininngg HeHeteterogegenen itity y anand dCombining ReReesusuultlttsss frfrf omomom SSSeveveverere alalal SStututudiiiesese iiin n n MeMeMetataa-A-AAnanan lyyysisisis.s.s SySySystststememematata icicic RRRevevevieiei wswsws iiin n n HeHeHealth Care. BMBMJJ PuPublblisishihingng GGroroupup;; 20200101:2:28585 3-31212
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
19
47. Ionescu-Ittu R, Abrahamowicz M, Jackevicius CA, Essebag V, Eisenberg MJ, Wynant W, Richard H, Pilote L. Comparative effectiveness of rhythm control vs rate control drug treatment effect on mortality in patients with atrial fibrillation. Arch Intern Med. 2012;172:997-1004. 48. Fewell Z, Davey SG, Sterne JA. The impact of residual and unmeasured confounding in epidemiologic studies: a simulation study. Am J Epidemiol. 2007;166:646-655. 49. Walker AM. Confounding by indication. Epidemiology. 1996;7:335-336. 50. Normand SL, Sykora K, Li P, Mamdani M, Rochon PA, Anderson GM. Readers guide to critical appraisal of cohort studies: 3. Analytical strategies to reduce confounding. BMJ. 2005;330:1021-1023.
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
20
Table 1. Baseline Characteristics of Patients with Atrial Fibrillation
Dialysis Patients, N = 1,626
Non-dialysis Patients, N = 204,210
Warfarin users,N = 756
No-warfarinusers, N = 870
Warfarin users, N = 103,473
No-warfarinusers, N = 100,737
Patients diagnosed with AF: AF as a main diagnosis, n (%) 150 (20) 125 (14) 34,710 (34) 19,802 (20) Age at the index AF admission in years, mean ± SD* 75.3 ± 8.1 75.1 ± 8.5 77.9 ± 9.5 78.8 ± 10.6 Male sex, n (%) 459 (61) 533 (61) 49,133 (48) 50,425 (50) Length of hospitalization in days, mean ± SD* 19.4 ± 37.2 21.1 ± 44.5 10.4 ± 20.9 10.5 ± 24.0 Co-morbidities, n (%): Coronary artery disease 470 (62) 517 (59) 40,163 (39) 40,199 (40) Acute myocardial infarction 201 (27) 249 (29) 15,489 (15) 16,413 (16) Valvular heart disease 131 (17) 115 (13) 15,633 (15) 10,140 (10) Liver disease 28 (4) 33 (4) 1,792 (2) 2,413 (2) History of bleeding event 65 (9) 139 (16) 4,680 (5) 9,042 (9) Specific components of CHADS2 score†, n (%):
Congestive heart failure 312 (41) 299 (34) 33,659 (33) 27,494 (27) Hypertension 582 (77) 655 (75) 47,972 (46) 41,738 (41) Age 75 years 386 (51) 415 (48) 65,333 (63) 65,814 (65) Diabetes 330 (44) 340 (39) 21,574 (21) 19,756 (20) History of stroke/TIA 42 (6) 44 (5) 9,464 (9) 5,283 (5) CHADS2 score†, n (%): Low risk (0) 23 (3) 59 (7) 11,870 (11) 14,308 (14) Moderate risk (1) 153 (20) 215 (25) 31,533 (30) 34,450 (34) High risk ( 2) 580 (77) 596 (69) 60,070 (58) 51,979 (52) HAS-BLED score‡, n (%): Low and moderate risk§ (1-2) 119 (16) 126 (14) 80,747 (78) 73,260 (73) High risk ( 3) 637 (84) 744 (86) 22,726 (22) 27,477 (27) First filled prescription within 30 days after AF discharge, n (%): Rate control drugs 519 (69) 462 (53) 75,656 (73) 55,167 (55) Rhythm control drugs 203 (27) 172 (20) 23,512 (23) 16,508 (16) Aspirin 166 (22) 241 (28) 11,814 (11) 24,544 (24) Clopidogrel 30 (4) 58 (7) 1,843 (2) 4,158 (4) NSAIDs 8 (1) 20 (2) 2,109 (2) 3,336 (3) Abbreviations: AF, atrial fibrillation; SD, standard deviation; TIA, transient ischemic attack; NSAIDs, non-steroidal anti-inflammatory drugs; Results are weighted average for results from Quebec and Ontario. We presented continuous variables as mean ± SD and dichotomous variables as number (%). *We used following formula to combine standard deviation: SDcombined = (SD1)2+(SD2)2. †CHADS2 score is a clinical prediction score for estimating the risk for stroke. ‡HAS-BLED score is a clinical prediction score for estimating the risk for bleeding. §HAS-BLED score has minimum score of one and two for non-dialysis patients and dialysis patients, respectively. In this study, all AF patients are age 65 years, which accounts for one point. In dialysis group, all patients have abnormal renal function, which also accounts for one point.
Liver disease 28 (4) 33 (4) 1,792 (2) 2,2,414133 (2(2) History of bleeding event 65 (9) 139 (16) 4,680 (5) 9,9,9 0404042 2 2 ((9(9)
Specific components of CHADS2 score†, n (%):
Congestive heart failure 312 (41) 299 (34) 33,659 (33) 27,494 (27) HyHyypepepertrtrtenenensisisiononon 582 (77) 655 (75) 47,9,9972722 (46) 41,738 (41) AAgAgee e 75 yeyearaars 338686 ((5151)) 4155 (4(4( 8)8)) 65,5,333333 (63)3) 665,5,818 4 (6(65) DDiDiaaabetes 33333000 (444) 34000 (((39399) )) 2121,5,5,5744 ((212121)) ) 19191 ,7,7,7565656 ((2202 ) HHiH sststory of strtrokee/e/TTTIA 4242 (66) 44 4 4 (5(5(5))) 9,444644 (9(99) 5,2833 (555)
CHCHHADADADSS22 scscorororee††, nnn ((%(%)):: Loow w riiri ksksk ((0)0 23 (3(33)) ) 5959 (((7)7) 111,1,878700 (1(11)1) 114,4,30308 8 (1(14)4) Moderate rissk k k (1(11) ) 1515153 (2(2( 0)0)0) 2221515 (((252525) ) ) 313131,5,5,5333333 (((30303 ) ) 34,450 (34))) HiHighgh rrisiskk (( 22)) 585800 (7(77)7) 559696 ((6969)) 6060 007070 ((5858)) 5151 997979 ((5252)))
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
21
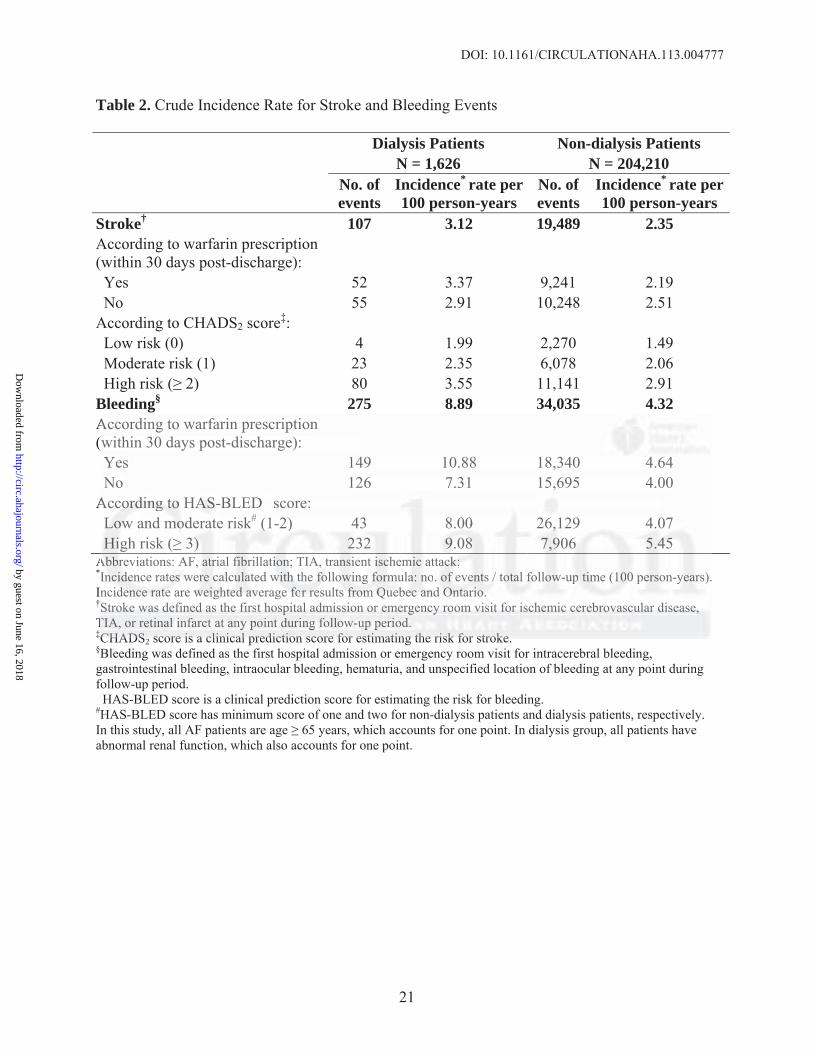
Table 2. Crude Incidence Rate for Stroke and Bleeding Events
Dialysis Patients Non-dialysis Patients N = 1,626 N = 204,210
No. of events
Incidence* rate per 100 person-years
No. ofevents
Incidence* rate per 100 person-years
Stroke† 107 3.12 19,489 2.35According to warfarin prescription (within 30 days post-discharge): Yes 52 3.37 9,241 2.19 No 55 2.91 10,248 2.51 According to CHADS2 score‡: Low risk (0) 4 1.99 2,270 1.49 Moderate risk (1) 23 2.35 6,078 2.06 High risk ( 2) 80 3.55 11,141 2.91 Bleeding§ 275 8.89 34,035 4.32According to warfarin prescription (within 30 days post-discharge): Yes 149 10.88 18,340 4.64 No 126 7.31 15,695 4.00 According to HAS-BLED� score: Low and moderate risk# (1-2) 43 8.00 26,129 4.07 High risk ( 3) 232 9.08 7,906 5.45 Abbreviations: AF, atrial fibrillation; TIA, transient ischemic attack; *Incidence rates were calculated with the following formula: no. of events / total follow-up time (100 person-years). Incidence rate are weighted average for results from Quebec and Ontario. †Stroke was defined as the first hospital admission or emergency room visit for ischemic cerebrovascular disease, TIA, or retinal infarct at any point during follow-up period. ‡CHADS2 score is a clinical prediction score for estimating the risk for stroke. §Bleeding was defined as the first hospital admission or emergency room visit for intracerebral bleeding, gastrointestinal bleeding, intraocular bleeding, hematuria, and unspecified location of bleeding at any point during follow-up period. �HAS-BLED score is a clinical prediction score for estimating the risk for bleeding. #HAS-BLED score has minimum score of one and two for non-dialysis patients and dialysis patients, respectively. In this study, all AF patients are age 65 years, which accounts for one point. In dialysis group, all patients have abnormal renal function, which also accounts for one point.
According to warfarin prescription within 30 days post-discharge): Yes 149 10.88 18,340 4.64 No 126 7.31 15,695 4.00
Accocoordrdrdinining g g tototo HASASAS-B-BLED� score: LoLLowww ana d momomodeeraratete rrisskk# (((1-1-2)2) 4433 8.8.0000 226,6,,121 9 4.4.0707 HiHiiggh risk ( 33) )) 22232 9.9..08088 777,999066 55.444555
AbAbA brrreve iations: AAF, aatrrrial ffifibrrillaatitiiononn; TTIAIA, , trtraannssiient iisccchemmicc attacacck;k;k;InInncicc dededencnce raratetees s wewerrre ccalalcucuulaaateed d wwiwithhh tthehe fffoloollooowiwingng ffforrmumulalaa: nnno. ofoff eeveveenttss / / totootaaal l fofof llllowoww-u-uppp tiimemem ((11010000 peeerssonon-y-yeaarrs).nncic dededencncncee e rararatetete aarere wwweieieighghghteteteddd avavavereragge e e fofoforr r rreresusultts s frfrfromomom QQQuueuebebebeccc ananand d OnOnOntatatariririoo.o. StStStrororokekeke wwwasasas dddefefefinininededed aaasss thththeee fififirsrsrsttt hohohospspspitititalalal aaadmdmdmisisissisisiononon ooorrr emememererergegegencncncyyy rororoomomom vvvisisisititit fffororor iiiscscschehehemimimiccc cececerererebrbrbrovovovasasascucuculalalarrr dididiseseseasasasee,e,
TIA, or retinall inininfafafarcrcr tt t atatat aanynyny ppoioiintntnt dddurrrinininggg fofofolll owowow-u-uuppp pepeperirir ododod..CHCHADADSS sscocorere iiss aa clclininicicalal ppreredidictctioionn scscororee foforr esestitimamatitingng tthehe rrisiskk foforr ststrorokeke
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCULATIONAHA.113.004777
22
Table 3. Association between Warfarin Use and the Risk for Stroke and Bleeding in Patients with Atrial Fibrillation
Patients with AF Outcomes Adjusted* HR (95% CI)
Propensity Score†
Adjusted HR (95% CI) Dialysis (n = 1,626) Stroke‡ 1.14 (0.78, 1.67) 1.17 (0.79, 1.75)
Bleeding§ 1.44 (1.13, 1.85) 1.41 (1.09, 1.81) Non-dialysis (n = 204,210) Stroke‡ 0.87 (0.85, 0.90) 0.89 (0.87, 0.92)
Bleeding§ 1.19 (1.16, 1.22) 1.20 (1.17, 1.23) Abbreviations: AF, atrial fibrillation; HR, Hazard Ratio; CI, Confidence Interval; TIA, transient ischemic attack; NSAIDs, non-steroidal anti-inflammatory drugs; *Stroke outcome was adjusted for: age (years), sex, specific components of CHADS2 stroke prediction score (congestive heart failure, hypertension, diabetes, and history of stroke/TIA). *Bleeding outcome was adjusted for: age (years), sex, specific components of HAS-BLED bleeding prediction score (liver disease, hypertension, history of stroke/TIA, history of bleeding, and use of aspirin, clopidogrel, or NSAIDs). †Propensity score was derived from the following variables: age 75 years, sex, type of AF (primary vs. secondary), CHADS2 scores (1 and 2), liver disease, congestive heart failure, hypertension, diabetes, history of stroke/TIA, history of bleeding, use of rate control drug, rhythm control drug, aspirin, clopidogrel, and NSAIDs. ‡Stroke was defined as the first hospital admission or emergency room visit for ischemic cerebrovascular disease, TIA, or retinal infarct at any point during follow-up period. §Bleeding was defined as the first hospital admission or emergency room visit for intracerebral bleeding, gastrointestinal bleeding, intraocular bleeding, hematuria, and unspecified location of bleeding at any point during follow-up period.
Figure Legends:
Figure 1. Warfarin Use and the Risk for Stroke in Patients with Atrial Fibrillation Undergoing
Dialysis. Abbreviations: HR, Hazard Ratio; LCL, Lower Confidence Limit; UCL, Upper
Confidence Limit; TIA, transient ischemic attack; Chan et al. defined stroke outcome as
hospitalization or death from ischemic stroke, hemorrhagic stroke, or TIA.8 45% (747/1,671)
patients were receiving warfarin.8 Wizemann et al. defined stroke outcome as hospitalization or
death from stroke or cerebrovascular event.17 15% (146/1,001) patients, 17% (192/1,137)
patients, and 15% (171/1,107) patients in age group 65 years, 66 to 75 years, and > 75 years
were receiving warfarin, respectively.17 Winkelmayer et al. defined stroke outcome as ischemic
or hemorrhagic stroke.16 11% (249/2,313) patients were receiving warfarin.16 237 warfarin users
y g, g, y g, p , p g ,Stroke was defined as the first hospital admission or emergency room visit for ischemic cerebrovvvasasascucuculalalarr r dididiseseseasasase,e,e
TIA, or retinal infarct at any point during follow-up period. Bleeding was defined as the first hospital admission or emergency room visit for intracerebral bbleleedededinining,g
gastrointestinal bleeding, intraocular bleeding, hematuria, and unspecified location of bleeding at any point during ollow-up period.
g re Legen : FFiguure Legends:
Figure 1. WaWaWarfrfrfarararinini UUUsese aandndnd tttheh RRRisiskk k foforr StStrorokekeke iinn PaPaPatitienentsts wwititth hh AtAttriririalalal FFFibibibririllllatattioion n UnUnUnderggoingg
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCULATIONAHA.113.004777
23
were matched to 948 non-users.16 Olesen et al. defined stroke outcome as hospitalization or
death from stroke or systemic thromboembolism (ischemic stroke, peripheral artery embolism,
and TIA).1 20% (178 / 901) patients were receiving warfarin only.1 Our study defined stroke as
the first hospital admission or emergency room visit for ischemic cerebrovascular disease, TIA,
or retinal infarct at any point during follow-up period. 46% (756/1,626) patients were receiving
warfarin.
Figure 2. Warfarin Use and the Risk for Bleeding in Patients with Atrial Fibrillation Undergoing
Dialysis. Abbreviations: HR, Hazard Ratio; LCL, Lower Confidence Limit; UCL, Upper
Confidence Limit; GI, Gastrointestinal; Winkelmayer et al. defined bleeding outcome as GI
bleeding.16 11% (249/2,313) patients were receiving warfarin.16 237 warfarin users were matched
to 948 non-users.16 Olesen et al. defined bleeding outcome as hospitalization or death from GI,
intracranial, urinary tract, and air-way bleeding.1 20% (178/901) patients were receiving warfarin
only.1 Our study defined bleeding outcome as the first hospital admission or emergency room
visit for intracerebral bleeding, GI bleeding, intraocular bleeding, hematuria, and unspecified
location of bleeding at any point during follow-up period. 46% (756/1,626) patients were
receiving warfarin.
Confidence Limit; GI, Gastrointestinal; Winkelmayer et al. defined bleeding outctccommmee asasas GGGI I I
bleeding.16 11% (249/2,313) patients were receiving warfarin.16 237 warfarin users were matched
oo 999484848 nnnononn-u-ussserss..16616 OlO esen et al. defined bleedinnng g g oouutcome as hosspipp taaliliizazazatit on or death from GI,
nntrraaca ranial, ururinininarrry trtrracaccttt, aaandndnd aairir-w-w-wayay bblleedddinnng.1 22000% (((11717888/990901)1)) ppatatieiennntsss weweerrere rrececceieieivivivinngng wwaararfafafarin
onnlylyly.11 OuOuO rr stststududyy y dedeefifinnnedd d blb eeeedidiingngng oooututccocomememe aas s thththeee fifiirsr tt t hohohospspspittalalal aaadmdmmisisi ssiionnn oorr r ememmererrgegegencccyy roroomomm
visit for intracaccerererebebbrararal l blblbleee dididingngng, GIGIGI bbblell edededininng,g,g, iiintntntrraoaoaocucuculal r r r blblbleeeeeedididingngng,, hehehemamamatututuririria,a,a aaandndnd uuunsnsnspepp cified
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

Figure 1
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from
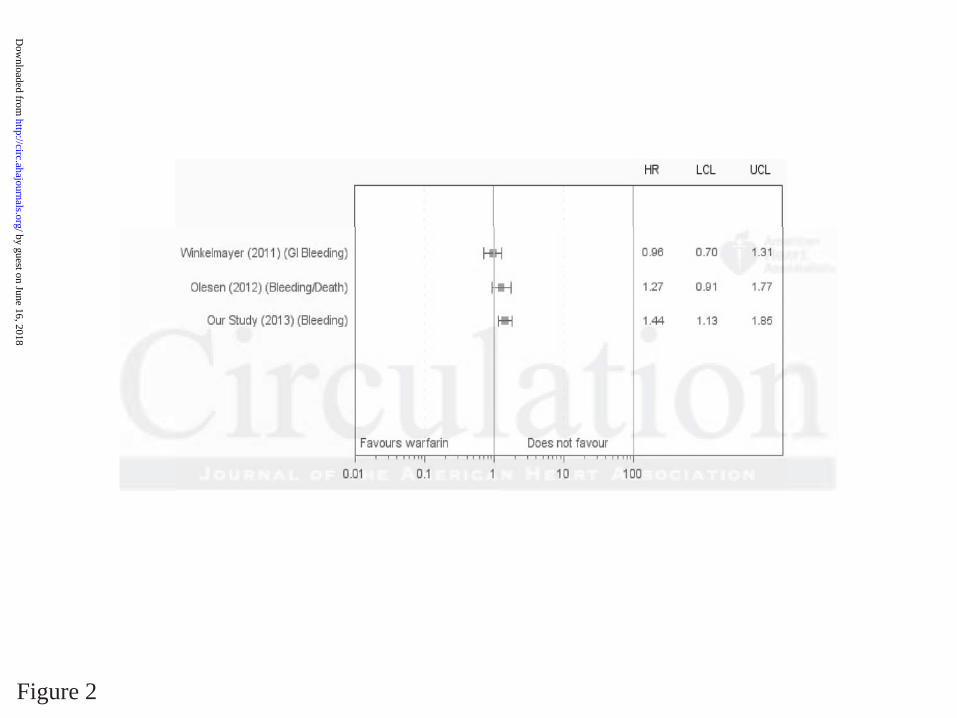
Figure 2
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

Rahme, Karin H. Humphries, Jack V. Tu, Hassan Behlouli, Helen Guo and Louise PiloteMitesh Shah, Meytal Avgil Tsadok, Cynthia A. Jackevicius, Vidal Essebag, Mark J. Eisenberg, Elham
Undergoing DialysisWarfarin Use and the Risk for Stroke and Bleeding in Patients with Atrial Fibrillation
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online January 22, 2014;Circulation.
http://circ.ahajournals.org/content/early/2014/01/22/CIRCULATIONAHA.113.004777World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2014/01/22/CIRCULATIONAHA.113.004777.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 16, 2018http://circ.ahajournals.org/
Dow
nloaded from

1
SUPPLEMENTAL MATERIAL
Supplemental Table 1. Databases in Quebec and Ontario
Data Type Quebec, Canada Ontario, Canada
Hospital
Discharges
Maintenance et Exploitation des
Données pour l’Étude de la Clientèle
Hospitalière (Med-Echo)
Canadian Institute for Health
Information (CIHI)
Physician
Claims
la Régie de l’assurance maladie du
Québec (RAMQ)
Ontario Health Insurance Plan
Prescription
Claims
RAMQ Ontario Drug Benefit Plan
Vital Status Med-Echo & RAMQ Ontario Registered Persons and
CIHI Databases
2
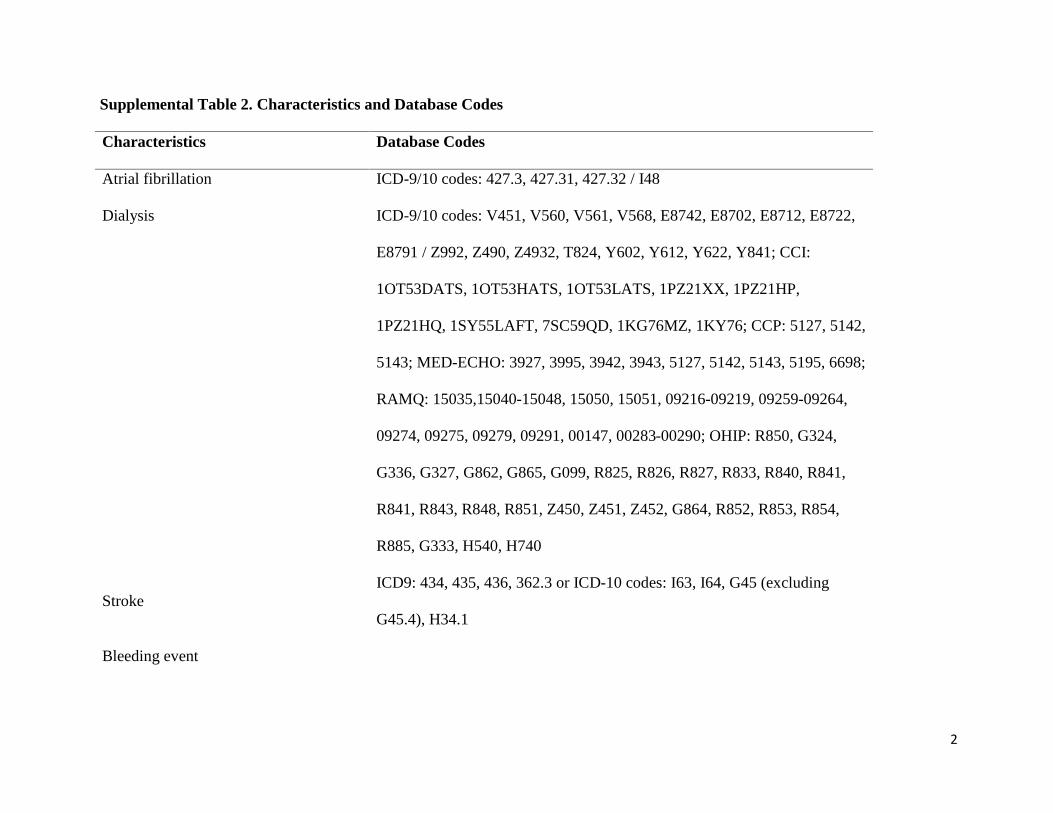
Supplemental Table 2. Characteristics and Database Codes
Characteristics Database Codes
Atrial fibrillation ICD-9/10 codes: 427.3, 427.31, 427.32 / I48
Dialysis ICD-9/10 codes: V451, V560, V561, V568, E8742, E8702, E8712, E8722,
E8791 / Z992, Z490, Z4932, T824, Y602, Y612, Y622, Y841; CCI:
1OT53DATS, 1OT53HATS, 1OT53LATS, 1PZ21XX, 1PZ21HP,
1PZ21HQ, 1SY55LAFT, 7SC59QD, 1KG76MZ, 1KY76; CCP: 5127, 5142,
5143; MED-ECHO: 3927, 3995, 3942, 3943, 5127, 5142, 5143, 5195, 6698;
RAMQ: 15035,15040-15048, 15050, 15051, 09216-09219, 09259-09264,
09274, 09275, 09279, 09291, 00147, 00283-00290; OHIP: R850, G324,
G336, G327, G862, G865, G099, R825, R826, R827, R833, R840, R841,
R841, R843, R848, R851, Z450, Z451, Z452, G864, R852, R853, R854,
R885, G333, H540, H740
StrokeICD9: 434, 435, 436, 362.3 or ICD-10 codes: I63, I64, G45 (excluding
G45.4), H34.1
Bleeding event

3
Intracerebral hemorrhage ICD-9/10 codes: 431, 432 / I61
Gastrointestinal hemorrhage
ICD-9/10 codes: 578 (main code), 530.7, 531.0, 531.2, 531.4, 531.6, 532.0,
532.2, 532.4, 532.6, 533.0, 533.2, 533.4, 533.6, 534.0, 534.2, 534.4, 534.6 /
K92.0, K92.1, K92.2, (1st 3 are main codes) K25.0, K25.2,K25.4, K25.6 ,
K26.0, K26.2, K26.4, K26.6 , K27.0, K27.2, K27.4, K27.6, K28.0, K28.2,
K28.4, K28.6, K29.0
Intraocular hemorrhage ICD-9/10 codes: 362.8, 379.2 / H43.1, H35.6
Hematuria ICD-9/10 codes: 599.7 / N02, R31
Hemorrhage not other specified (NOS) ICD-9/10 codes: 459 / na







