
www.pspbc.ca
Bilateral Knee Osteoarthritis Case 6 : Ruth-Ann

2
Faculty/Presenter Disclosurewith Faculty’s Name:
Faculty’s Name: Faculty’s Name:
3
Disclosure of Commercial Support
.
Mitigating potential biasN/A N/A
.
N/A

4
Objectives
When working with CPP, you will be able to:
Identify key elements of osteoarthritis history
List 3 assessment tools that may be useful
Identity appropriate investigations Appropriate management
5
Bilateral Knee Pain
Ruth Ann is a 62 yr old retired elementary school teacher
She was touring through Europe 3 weeks ago when she tripped on some cobblestone roads and landed straight on her knee caps. She noticed some initial mild swelling the next day but had significant swelling and pain after flying home.
She is gradually improving but still complains of anterior and medial pain bilaterally especially with descending stairs, prolonged standing greater than 15 minutes and with using the elliptical machine at the gym.
6
What are your Key Questions?
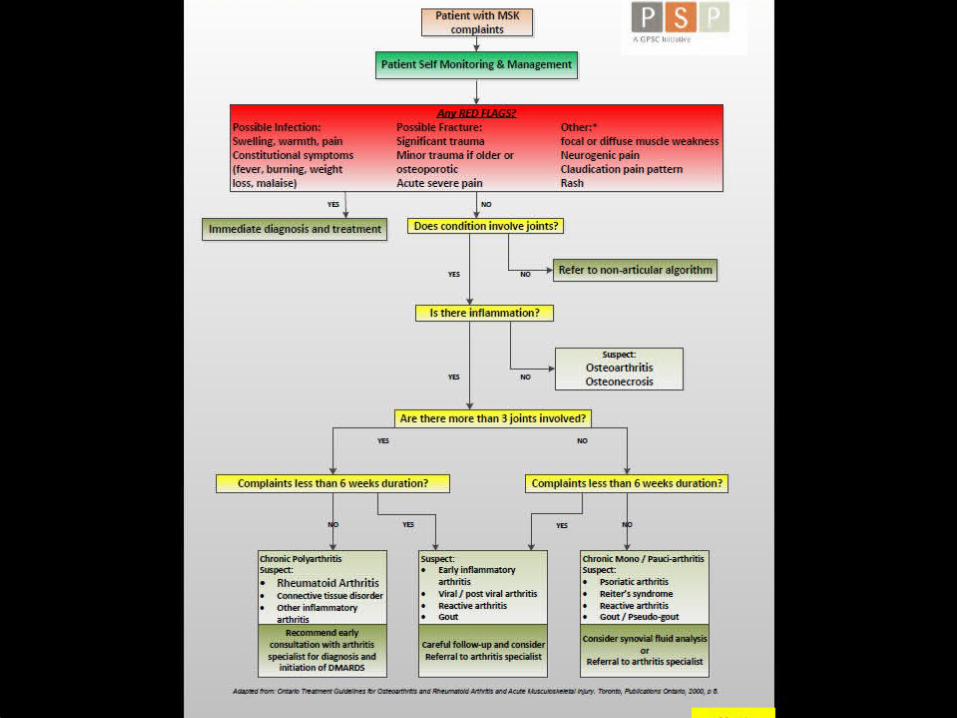
How do you determine if this is osteoarthritis or a structural trauma?

7
Common Patient History for MSK Complaints
8
History
Prior to her fall 3 weeks ago, she complained of intermittent knee pain with long walks and gardening. She had never sought medical care for this complaint but often used a menthol rub for relief of aching.
She currently describes intermittent deep aching, like a bruise, that is combined with occasional sharp pain under her knee cap especially with going down stairs.
She get relief with heat and rest.
9
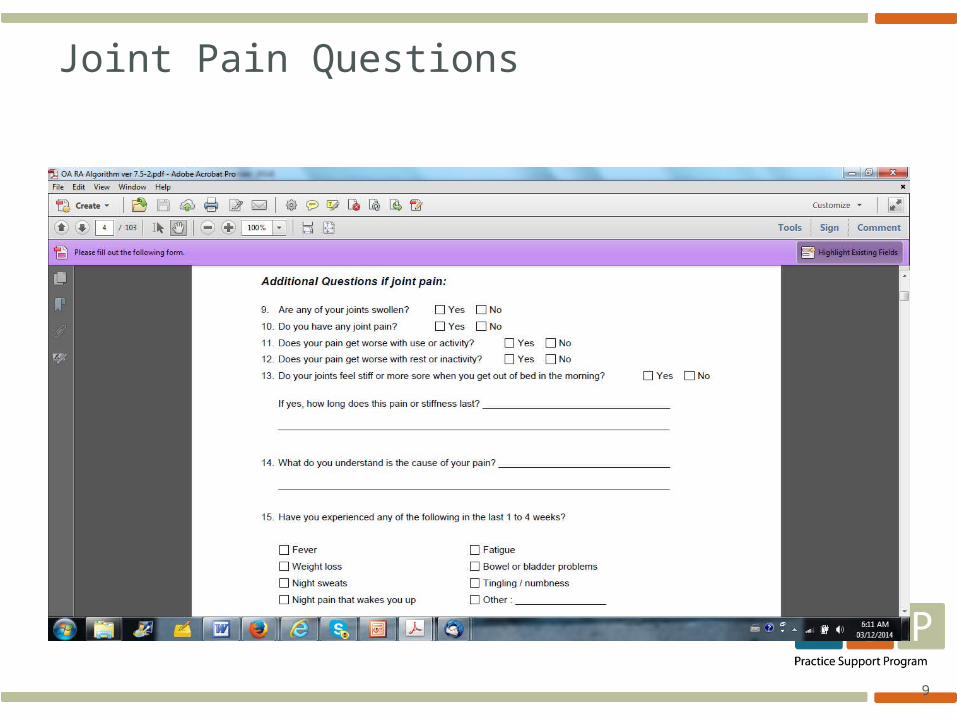
Joint Pain Questions
10
11
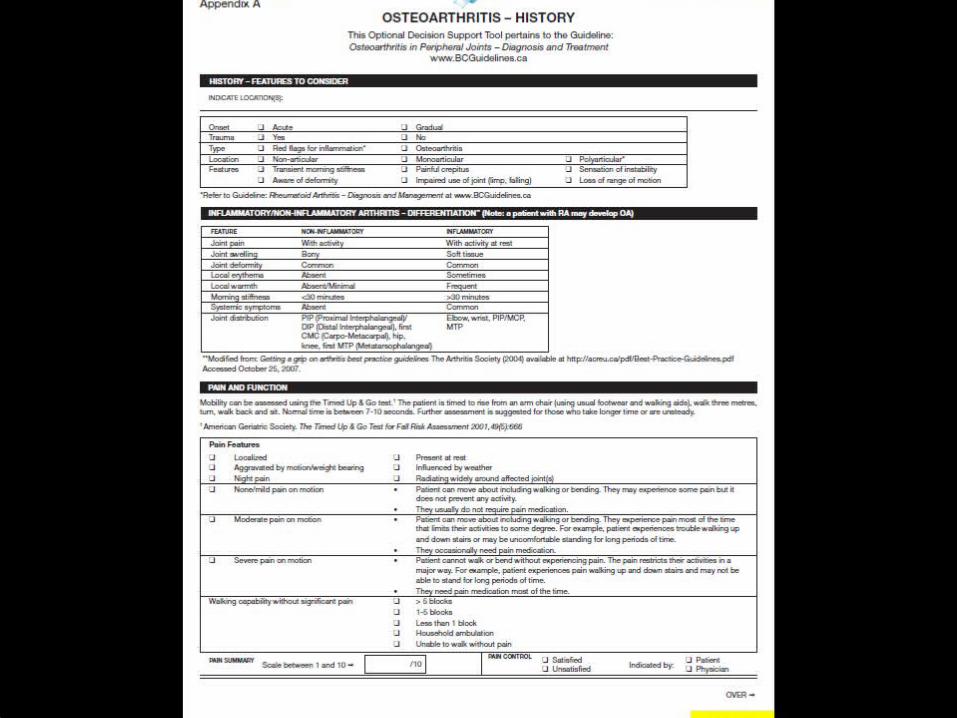
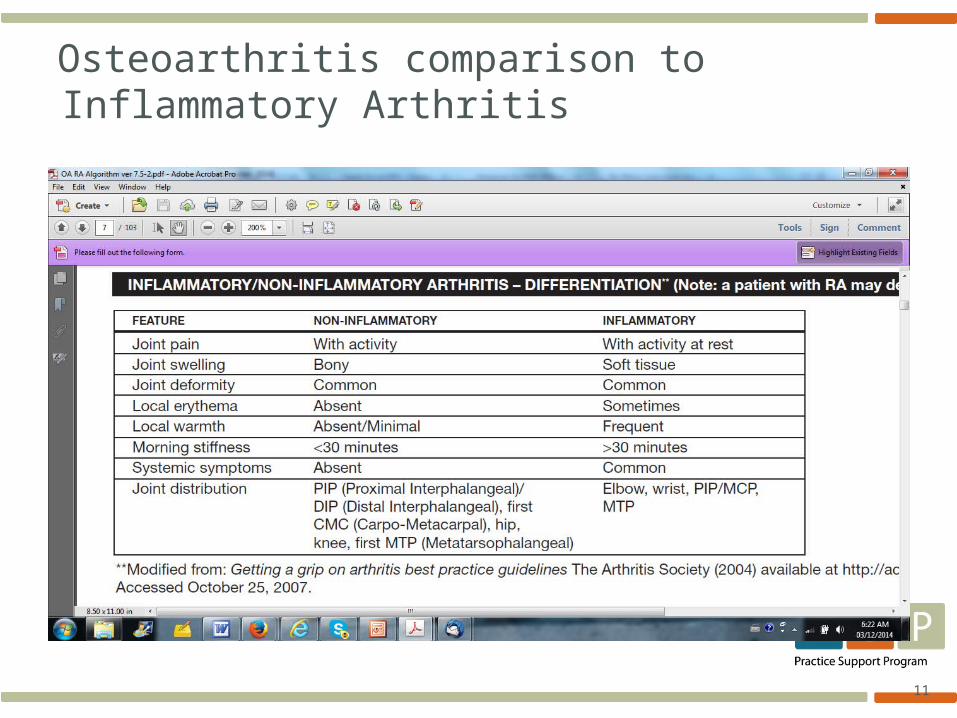
Osteoarthritis comparison to Inflammatory Arthritis

12
Brief Pain Inventory Screen

13
Knee Symptoms indicating Structural Instability
Swelling
Locking
Giving Way
Clicking
Sudden, large effusion versus small delayed swelling
Knee is stuck in position, indicative of meniscal tear
Knee buckles, unexpected fall, instability from ligament tear, large meniscal tear
Common and often non-painful, often patellar related
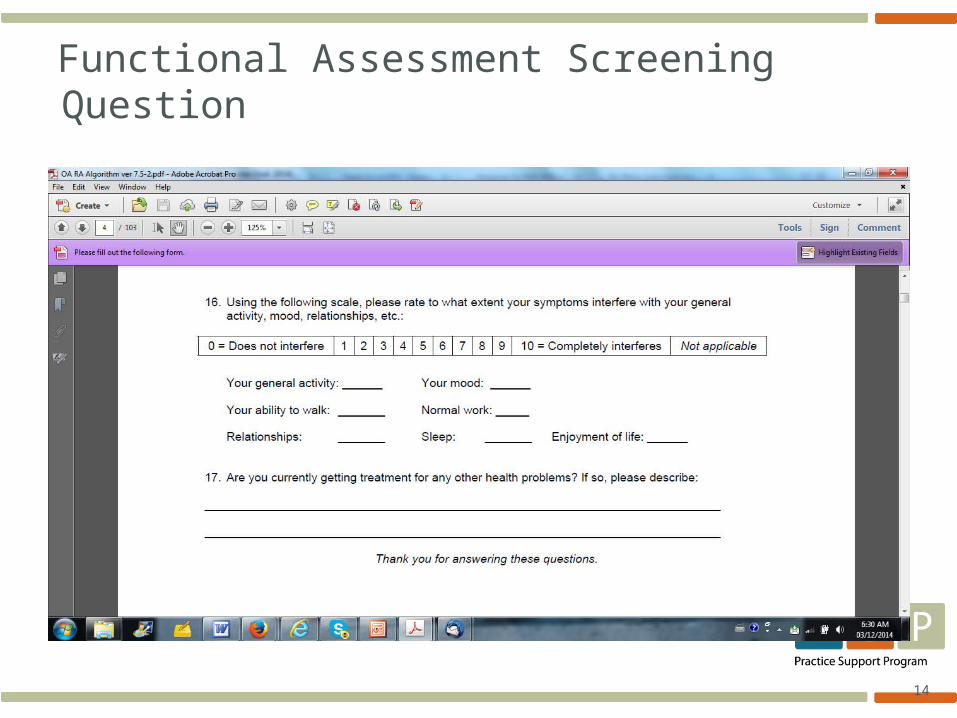
14
Functional Assessment Screening Question
15
16
17

18
19
Physical Exam What physical examination techniques would
you use?We found:
Right Knee active flexion 110 degrees - pain end range, Passive flexion is 125 degrees - pain end range.
Left Knee active and passive flexion is full.
Patellar compression causes pain on right knee
Mild Joint effusion on right knee
Ligaments and mensici are intact
Gait demonstrates mild limp on right for first 5 steps then normalizes.

20
Physical Exam
21
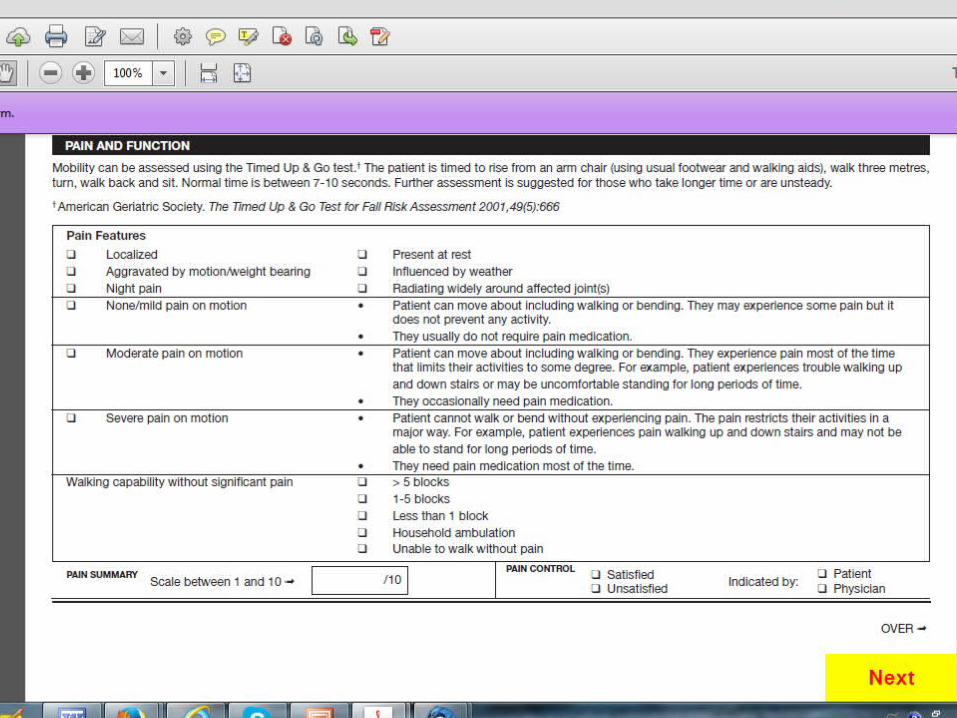
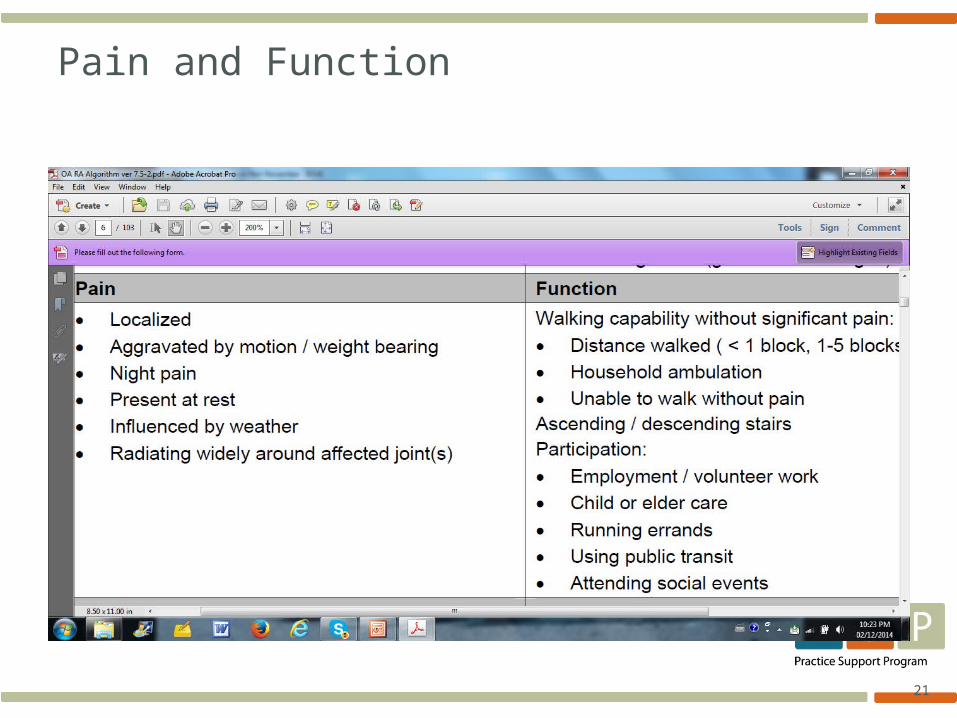
Pain and Function

22
23
Management Tools
How would you determine if investigations were appropriate ?
We used:
a) Is there poor or no response to appropriate treatment?
b)Are pain levels unmanaged with best medications?
c) Are there prolonged rheumatological symptoms greater than 6 weeks ?

24
25
What is best Management
Ruth-Ann has mild to moderate osteoarthritis likely in the patellar and medial compartments
Her pain is improving but she is hesitant to continue with activity for fear of flaring her symptoms
Best Practice would focus on: Medications Rehabilitation and Exercise Patient Education and Self- Management

26
Pain Relief

27
Pain Relief
28

29
30
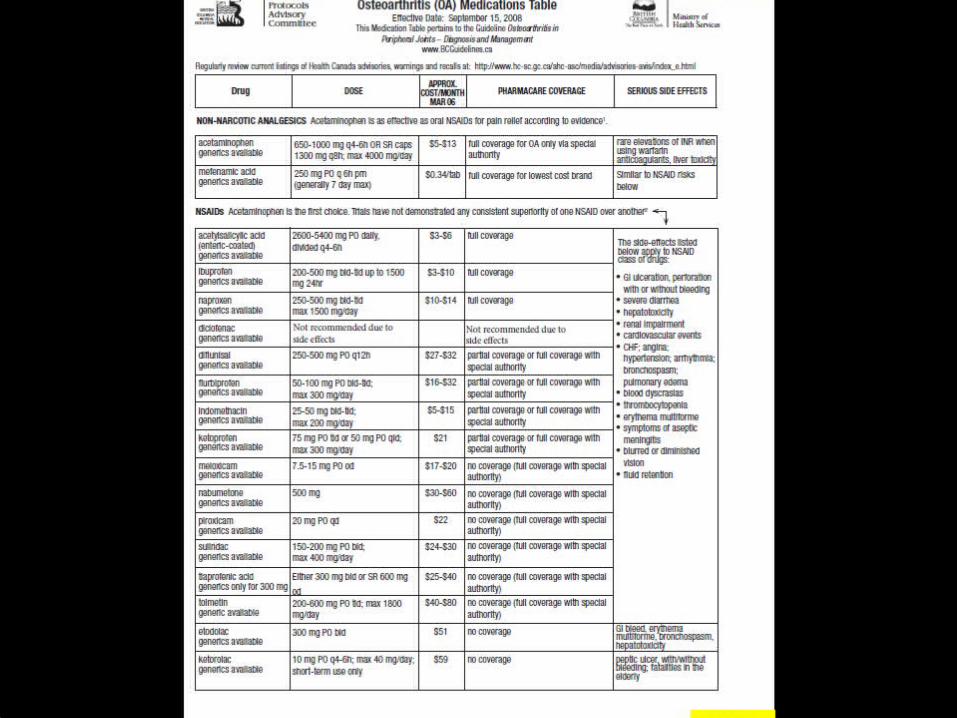
Medication Advice
Acteominophen extended release 650mg TID, po x 7 days then prn
When to use an NSAID? When to use a Topical ? When to recommend Injection?
31
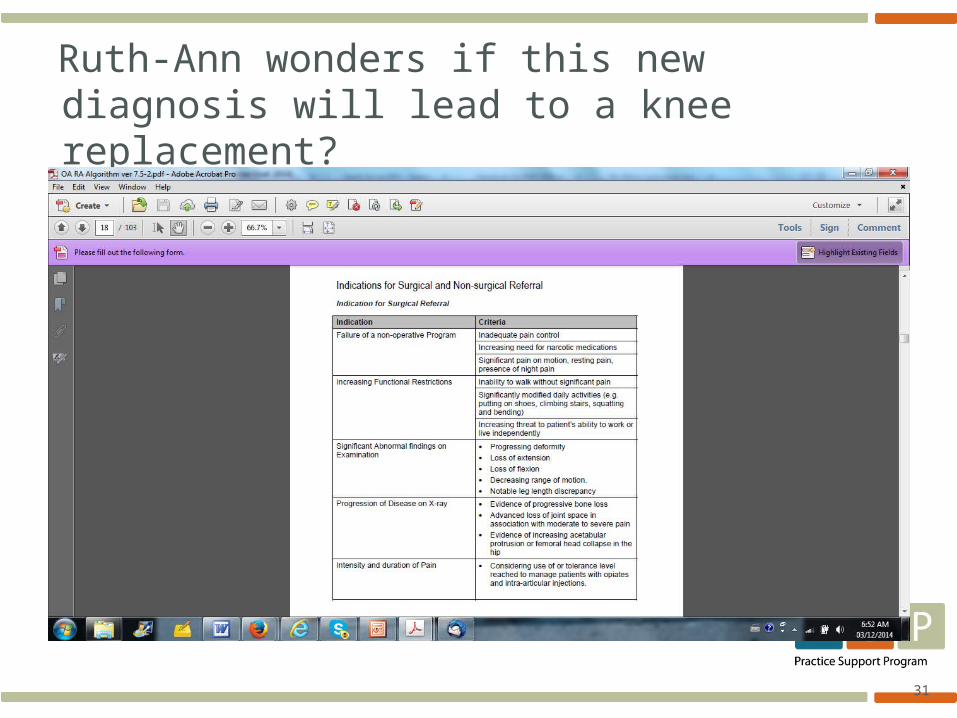
Ruth-Ann wonders if this new diagnosis will lead to a knee replacement?
32
33
Follow-Up
Monitor and Manage Swelling Pain Function
Enhance Education Promote Self-Management
34
35
36
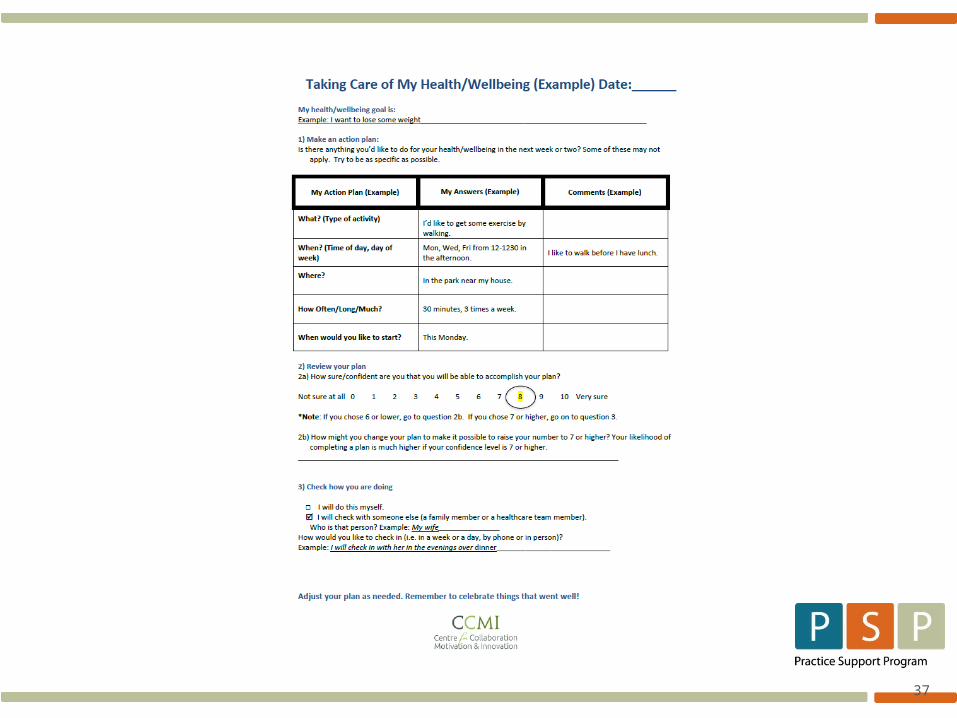
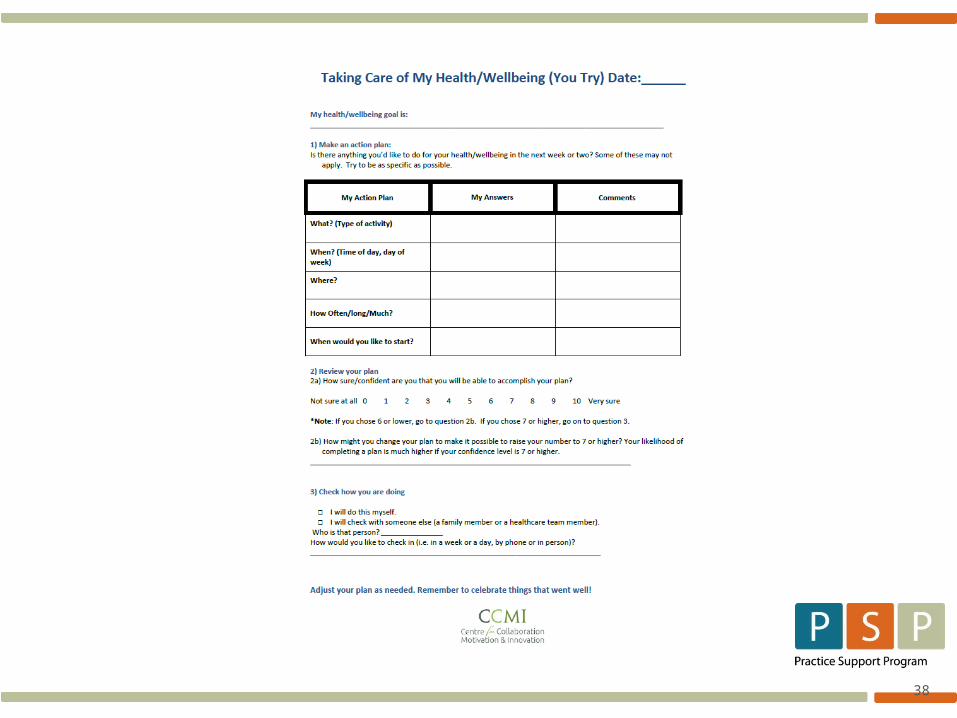
Goal Setting
Ruth-Ann is improving on her follow-up visit 3 weeks later.
She is using occasional pain medication after prolonged activity
She is back to her daily activities She would like to discuss “safe exercise” as
she has decided to join a seniors gym program and lose some weight.
37
38
39
40
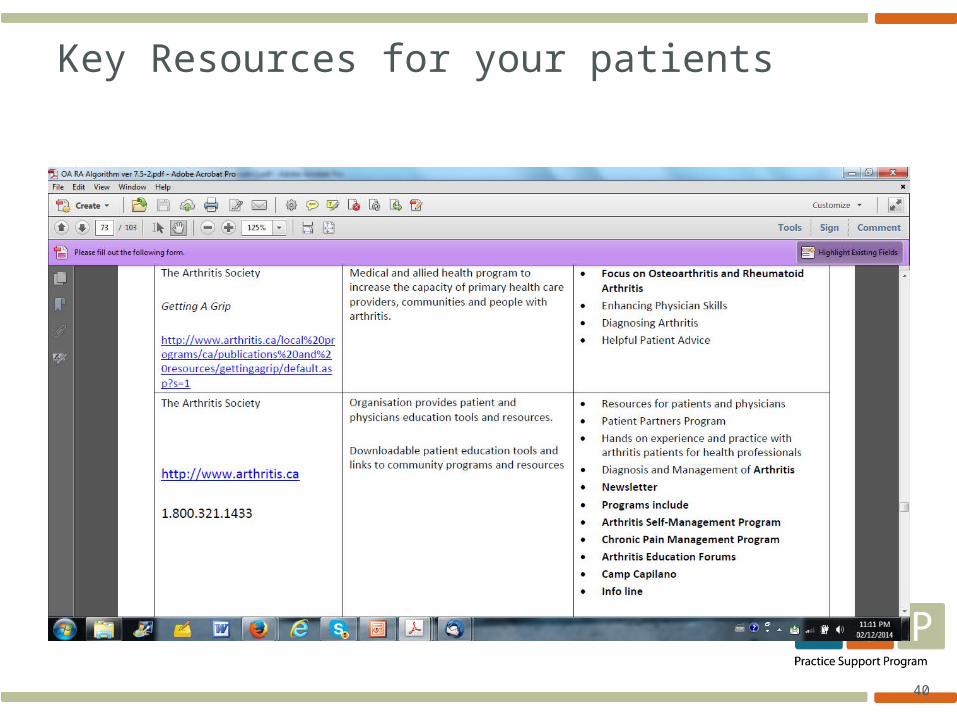
Key Resources for your patients

41
Clinical Impression Bilateral Knee Osteoarthritis
Right worse than left Patellar and Medial compartments
Mild to Moderate Pre-existing mild with moderate exacerbation
after trauma
Managed with pain medications, rehabilitation exercise, education and promotion of self management
Investigations if concerned about inflammatory symptoms
Xrays if suspected fracture or for OA prognosis

42
Key Clinical Information
What are the key criteria for Osteoarthritis? Morning Stiffness less than 30 min. Intermittent Pain associated with activity Recurrent episodes May lead to bony deformity and decreasing
function
43
Summary
When working with Osteoarthritis, it is important to:
- Identify the differences between inflammatory and non-inflammatory joint disease
- Focus on Pain and Function in assessment and management
- Focus on patient self management for lifestyle factors
44
References
Arthritis Resource Guide, Arthritis .ca
Guidelines and Protocols Advisory Committee Bcguidelines.ca







