46
UPPER GASTROINTESTINAL BLEEDING
| Date post: | 16-Feb-2016 |
| Category: |
Documents |
| Upload: | rashed-shatnawi |
| View: | 4 times |
| Download: | 0 times |

UPPER GASTROINTESTINAL
BLEEDING

Definition • Hemorrhage in the upper
gastrointestinal tract.• The anatomic cut-off for upper GI
bleeding is the ligament of Treitz, which connects the fourth portion of the duodemum to the diaphragm near the splenic flexure of the colon.
• Common. Incidence about 300 per 100000
• Mortality 5-10% and increased in elderly

CAUSES ?


PEPTIC ULCERSCommon sites for peptic ulcers are the first
part of the duodenum and the lesser curve of the stomach.
In general, the ulcer occurs at a junction between different types of epithelium, it occurs in the epithelium least resistant to acid damage.
infection with H. pylori is the most important factor in the development of peptic ulceration.
other factors: NSAIDs, Cigarette smoking…

Duodenal ulceration• Most duodenal ulcers occur in the first
part of the duodenum.• Anteriorly placed ulcers tend to
perforate and, in contrast, posterior duodenal ulcers tend to bleed, sometimes by eroding a large vessel such as the gastroduodenal artery.
• malignancy in this region is uncommon.

Gastric ulcerationSame as with duodenal ulceration, H. pylori,
NSAIDs and smoking are the important etiological factors in gastric ulceration.
gastric ulceration is substantially less common than duodenal ulceration.
equal between the sexes.population with gastric ulcers tends to be
older age.more prevalent in low socioeconomic
groups.

• Large chronic ulcers may erode posteriorly into the pancreas and, on other occasions, into major vessels such as the splenic artery.
• Less commonly, they may erode into other organs such as the transverse colon.
• Chronic gastric ulcers are associated with malignancy.

Clinical features of peptic ulcers
• Epigastric pain • Periodicity • Alteration in weight • Bleeding • Vomiting
Complications of peptic ulceration
• Perforation• Bleeding• Stenosis

GASTRIC EROSIONS• occurs when the mucous
membrane lining the stomach becomes inflamed
• Common in elderly especially those taking NSAIDs.
• Fortunately, most such bleeding settles spontaneously.

MALLORY–WEISS SYNDROME
In Mallory–Weiss syndrome, vigorous vomiting produces a vertical split in the gastric mucosa, immediately below the squamocolumnar junction.
at the cardia in 90% of cases. In only 10% is the tear in the
oesophagus.The condition presents with
haematemesis.

DIEULAFOY’S DISEASEIs a gastric arterial venous malformation
that has a characteristic histological appearance.
The lesion itself is covered by normal mucosa and, when not bleeding, it may be invisible.
If it can be seen during the bleeding, all that may be visible is profuse bleeding coming from an area of apparently normal mucosa.

AORTOENTERIC FISTULAConsidered in any patient with haematemesis
and melena that cannot be otherwise explained.
bleeding from such patients is not always massive, although it can be.
The vast majority of patients will have had an aortic graft
It is usually secondary to an abdominal aortic aneurysm repair.
CT angiography scan typically allow the diagnosis to be made with certainty.
In the endoscopy you will find nothing.

Other causes Stress ulceration
commonly occurs in patients who have a major injury or illness, who have undergone major surgery or who have a major comorbidity.
Curling’s ulcer : is the stress ulceration that occur in burn patients.
Cushing’s ulcer: is the stress ulceration that occur in patients with head injury.
only 5% develop significant gastric bleeding.

NSAID 50% of patients > 60 yr presented with UGIB has history of NSAID.
Poorly controlled Anticoagulant therapy.

Signs & Symptoms of UGIB• Hematemesis• Melena• Syncope• Shock• Fatigue• Hematochezia• Epigastric pain• Weight loss
Hematemesis is the vomiting of blood that is either bright red or resembling coffee-ground in appearance. Usually indicates a bleeding source proximal to the ligament of treitz. Coffee-ground hematemesis indicates that the blood has been in contact with gastric acid long enough to become converted from hemoglobin to methemoglobin.
Melena is the passage of black, usually tarry, stools. Although melena signifies a longer time within the GI tract than bright red blood, it does not guarantee that the bleeding is from the upper tract.

•Hematochezia is the passage of bright red blood by rectum. Although it indicates GI bleeding, it does not specify the level within GI tract. (if profuse, UGIB)


RISK FACTORS• Aspirin / NSAIDS / anticoagulant /
steroid • Cigarettes , alcohol• Recurrent vomiting• Burn / trauma• Liver disease , hx of PUD ,
esophageal varices, portal hypertension

MANAGEMENT• Three steps:
oResuscitationoEstablishment of a diagnosisoManagement of specific conditions

1. RESUSCITATION• ABC (pulses, Measure BP and HR)
- hypotensive & tachycardia with upper GI bleeding
• Two large IV lines• Protect airway and give high-flow
oxygen• NPO: for 24 hr

• Draw blood samples for:A. CBC (Hb,platelets…).B. KFT (K,Na,Urea,Creatinine…)C. LFT.(13% of UGIB is secondary
to liver dis. …)D. PT, PTT.( liver dis. , inadequately
controlled warfarin therapy…)E. Blood group and cross match.

• IV plasma expanders: Crystalloid(ringer lactate) or colloid (Hess).
• Admission (if SBP < 100 or HR >100 ICU admission).
• Start blood transfusion when ready.• How much to give? It depends on the
patient response to resuscitation… we monitor by:
1-Insert Foley’s catheter: to monitor the urine out put hourly(discard 1st pass..). Must be >30 ml/hr
2-CVP line: used either for fluid replacement or for monitoring intracardiac pressure.

• NG tube- blood upper - bile & gastric contents not upper- only gastric contents endoscopy to rule out duedonal bleeding…)

2. ESTABLISHMENT OF A DIAGNOSIS
•After stabilization Upper GI endoscopy.•Never send a patient with upper GI bleeding to endoscopy while he is hemodynamically unstable.
•Doing endoscopy depends on many factors: ideally should be within 24 hrs of admission, but the perfect situation is to be done within 4 hours from stabilization.

Advantages of endoscopy:
1. Determination of the size and number of lesions in most cases.
2. Assessment of which site is actively bleeding
3. Assessment of rate of bleeding.4. Distinction between an ulcer, varices,
gastritis and a tear in the esophagus(Mallory-weiss syndrome) that follows forceful vomiting.
5. Determination of whether a lesion is benign or malignant.
6. Therapeutic hemostatic procedures “adrenaline, laser diathermy, cautery …”

MANAGEMENT OF SPECIFIC CONDITIONS
1. BLEEDING Duodenal ulcer: The bleeding artery is the gastroduodenal
artery (branch of right gastirc artery) Methods of stopping bleeding:
1. Inject Adrenaline:2. Cautery3. Laser.
The bleeding stops and the patient stays 1-2 days NPO given PPI for 6 weeks, after 1-2 days the patient can eat and drink.
Alcohol also stop bleeding but it cause necrosis of the duodenal wall and may lead to perforation

2. BLEEDING Gastric ulcer:
• Same modality for treatment of doudenal ulcer but we give him PPI for 8 weeks plus eradication for H.pylori.
• Gastric Ulcer could be MALIGNANT but looks benign. Should take biopsy to rule out malignancy .

3. ESOPHAGEAL VARICES• High mortality and morbidity and high
recurrence rate.1) Injection sclerotherapy :
“ethanolamine or Tetradecaylsulfate.”2) Rubber band ligation : by endoscope3) Transjugular intrahepatic porto-
systemic shunt (TIPSS) : the shunt inserted using fluoroscopic or Ultrasonography guidance through IJV and SVC , between the hepatic vein and portal vein which will treat the portal hypertension .

4) Blakemore Sengstaken (Manisota) tube : A tube which has 4 lumens labeled EI : Esophageal inflation EA : Esophageal aspirationGI : Gastric inflationGA : Gastric aspirationInsert the tube through the mouth, by GA aspirate
the gastric blood, then by GI inflate by 250 ml saline, we pull the tube from the mouth so the GI part will press at the gastric element of Gastro-esophageal varices, if the bleeding continue ..
By EA we aspirate esophageal blood the by EI inflate by air (not saline) and monitor the pressure not to be more than 35 mmHg .
Keep the tube for 24 hours, deflate, re-check if there is re-bleeding


5) Gastric deconnection.6) Gastric transection

4. GASTRIC EROSIONS
• Treatment is conservative Nil by mouthIV H2 blocker or proton pump inhibitor.
Total gastrectomy for persistent bleeding “high mortality”

5. MALLORY-WEISS TEAR• Conservative, NPO, blood transfusion
if needed, local injection of adrenaline
If bleeding persist do Laparotomy-Direct suturing.

6. Vascular malformations “Dieulafoy’s disease”
Endoscopic hemostasis.◦ Adrenaline injection ,
electrocoagulation, injection sclerotherapy, heater probe, laser photocoagulation
7. Portal hypertensive gastropathy
• one in seven patients with portal hypertensive gastropathy will develop bleeding
• Treatment :Electrocautery , cryotherapy by
endoscopeTIPSS

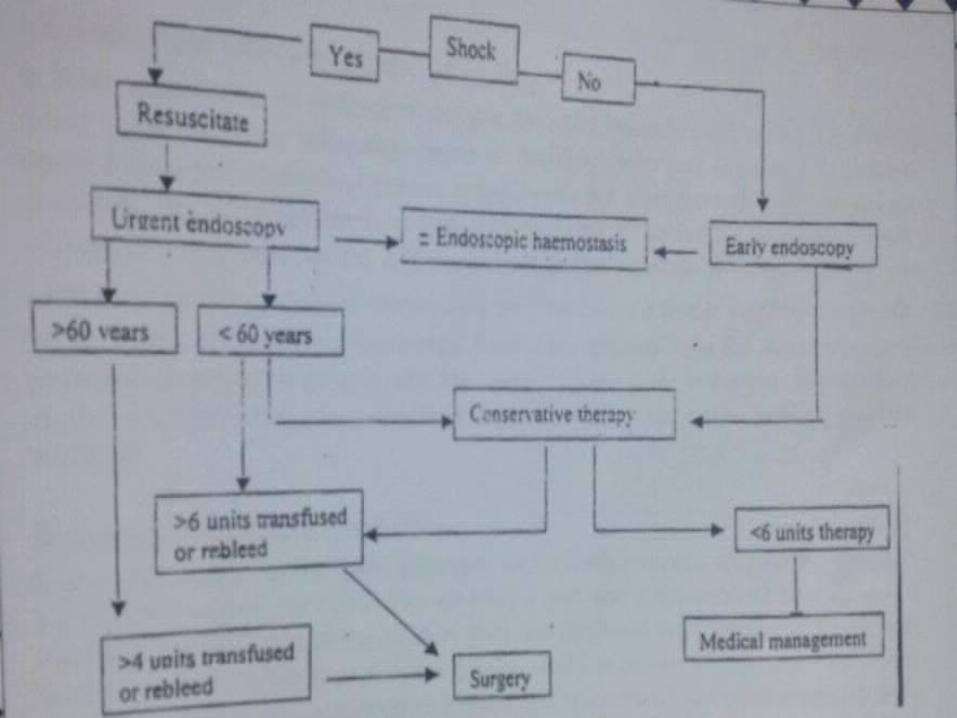
HEMODYNAMICALLY UNSTABLE PATIENT
In the cases of giving the pt blood and no improvement or in cases of significant rebleeding
Indication for surgery depends on age1. >60 years if needs > 4 units of blood2. <60 years if needs > 6 units of blood
Emergency surgery◦ In bleeding DU, open the duodenum and
do “ figure of eight stitch”

Aorto-enteric fistula• Aortic aneurysm graft• Any pt who has upper GI bleeding and a
history of aortic surgery suspect aorto-duodenal fistula
• Because of high morbidity and mortality associated with AEF , surgery is always recommended
• However , the morbidity and mortality of treated AEF is also high 75%

ROCKALL’S RISK SCORE• Score that predicts poor prognosis,
i.e. death, from upper GI haemorrhage
• It uses clinical criteria (increasing age, co-morbidity, shock) as well as endoscopic finding (diagnosis, stigmata of acute bleeding)

Variable Score
0 1 2 3
Age (years) <60 60-79 >80
Shock Pulse rate SBP (mmHg)
“No shock”
< 100 > 100
“Tachycardia”,
> 100 > 100
“Hypotension”
< 100
Comorbidity No Cardiac failure, ischaemic heart disease, any major comorbidity
Renal failure, liver failure, disseminated malignancy
Diagnosis Mallory-Weiss tear, no lesion identified and no SRH/blood
All other diagnosis
Malignant lesion of UGIT
Major SRH(Stigmata of recent heamorrhage)
None or dark spot only
Blood in the UGIT, adherent clot, visible or spurting vessel

Score %of Total Rebleeding Death
0 5.6 4.9 0
1 11 3.2 0
2 12.8 5 0.3
3 15.9 12.2 2
4 17.8 13.8 4.2
5 14.5 16.9 7.9
6 9.4 29.4 15.1
7 8 39.6 19.8
<8 5.1 47.7 39.1

Score Mean Hospital Stay (days)
0 3.7
1 4.1
2 6.1
3 7.6
4 9.3
5 10.8
6 10.6
7 12.7
<8 15.3
Total 8.6

THANK YOU

















