

Whose Evidence, What Kind of Practice: Profits, Research
and Medical Practice
Joel Lexchin MD
School of Health Policy and Management
York University
Emergency Department
University Health Network

Outline
• Who is spending money• Funding and choice of research topic• Funding and outcome of research• Suppressing & biasing research results• Conflict-of-interest
– Research results– Clinical Practice Guidelines
• Money and medical journals• Prescribing behaviour
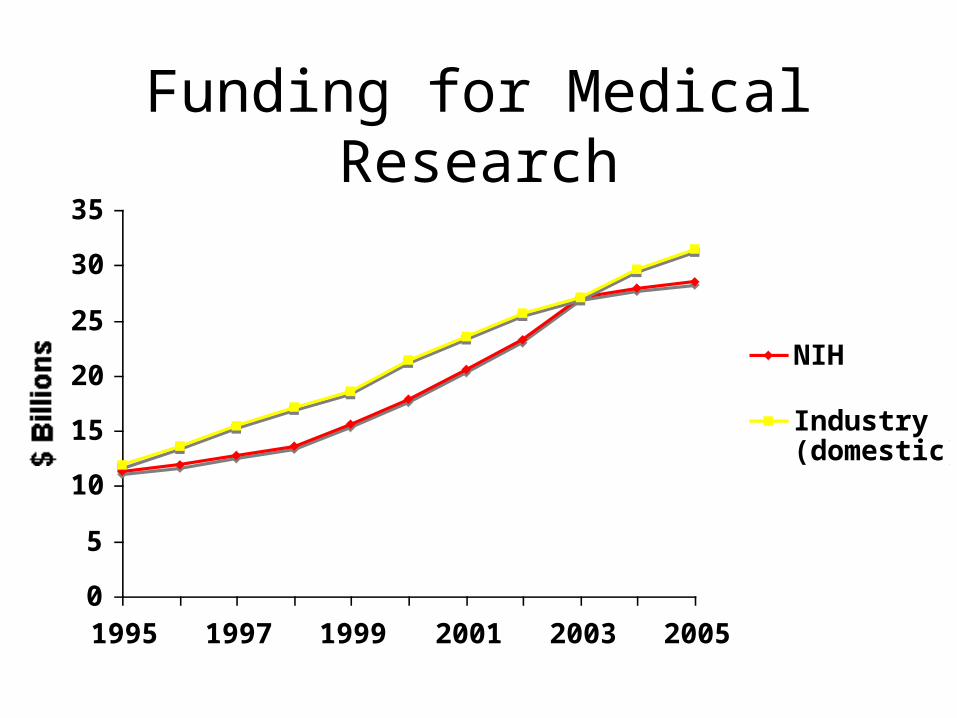
Funding for Medical Research
0
5
10
15
20
25
30
35
1995 1997 1999 2001 2003 2005
$ Billions
NIH
Industry(domestic)

Funding for Clinical Research, United States, 2002
$3.90
$0.56
$1.10
BiopharmaDevice makersNIH
Billions
CenterWatch 2003

Fewer Non-Industry Funded Trials in the UK
Chalmers et al. BMJ 2003;327:1017-20

Health R&D in Canada, 2004
1.10
0.36
1.561.49
0.46
0.79
FederalgovernmentProvincialgovernmentBusiness enterprise
Higher education
Private non-profit
ForeignSpending in billions of dollars, total $5.75 billion
Statistics Canada. Science Statistics. Catalogue 88-001-XIE
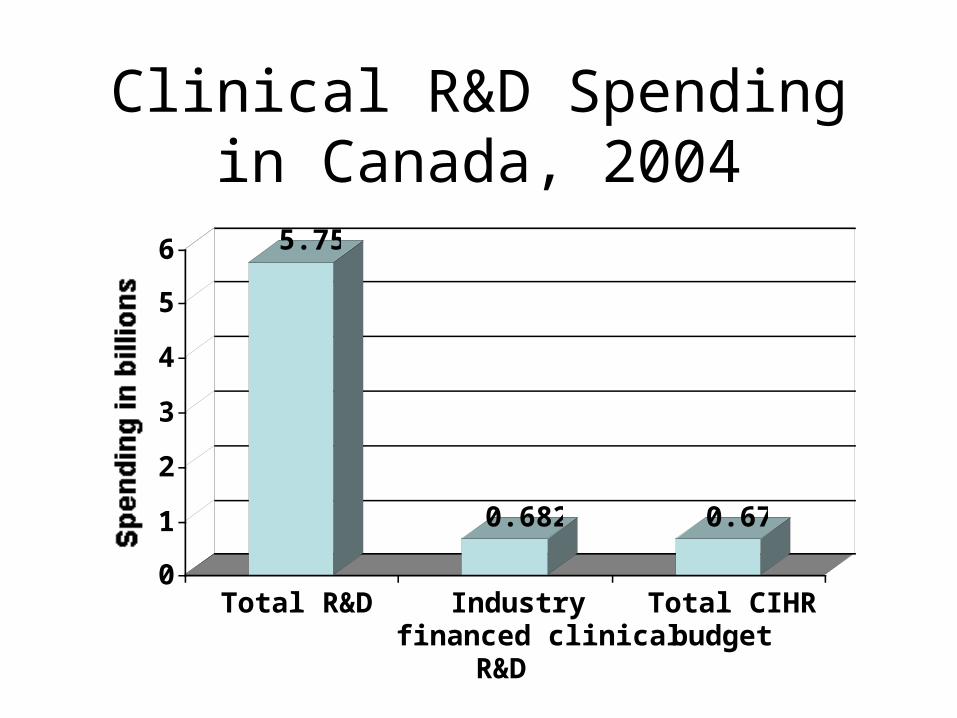
Clinical R&D Spending in Canada, 2004
5.75
0.682 0.67
0
1
2
3
4
5
6
Spending in billions
Total R&D Industryfinanced clinical
R&D
Total CIHRbudget

The Willie Sutton Rule
Why did he rob
banks?
“That’s where the
money is”

Source of Support and Choice of Research Topic
Industry support No industry support
1985
(%)
1994/5
(%)
1985
(%)
1994/5 (%)
Choice of research topic influenced by commercial application
30 35 7 14
Blumenthal et al. Science 1986;232:1361-6Blumenthal et al. NEJM 1996;335:1734-9

Drug Companies Directing Research: OA of the Knee
Treatment Commercially sponsored
(number)
Alternative & complementary
5
Drug (injected) 5
Drug (oral) 109
Education 1
Physiotherapy & exercise
3
Surgery 5
Total 128
Tallon et al. Lancet 2000;355:2037-40
Drug Companies Directing Research: OA of the Knee
Rheumatologist Focus Group• NSAIDs over-researched especially through commercial sponsored
drug trials
Patient Focus Group• Favoured conservative treatments such as physiotherapy• More research on education and self-help
GP Focus Group• Research on surgical success rates and conservative treatments• Oral drugs over-researched
Physiotherapist Focus Group• Absence of research on physiotherapy & exercise• Dominance of drug trials

Outcome of Industry Funded ResearchOdds ratio meta-analysis plot (fixed effects)
0.10.20.51251010010001.00E+05Yaphe et al (44)Vandenbroucke et al (42)Thomas et al (41)Sacristan et al (39)^^Sacristan et al (39)^Mandelkern (35)Koep et al (33)Kamal-Bahl et al (29)##Kamal-Bahl et al (29)#Friedberg et al (26)**Friedberg et al (26)*Djulbegovic et al (23)Djulbegovic et al (22)Dieppe et al (21)Davidson (19)Clifford et al (18)Cho et al (17)Azimi et al (15)
MH pooled odds ratio = 4.051419 (95% CI = 2.978525 to 5.510779)
Lexchin et al. BMJ 2003;326:1167-70
O.R. 4.09
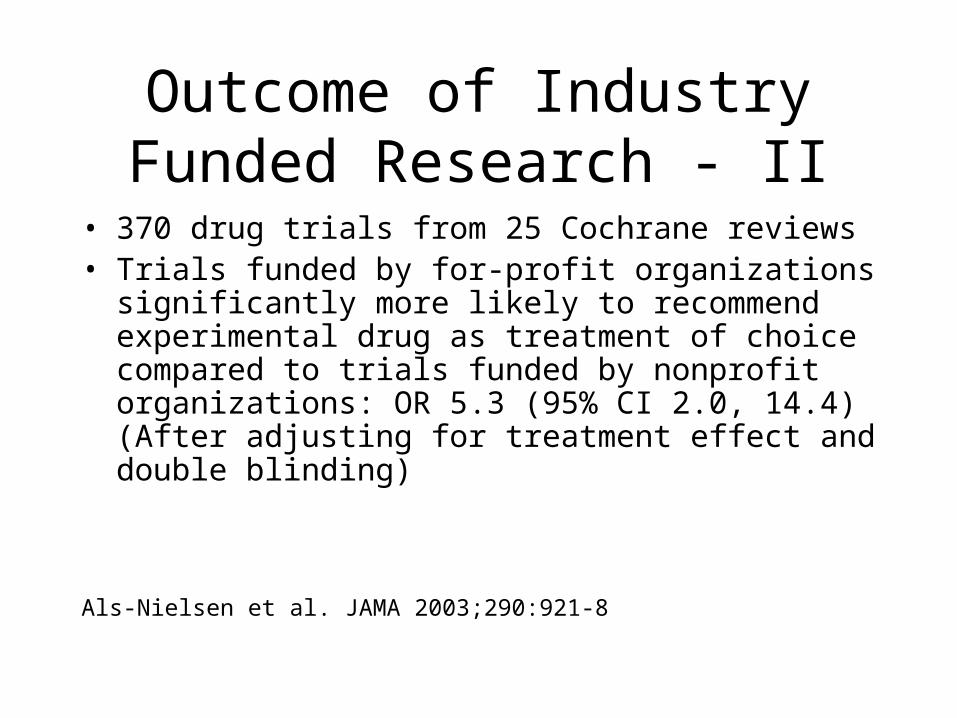
Outcome of Industry Funded Research - II
• 370 drug trials from 25 Cochrane reviews• Trials funded by for-profit organizations significantly
more likely to recommend experimental drug as treatment of choice compared to trials funded by nonprofit organizations: OR 5.3 (95% CI 2.0, 14.4) (After adjusting for treatment effect and double blinding)
Als-Nielsen et al. JAMA 2003;290:921-8

Outcome of Industry Funded Research - III
• Moncrieff. Br J Psych 2003;163:161-6– Industry funded clinical trials on clozapine showed greater positive
effect than trials with other sources of funding
• Baker et al. Br J Psych 2003;183:498-506– Pharmacoeconomic studies of antidepressants revealed clear
associations of study sponsorship with quantitative outcome
• Bhandari et al. CMAJ 2004;170:477-80– 158 RCTs of drug products from 5 high-impact general medical
journals – Industry trials more likely to be favourable to product OR 1.6 (95%
CI 1.1, 2.8)

Outcome of Industry Funded Research - IV
• Montgomery et al. Controlled Clinical Trials 2004;25:598-612– Industry funded studies significantly favoured second generation over first
generation antipsychotics compared to non-industry funded studies
• Heres et al. Am J Psychiatry 2006;163:185-94– 33/42 head-to-head trials of second generation antipsychotics funded by
industry– 90% of these reported overall outcome favoured sponsor’s drug– Same drugs compared but with different sponsors had contradictory
results
• Bell et al. BMJ 2006; on-line 31 March 2006– 494 studies measuring health effects in QALYs published up to December
2003– Cost effectiveness studies funded by industry more likely to report rates
favourable ratios (below $20,000, $50,000 and $100,000)

Outcome of Industry Funded Research - V
• Ridker et al. JAMA 2006;295:2270-5– 324 superiority trials of cardiovascular medicine published between
Jan. 1, 2000 and July 30, 2005 in JAMA, Lancet and NEJM
– 205 trials on drugs: proportions favouring newer treatments were 39.5% not-for-profit funding, 54.4% jointly funded and 65.5% for-profit funding (p for trend 0.002)
• Perlis et al. Journal of the American Academy of Dermatology 2005;52:967-71– 179 RCTs in dermatology published between Oct. 1, 2000 and Oct.
1, 2003
– Industry funded studies more likely to report positive findings (65% vs. 35%, p = 0.001)

Outcome of Industry Funded Research - VI
• Perlis et al. American Journal of Psychiatry 2005;162:1957-60– 162 double-blinded placebo-controlled RCTs published between
2001 and 2003– Industry support not associated with positive outcome but if one or
more authors had potential conflict of interest there was a significant association with positive trial outcomes among all studies regardless of funding source (p<0.001) and among industry-supported studies (p<0.001)
• Barden et al. Pain 2006;121:207-18– Examined industry funded analgesic trials where same drug was
“test” and “comparator”– Except for one case (sumatriptan & headache response at 2 h) no
difference in pain relief when drug was test or comparator
Outcome of Industry Funded Research - VII
• Procyshyn et al. Can J Psych 2004;49:601-606– 372 clinical trials on 3 atypical antipsychotics; 124 industry
sponsored– No industry sponsored trial reported negative results (findings
favouring comparator; serious concerns about safety or efficacy; recommended comparator)
• Jorgensen et al. BMJ 2006;333:782– Industry supported meta-analyses less transparent, fewer reservations
about methodological limitations of included trials and more favourable conclusions than corresponding Cochrane reviews

Research Results and Funding
Type of research
Results favour
industry
Results do not favour industry
Clinical trials 10 1
Pharmaco-economic studies
3 0
Meta-analyses 1 0

“Study 329 … showed trends in efficacy”
The second study … failed demonstrate any separation of Seroxat/Paxil from placebo
Data from these 2 studies … will therefore not be submitted to the regulatory authorities


And GSK Gagged Researchers
“Those researchers, including myself, who did seeresults of negative paroxetine industry trials wereprohibited by nondisclosure contracts fromdiscussing them.”
Jane Garland MDPediatric PsychiatristVancouver
Garland. CMAJ 2004;170:489-91


JAMA 2001;286:2398



Ghostwriting - Articles on Paroxetine
Source of article
Current Medical Directions
(Ghostwritten)
Other
(Not ghostwritten)
Medline listing per author
70 37
Literature profile per article
1839 283
Citation rate of series
20.2 7.7
Healy et al. British Journal of Psychiatry 2003;183:22-7
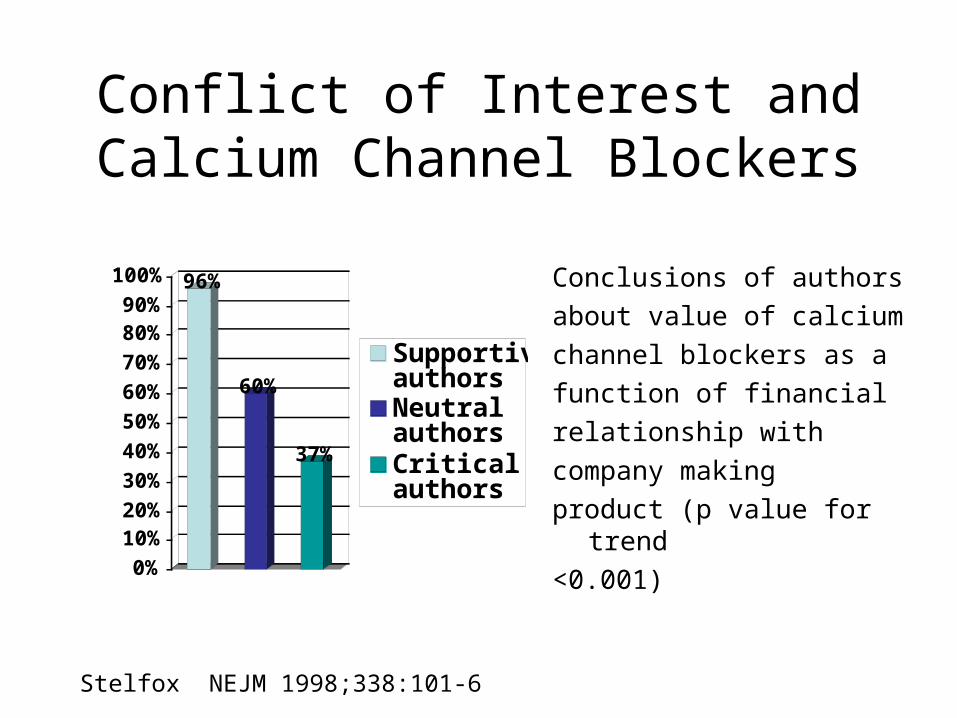
Conflict of Interest and Calcium Channel Blockers
96%
60%
37%
0%
10%20%
30%
40%
50%
60%
70%
80%90%
100%
SupportiveauthorsNeutralauthorsCriticalauthors
Conclusions of authors
about value of calcium
channel blockers as a
function of financial
relationship with
company making
product (p value for trend
<0.001)
Stelfox NEJM 1998;338:101-6

Declaration of Conflict of Interest
0
10
20
30
40
50
60
70
80
90
Percent of studies
Positive Mixed Negative Other
Drug treatment studieswith COIDrug treatment studiesno COI
Friedman, JGIM 2004;19:51-6

Declaration of Conflict of Interest
Higher the score, themore strongly the treatment is recommended
Kjaergard et al. BMJ 2002;325:249

CPGs and Conflict-of-Interest
JAMA 2002;287:612-7

Conflicts of Interest in Clinical Practice Guidelines
Over 200 guidelines examined; only 90 contained details aboutindividual conflicts of interest; of those only 31free of industry influence
Nature 2005;437:1070-1

Lilly and Xigris
NEJM 2006;355:1640-2

Lilly and Xigris
2002 - Lilly hires Belsito & Co. to improve sales of Xigris– Part of campaign focused on drug being rationed
because of expense and doctors “systematically forced” to decide who would live and die
– Lilly provided group of doctors and bioethicists with $1.8 million grant to address ethical issues raised by rationing in ICU setting
Lilly and Xigris
Surviving Sepsis Campaign– Lilly provided 90% of funding for creation &
publication of guidelines around sepsis management
– Guidelines give highest grade to therapies subject to RCTs - therefore Xigris got very favourable rating (grade B) because of PROWESS study whereas antibiotics, fluids, vasopressors received lower ratings (grades D or E) because had not undergone RCTs owing to lack of equipose

Lilly and Xigris
• PROWESS showed increased risk serious bleeding with Xigris
• Two further studies (ADDRESS and RESOLVE) terminated early because unlikely to show benefit confirmed bleeding risk– No mention of ADDRESS study in guidelines
• ENHANCE study indicated bleeding risk might be greater than originally estimated– Guidelines included data from ENHANCE but possible
magnitude of increased risk not noted
• Guidelines do not note that Infectious Disease Society of America declined to endorse them

Reluctance to Run Critical Articles
• Transplantation and Dialysis rejected editorial questioning value of epoetin in end-stage renal disease
• Letter from editor to author:“I have been over-ruled by our marketing department with regard to publishing your editorial…the publication of your editorial would, in fact, not be accepted in some quarters…and apparently went beyond what our marketing department was willing to accommodate”
Dyer. BMJ 2004;328:244

Does Ad Revenue Bias Journal Content?
Annuals of Internal Medicine, June 1992• Article analyzing 102 journal advertisements
from 10 leading medical journals• Expert reviewers
– 44% ads lead to improper prescribing– 34% ads needed major revisions– 28% ads should not have been published
Wilkes et al. Ann Intern Med 1992;116:912-9

What Happened to Ad Revenue?
05
101520253035404550
Percent decrease in volume of drug ads inperiod 7/92-12/94 (compared 1/91-6/92)
Ann Int MedArch Int MedJAMAAJMNEJM
Landefeld et al: JGIM 1995;10(Suppl):111

Why Did This Happen?
Robert Fletcher (co-editor of Annals):“The episode revealed the true colours of thepharmaceutical industry, which was willing toflex its considerable muscles when it felt itsinterests were threatened.”
Fletcher. Lancet 2003;361:10

Changes in Prescribing for Hypertension
Drug class 1985 1995
Percent of respondents
Daily ingredient
cost ($)
Percent of respondents
Daily ingredient
cost ($)
ACE 5.2 1.03 25.4 0.91
Beta-blocker 21.9 0.62 22.1 0.68
CCB 2.1 1.07 19.7 1.24
Diuretic 31.3 0.05 17.2 0.10
Combination or other
39.6 0.63 15.6 1.32
Wolf et al. CMAJ 1999;161:699-704

Prescribing of Some New Products is Additive Not
Replacement
Total NSAID prescribing increased when COXIBs came on the market
ICES, Nov. 2003

The Result: More GI Bleeds

Conclusion
• Follow the money• Different funders have different interests• Those interests determine
– What kind of research gets done– What kinds of bias might be present– What the outcomes are– How those outcomes are reported– Ultimately how doctors prescribe
• Right now the pharmaceutical industry has the money







