Get Homework/Assignment Done Homeworkping.com Homework Help https://www.homeworkping.com/ Research Paper help https://www.homeworkping.com/ Online Tutoring https://www.homeworkping.com/ click here for freelancing tutoring sites
COLEGIO DE SAN JUAN DE LETRAN – CALAMBASchool of Nursing
Brgy. Bucal, Calamba City
Case StudyOn
COLON CANCER
Submitted by:PANGANIBAN, DANICA D.
Submitted to:Ms. Carol Alcantara RN, MAN
I. INTRODUCTION
BACKGROUND OF THE STUDY:
Colon cancer is cancer of the large intestine (colon), the lower part of your digestive system. Rectal cancer is cancer of the last several inches of the colon. Together, they're often referred to as colorectal cancers. Most cases of colon cancer begin as small, noncancerous (benign) clumps of cells called adenomatous polyps. Over time some of these polyps become colon cancers. Polyps may be small and produce few, if any, symptoms. For this reason, doctors recommend regular screening tests to help prevent colon cancer by identifying polyps before they become colon cancer.
SIGNS AND SYMPTOMS:
A change in your bowel habits, including diarrhea or constipation or a change in the consistency of your stool
Rectal bleeding or blood in your stool
Persistent abdominal discomfort, such as cramps, gas or pain
A feeling that your bowel doesn't empty completely
Weakness or fatigue
Unexplained weight loss
CAUSES:
Precancerous growths in the colon Colon cancer most often begins as clumps of precancerous cells (polyps) on the inside lining of the colon. Polyps can appear mushroom-shaped, or they can be flat or recessed into the wall of the colon. Removing polyps before they become cancerous can prevent colon cancer.
Inherited gene mutations that increase the risk of colon cancer Inherited gene mutations that increase the risk of colon cancer can be passed through families, but these inherited genes are linked to only a small percentage of colon cancers. Inherited gene mutations don't make cancer inevitable, but they can increase an individual's risk of cancer significantly.
RISK FACTORS:
Older age A personal history of colorectal cancer or polyps Inflammatory intestinal conditions Family history of colon cancer and colon polyps Low-fiber, high-fat diet A sedentary lifestyle Diabetes Obesity Smoking Alcohol Radiation therapy for cancer
DIAGNOSTIC TEST:
Colonoscopy
CT Scan
STAGES OF COLON CANCER:
Stage I. Your cancer has grown through the superficial lining (mucosa) of the colon or rectum but hasn't spread beyond the colon wall or rectum.
Stage II. Your cancer has grown into or through the wall of the colon or rectum but hasn't spread to nearby lymph nodes.
Stage III. Your cancer has invaded nearby lymph nodes but isn't affecting other parts of your body yet.
Stage IV. Your cancer has spread to distant sites, such as other organs — for instance to your liver or lung.
TREATMENT:
Chemotherapy
Radiation Therapy
Drug Therapy
RATIONALE FOR CHOOSING THE CASE:
• I chose this study to promote awareness to the people who had this kind of disease by giving them information about the actions to be done and those contributing factors that made the treatment more seriously. I also want to determine management that can be done to help them to relieve some of the signs and symptoms of the disease as well as to teach them to prevent further complications.
SIGNIFICANCE OF THE STUDY:
• The importance of this study is to have information about the proper management and care for those clients who have this kind of illness. We can also educate people on how they can prevent and reduce the complication of the disease even if they already have the disease or not. It can also promote awareness and consciousness.
SCOPE AND LIMITATION OF THE STUDY:
• I will be focused on the nursing aspect of care, to give a basic knowledge about Colon Cancer.
II. CLINICAL SUMMARY:
A. PERSONAL DATA
Name: Patient C
Age: 72
Sex: Male
Address: 110 Pulo, Cabuyao, Laguna
Birth Date: May 28, 1941
Religion: Roman Catholic
Date of Admission: December 4, 2013, 11:30 am
Diagnosis: Caloric Mass T/C Colon Cancer
B. CHIEF COMPLAINT
Loss of Appetite
C. HISTORY OF PRESENT ILLNESS:
1 week prior to confinement patient have mass on the abdomen
D. PAST MEDICAL HISTORY:
(+) Acute Gastritis
(+) Hepa A
III. PHYSICAL EXAMINATION
AREA TECHNIQUE NORMS FINDINGS ANALYSIS AND INTERPRETATION
body built, height and weight in relation to client’s age
Inspection Proportionate, varies with lifestyle Small body built, height and weight was not taken
ABNORMALDue to his present
conditionPosture while sitting Inspection Relaxed, erect, posture, coordinated
movementThe patient can’t sit ABNORMAL
Due to his present condition
.body and breath odor Inspection (talking with the patient)
No body odor or minor odor relative to work, or exercise; no breath odor
No body odor and breath odor NORMAL
signs of distress in posture or facial expression
Inspection No distress noted The patient looks weak ABNORMALDue to his present
conditionsigns of health and illness Inspection Healthy appearance The client appears weak ABNORMAL
Due to his present condition
client’s attitude Inspection Cooperative, able to follow instructions
The patient was cooperative NORMAL
client’s affect/ mood; appropriateness of client’s responses
Inspection Appropriate to the situation The patient answers questions coherently without assistance
NORMAL
quantity of speech, quality and organization
Inspection Understandable, moderate pace, clear tone, exhibits thought association
Understandable, moderate and clear
NORMAL
relevance and organization of thoughts
Inspection Logical sequence, makes sense, has sense of reality
Makes sense and has sense of reality
NORMAL
I. SKINAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONskin color Inspection Varies from light to deep brown;
from yellow overtones to oliveUniform skin color NORMAL
. uniformity of skin color
Inspection Generally uniform except in areas exposed to the sun; areas lighter pigmentation (palms, lips, nailbeds) in dark skinned
Uniform in skin color NORMAL
assess edema Inspection No edema No edema NORMALskin lesions Inspection Freckles, some birthmarks, no
abrasions or other lesionsNo lesions NORMAL
skin moisture Inspection Moisture in skin folds and axillae
Skin is dry ABNORMALDue to dehydration.
II. HAIRAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONevenness of the growth, thickness or thinness of hair
Inspection Evenly distributed and covers the whole scalp
Evenly distributed and covers the whole scalp
NORMAL
texture and oiliness over the scalp
Inspection Silky, resilient hair Silky resilient hair NORMAL
presence of infection and infestation
Inspection No infection and infestation No Infection and Infestation NORMAL
amount of body hair Inspection Variable Variable. No abnormal hairiness
NORMAL
III. NAILSAREA TECHNIQUE NORMS FINDINGS ANALYIS AND
INTERPRETATIONfingernail plate shape Inspection Convex, curvature; angle of nail
plateConvex NORMAL
fingernail and toenail texture
Inspection Smooth texture Smooth texture NORMAL
fingernail and toenail bed color
Inspection Highly vascular and pink in light skinned clients; dark skinned clients may have brown or black
Pale in color ABNORMALDue to anemia
pigmentation in longitudinal streaks
tissues surrounding nails Inspection Intact epidermis Intact epidermis NORMALblanch test of capillary refill
Inspection, palpation
Promptly return of pink or usual color (generally less than 4 seconds)
Less than 4 seconds ABNORMAL Due to low
hemoglobin or anemia
IV. HEADAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONsize, shape and symmetry of the skull
Inspection Round (normocephalic with symmetrical frontal, parietal, and occipital prominences) smooth skull contour
The client’s head is round, normocephalic with symmetrical frontal, parietal, and occipital prominences
NORMAL
presence of nodules, masses and depressions
Inspection and palpation
Smooth uniform consistence; absence of nodules, or masses
Smooth, absence of nodules or masses
NORMAL
presence of edema and hollowness in the eye
Inspection and palpation
No edema and hollowness No edema or hollowness NORMAL
V. EYESAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONcolor, texture and presence of lesions in the palpebral conjunctiva
Inspection Pinkish in color with presence of small capillaries; moist, no foreign bodies
Pale in color ABNORMALDue to low hemoglobin
sclera: color and clarity Inspection White in color; clear, no yellowish discoloration, some capillaries may be visible
Yellowish in color ABNORMALDue to past medical history of HEPA A
iris: shape and color Inspection Anterior chamber is transparent; no noted visible materials, color depends on the person’s race
Anterior chamber is transparent; no noted visible materials, black in color
NORMAL
cornea: clarity and texture
Inspection No irregularities on the surface, looks smooth, clear or transparent
No irregularities on the surface; clear
NORMAL
pupils: color, shape and symmetry of size
Inspection Color depends on person’s race; size ranges from 3- 7 mm; and are equal in size; equally round
Black, equal in size; equally round; 4mm in size
NORMAL
light reaction and accommodation
Inspection Constrict briskly/ sluggish Constricts briskly NORMAL
visual acuity: near vision Inspection Can detect light and dark Can detect light and dark NORMALlacrimal gland: palpability and tenderness of lacrimal gland
Palpation No edema or tenderness over lacrimal gland
No edema or tenderness NORMAL
extraocular muscles eye alignment
Inspection Both eyes coordinated, moved in unison with parallel alignment
Both eyes are coordinated in movement; parallel alignment
NORMAL
visual fields: peripheral visual fields
Inspection When looking straight ahead the client can see objects in the periphery
Patient sees objects in periphery
NORMAL
VI. EARSAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONauricles: color, symmetry of size and position
Inspection Color same as facial skin; symmetric; auricle aligned with outer canthus of the eye; about 10 degrees from vertical
Aligned with outer canthus of the eye, same color as facial skin, both auricle are symmetrical
NORMAL
texture, elasticity and areas of tenderness
Inspection and palpation
Mobile, firm and not tender, pinna recoils after it is folded
Mobile firm and not tender; pinna recoils after folded
NORMAL
hearing acuity test: client response to normal voice tones
Inspection/ rinne test
Normal voice tones audible The client can hear whispered voices
NORMAL
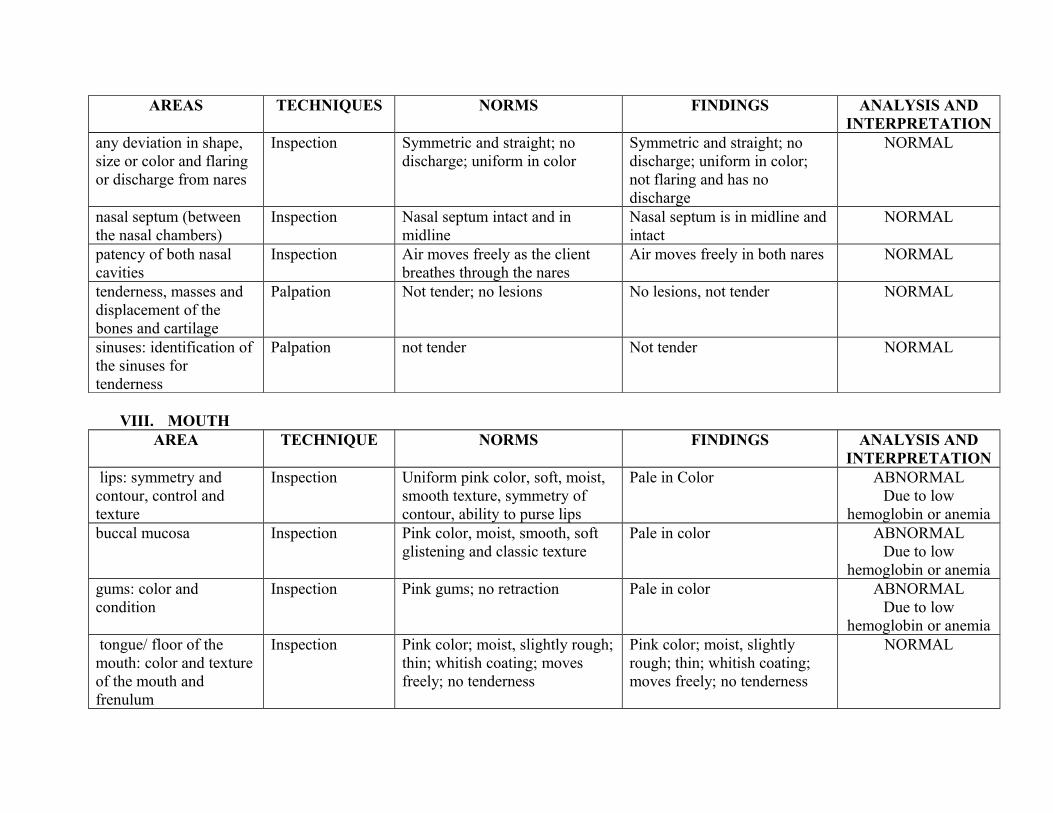
VII. NOSE
AREAS TECHNIQUES NORMS FINDINGS ANALYSIS AND INTERPRETATION
any deviation in shape, size or color and flaring or discharge from nares
Inspection Symmetric and straight; no discharge; uniform in color
Symmetric and straight; no discharge; uniform in color; not flaring and has no discharge
NORMAL
nasal septum (between the nasal chambers)
Inspection Nasal septum intact and in midline
Nasal septum is in midline and intact
NORMAL
patency of both nasal cavities
Inspection Air moves freely as the client breathes through the nares
Air moves freely in both nares NORMAL
tenderness, masses and displacement of the bones and cartilage
Palpation Not tender; no lesions No lesions, not tender NORMAL
sinuses: identification of the sinuses for tenderness
Palpation not tender Not tender NORMAL
VIII. MOUTHAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATION lips: symmetry and contour, control and texture
Inspection Uniform pink color, soft, moist, smooth texture, symmetry of contour, ability to purse lips
Pale in Color ABNORMALDue to low
hemoglobin or anemiabuccal mucosa Inspection Pink color, moist, smooth, soft
glistening and classic texturePale in color ABNORMAL
Due to low hemoglobin or anemia
gums: color and condition
Inspection Pink gums; no retraction Pale in color ABNORMALDue to low
hemoglobin or anemia tongue/ floor of the mouth: color and texture of the mouth and frenulum
Presence of abdominal mass ABNORMAL Due to his present condition (colon
cancer)enlargement of liver or spleen
palpation No evidence of enlargement of liver or spleen
No evidence of enlargement of spleen or liver
NORMAL
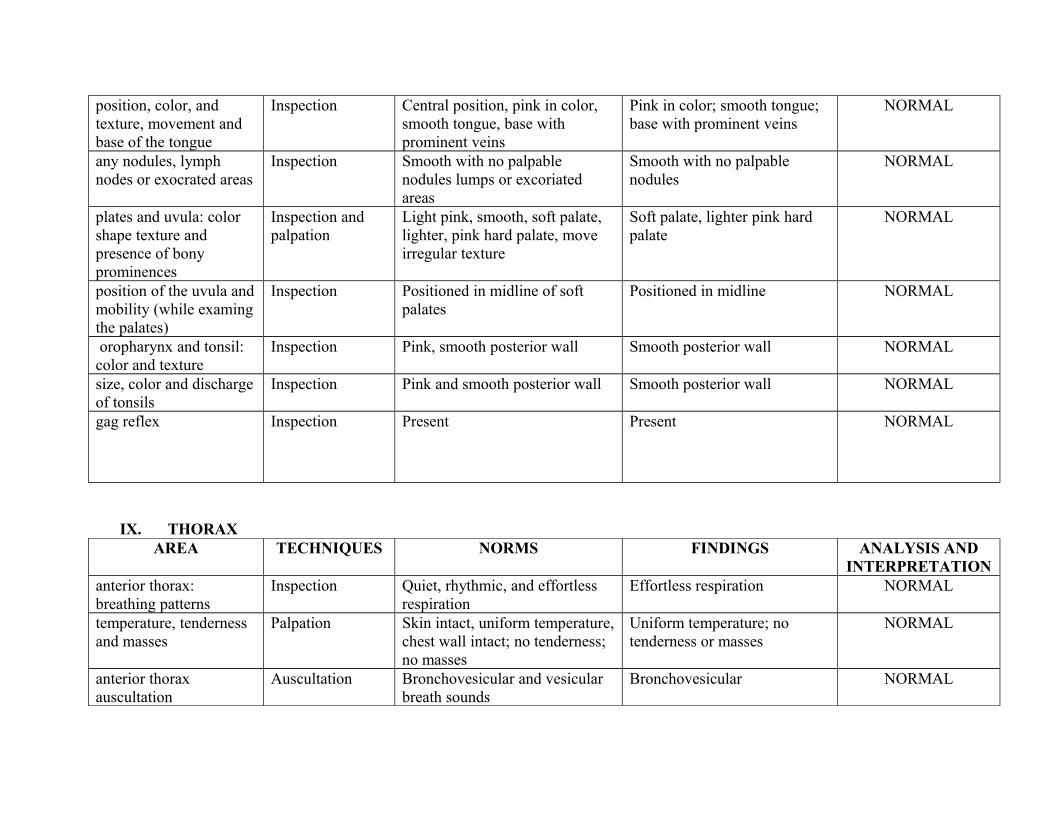
symmetry of contour Inspection Symmetric contour Symmetric contour NORMALabdominal movements associated with respiration, peristalsis or aortic pulsations
Auscultation Symmetric movements caused by respiration; visible peristalsis in very lean people; aortic pulsations in thin persons at epigastric area
Symmetric movement NORMAL
vascular pattern Inspection No visible vascular patter No visible vascular pattern NORMAL
XI. MUSCULOSKELETAL SYSTEMAREAS TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATION
muscle size and comparison on the other side
Inspection Proportionte to body; even in both sides
Proportionate to body, equal strength on both sides
NORMAL
fasciculation and tremors in muscle
Inspection No fasciculation and tremors No fasciculation and tremors NORMAL
muscle tonicity Inspection Even and firm in muscle tone Even and firm in muscle tone NORMALmuscle strength Inspection Has equal strength on both sides Has equal strengths NORMAL
XII. JOINTSAREA TECHNIQUE NORMS FINDINGS ANALYSIS AND
INTERPRETATIONjoint swelling Inspection and
palpationNo swelling; no warmth, no redness, no pain, no crepitus
No swelling, redness, pain or crepitus
NORMAL
Extremities Inspection and palpation
No swelling, no warmth, no redness, no pain
No swelling, warmth or redness
NORMAL
IV. GORDON’s 11 FUNCTIONAL HEALTH PATTERN OF ASSESSMENT
GORDON’S FUNCTIONAL HEALTH PATTERNS
PRIOR TO HOSPITALIZATION DURING HOSPITALIZATION
Health Perception and Health Management
The client thinks that health is a state of being well. The client thinks that it is important to consult to the doctor when he doesn’t feel well.
Nutritional- Metabolic He eats 3 times a day and drinks 8 glasses of water a day. He can’t eat everything he wants because of some restrictions on foods.
Elimination The client said he defecates 1-2 times daily and urinates 3-4 times a day
The client can defecate and urinate.
Activity and Exercise The client said he is not doing any exercise. He is unable to perform any exercise at all.
Cognitive- Perceptual The client said he is a positive thinker. The client is still positive thinker.
Sleep and Rest The client said the he always have 8 hours of sleep every day The client said that he can’t sleep well
Role Relationship The client is a responsible father. He is being dependent to everyone because of his condition.
Coping Stress The client said he is coping to stress by means of rest. During hospitalization the client copes to stress by means of sleeping.
Value Belief The client said she is a Roman Catholic. God serves as a guide to his family.
The client thinks the same.
V. ACTIVITIES OF DAILY LIVING
ASPECT PRIOR TO HOSPITALIZATION DURING HOSPITALIZATION ANALYSIS AND INTERPRETATION
1. NUTRITION LOW APPETITE LOW APPETITE Due to hospitalization the patient has low appetite because she doesn’t feel well.
2. ELIMINATION Urinates 3-4 times a day and defecates 1-2 times a day.
Urinates 2-3 times a day and defecates once a day
Due to hospitalization the patient can eliminate properly.
3. EXERCISE The patient cannot exercise The patient cannot exercise Due to hospitalization the patient cannot do his daily routine because of his condition.
4. HYGIENE Proper hygiene The patient cannot go to CR to take a bath.
Due to hospitalization the patient cannot go to CR to take a bath and need relative to assist him in doing his personal hygiene
5. SLEEP AND REST 8 hours of sleep and take a naps during the afternoon
He can’t sleep well because he feels uncomfortable.
Due to hospitalization the patient have altered sleeping pattern because he doesn’t feel comfortable.
VI. ANATOMY AND PHYSIOLOGY
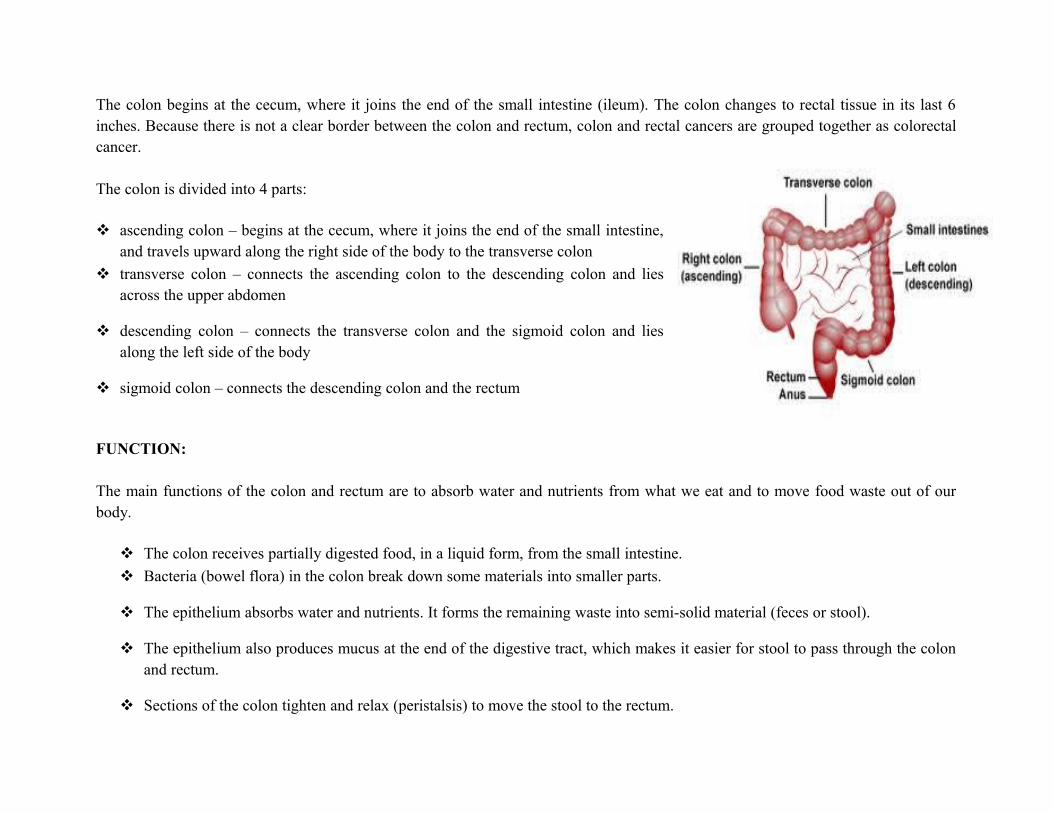
The large intestine is a hollow tube that makes up the last 6 feet of the digestive tract. It is often referred to as the large bowel or colon (which is technically just one part of the large intestine). The large intestine consists of the cecum (a pouch-like structure at beginning of the large intestine), colon, rectum and anus. The colon and rectum are next to other organs, including the spleen, liver, pancreas, and reproductive and urinary organs. Each of these organs can be affected if colorectal cancer spreads beyond the large intestine.
STRUCTURE:
The colon begins at the cecum, where it joins the end of the small intestine (ileum). The colon changes to rectal tissue in its last 6 inches. Because there is not a clear border between the colon and rectum, colon and rectal cancers are grouped together as colorectal cancer. The colon is divided into 4 parts:
ascending colon – begins at the cecum, where it joins the end of the small intestine, and travels upward along the right side of the body to the transverse colon
transverse colon – connects the ascending colon to the descending colon and lies across the upper abdomen
descending colon – connects the transverse colon and the sigmoid colon and lies along the left side of the body
sigmoid colon – connects the descending colon and the rectum
FUNCTION:
The main functions of the colon and rectum are to absorb water and nutrients from what we eat and to move food waste out of our body.
The colon receives partially digested food, in a liquid form, from the small intestine.
Bacteria (bowel flora) in the colon break down some materials into smaller parts.
The epithelium absorbs water and nutrients. It forms the remaining waste into semi-solid material (feces or stool).
The epithelium also produces mucus at the end of the digestive tract, which makes it easier for stool to pass through the colon and rectum.
Sections of the colon tighten and relax (peristalsis) to move the stool to the rectum.
The rectum is a holding area for the stool. When it is full, it signals the brain to move the bowels and push the stool from the body through the anus.
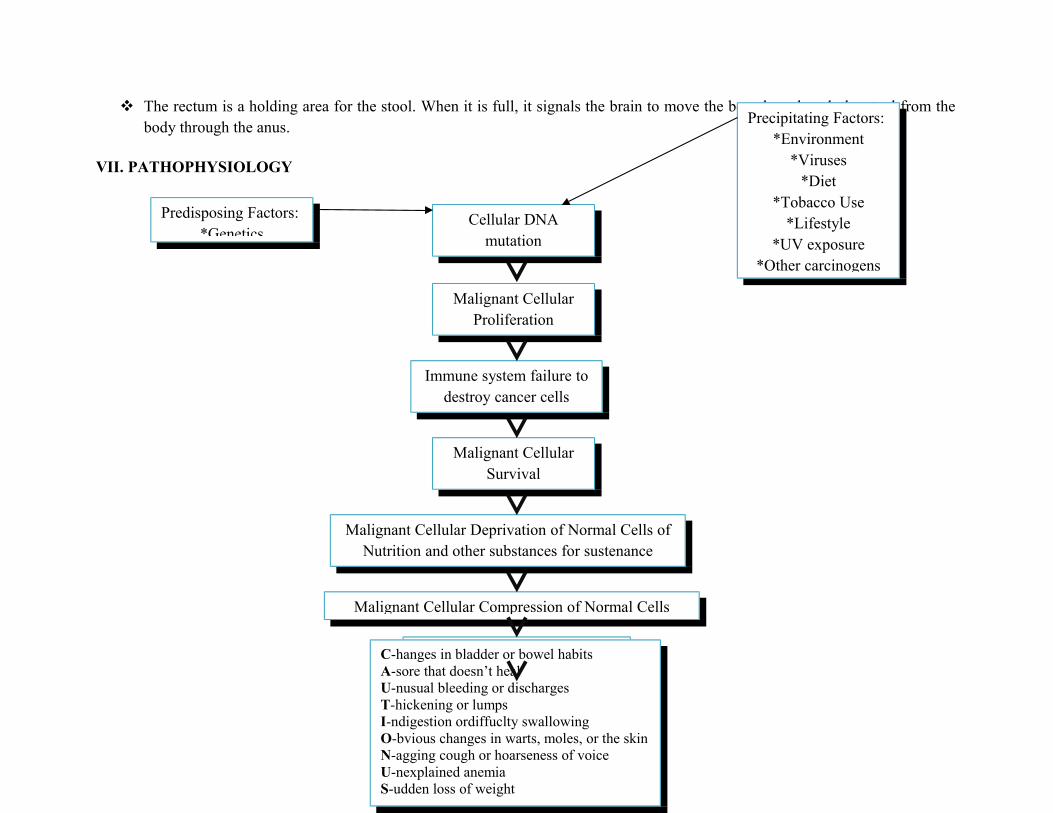
VII. PATHOPHYSIOLOGY
Predisposing Factors:*Genetics
Precipitating Factors:*Environment
*Viruses*Diet
*Tobacco Use*Lifestyle
*UV exposure*Other carcinogens
Malignant Cellular Proliferation
Immune system failure to destroy cancer cells
Malignant Cellular Survival
Cellular DNA mutation
Malignant Cellular Deprivation of Normal Cells of Nutrition and other substances for sustenance
Malignant Cellular Compression of Normal Cells
Normal Cell DeathC-hanges in bladder or bowel habitsA-sore that doesn’t healU-nusual bleeding or dischargesT-hickening or lumpsI-ndigestion ordiffuclty swallowingO-bvious changes in warts, moles, or the skinN-agging cough or hoarseness of voiceU-nexplained anemiaS-udden loss of weight
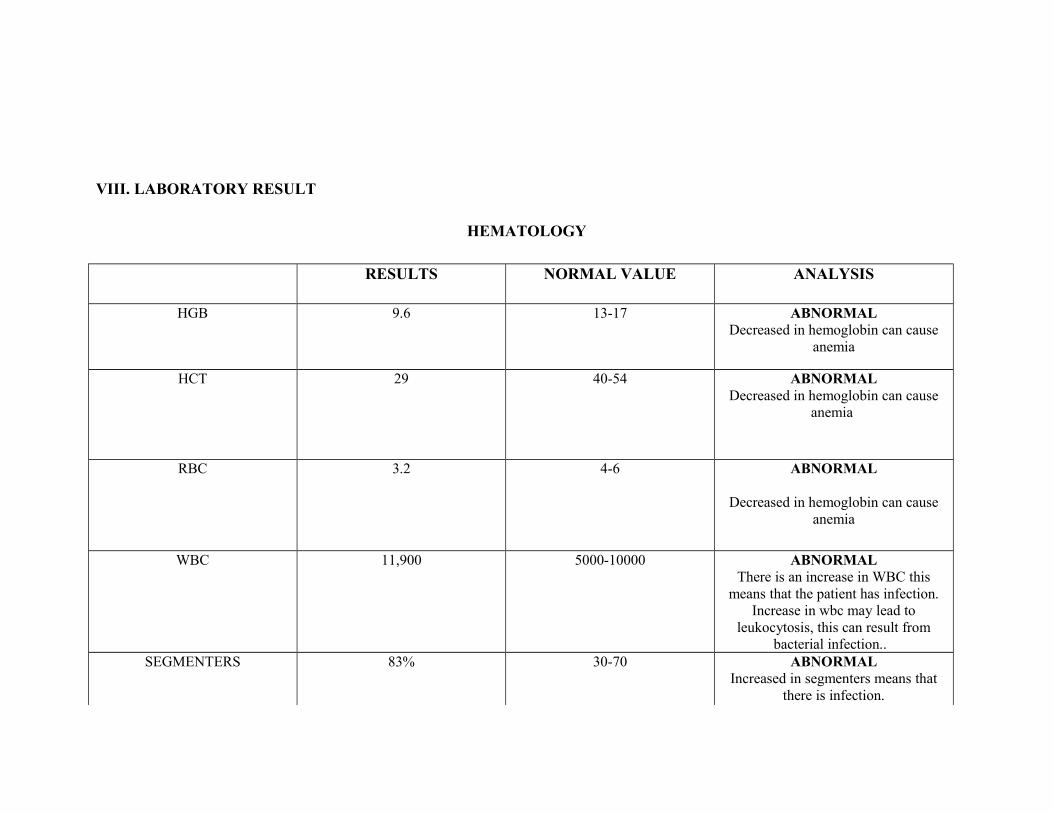
VIII. LABORATORY RESULT
HEMATOLOGY
RESULTS NORMAL VALUE ANALYSIS
HGB 9.6 13-17 ABNORMALDecreased in hemoglobin can cause
anemia
HCT 29 40-54 ABNORMALDecreased in hemoglobin can cause
anemia
RBC 3.2 4-6 ABNORMAL
Decreased in hemoglobin can cause anemia
WBC 11,900 5000-10000 ABNORMALThere is an increase in WBC this
means that the patient has infection. Increase in wbc may lead to
leukocytosis, this can result from bacterial infection..
SEGMENTERS 83% 30-70 ABNORMALIncreased in segmenters means that
there is infection.
LYMPHOCYTES 14% 20-40 ABNORMALIncreased in lymphocytes means that
there is infection.
IX. DRUG STUDY
NAME OF DRUG
CLASSIFICATION MECHANISM OF ACTION
SIDE EFFECTS CONTRAINDICATION NURSING RESPONSIBILITY
Appetite Plus 1 cap BID
Appetite Enhancers Stimulates appetite & enhances weight gain
Headache Nausea Constipation Upset stomach
Hypersensitivity Should be taken with food.
Monitor vital signs
Monitor Intake and Output
Heraclene Forte 1 tab OD
Appetite Enhancers Used for taking care of weight loss, It also may be used for treating tuberculosis and additional persistent diseases, recuperating from severe surgery or infection and defective nutrition in elderly patients.
Nausea and vomiting
Diarrhea Acidity Headache GI disorders
Hypersensitivity Pregnancy Lactation
Monitor vital signs
Monitor I & O
X. FDAR
FOCUS DATA ACTION
IMBALANCED NUTRITION
Received patient awake, lying on bed with ongoing D5NM 1L @ 800 cc Level.
Body Malaise
Weight Loss
Poor muscle tone
VS taken as follows:
• BP- 100/60
• T- 36.3
• P-76
• R- 26
IV fluids maintained and
regulated
Encouraged to consume high-
caloric diet with adequate fluid
intake
Provided health teaching
regarding healthy nutritious food
Monitored intake and output
Administered prescribe
medication
RESPONSE:
Still for Continuity of care
XII. DISCHARGE PLANNING
Medications • Write the exact time and instruction when to take the medication and how to take the
medication.• Emphasize proper dosage of medication to be taken for the proper continuity of care.
Exercise • Instruct client to have light exercises.
Treatment • Continue medication as ordered by the physician
Health Teachings • Instruct the client’s relative to provide adequate rest
Out -patient • Follow up check up
Diet • Advise client’s relative to provide increased intake of fluid
• Advise client’s relative to provide high- calorie and food that rich in protein
Spiritual/sexual activity • Encourage patient to Pray always


























![Home | Cancer Research - Case-Control Study of ......[CANCER RESEARCH 46, 5360-5363, October 1986] Case-Control Study of Decaffeinated Coffee Consumption and Pancreatic Cancer1 Ernst](https://static.documents.pub/doc/80x56/5f25bcd492746226463c96a4/home-cancer-research-case-control-study-of-cancer-research-46-5360-5363.jpg)






