2
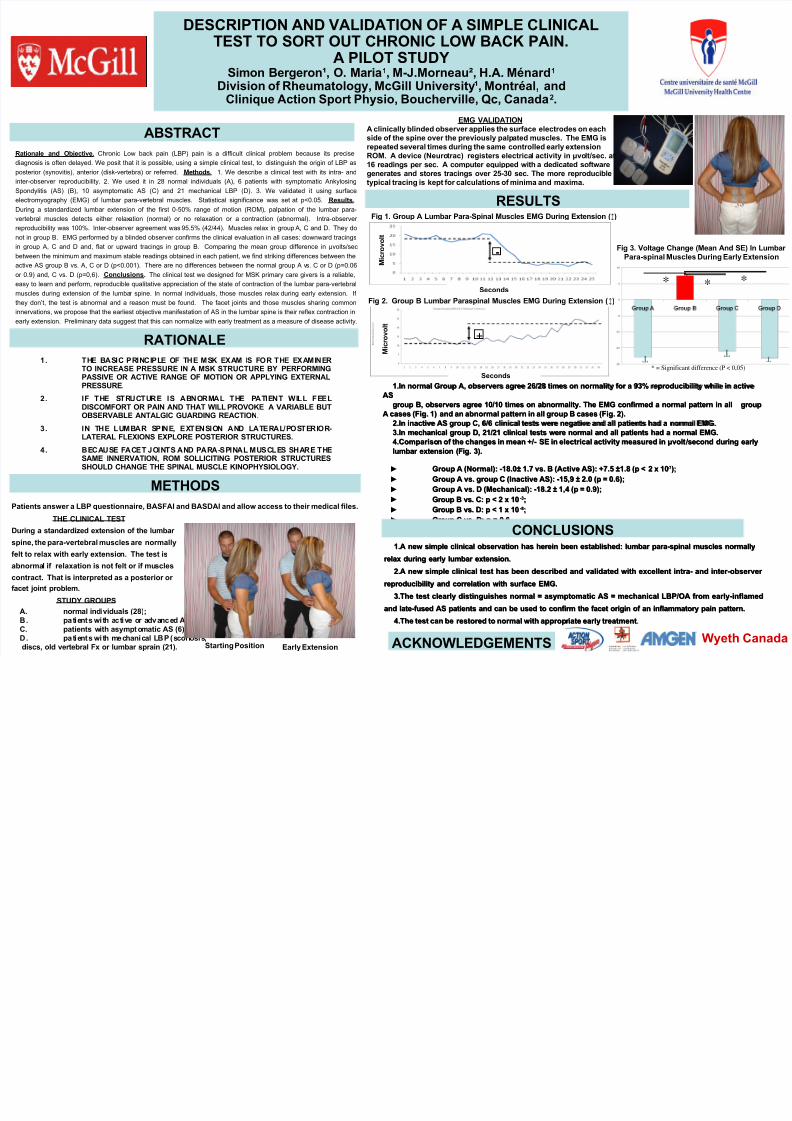
DESCRIPTION AND VALIDATION OF A SIMPLE CLINICAL TEST TO SORT OUT CHRONIC LOW BACK PAIN. A PILOT STUDY Simon Bergeron¹, O. Maria 1 , M-J.Morneau², H.A. Ménard 1 Division of Rheumatology, McGill University ¹, Montréal, and Clinique Action Sport Physio, Boucherville, Qc, Canada 2 . 1. 1.A new simple clinical observation has herein been established: lumbar para-spinal muscles normally A new simple clinical observation has herein been established: lumbar para-spinal muscles normally relax during early lumbar extension. relax during early lumbar extension. 2. 2.A new simple clinical test has been described and validated with excellent intra- and inter-observer A new simple clinical test has been described and validated with excellent intra- and inter-observer reproducibility and correlation with surface EMG. reproducibility and correlation with surface EMG. 3. 3.The test clearly distinguishes normal = asymptomatic AS = mechanical LBP/OA from early-inflamed The test clearly distinguishes normal = asymptomatic AS = mechanical LBP/OA from early-inflamed and late-fused AS patients and can be used to confirm the facet origin of an inflammatory pain pattern. and late-fused AS patients and can be used to confirm the facet origin of an inflammatory pain pattern. 4. 4.The test can be restored to normal with approp riate early treatment The test can be restored to normal with appropr iate early treatment. Rationale and Objective. Chronic Low back pain (LBP) pain is a difficult clinical problem because its precise diagnosis is often delayed. We posit that it is possible, using a simple clinical test, to distinguish the origin of LBP as posterior (synovitis), anterior (disk-vertebra) or referred. Methods. 1. We describe a clinical test with its intra- and inter-observer reproducibility. 2. We used it in 28 normal individuals (A), 6 patients with symptomatic Ankylosing Spondylitis (AS) (B), 10 asymptomatic AS (C) and 21 mechanical LBP (D). 3. We validated it using surface electromyography (EMG) of lumbar para-ve rtebral muscles. Statistical significance was set at p<0.05. Results. During a standardized lumbar extension of the first 0-50% range of motion (ROM), palpation of the lumbar para- vertebral muscles detects either relax ation (normal) or no relaxation or a contraction (abnormal). Intra-observer reproducibility was 100%. Inter-observer agreement was 95.5% (42/44). Muscles relax in group A, C and D. They do not in group B. EMG performed by a blinded observer confirms the clinical evaluation in all cases: downward tracings in group A, C and D and, flat or upward tracings in group B. Comparing the mean group difference in μvolts/sec between the minimum and maximum stable readings obtained in each patient, we find striking differences between the active AS group B vs. A, C or D (p<0.001). There are no differences between the normal group A v s. C or D (p=0.06 or 0.9) and, C vs. D (p=0,6). Conclusions. The clinical test we designed for MSK primary care givers is a reliable, easy to learn and perform, reproducible qualitative appreciation of the state of contraction of the lumbar para-vertebral muscles during extension of the lumba r spine. In normal individuals, those muscles relax during early extension. If they don’t, the test is abnormal and a reason must be found. The facet joints and those muscles sharing common innervations, we propose that the earliest objective manifestation of AS in the lumbar spine is their reflex contraction in early extension. Preliminary data suggest that this can normalize with early treatment as a measure of disease activity. 1. 1.In normal Group A, observers agree 26/28 times on normality for a 93% reproducibility while in active In normal Group A, observers agree 26/28 times on normality for a 93% reproducibility while in active AS AS group B, observers agree 10/10 times on abnormality. The EMG confirmed a normal pattern in all group B, observers agree 10/10 times on abnormality. The EMG confirmed a normal pattern in all group group A cases (Fig. 1) and an abnormal pattern in all group B cases (Fig. 2). A cases (Fig. 1) and an abnormal pattern in all group B cases (Fig. 2). 2. 2.In inactive AS group C, 6/6 clinical tests were negative and all patients had a normal EMG. In inactive AS group C, 6/6 clinical tests were negative and all patients had a normal EMG. 3. 3.In mechanical group D, 21/21 clinical tests were normal and all patients had a normal EMG. In mechanical group D, 21/21 clinical tests were normal and all patients had a normal EMG. 4. 4.Comparison of the changes in mean +/- SE in electrical activity measured in Compariso n of the changes in mean +/- SE in electrical activity measured in μ μvolt volt /second during early /second during early lumbar extension (Fig. 3). lumbar extension (Fig. 3). ▶ Group A (Normal): -18.0± 1.7 vs. B (Active AS): +7.5 ±1.8 (p < 2 x 10 Group A (Normal): -18.0± 1.7 vs. B (Active AS): +7.5 ±1.8 (p < 2 x 10 -7 -7 ); ); ▶ Group A vs. group C (Inactive AS): -15,9 ± 2.0 (p = 0.6); Group A vs. group C (Inactive AS): -15,9 ± 2.0 (p = 0.6); ▶ Group A vs. D (Mechanical): -18.2 ± 1,4 (p = 0.9); Group A vs. D (Mechanical): -18.2 ± 1,4 (p = 0.9); ▶ Group B vs. C: p < 2 x 10 Group B vs. C: p < 2 x 10 -3 -3 ; ▶ Group B vs. D: p < 1 x 10 Group B vs. D: p < 1 x 10 -8 -8 ; ; ▶ Group C vs. D: p = 0.6 Group C vs. D: p = 0.6 ABSTRACT EMG VALIDATION A clinically blinded observer applies the surface electrodes on each side of the spine over the previously palp ated muscles. The EMG is repeated several times during the same controlled early extension ROM. A device (Neuro trac) registers electrica l activity in μvo lt/sec. at 16 readings per sec. A computer equipped with a dedicated software generates and stores tracings over 25-30 sec. The more reproducible typical tracing is kept for calculations of minima and maxima. Fig 3. Voltage Change (Mean And SE) In Lumbar Para-spinal Muscles During Early Extension T T T T * * * * = Significant difference (P < 0,05) 1. TH E BASIC PRINCI PL E OF T HE MS K EXAM I S FOR THE EXAMI NER TO INCREASE PRESSURE IN A MSK STRUCTURE BY PERFORMING PASSIVE OR ACTIVE RANGE OF MOTION OR APPLYING EXTERNAL PRESSURE. 2. IF THE S TR UCTU RE IS ABNORMAL THE P AT IENT WI LL FEEL DISCOMFORT OR PAIN AND THAT WILL PROVOKE A VARIABLE BUT OBSERVABLE ANTALGIC GUARDING REACTION. 3. IN T HE LUMBAR S P IN E, EX TE N SI ON AND LATERAL / PO ST ER IO R- LATERAL FLEXIONS EXPLORE POSTERIOR STRUCTURES. 4. BEC AU SE FA CE T J OI NT S A ND PA RA -S PI NA L M USCL ES SH AR E THE SAME INNERVATION, ROM SOLLICITING POSTERIOR STRUCTURES SHOULD CHANGE THE SPINAL MUSCLE KINOPHYSIOLOGY. Patients answer a LBP questionnaire, BASFAI and BASDAI and allow access to their medical files. THE CLINICAL TEST During a standardized extension of the lumbar spine, the para-vertebral muscles are normally felt to relax with early extensio n. The test is abnorma l if relaxation is not felt or if mu scles contract. That is interpreted as a posterior or facet joint problem. STUDY GROUPS A. normal individuals (28); B. pa ti ent s wit h a ct iv e or adv anc ed A S (1 0) ; C. patients with asympto matic AS (6); D. pat ie nts wit h mec hanic al LBP (s coli osis , discs, old vertebral Fx or lumbar sprain (21). Starting Position Early Extension RATIONALE RESULTS + Fig 1. Group A Lumbar Para-Spinal Muscles EMG During Extension (↕) - Fig 2. Group B Lumbar Paraspinal Muscles EMG During Extension (↕) Seconds M i c r o v o l t M i c r o v o l t Seconds METHODS CONCLUSIONS ACKNOWLEDGEMENTS Wyeth Canada