

WHAT’SWHAT’S UNDER YOUR SKIN?UNDER YOUR SKIN?
Skin Care of Breast Cancer Patients Undergoing Standard External
Beam RadiationDonna M. Braunreiter RN BSN OCN
MSN Student Alverno College
Spring 2009, MSN 621dmbraunreiter @ aol.com
dmbraunreiter @ wi.rr.com

Objectives 1. Explain effects of external beam radiation
therapy.2. Briefly describe genetic mechanisms involved
in radiation.3. Summarize the acute physiologic
mechanisms of inflammation.4. Describe the structure and function of skin. 5. Identify breast skin changes after radiation
treatment.6. Review nursing care for breast cancer
patients undergoing radiation therapy.
DirectionsTo move to the next slide, click this
To move to the previous slide, click this
To return to the beginning, click this
To return to the topics section, click this

RADIATION
GENETICS
INFLAMMATION
SKIN STRUCTURE AND FUNCTION
BREAST SKIN CHANGES
NURSING CARE AND PATIENT EDUCATION

RADIATION
Microsoft Office Clip Art 2007
Radiation Treatment
• Skin reaction is the most common side effect during breast cancer radiation treatments
• Over 90% of women receiving radiation for breast cancer will develop some skin changes during their course of treatment

Radiation
• Interacts with all biological materials in its path
• Direct and indirect damage to cells causes DNA changes
• Causes many molecular responses that induce cellular mechanisms for DNA repair, cell cycle arrests, and apoptosis
Radiation
• Major effect on dividing cells is reproductive death
• Leaves cells unable to reproduce • Radiosensitivity of cell determines degree of
injury and when it will happen

Radiation Direct Effect
• DNA absorbs radiation • The atoms become ionized and damaged • Less common than indirect damage
Microsoft Office Clip Art 2007

Radiation Indirect Effect
• Water molecules surrounding DNA are ionized • Creates highly reactive free radicals such as
hydroxyl radicals, peroxide, hydrated electrons, and oxygen radicals
• These radicals interfere with DNA and cause damage and strand breakage
• Common because 80% of a cell is water

Radiation Damage
• Direct and indirect damage break bonds in DNA backbone
• Results in loss of base, nucleotide, or one or both strands of DNA
• Single-strand DNA breaks are repaired using the opposite strand as a template
• Can result in mutation if not repaired correctly
Radiation Damage
• Double-strand DNA breaks related to cell killing• Results in mitotic death• X-rays are sparsely ionizing and cause
locally clustered damage • Leads to clinically significant
events
DNA Structure
United States National Library of Medicine http://ghr.nlm.nih.gov/handbook/illustrations.dnastructure.jpg

Radiation
CONTROLS CANCER CELLS BY
1.Inducing apoptosis2.Causing permanent cell cycle arrest or
terminal differentiation 3.Inducing cells to die of mitotic catastrophe

Apoptosis
• Programmed cell death• Radiation damage triggers signaling cascades
which causes cell self-destruct mechanisms• Characteristics are nucleus fragmentation and
blebbing • Tumors undergoing apoptosis have good
clinical response
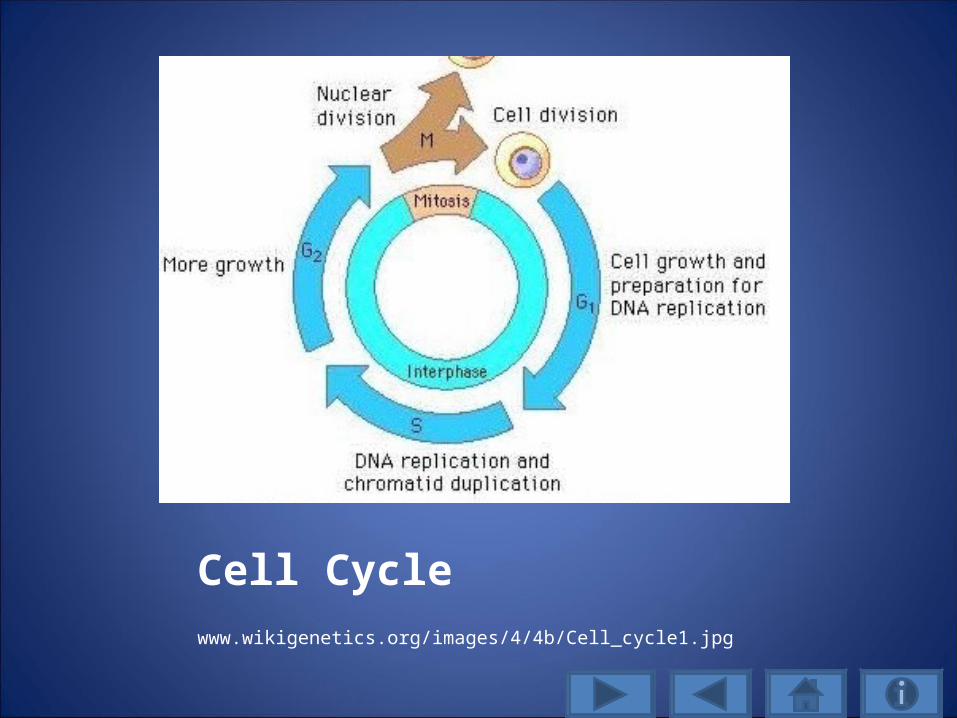
Cell Cycle www.wikigenetics.org/images/4/4b/Cell_cycle1.jpg

Cell Cycle Death/Terminal Differentiation (Denucleation)
• Cells can arrest in any phase of cell cycle• Radiation damage mainly in G1 and G2 phases• Normal cells and cancer cells retaining p53
function block in G1• Cancer cells with p53 loss or mutation block in
G2 phase• G2 arrest related to cellular repair of DNA
radiation-induced DNA damage
Radiation Effects
Radiosensitive
• Cells renewing rapidly with little or no differentiation
• Examples are skin cells, mucous membranes, and hematopoietic stem cells
Radioresistant
• Cells that do not divide regularly or at all and are highly differentiated
• Examples are muscle cells and nerve cells

Radiation Effects
Radiosensitive• Acute effects• Damage within weeks to
months of exposure• Temporary• Normal cells affected are
capable of repair• Dependent upon dose-time-
volume factors
Radioresistant• Late effects• Damage months or years
after first exposure• Permanent• Damage becomes more
severe as time goes on• Dependent upon dose-time-
volume factors

Radiation Effects
Radiosensitive• Higher doses over shorter
periods of time to larger volumes of tissues result in more severe acute reactions
• Acute damage results from depletion of actively proliferating parenchymal or stromal cells
• Characteristics are vascular dilation, local edema, and inflammation
Radioresistant• Severity of late effects more
dependent upon total dose delivered and volume if tissue irradiated
• Damage to endothelial cells or connective tissues results in late effects occurring as a result of narrowing or occlusion of small vasculature and fibrosis

Radiation Effects
• Acute and late side effects from radiation therapy are LOCAL and ONLY affect tissues receiving treatment
• Presence and severity of acute effects can not predict late effects of radiation
• Late reactions such as tissue necrosis or dense tissue fibrosis can occur independently of acute reactions

SUPINE POSITION• Most common position for breast cancer
radiation therapy• MUST be used if lymph nodes need to be
treated• May involve radiation exposure to heart,
lungs, ribs, and contralateral breast
Microsoft Office Clip Art 2007

PRONE POSITION• Used for women with larger pendulous breast,
cardiac and/or pulmonary comorbidities• Possible improved dose homogeneity• Potential reduction in lung and heart
irradiation
Microsoft Office Clip Art 2007
Patient-Related Considerations
Normal age-related changes: • thinning of the epidermis and dermis, • diminished elasticity, • decreased dermal turgor, which results in delayed healing. Nutritional status is also important for healing.
What is the effect of radiation on cells?
A. Reproductive death of cells throughout the body
C. Radiation skin reactions cause internal injuries.
D. Radiation helps repair DNA damage.
B. Reproductive death of cells in the treated area only

Wrong answer, try again.
Radiation only affects the area being treated and causes damage to DNA.
Click here to return to question

Correct! Radiation causes the reproductive death of cells in the
treated area only.

GENETICS
Microsoft Office Clip Art 2007

Chromosome:rod-shaped molecule of DNA threaded around proteins containing
specific genes that carry hereditary informationHistones are proteins that act as spools around which DNA winds, as
compaction is necessary to large genes inside cell nuclei; histones also function as gene regulators
United States National Library of Medicine http://ghr.nlm.nih.gov/handbook/illustrations/chromosomestructure.jpg

GENE: biological unit of hereditary; segment of DNA needed to contribute to a function and specifies a trait
United States Library of Medicine http://ghr.nlm.nih.gov/handbook/illustrations/geneinchromosome.jpg
Radiation effect on genes
1. Ionizing radiation causes phosphorylation of histone H2AX (forming gamma-H2AX)
2. Reaction dependent on ataxia telangiectesia mutated (ATM) molecule
3. Followed by accumulation of 53BP1, a protein acting as central mediator for critical pathways, including phosphorylating (which conveys the DNA damage signal to) tumor suppressor protein p53

Genetics in Radiation
4. Next, phosphorylating the ATM protein amplifies the damage signal
5. And recruits proteins critical for repair, such as the BRCA1 and HDAC4
6. Which allows a G2 cycle checkpoint7. 53BP1 important in double-strand DNA
damage sensing, repair, and tumor suppression

Genetics in Radiation
• HR (homologous repair) efficient in late S or G2 phase when sister chromatids have replicated but not separated
• Repair is cell cycle dependent• Undamaged homologous chromosome or
sister chromatid or replicated chromosome is used as a template to fill in missing DNA sequences in damaged chromosome

Genetics in Radiation
• Human tumor cells block in G2 after DNA double-strand damage, when repairs are detectible, and irradiation induced G2 checkpoint allows more time for cells to undergo HR (homologous repair) and survive radiation

Genetics in Radiation
• NHEJ (nonhomologous endjoining) is where blunt ends of chromosomes severed by radiation are directly rejoined
• Less cell cycle dependent• Highly mutagenic due to template-free
rejoining lacks specificity of HR• Ends of different chromosomes can be
rejoined, leading to chromosomal aberrations or expression of dangerous fusion proteins

p53 Tumor Suppressor Gene• p53 stops activity of tumors • Loss or mutation of p53 predisposes to cancer (e.g. inheriting only one functional copy of p53
gene from parents)• p53 protein binds DNA and stimulates another
gene to produce protein p21 and blocks next stage of cell division
• Mutant p53 no longer binds DNA and does not interact with p21
• Results in p21 unable to act as a stop signal• Cells divide uncontrollably

Genetics in Radiation• Ras, Raf, and EGFR alter cellular sensitivity to
radiation, but exact mechanisms unknown• Ras is a proto-oncogogene (portion of DNA
that regulates normal cell proliferation and repair)
• Raf is a gene coding for protein kinase• EGFR (epidermal growth factor receptor)
found on surface of some cells and where epidermal growth factor binds, causing the cells to divide

What is a common gene that can lead to many cancers it is mutated
or lost?A. EGFR
B. p 21
D. Ras
C. p 53
Wrong answer, try again.
EGFR is epidermal growth factor, Ras is a proto-oncogene, and p21 is a protein influenced by p53 and acts as a stop signal in the cell cycle.
Click here to return to question
Correct! p 53

INFLAMMATION
Microsoft Office Clip Art 2007
Inflammation
• Reaction of vascularized tissue to local injury.• Causes are many and varied.• Commonly it results from an immune
response to infection organisms.• Other causes are trauma, surgery, caustic
chemicals, extremes of heat and cold, and ischemic damage to body tissues.
(Porth, 2005).

Five Cardinal Signs of Inflammation
1. Redness2. Swelling3. Heat4. Pain5. Loss of function Microsoft Office Clip Art 2007
Acute InflammationTwo major components
1. VASCULAR2. CELLULAR
Inflammatory mediators, acting together or in sequence, amplify the initial response and influence its evolution by regulating the subsequent vascular and cellular responses (Porth, 2005).
Microsoft Office Clip Art 2007
Vascular Stage
• Constriction of small blood vessels in injured area
• Vasoconstriction followed rapidly by vasodilation of the arterioles and venules
• Causes the area to becomes congested and results in redness and warmth

Vascular Stage• Capillary permeability increases causes swelling,
pain, and impaired function• Movement of fluid from capillaries into
interstitial spaces (swelling) dilutes the offending agent
• Extravasation of plasma proteins into extracellular spaces causes exudate
• Blood stagnation and clotting of blood in the capillaries around the injury site; aids in localizing the spread of infectious microorganisms

Vascular Stage1. FIRST is immediate transient response 2. SECOND is immediate sustained response
which occurs with more serious injury and continues for several days and damages vessels in the area
3. THIRD is a delayed hemodynamic response, which increases capillary permeability that occurs 4 to 24 hours after injury, seen with RADIATION types of injuries

Cellular Stage
• Movement of phagocytic white blood cells (leukocytes) into area of injury
• Two types of leukocytes involved--granulocytes and monocytes
• Requires the release of chemical mediators from sentinel cells (mast cells and
macrophages) already positioned in tissues
Cellular Stage: Granulocytes
Granulocytes divided into three types neutrophils, eosinophils, and basophils.
1.Neutrophils are primary phagocytes; arrive within 90 minutes to injury site; contain enzymes and antibacterial substances that destroy and degrade engulfed particles.

Segmented Neutrophils
http://upload.wikimedia.org/wikipedia/commons/2/29/S

Cellular Stage: Monocytes• Mononuclear phagocytes are largest of white
blood cells • Last 3 to 4 times longer than granulocytes and
survive longer in the tissues.• Help to destroy agent, aid in signaling processes
of specific immunity, and help to resolve inflammatory process.
• Arrive by 24 hours and at 48 hours monocytes and macrophages are predominant cells at injury site
• Engulf larger and greater quantities of foreign materials and migrate to lymph nodes.
Phases of Acute Inflammation Response
MARGINATION
Leukocytes increase adhesion molecules, slow migration, and move along periphery of
blood vessels

Phases of Acute Inflammation Response
EMIGRATION
Leukocytes pass through capillary walls and migrate into tissue spaces

Phases of Acute Inflammation Response
CHEMOTAXIS
Leukocytes in tissues guided by cytokines, bacteria, and cell debris
Phases of Acute Inflammation Response
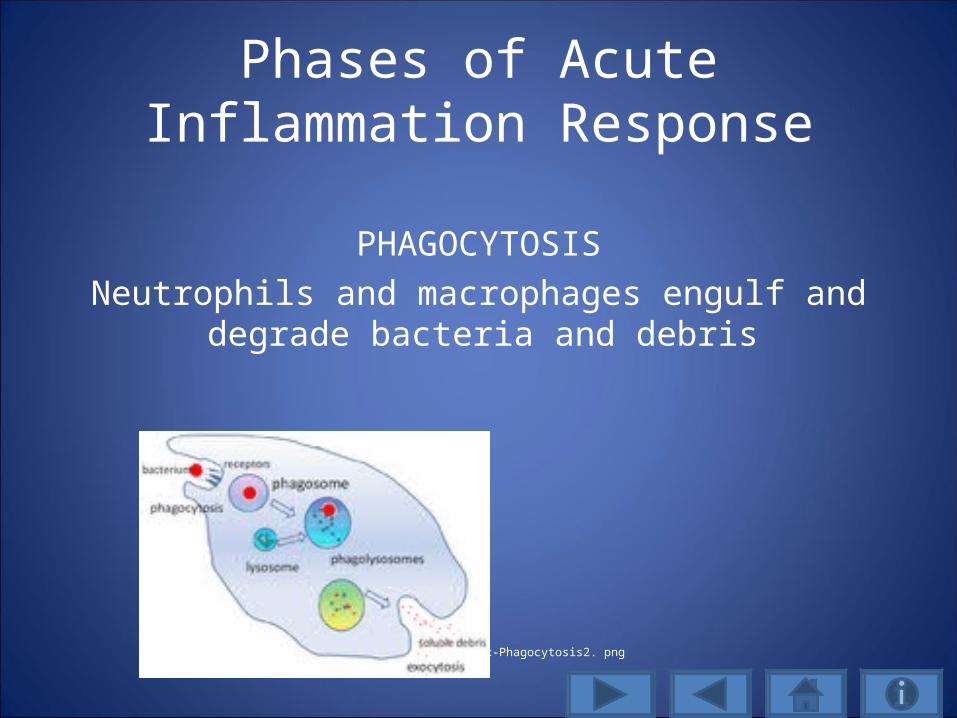
PHAGOCYTOSIS
Neutrophils and macrophages engulf and degrade bacteria and debris
Phagocytosis
http://upload.wikimedia.org/.../180px-Phagocytosis2. png

Inflammatory Mediators CYTOKINES Polypeptide products of various cell types- mostly lymphocytes and macrophages modulate functions of other cell types
COLONY-STIMULATING FACTORS directs growth of immature marrow precursor cells INTERLEUKINS (Ils) INTERFERONS (Ifs) TUMOR NECROSIS FACTOR

Inflammation with Chemical Mediator
INFLAMMATORY RESPONSE
Swelling, redness, and tissue warmth (vasodilation and increased
capillary permeability)
CHEMICAL MEDIATOR Histamine (fast acting and
causes dilatation and increased permeability of capillaries),
Prostaglandins, Leukotrienes, Bradykinin, Platelet-activating factor (attracts neutrophils)

Inflammation with Chemical Mediators
INFLAMMATORY RESPONSE
Tissue Damage
CHEMICAL MEDIATOR
Lysomomal enzymes and products released from neutrophils, macrophages, and other inflammatory cells

Inflammation with Chemical Mediators
INFLAMMATORY RESPONSE
Pain
CHEMICAL MEDIATOR
Prostaglandins Bradykinins

Inflammation with Chemical Mediator
INFLAMMATORY RESPONSE
Leukocytosis
CHEMICAL
MEDIATOR
Interleukin-1 Other Cytokines

What are the five major signs of inflammation?
A. Redness, pus, fever, pain, and swelling
B. Pain, swelling, numbness, tingling, and cold
C. Heat, pain, swelling, pus, and loss of function
D. Redness, swelling, heat, pain, and loss of function
C. Heat, pain, swelling, pus, and loss of function

Wrong answer, try again.
Click here to return to question

Correct! Redness, swelling, heat, pain, and loss of function.

SKIN STRUCTURE AND FUNCTION
Microsoft Office Clip Art 2007

SKIN
• Largest organ of the body
• Receives approximately one-third of heart’s oxygenated blood
• Body’s FIRST defense mechanism

SkinThree Layers
• Epidermis (outer layer)
• Dermis (middle layer)
• Subcutaneous tissue (inner layer) Microsoft Office Clip Art 2007
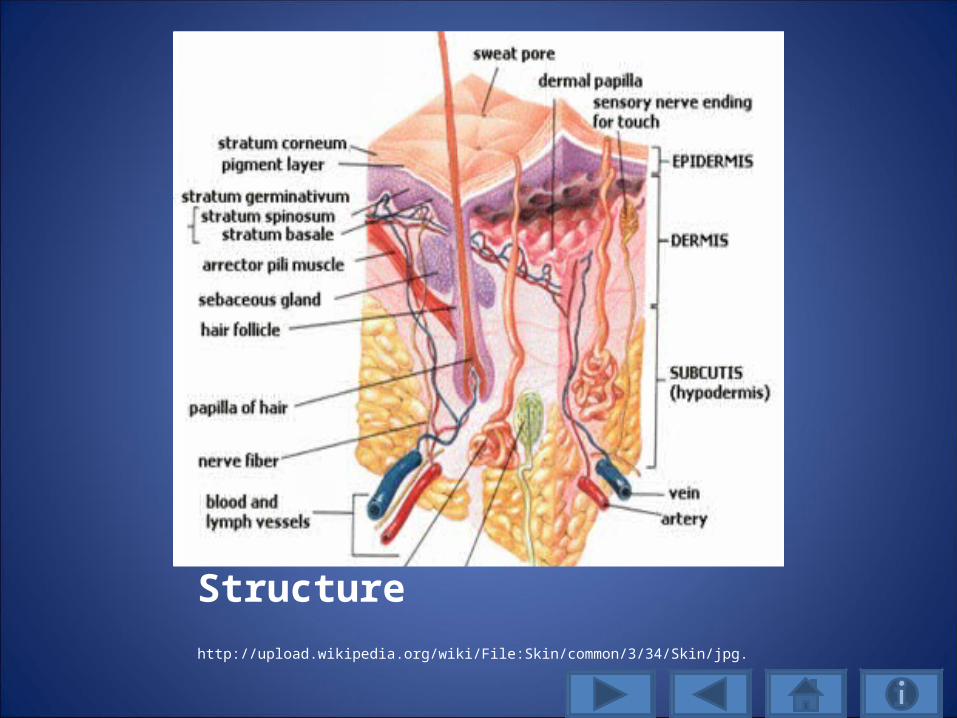
Skin Structure http://upload.wikipedia.org/wiki/File:Skin/common/3/34/Skin/jpg.
Epidermis
1. Multi-layered and impermeable 2. Outer layer that forms a resistant cover and
permeability barrier of varying thickness3. Renews itself continuously through cell
division in deepest (basal) layer4. Undergoes keratinization to produce scales
that are shed from outer layer 5. Avascular and receives nutrients from dermis

Epidermal Layers
1. Stratum corneum is outermost layer composed of flattened dead cells and is about 25% of total thickness
2. Stratum granulosum is thin transitional layer3. Stratum spinosum (squamous cell) is viable
layer made up of mainly post-mitotic cells4. Basal cell layer is viable and deepest layer
where majority of cell division occurs
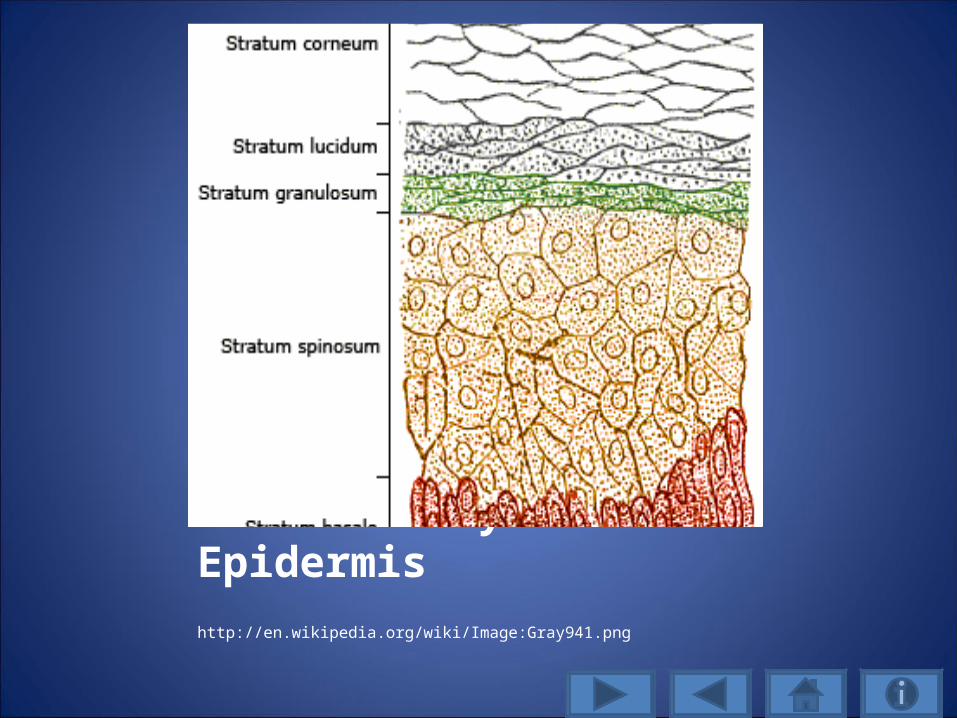
Layers of Epidermis http://en.wikipedia.org/wiki/Image:Gray941.png
Terminal Transition in Epidermis1. Half the cells produced in basal layer undergo
mitosis 2. After dividing, cells leave basal cell layer and
enter stratum spinosum and then stratum granulosum
3. This is where the cells flatten, lose organelles, and become mature, keratininized cells of the stratum corneum
4. Cells detach and desquamate, but are continually replaced by cells produced in basal layer (turnover process is 30 days)

Dermis
1. Tough and durable middle layer 1-3mm thick2. Gives skin strength, elasticity, and softness3. Protects deeper structures from injury4. Contains blood vessels that regulate body
temperature and provide nourishment to epidermis; also contains nerves, hair follicles and various glands
5. Interacts with epidermis during wound repair

Subcutaneous Tissue
1. Composed mostly of adipose tissue2. Cushion to physical trauma3. Insulator to temperature change4. Energy reservoir5. Nerves, blood vessels, and lymphatics run
through it
Functions of Skin
1. PROTECTION - MOST IMPORTANT!2. Regulation of body temperature3. Sensory perception4. Vitamin D production 5. Provides an active system of immunologic
defense (dermal lymphocytes, mast cells, mononuclear phagocytes, Langerhans cells)
6. Excretion

Skin
First line of defense against bacteria and foreign substances, physical trauma,
heat, or rays
Microsoft Office Clip Art 2007
Protection works by:(1) eccrine gland sweating(2) insulation by the skin
and subcutaneous tissue(3) regulation of cutaneous
blood flow (vasoconstriction and
vasodilation)(4) muscle activity (shivering)
What is the major function of the skin?
A. Vitamin D Production
B. Sensory perception.
C. Regulation of body temperature.
D. Protection
Wrong answer, try again.
Click here to return to picture

Correct! Protection.

BREAST SKIN CHANGES
Microsoft Office Clip Art 2007

Radiation Changes
• Reflect injury occurring mostly in the epidermis
• Primary target for acute radiation skin reactions is the basal cell layer
• Entire epidermis turns over in 30 days

Radiation Changes
• Early erythema within few hours after radiation and subsides after 24-48 hours
• Inflammatory response from histamine-like substances that cause dermal edema from the permeability and dilatation of capillaries

Radiation Changes
• Main erythematous reaction occurs 3-6 weeks after radiation begins and is due to a varying severity loss of epidermal basal cells
• Basal cell density changes with higher doses of radiation
• Reddening of the skin due to a secondary inflammatory reaction or hyperemia

Radiation Changes
• Higher radiation doses reduce number of mitotic cells and increase in degenerate cells
• When cells are not being reproduced at the same rate in the basal cell layer and the normal migration of cells to stratum corneum continues, epidermis is denuded in time equal to natural turnover (30 days)

Dry Desquamation• If enough numbers of clonogenic cells (cells
giving rise to a clone of cells) remain to replace injured cells, there is atypical thickening of the stratum corneum
• The populations of the basal-layer stem cells become depleted in the radiation treated area
• This can result in dry flaking, scaling, and itching in the treated area

Dry Desquamation Adapted with permission by Nature Publishing Group: Leukemia, volume 17, issue 7, 2003. www. Nature.com/leu/journal/v17/n7images/240991f1.jpg
Moist Desquamation • If new cell proliferation is inadequate, there is
exposed dermis with oozing of serum• Repopulation of the basal cell layer of
epidermis after irradiation is mainly from surviving clonogenic cells (cells giving rise to a clone of cells) within the irradiated area
• If the treated area is completed denuded of clonogenic epithelial cells, then healing results from division and migration of viable cells from skin around the irradiated area

Moist DesquamationUsed with permission , Adapted from Ostomy Wound Management ,
volume 51, issue 10, Managing Radiation Skin Injury www.o-wm/com/article/4752/files/photos/notesfig19867.gif

Acute Skin Reactions
ERYTHEMARedness that outlines treatment field and
intensifies as treatment continuesIncreased skin temperature
EdemaFollows after 2-3 weeks after standard
fractionated radiation and resolves 20-30 days after last treatment

Acute Skin Reactions
DRY DESQUAMATIONDrynessFlakingPeeling
PruritusFollowing 3-4 weeks of standard fractionated
radiation and resolves 1-2 weeks after completion of treatments

Acute Skin Reactions
HYPERPIGMENTATION
Tanned appearance
Following 2-3 weeks of standard fractionated therapy and is usually resolved in 3 months to
1 year after treatment but may be chronic

Acute Skin Reactions
MOIST DESQUAMATION
Bright erythemaSloughing skin
Exposed dermisSerous exudate
Pain

Acute Skin Reactions
MOIST DESQUAMATIONCan occur with radiation or with trauma or friction and most recovery usually 2-4 weeks
after completion of treatmentSKIN REGROWTH
New skin is smooth, pink, thin, and dryerDepends upon severity but usually is complete
2-3 months after therapy

Late Skin Reactions
PHOTOSENSITIVITY
Enhanced erythema over skin exposed to UV radiation from sun and tanning bed/booths
Begins during treatment and is lifelong
What develops after 3 -4 weeks of radiation with symptoms of dry,
flaking, and peeling skin?A. Dry desquamation
B. Erythema
C. Moist desquamation
D. Hyperpigmentation
Sorry, wrong answer.
Click here to return to question

Yes! Dry desquamation.

NURSING CARE AND PATIENT EDUCATION
Microsoft Office Clip Art 2007

Nursing Care• Perform skin assessment before radiation
treatments, at least weekly during treatments, 1 month following completion of treatment, and
each follow-up appointment.• Initial assessment includes the patient’s present
skin condition, preexisting skin disorders, medical conditions, medications, age-related factors, and nutritional status.
• Consistency in assessment and documentation is important.

Patient Instructions
• Use gentle soaps ONLY, such as Dove or Ivory, which do not contain additives
• Use a moisturizing lotion on the treatment area twice a day
• Expose the treated area to the air as much as possible
• Do not wear underwire bras• Do not wear tight-fitting clothing that rubs or
binds underneath the breast

Patient Instructions
• Wear a comfortable bra. Wear cotton t-shirts underneath your bra to absorb moisture.
• Drink 8-10 glasses of water a day.• Eat well-balanced meals and maintain your
weight during treatment. • Continue with your normal daily activities.

Patient Instructions
• Sexual activity may continue during treatment. You are not radioactive and there are no dangers to your partner.
• Avoid extreme temperatures to the affected area. Do not use water bottles, heating pads, sun lamps, ice bags, etc.
• Avoid exposing your skin to the sun, as the sun and sun rays are an additional form of radiation to the skin. Always apply sunscreen with SPF or 15 before sun exposure.

Patient Instructions
• Do not apply tape or adhesive bandages to the treated area.
• Speak with your nurse about deodorant use • Continue with the range of motion exercises
for your arm and shoulder. • Report any pain or swelling to your doctor or
nurse.

Breast Skin Products
Cleanser and moisturizerGiven to every breast cancer patient being
treated with radiationHave patients use twice a day

Breast Skin Products
Healing ointment and skin protectantUsed for dry desquamation
Apply to affected area

Breast Skin Products
MOIST DESQUAMATIONTopical aluminum acetate packets (astringent)
mixed with normal saline Gently debride area and apply solution to area for
20 minutes; rewet every 10 minutes and repeat once a day
Apply hydrocolloid dressing over affected area and secure
Do NOT use hydrocolloid dressing 4 hours before treatment
What is the recommended treatment for every radiation
patient?A. Soap and water once a day
B. Apply cleanser and moisturizer twice a day on the affected area
C. Apply a hydrocolloid over the treated area
D. Encourage daily sun exposure.
Sorry, incorrect. Try again.
Click here to return to the
question

Yes! Apply cleanser and moisturized twice a day to the
affected area.
Case Study
Mrs. K is a breast cancer patient who has received radiation to her left breast for the past 4 weeks. She is complaining of increasing pain and her left breast is bright red in color, with sloughing skin and a serous exudate.
What is the name of this skin condition
caused by radiation? What would be the nurse’s actions and interventions?

Case Study
Moist desquamation. The nurse would apply an aluminum acetate
solution for 20 minute and gently debride the area.
A hydrocolloid dressing would then be placed over this area and secured.
The patient would be given instructions about this treatment once a day.
Pain management will be addressed.

ReferencesAbeloff, M.D., Armitage, J. O., Niederhuber, J. E., Kastan, M. B., & McKenna, W. G. (2004). Clinical oncology (3rd ed.). Philadelphia, PA: Elsevier, Inc.Bruner, D. W., Bucholtz, J. D., Iwamoto, R., & Strohl, R. (Eds.) (1998). Manual for radiation oncology nursing practice and education. Pittsburgh, PA: Oncology Nursing Society.Fox, S. I. (1996). Human physiology (5th ed.). Dubuque, IA: Wm. C. Brown Publishers.Groenwald, S.L., Frogge, M.H., Goodman, M., & Yarbro, C.H. (1993). Cancer nursing:
Principles and practice (3rd ed.). Boston, MA: Jones & Bartlett. Hill, S. (2008). Managing radiation skin injury. Ostomy Wound Management, 51(10), 1-2. Retrieved May 13, 2009, from, http://www.o-wn.com/article/4752. Mahon, S. M. (Ed.). (2007). Breast cancer. Pittsburgh, PA: Oncology Nursing Society. Milojkovic, D., Short, K., Salisbury, J. R., creamer, D., du Vivier a. W. P., & Mufti, G. J.
(2003). Dose-limiting dermatological toxicity secondary to imatinib mesylate (STI571) in chronic myeloid leukaemia. Leukemia, (17), 1414-1416. Retrieved May
13, 2009, from http://nature.com/leu/journal/v/17/n7/full/24024991a.html.Microsoft Clip Art 2007 retrieved on various dates in April and May of 2009, from
http://officeMicrosoft.com/en-us/clipart/default.aspx.
National Human Genome Research Institute (n.d.). Chromosome. Retrieved May 12, 2009, from http://www.genome.gov/Hyperion/DIR/VIP/Glossary/Illustration/chromosome.cfm?key=chromosome.
Otto, S. E. (2001). Oncology nursing (4th ed.). St. Louis, MO: Mosby, Inc.Porth, C. M. (2005). Pathopphysiology: Concepts of altered health status (7th ed.). Philadelphia, PA: Lippincott, Williams & Wilkins. Singer, M. (1992). The Ras gene and cancer. Winding your way through DNA. Symposium conducted at the University of California. San Francisco. Retrieved May 13, 2009, from http://www/accessexcellence.or/RC/AB/BA/Ras_Gene_and Cancer.php. United States National Library of Medicine (n.d.). DNA structure. Genetics home
reference: Your guide to understanding genetic conditions. Retrieved May 9, 2009, from http://ghr.nlm.nih.gov/handbook/illustrations/dnastructure..United States National Library of Medicine (n.d.). Chromosome structure. Genetics home reference: Your guide to understanding genetic conditions. Retrieved May 13, 2009, from http://ghr.nlm.nih.gov/handbood/illustrations/chromosomestructure.United States National Library of Medicine (n.d.). Gene. Genetics home reference: Your guide to understanding genetic conditions. Retrieved May 13, 2009, from http://ghr.nlm.nih.gov/handbood/illustrations/genein chromosome.

White, J., & Joiner, M. C. (2006). Toxicity from radiation in breast cancer. In W. Small Jr., & G. E. Woloschack (Eds.)., Radiation toxicity: A practical guide. Springer Science + Media Business, Inc.
Wikigenetics (n.d.). The cell cycle. Retrieved May 9, 2009, from wikigenetics.org/index.php./The_Cell_Cycle.Wikimedia Commons (n.d.). Segmented neutrophils. Retrieved May 14, 2009, from http://commons.wikimedia.org/wiki/File:Segmented_neutrophils.jpg.Wikimedia Commons (n.d.). Skin. Retrieved May 13, 2009, from http://commons.wikimedia.org/wiki/File:Skin.jpg.Wikimedia Commons (n.d.). Skin layers. Retrieved May 13, 2009, from http://commons.wikimedia.org/wiki/File:Skinlayers.png.Wikipedia (n.d.). Phagocytosis. Retrieved May 14, 2009, from
http://en.wikipedia.org/wiki/Phagocyte.

Good Job
Microsoft Office Clip Art 2007







