WSCC Model: Coordinating and Leading Toward Improved Oral Health and Academic Success
Sue Baldwin, PhD, MCHES, FASHA Buffalo Public Schools, District Wellness Coordinator Renee Retton, Doctoral Student, MS, CHES University Pediatric Dentistry Associates, A.T. Still University

WSCC Model Health education
Physical Education &
Physical Activity
Nutrition Environment &
Services
Health Services
Counseling, Psychological &
Social Services
Social & Emotional Climate
Physical Environment
Employee Wellness
Family Engagement
Community Involvement

Learning Objective #1 Assess social, environmental, and political conditions surrounding oral health that may impact health education and use assessment results to:
Inform School Health Services /
Stakeholders
Drive Programming Planning Processes

Learning Objective #2 Analyze factors that enhance or compromise oral health and that foster or hinder the learning process.
“Tooth decay is one of the most common chronic conditions of childhood in the United States. Untreated tooth decay can cause pain and infections that may lead to problems with eating, speaking, playing, and learning.” Centers for Disease Control and Prevention - 2014

Learning Objective #3 Identify gaps in oral health monitoring/surveillance instruments.
1. CDC, Youth Risk Behavior Surveillance Survey (YRBSS)
2. CDC, School Health Index (SHI)
3. Rudd Center, Wellness School Assessment Tool (WellSat 2.0)
4. ASCD School Improvement Tool (SIT) – “Whole Child Approach”

Learning Objective #4 Critique this District’s existing YRBSS data collection instrument and explore potential new items to include in the:
1. Youth Risk Behavior Surveillance Survey
2. School Health Index (SHI)
3. WellSat
4. School Improvement Tool (SIT)

http://www.ascd.org/programs/learning-and-health/wscc-implementation.aspx

In Summary A national initiative exists to increase pediatric oral health access for: preventative
services, interventions and monitoring. Healthy children are better learners! Most current school health surveillance tools do not include dental health items.
• YRBSS – one item (2015) National high school version #94 / Standard high school version #86 / none middle school version
• SIT – 1 item – healthy indicator section item #9 Dental health has an effect on: a child’s school performance, attendance, self-esteem,
quality of life, overall health and success later in life. (Kwan, Petersen, Pine & Borutta, 2005) The targeted urban area depicted in this presentation is using the WSCC Model and is
considered “ a dental health desert.” Aim: we hope this dissemination will expand the inclusion of oral health item use in
the following tools: YRBSS, SHI, WellStat, and SIT.

Current Trends in Pediatric Oral Health: Establishing Importance Tooth decay/cavities – one of most preventable common chronic conditions of childhood in the
US.
About 1 of 5 (20%) children aged 5–11 years have at least one untreated decayed tooth.
About 1 of 7 (13%) adolescents aged 12–19 years have at least one untreated decayed tooth.
Percentage of children and adolescents aged 5–19 years with untreated tooth decay is twice
as high for those from low-income families (25%) compared with children from higher-income
households (11%).
Dye, Xianfen and Beltrán-Aguilar, 2012

Urban District Background Challenges and Opportunities:
DISTRICT PROFILE
∗ 34,066 students – 56 schools
∗ 79% minority; 49% African-American
∗ 78% receive free/reduced lunch
∗ 55 of 56 schools Title 1
∗ 22 schools receive SIG grants
∗ 25 out of 59 schools in receivership; 5
persistently struggling (Jan, 2016)
ACADEMIC ACHIEVEMENT
* 56% high school graduation rate
* 8% drop out rate
* 11 of 17 high schools with 3 or fewer AP courses
* District wide average ACT 20.3; only 12.5% college
ready
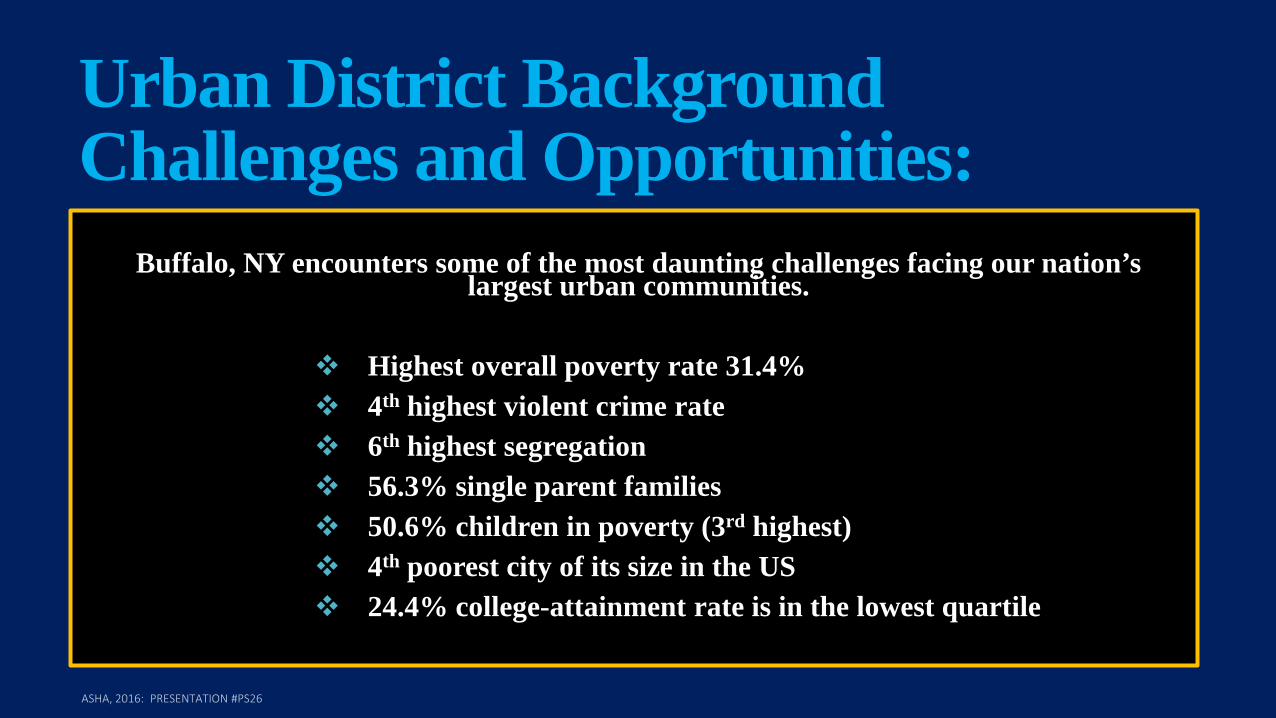
Urban District Background Challenges and Opportunities:
Buffalo, NY encounters some of the most daunting challenges facing our nation’s
largest urban communities.
Highest overall poverty rate 31.4% 4th highest violent crime rate 6th highest segregation 56.3% single parent families 50.6% children in poverty (3rd highest) 4th poorest city of its size in the US 24.4% college-attainment rate is in the lowest quartile

Barriers or Simply Speed Bumps? Identifying stakeholders: multiple levels (target audiences)
Engaging stakeholders
Buy in
$$$$$$$$
Evaluating results
Interventional programming
Sustainability
Where do we go from here?

Forming Strategic Policy: Where We Started
PHA
SE 1
BASIC SERVICES -A nurse in every school -Providing basic care -Maintaining health records pertaining to physicals, immunizations, etc.
PHA
SE 2
ENHANCED SERVICES -School-based health centers -Mental health clinics -Dental program -Lead screenings -Assisting pregnant & parenting teens
PHA
SE 3
WHOLE SCHOOL WHOLE COMMUNITY WHOLE CHILD -Research on best practice models -Data collection (Youth Risk Behavior Survey) -Development of comprehensive District Wellness Policy -Implementation of whole child framework for health and learning

Step #1 - Wellness Policy Over 100 people engaged in policy work sessions with Student Support Services
Center of the Genesee Valley Educational Partnership on the WellSAT tool developed
by the Rudd Center (www.wellsat.org) - NYS DOH Grant: Healthy Schools (2010)
Over 15 work sessions between 2011-2012
Adopted: Spring 2012 by BPS Board of Education
District Wellness Coordinator Hired: September 2013 funded via NYS School
Health Grant to District
Coordinator’s dissertation and research in Coordinated School Health, attended
2014 SOPHE conference on WSCC ASHA, 2016: PRESENTATION #PS26
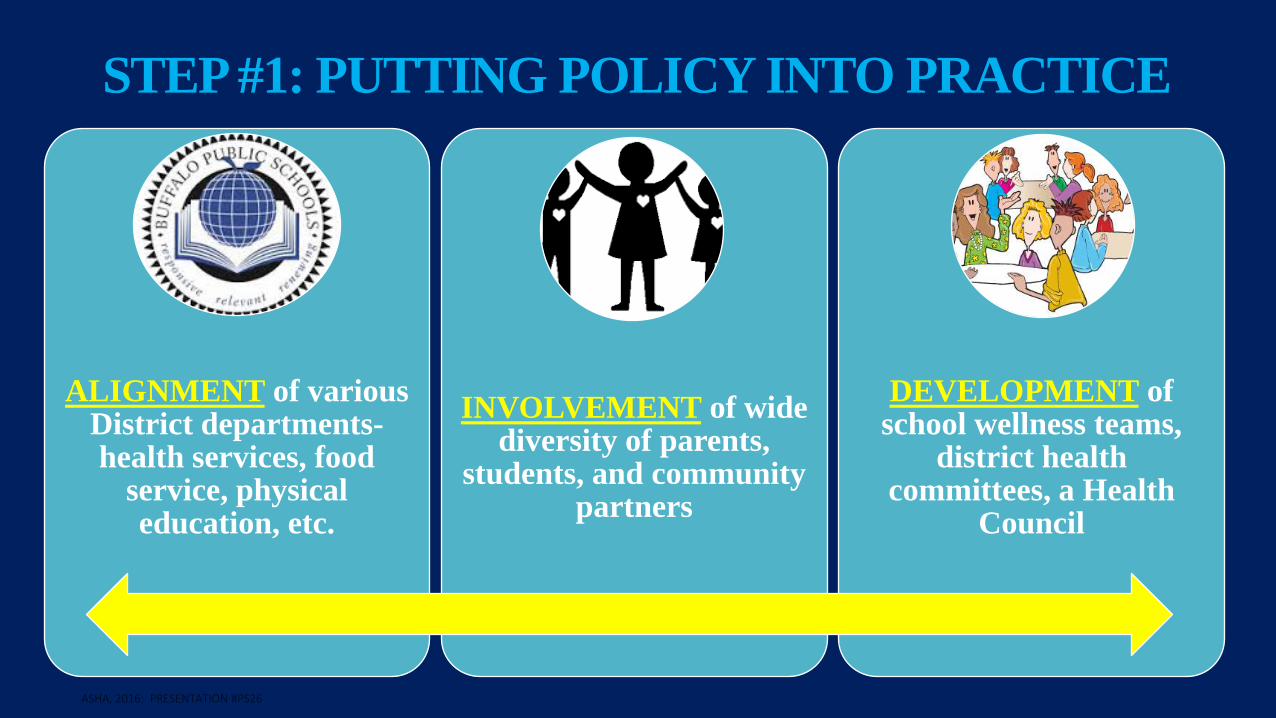
STEP #1: PUTTING POLICY INTO PRACTICE
ALIGNMENT of various District departments- health services, food
service, physical education, etc.
INVOLVEMENT of wide diversity of parents,
students, and community partners
DEVELOPMENT of school wellness teams,
district health committees, a Health
Council
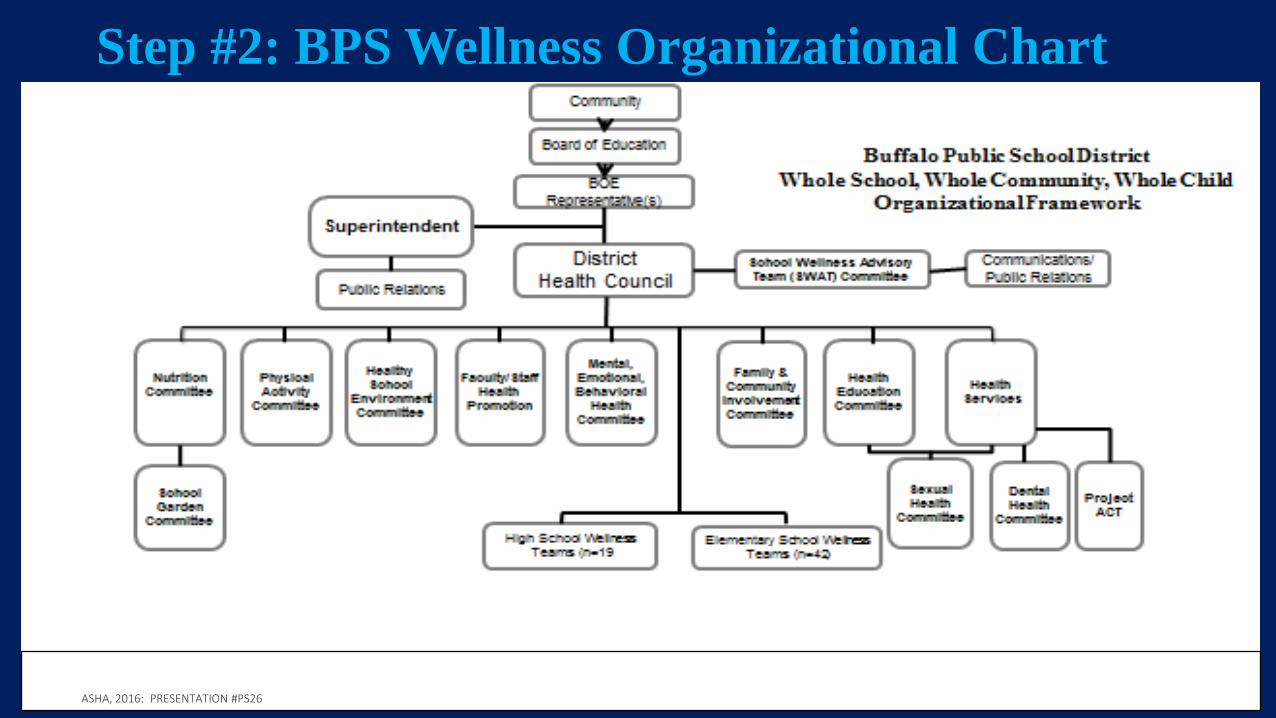
Step #2: BPS Wellness Organizational Chart

To create healthy, safe, supported engaging, and challenging school communities in all schools that seek the input from families,
school employees and community partners by 2020.
STEP #2: DISTRICT WELLNESS VISION:

Our mission is to build the capacity of school communities to be healthy, safe, challenging and supporting through the engagement of families,
educators and community members to create, enrich, promote and sustain supportive learning
environments as well as to reduce health-related barriers to learning that impact on academic
achievement and citizenship.-BPS
Step #2: DISTRICT WELLNESS MISSION:

A few of our Partners:

WSCC Model Implementation in our Urban District WSCC Model was implemented across 58 schools (district- and school-level) on May, 2014.
Aim: “To change the culture and climate in the District to one of health and wellness linked to school improvement plans (Dr. Sue Baldwin, District Wellness Coordinator).” –ASCD, 2016

Assessing Needs 1. CDC YRBSS
- all students grades 6-12 district-wide
2. CDC School Health Index
- all schools with School Wellness Team; create 24 actions (3 per module)
3. Rudd Center Wellness School Assessment Tool (WellSat 2.0)
- every four years assess and update District Wellness Policy
4. ASCD School Improvement Tool

Social, Environmental, and Political Conditions: Department of Health and Human Services [DHHS], 2016
https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health

Coordination of Efforts
Tool Implementation District Wellness Policy/School-Level Mandates:
Create a comprehensive School Wellness Team (SWTs)
Conduct the School Health Index (SHI) needs assessment every 2 years (@ 7
hours with team))
Conduct the NYS Heart Check assessment every 2 years
Conduct the Youth Risk Behavior Survey (YRBS) every 2 years (2015: trend
data October 5-16th)

Group Activity: Assess YRBSS Tool You have been provided the oral health questions we integrated into our District YRBSS Surveying activities. 1. Please go through the YRBSS materials provided to
you and respond to the questions provided. 2. Please give your presenters your answer
sheets/packets before leaving this Session.

Group Activity: Assess SHI Tool You have been provided with the SHI activity packets. Please complete the activity and leave your completed packets with your presenter(s) prior to exiting this Session.

Group Activity: Assess WellSat Tool You have been provided with the WellStat Tool and 6 individual packets. 1. Please complete your activity which includes adding oral
health either through incorporation of current sections (integrated) or create changes for a standalone section.
2. Please discuss as a group and give the activity paper packets back to your presenters before leaving this session.

Group Activity: Assess SIT Tool You have been provided with a SIT packet. Please use the information within this packet and incorporate possible inclusion of oral health components currently not contained within this tool / utility. Please respond to the questions provided to you and hand them to your presenter(s) before leaving this session.

Conclusions: Healthy children are better learners!
Success in school equates to successes in life
Linked to a higher socioeconomic status in adulthood
Healthier adults = increased health literacy and equity
Healthier communities / environments

"Coming together is a beginning. Keeping together is progress. Working together is success."
Henry Ford ASHA, 2016: PRESENTATION #PS26

And you think your having a bad day?

Sue Baldwin, PhD, MCHES, FASHA District Wellness Coordinator [email protected]
716-816-3912
Renee Retton Doctoral Student, MS, CHES
716-804-3215
Thank You

References
1. Association for Supervision and Curriculum Development. (2016). Whole school, whole community, whole child model: examples and ideas for implementation. Retrieved from http://www.ascd.org/ASCD/pdf/siteASCD/wholechild/WSCC_Examples_Publication.pdf
2. Centers for Disease Control and Prevention. (2014). Children’s oral health. Retrieved from http://www.cdc.gov/oralhealth/children_adults/child.htm
3. Department of Health and Human Services. (2016). Social determinants of health. Retrieved from https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health
4. Dye BA, Xianfen L, Beltrán-Aguilar ED. Selected Oral Health Indicators in the United States 2005–2008. NCHS Data Brief, no. 96. Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention; 2012.
5. Kwan SY, Petersen PE, Pine CM, Borutta A. 2005. Health-promoting schools: An opportunity for oral health promotion. Bulletin of the World Health Organization 83 (9): 677-685.