2018 OPEN ENROLLMENT PRINTABLE INDEX OF FORMS AND NOTICES Health Insurance Enrollment Form (80/20 Plan, High Deductible Plan, Dental & Vision) Health Savings Account (HSA) Application (ONLY for use if enrolling in the High Deductible Health Plan) HSA Terms, Conditions & Signature Page HSA Frequently Asked Questions (FAQs) HSA Worksheet Health Insurance Waiver Affidavit of Declaration of Financial Interdependence Extension of Dependent Coverage Form Medicare Secondary Payer – Employee Status Form Health Reimbursement Arrangement (HRA) Forms HRA Enrollment Form HRA Attestation Form HRA Flow Chart HRA Claim Form Notices Summary of Benefits and Coverage (Anthem: AFSCME, CODE, NON, BT, Police hires after 9/8/16, Fire hired after 4/27/16) Summary of Benefits and Coverage (Anthem: Police hired before 9/8/16 and Fire hired before 4/27/16) Summary of Benefits and Coverage (High Deductible Plan with HSA) Summary of Benefits and Coverage (Integrated HRA) Women’ s Health and Cancer Rights & Special Enrollment Michelle’ s Law & Grandfather Status Notice Children’s Health Insurance Program (CHIP) Notice COBRA Notice Letter Notice of City of Cincinnati’s Health Plan Privacy Practices (HIPAA) Medicare Part D Notice of Creditable Coverage *NEW* EEOC Notice Regarding Wellness Programs *NEW* Notice Regarding Wellness Program – Spouse/Dependent Authorization Glossary of Medical Terms
Transcript
2018 OPEN ENROLLMENT
PRINTABLE INDEX OF FORMS AND NOTICES Health Insurance Enrollment Form (80/20 Plan, High Deductible Plan, Dental &
Vision)
Health Savings Account (HSA) Application (ONLY for use if enrolling in the High
Deductible Health Plan)
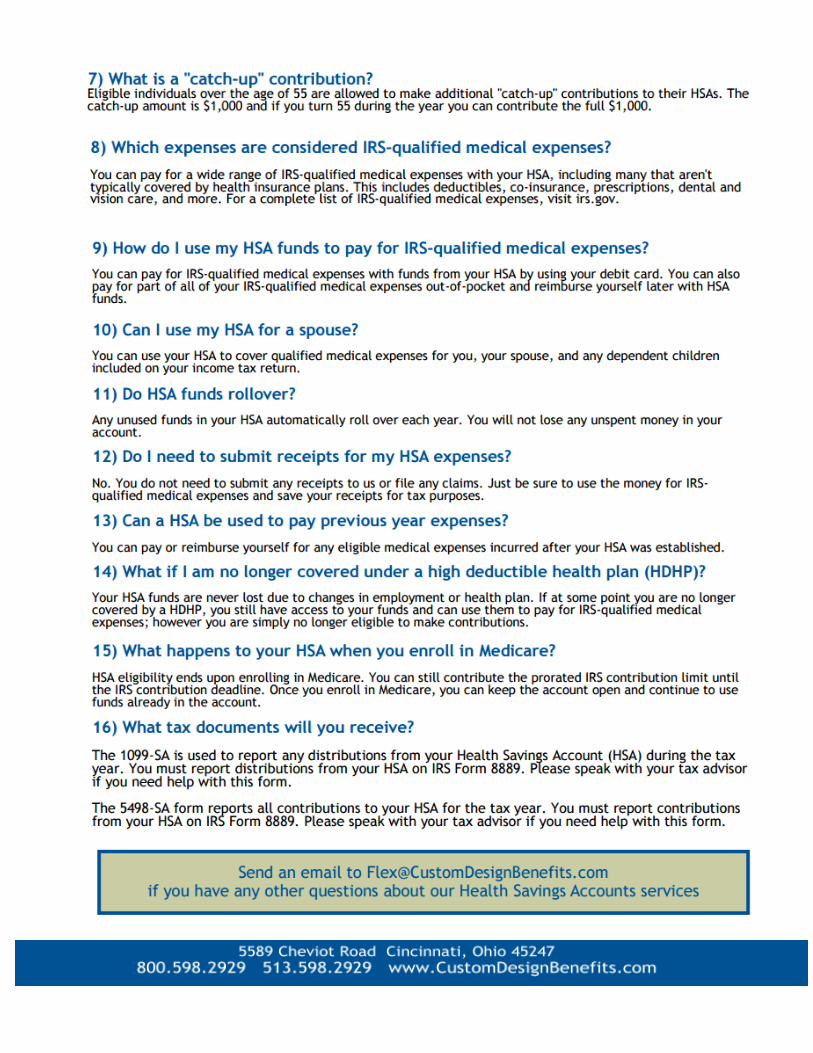
HSA Terms, Conditions & Signature Page
HSA Frequently Asked Questions (FAQs)
HSA Worksheet
Health Insurance Waiver
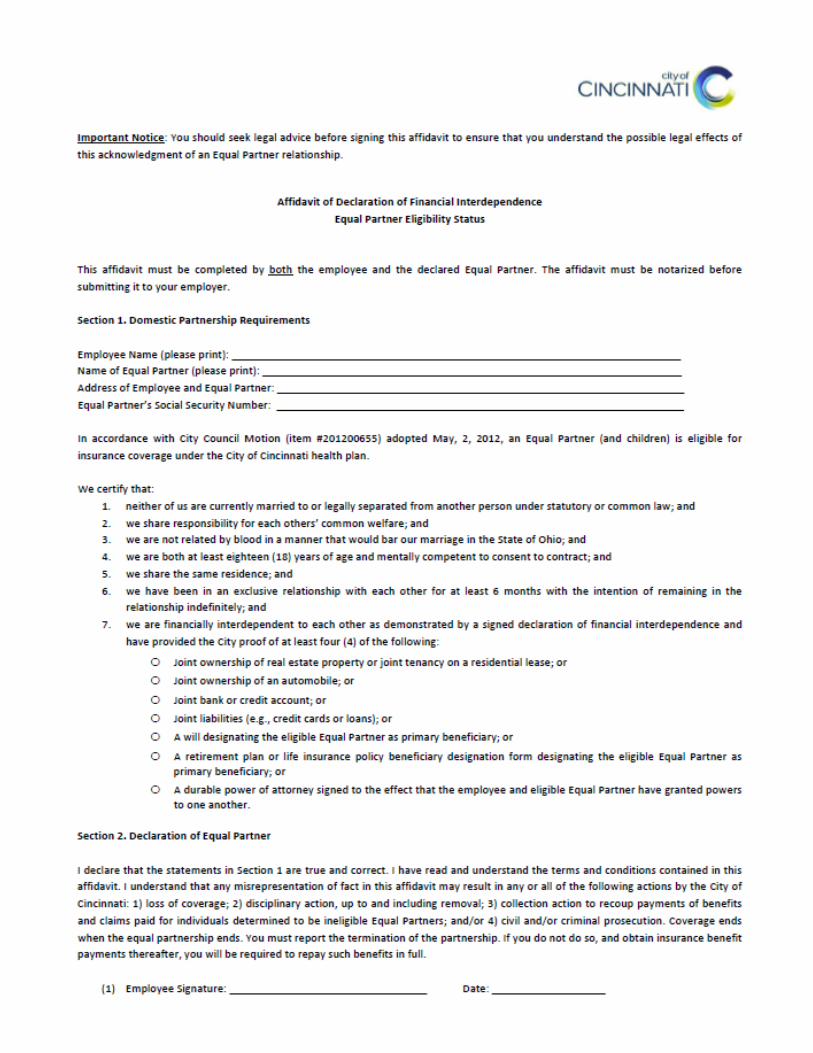
Affidavit of Declaration of Financial Interdependence
Extension of Dependent Coverage Form
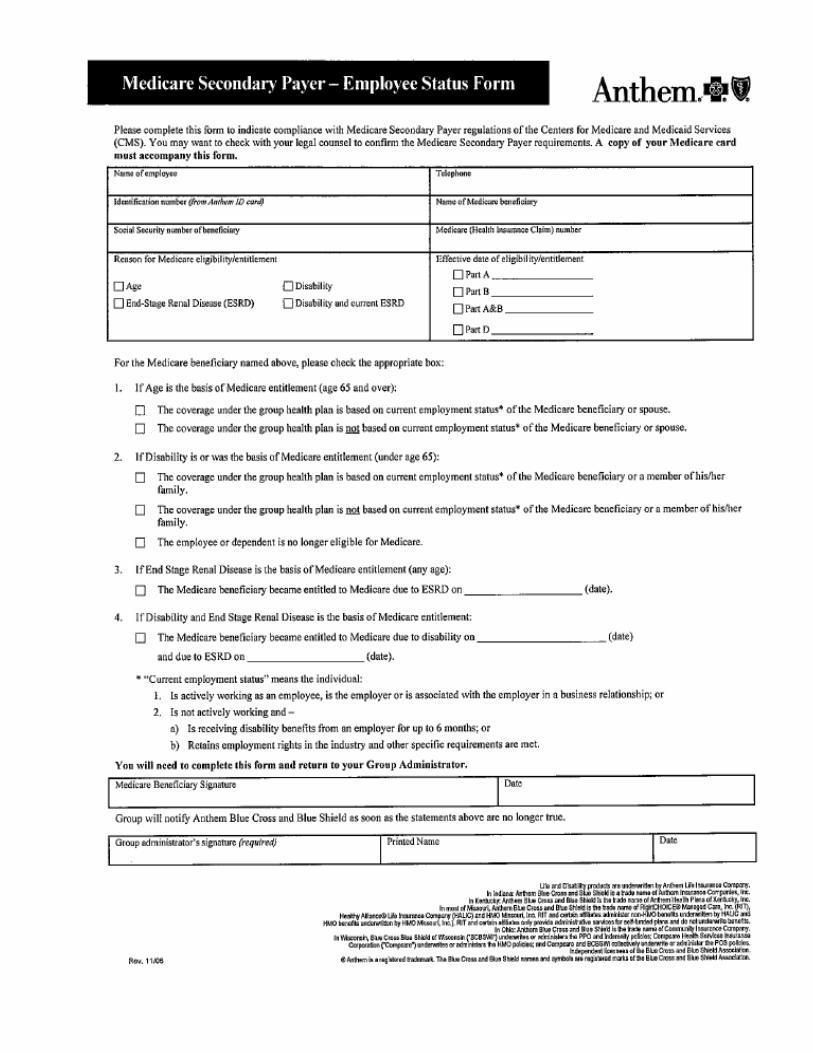
Medicare Secondary Payer – Employee Status Form
Health Reimbursement Arrangement (HRA) Forms HRA Enrollment Form
HRA Attestation Form
HRA Flow Chart
HRA Claim Form
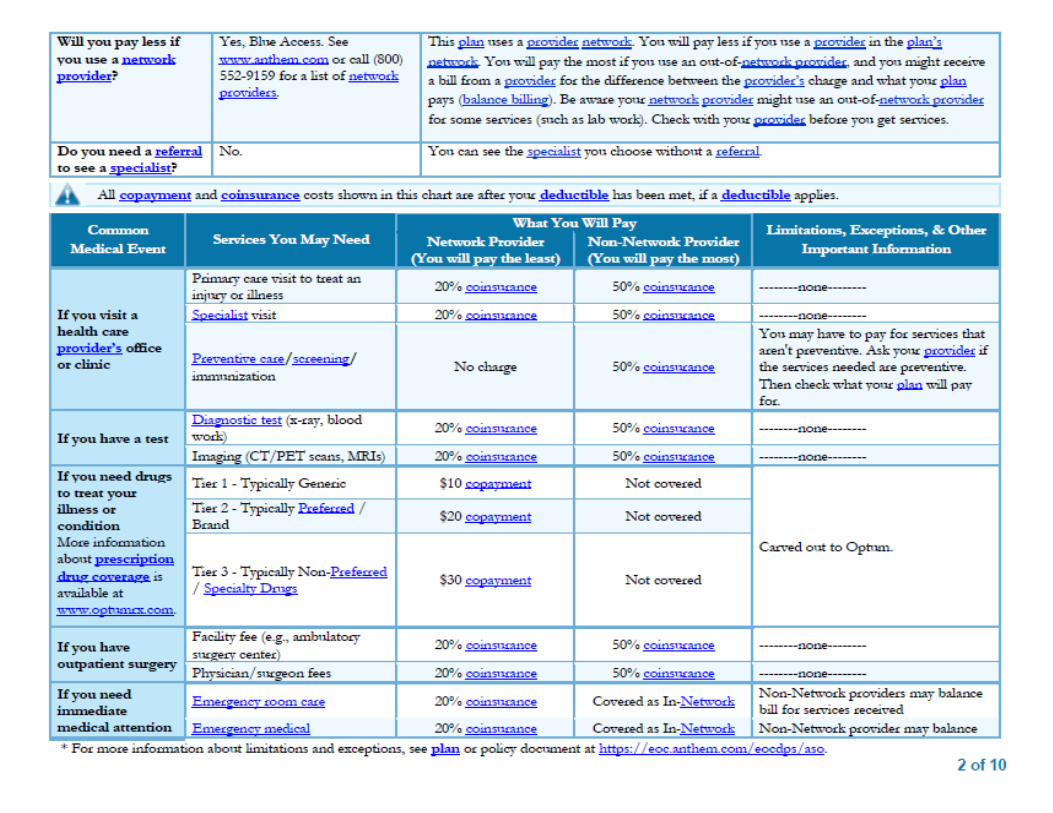
Notices Summary of Benefits and Coverage (Anthem: AFSCME, CODE, NON, BT, Police
hires after 9/8/16, Fire hired after 4/27/16)
Summary of Benefits and Coverage (Anthem: Police hired before 9/8/16 and Fire
hired before 4/27/16)
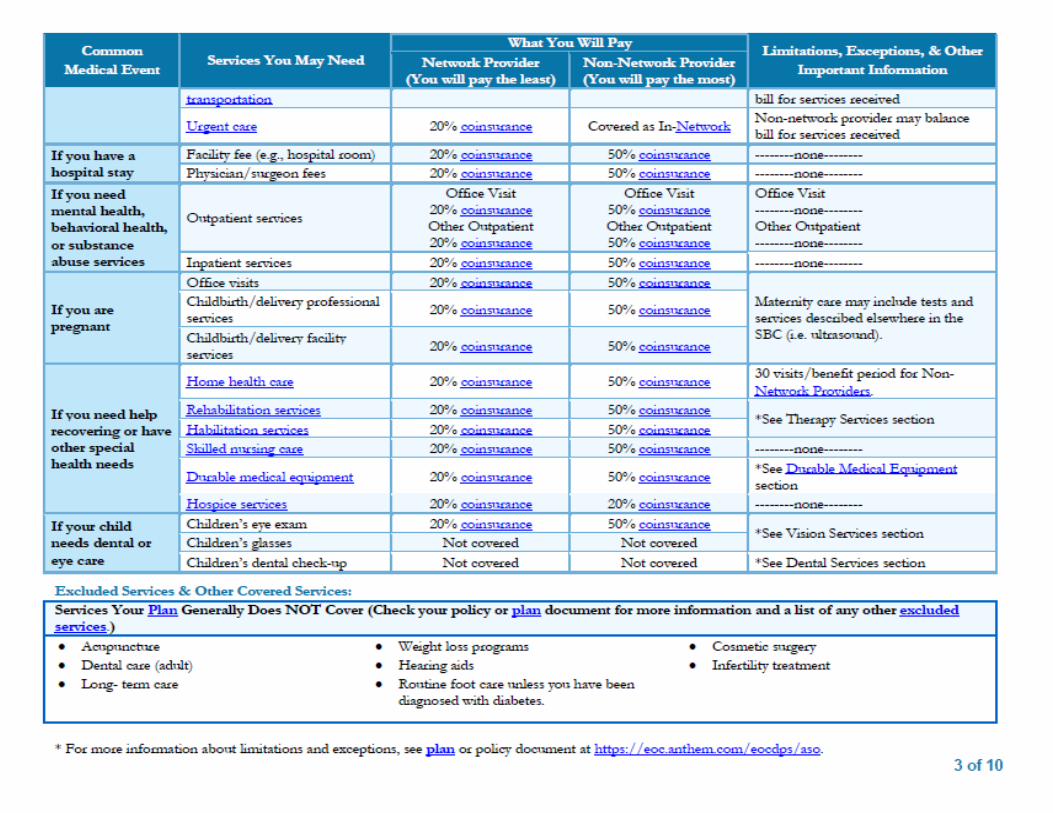
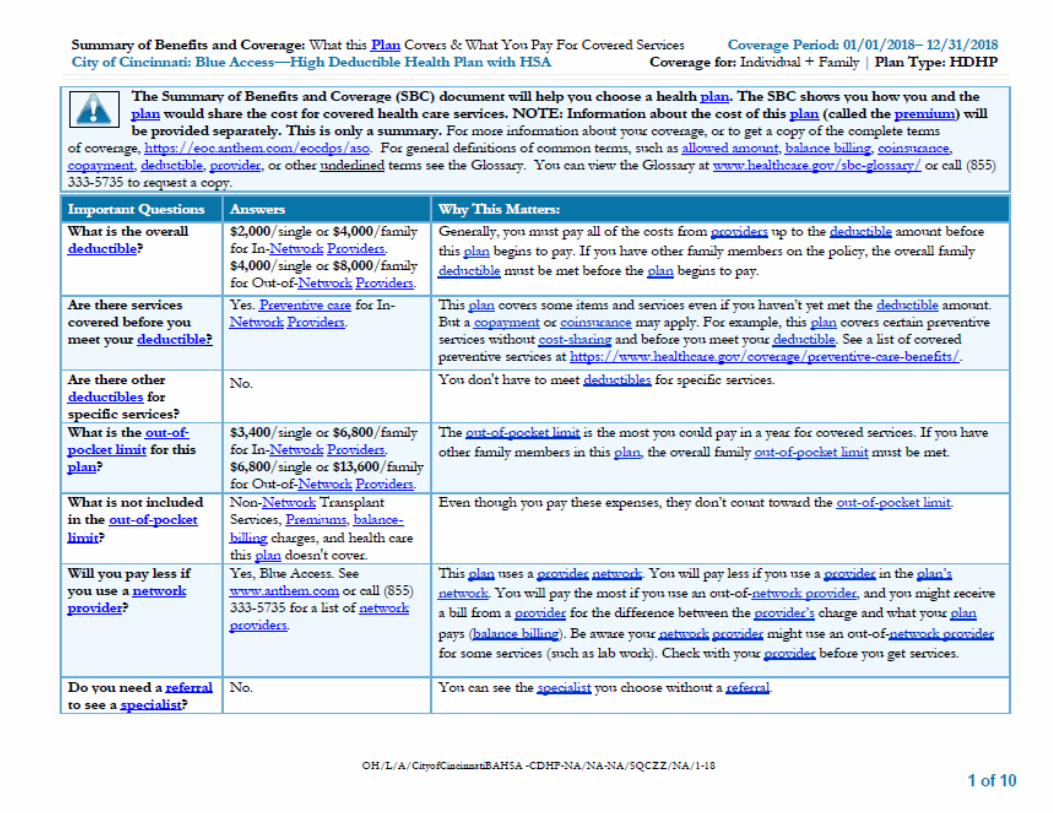
Summary of Benefits and Coverage (High Deductible Plan with HSA)
Summary of Benefits and Coverage (Integrated HRA)
Women’s Health and Cancer Rights & Special Enrollment
Michelle’s Law & Grandfather Status Notice
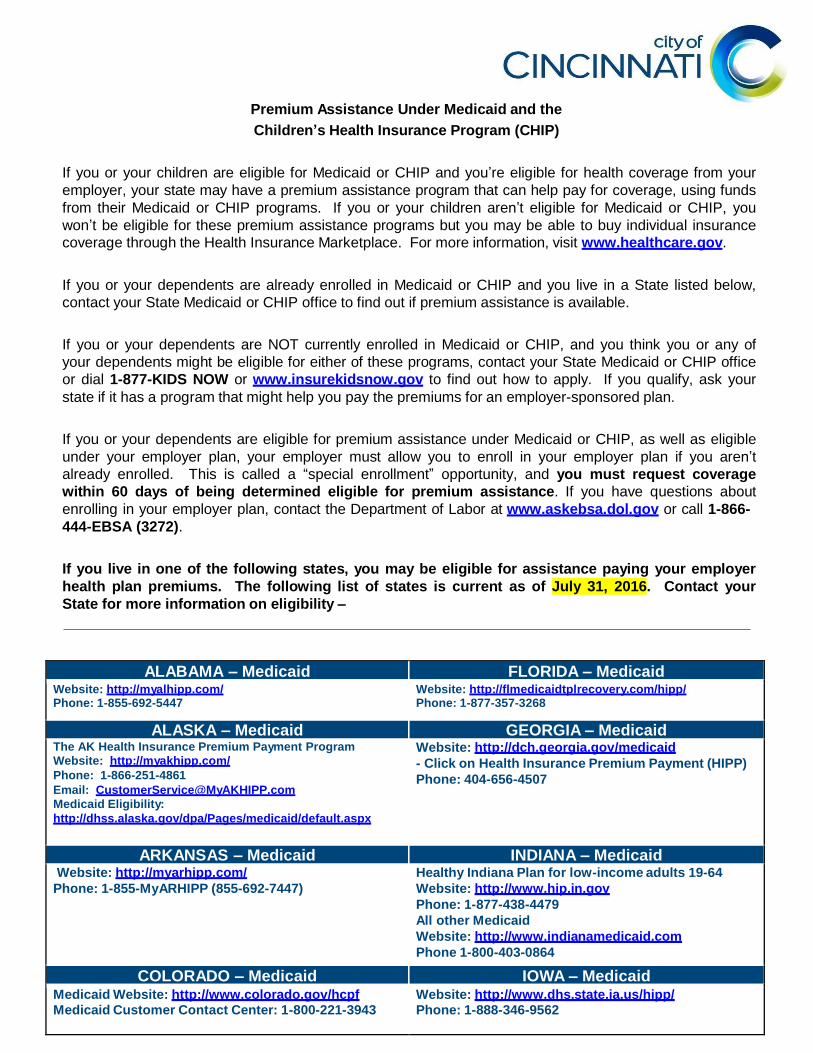
Children’s Health Insurance Program (CHIP) Notice
COBRA Notice Letter
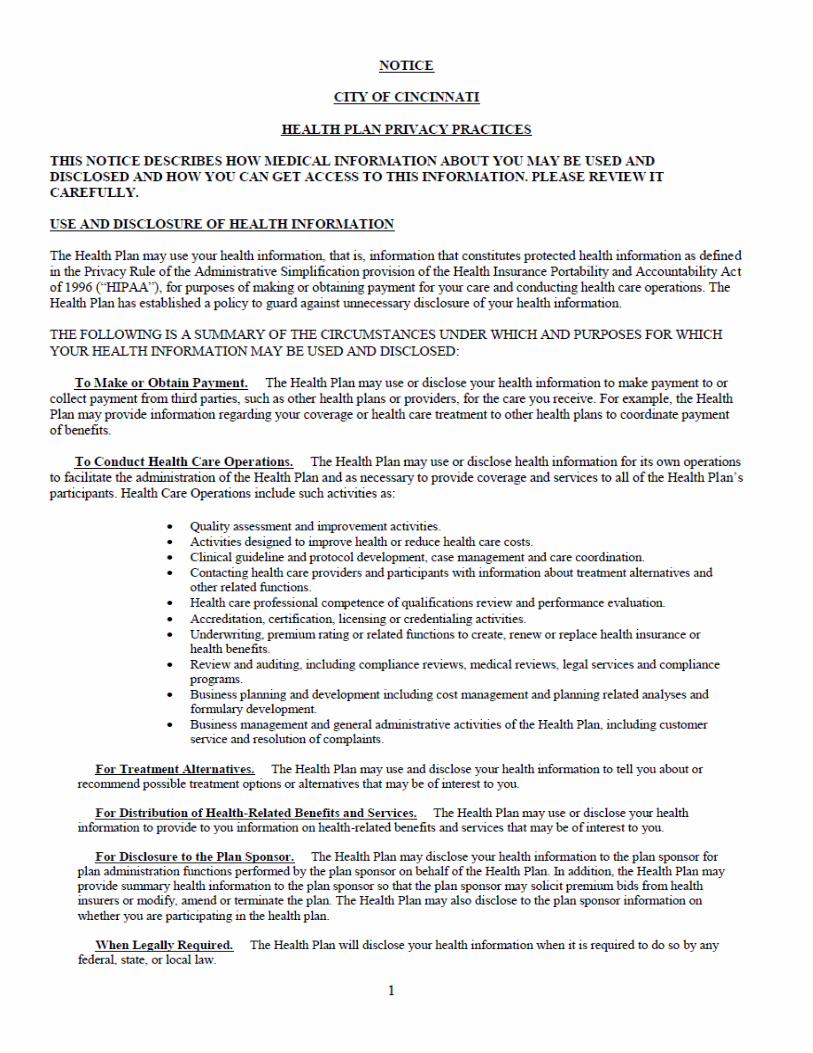
Notice of City of Cincinnati’s Health Plan Privacy Practices (HIPAA)
Medicare Part D Notice of Creditable Coverage
*NEW* EEOC Notice Regarding Wellness Programs
*NEW* Notice Regarding Wellness Program – Spouse/Dependent Authorization
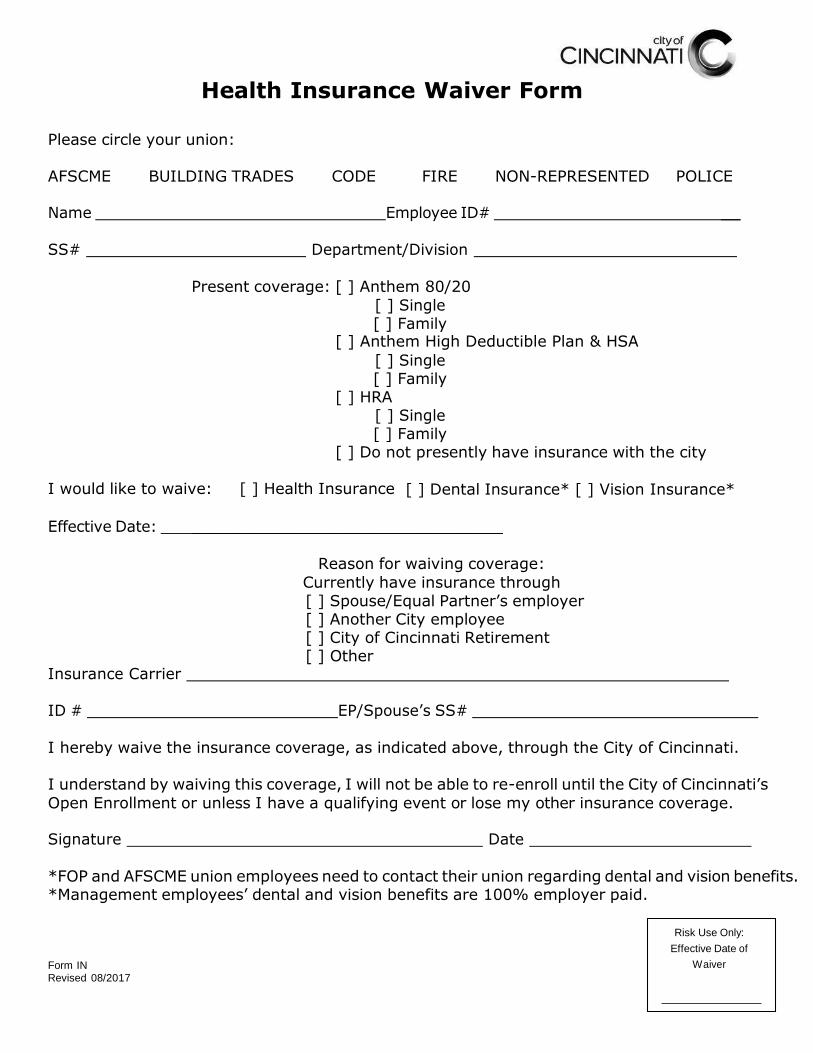
Please circle your union: AFSCME BUILDING TRADES CODE FIRE NON-REPRESENTED POLICE Name Employee ID# __ SS# Department/Division
Present coverage: [ ] Anthem 80/20
[ ] Single
[ ] Family [ ] Anthem High Deductible Plan & HSA
[ ] Single
[ ] Family [ ] HRA
[ ] Single
[ ] Family [ ] Do not presently have insurance with the city
I would like to waive: [ ] Health Insurance [ ] Dental Insurance* [ ] Vision Insurance*
Effective Date: ________________________________
Reason for waiving coverage:
Currently have insurance through
[ ] Spouse/Equal Partner’s employer
[ ] Another City employee
[ ] City of Cincinnati Retirement
[ ] Other Insurance Carrier ID # EP/Spouse’s SS# I hereby waive the insurance coverage, as indicated above, through the City of Cincinnati. I understand by waiving this coverage, I will not be able to re-enroll until the City of Cincinnati’s
Open Enrollment or unless I have a qualifying event or lose my other insurance coverage. Signature Date *FOP and AFSCME union employees need to contact their union regarding dental and vision benefits. *Management employees’ dental and vision benefits are 100% employer paid. Form IN
Revised 08/2017
J&K Third Party Administrator
Integrated HRA Enrollment Form – City of Cincinnati Employees EMPLOYER INFORMATION
Employer Name: City of Cincinnati
Please send completed enrollment forms and information to:
City of Cincinnati Risk Management - 805 Central Avenue, Suite 100 - Cincinnati, OH 45202
I am enrolling in the Integrated HRA for: Single Family
PARTICIPANT INFORMATION
Employee Name:
Birthdate:
Hire Date:
Social Security No: Employee ID No.: Gender: M F
Date Eligible for HRA:
Home Street Address:
City: State: Zip Code:
Home Phone: Work Phone: Cell Phone:
Email Address: Fire, Police or Union Affiliation:
SPOUSE INFORMATION
Spouse Name:
Birthdate: Gender: M F
Social Security No: Spouse’s Employer:
Spouse’s Pay Period for Health Premium Contribution: Monthly Semi-Monthly Bi-Weekly Weekly
Spouse’s Health Premium Contribution Pay Period: ** INCLUDE DOCUMENTATION, I.E. PAYSTUB OR BENEFIT STATEMENT
Are Spouse’s Health Premium Contribution / Deductions: Before Taxes (OR) After Taxes
* Contribution per pay period should include the cost for Medical only; Dental & Vision are not covered under this plan.
If submitting a spousal paystub, please circle the contribution/deduction amount on the submitted paystub. DO NOT BLACKOUT THE PAY PERIOD.
** Send a copy of your spouse’s paystub that shows the NEW contribution/deduction amount for the effective date listed above. This amount should reflect the cost of adding you and/or any dependents to the spouse’s plan. Please indicate if the medical deduction DOES NOT come out of every paycheck. Some
may be only once a month or the first two pays of each month.
* If your spouse’s plan has a High Deductible with an HSA, Health Savings Account, you are not eligible to participate in the Integrated HRA, unless the
spouse’s employer allows your spouse to drop the HSA portion of the plan. If your primary health insurance coverage is through Medicare, Tricare, or
any City of Cincinnati sponsored health plan you are not eligible for the Integrated HRA.
***You must provide proof of dependent eligibility i.e. marriage certificate, birth certificate, etc.***
DEPENDENT INFORMATION: (Attach a separate sheet if additional space is needed for additional dependents)
Name: Date of Birth: Gender: Male Female
Social Security No: Name: Date of Birth: Gender: Male Female
Social Security No: Name: Date of Birth: Gender: Male Female
Social Security No:
PARTICIPANT AUTHORIZATION
I hereby authorize the City of Cincinnati to enroll me into the employer sponsored Integrated HRA. I agree to comply with the terms and conditions of the
plan. I understand that if the health premium contributions are deducted on an After-Tax Basis, this will result in all premium reimbursements being income
tax free. However, if the contributions are on a Pre-Tax Basis, the premium reimbursements will be fully taxable. In either case, the deductible, co-pay and
co-insurance reimbursements will remain tax free. I further understand that if any current contributions are made to an HDHP/HSA, I am not eligible to
participate in the Integrated HRA offered through the City of Cincinnati.
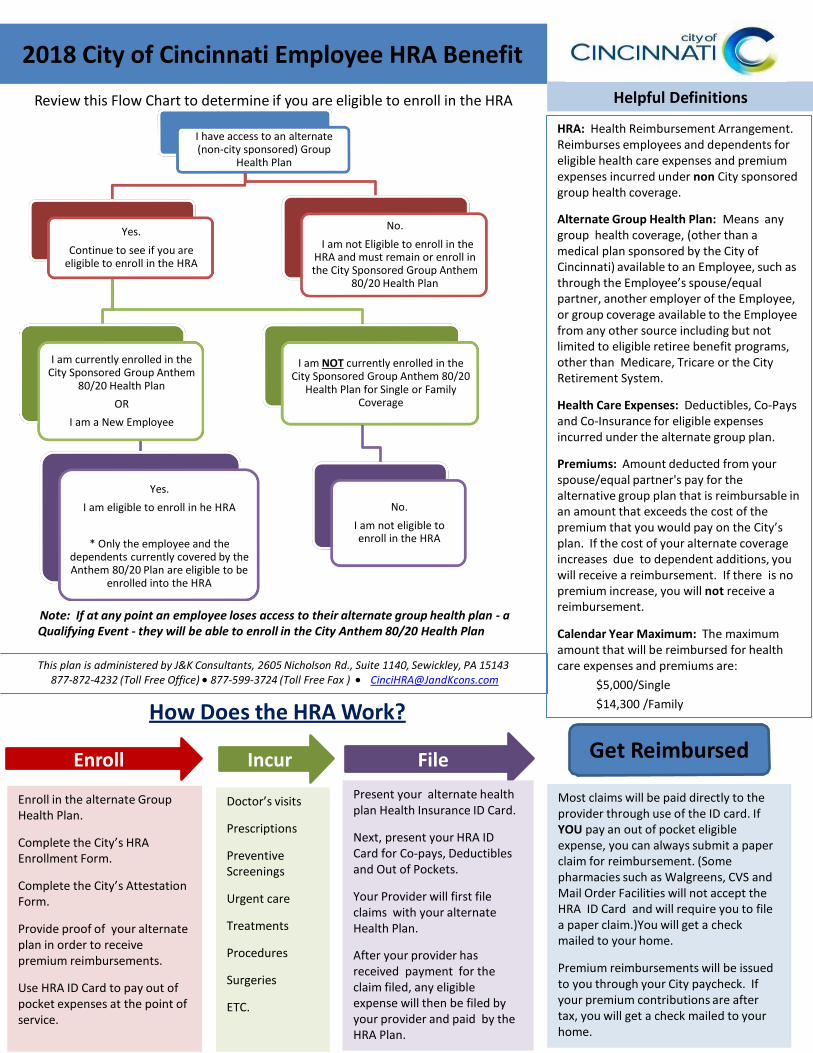
Review this Flow Chart to determine if you are eligible to enroll in the HRA
I have access to an alternate (non-city sponsored) Group
Health Plan
Helpful Definitions
HRA: Health Reimbursement Arrangement. Reimburses employees and dependents for eligible health care expenses and premium expenses incurred under non City sponsored group health coverage.
Yes.
Continue to see if you are eligible to enroll in the HRA
I am currently enrolled in the City Sponsored Group Anthem
80/20 Health Plan
OR
I am a New Employee
Yes.
I am eligible to enroll in he HRA
* Only the employee and the
dependents currently covered by the Anthem 80/20 Plan are eligible to be
enrolled into the HRA
No.
I am not Eligible to enroll in the HRA and must remain or enroll in the City Sponsored Group Anthem
80/20 Health Plan
I am NOT currently enrolled in the City Sponsored Group Anthem 80/20
Health Plan for Single or Family Coverage
No.
I am not eligible to enroll in the HRA
Alternate Group Health Plan: Means any group health coverage, (other than a medical plan sponsored by the City of Cincinnati) available to an Employee, such as through the Employee’s spouse/equal partner, another employer of the Employee, or group coverage available to the Employee from any other source including but not limited to eligible retiree benefit programs, other than Medicare, Tricare or the City Retirement System.
Health Care Expenses: Deductibles, Co-Pays and Co-Insurance for eligible expenses incurred under the alternate group plan.
Premiums: Amount deducted from your spouse/equal partner's pay for the alternative group plan that is reimbursable in an amount that exceeds the cost of the premium that you would pay on the City’s plan. If the cost of your alternate coverage increases due to dependent additions, you will receive a reimbursement. If there is no premium increase, you will not receive a
Note: If at any point an employee loses access to their alternate group health plan - a Qualifying Event - they will be able to enroll in the City Anthem 80/20 Health Plan
This plan is administered by J&K Consultants, 2605 Nicholson Rd., Suite 1140, Sewickley, PA 15143
Calendar Year Maximum: The maximum amount that will be reimbursed for health care expenses and premiums are:
$5,000/Single
$14,300 /Family
Enroll Incur File Get Reimbursed
Enroll in the alternate Group Health Plan.
Complete the City’s HRA Enrollment Form.
Complete the City’s Attestation Form.
Provide proof of your alternate plan in order to receive premium reimbursements.
Use HRA ID Card to pay out of pocket expenses at the point of service.
Doctor’s visits
Prescriptions
Preventive Screenings
Urgent care
Treatments
Procedures
Surgeries
ETC.
Present your alternate health plan Health Insurance ID Card.
Next, present your HRA ID Card for Co-pays, Deductibles and Out of Pockets.
Your Provider will first file claims with your alternate Health Plan.
After your provider has received payment for the claim filed, any eligible expense will then be filed by your provider and paid by the HRA Plan.
Most claims will be paid directly to the provider through use of the ID card. If YOU pay an out of pocket eligible expense, you can always submit a paper claim for reimbursement. (Some pharmacies such as Walgreens, CVS and Mail Order Facilities will not accept the HRA ID Card and will require you to file a paper claim.)You will get a check mailed to your home.
Premium reimbursements will be issued to you through your City paycheck. If your premium contributions are after tax, you will get a check mailed to your home.
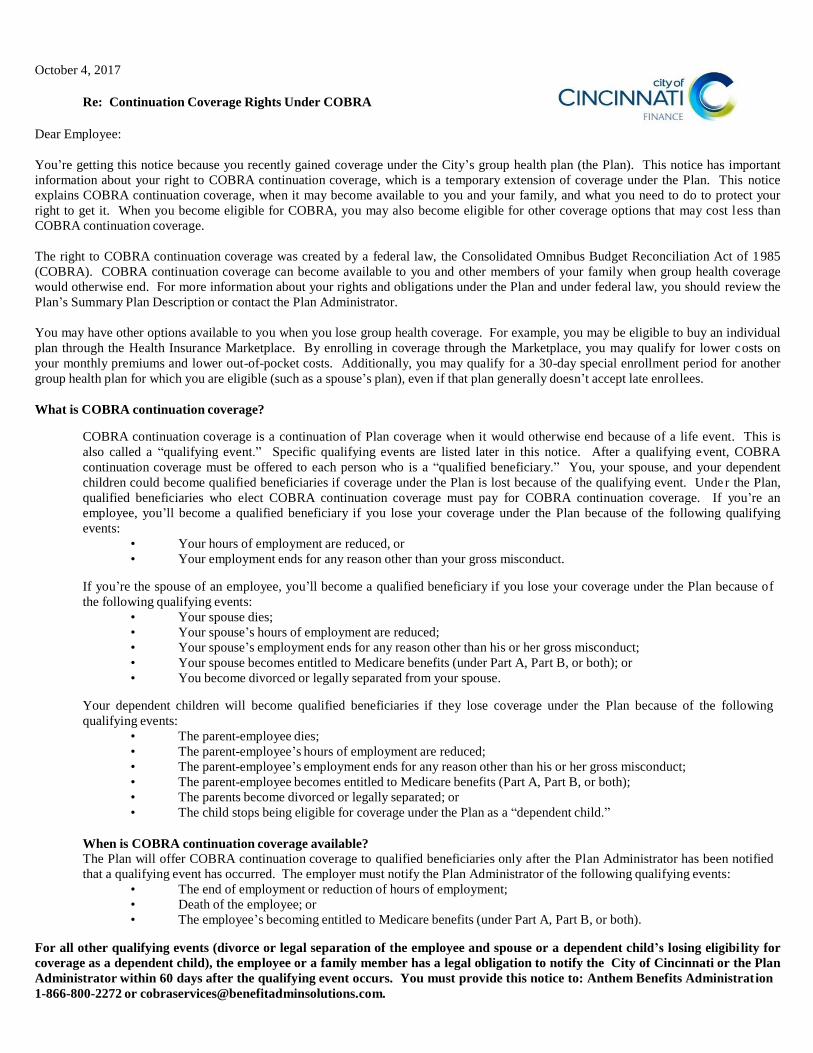
You’re getting this notice because you recently gained coverage under the City’s group health plan (the Plan). This notice has important
information about your right to COBRA continuation coverage, which is a temporary extension of coverage under the Plan. This notice
explains COBRA continuation coverage, when it may become available to you and your family, and what you need to do to protect your
right to get it. When you become eligible for COBRA, you may also become eligible for other coverage options that may cost l ess than
COBRA continuation coverage.
The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1 985
(COBRA). COBRA continuation coverage can become available to you and other members of your family when group health coverage
would otherwise end. For more information about your rights and obligations under the Plan and under federal law, you should review the
Plan’s Summary Plan Description or contact the Plan Administrator.
You may have other options available to you when you lose group health coverage. For example, you may be eligible to buy an individual
plan through the Health Insurance Marketplace. By enrolling in coverage through the Marketplace, you may qualify for lower c osts on
your monthly premiums and lower out-of-pocket costs. Additionally, you may qualify for a 30-day special enrollment period for another
group health plan for which you are eligible (such as a spouse’s plan), even if that plan generally doesn’t accept late enrollees.
What is COBRA continuation coverage?
COBRA continuation coverage is a continuation of Plan coverage when it would otherwise end because of a life event. This is
also called a “qualifying event.” Specific qualifying events are listed later in this notice. After a qualifying e vent, COBRA
continuation coverage must be offered to each person who is a “qualified beneficiary.” You, your spouse, and your dependent
children could become qualified beneficiaries if coverage under the Plan is lost because of the qualifying event. Unde r the Plan,
qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage. If you’re an
employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying
events:
• Your hours of employment are reduced, or
• Your employment ends for any reason other than your gross misconduct.
If you’re the spouse of an employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because o f
the following qualifying events:
• Your spouse dies;
• Your spouse’s hours of employment are reduced;
• Your spouse’s employment ends for any reason other than his or her gross misconduct;
• Your spouse becomes entitled to Medicare benefits (under Part A, Part B, or both); or
• You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because of the following
qualifying events:
• The parent-employee dies;
• The parent-employee’s hours of employment are reduced;
• The parent-employee’s employment ends for any reason other than his or her gross misconduct;
• The parent-employee becomes entitled to Medicare benefits (Part A, Part B, or both);
• The parents become divorced or legally separated; or
• The child stops being eligible for coverage under the Plan as a “dependent child.”
When is COBRA continuation coverage available? The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has been notified
that a qualifying event has occurred. The employer must notify the Plan Administrator of the following qualifying events:
• The end of employment or reduction of hours of employment;
• Death of the employee; or
• The employee’s becoming entitled to Medicare benefits (under Part A, Part B, or both).
For all other qualifying events (divorce or legal separation of the employee and spouse or a dependent child’s losing eligibi lity for
coverage as a dependent child), the employee or a family member has a legal obligation to notify the City of Cincinnati or the Plan
Administrator within 60 days after the qualifying event occurs. You must provide this notice to: Anthem Benefits Administrat ion
Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each of
the qualified beneficiaries. Each qualified beneficiary will have an independent right to elect COBRA continuation coverage. Covered
employees may elect COBRA continuation coverage on behalf of their spouses, and parents may elect COBRA continuation coverage on
behalf of their children.
COBRA continuation coverage is a temporary continuation of coverage that generally lasts for 18 months due to employment termination
or reduction of hours of work. Certain qualifying events, or a second qualifying event during the initial period of coverage, may permit a
beneficiary to receive a maximum of 36 months of coverage.
There are also ways in which this 18-month period of COBRA continuation coverage can be extended:
Disability extension of 18-month period of COBRA continuation coverage
If you or anyone in your family covered under the Plan is determined by Social Security to be disabled and you notify the Plan
Administrator in a timely fashion, you and your entire family may be entitled to get up to an additional 11 months of COBRA c ontinuation
coverage, for a maximum of 29 months. The disability would have to have started at some time before the 60th day of COBRA
continuation coverage and must last at least until the end of the 18-month period of COBRA continuation coverage. This 11-month
extension is available to all individuals who are qualified beneficiaries due to a termination or reduction in hours of employment. To
benefit from this extension, a qualified beneficiary must notify the Plan Administrator of that determination within 60 days and before the
end of the original 18-month period. The affected individual must also notify the Plan Administrator within 30 days of any final
determination that the individual is no longer disabled.
Second qualifying event extension of 18-month period of continuation coverage
If your family experiences another qualifying event during the 18 months of COBRA continuation coverage, the spouse and dependent
children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if the Plan is
properly notified about the second qualifying event. This extension may be available to the spouse and any dependent children getting
COBRA continuation coverage if the employee or former employee dies; becomes entitled to Medicare benefits (under Part A, Par t B, or
both); gets divorced or legally separated; or if the dependent child stops being eligible under the Plan as a dependent child. This extension
is only available if the second qualifying event would have caused the spouse or dependent child to lose coverage under the P lan had the
first qualifying event not occurred.
Are there other coverage options besides COBRA Continuation Coverage?
Yes. Instead of enrolling in COBRA continuation coverage, there may be other coverage options for you and your family throug h the
Health Insurance Marketplace, Medicaid, or other group health plan coverage options (such as a spouse’s plan) through what is called a
“special enrollment period.” Some of these options may cost less than COBRA continuation coverage. You can learn more abo ut many
of these options at www.healthcare.gov.
If you have questions Questions concerning your Plan or your COBRA continuation coverage rights should be addressed to the contact or contacts iden tified below. For more information about your rights under the Employee Retirement Income Security Act (ERISA), including COBRA, the
Patient Protection and Affordable Care Act, and other laws affecting group health plans, contact the nearest Regional or District Office of
the U.S. Department of Labor’s Employee Benefits Security Administration (EBSA) in your area or visit www.dol.gov/ebsa. (Addresses
and phone numbers of Regional and District EBSA Offices are available through EBSA’s website.) For more information about th e
Marketplace, visit www.HealthCare.gov.
Keep your Plan informed of address changes
To protect your family’s rights, let the Plan Administrator know about any changes in the addresses of family members. You s hould also
keep a copy, for your records, of any notices you send to the Plan Administrator.
Plan contact information
If you have any questions about COBRA, please contact Phyliss Ward at (513)352-2566. Also, if you have a change in family status
(marriage, divorce, birth, death etc.) please complete a Health Insurance Form and forward it to City of Cincinnati Risk Management, 805
Central Avenue, Suite 100, Cincinnati, Ohio 45202 within 31 days of the change.