Clinical Investigation 30 Gy or 34 Gy? Comparing 2 Single-Fraction SBRT Dose Schedules for Stage I Medically Inoperable Non-Small Cell Lung Cancer Gregory M.M. Videtic, MD, CM, FRCPC, Kevin L. Stephans, MD, Neil M. Woody, MD, Chandana A. Reddy, MS, Tingliang Zhuang, PhD, Anthony Magnelli, MS, and Toufik Djemil, PhD Department of Radiation Oncology, Taussig Cancer Institute, Cleveland Clinic, Cleveland, Ohio Received Feb 4, 2014, and in revised form May 12, 2014. Accepted for publication May 14, 2014. Summary This is the largest institu- tional series to date to report the safety and efficacy of single-fraction stereotactic body radiation therapy for the treatment of patients with medically inoperable early stage lung cancer. In comparing outcomes of our 2 single-fraction dose sched- ules (30 Gy and 34 Gy, respectively), we found that both of the schedules pro- vided equivalent local con- trol and overall survival rates with minimal toxicity. This study further develops our understanding of the feasi- bility and appropriateness of lung radiosurgery. Purpose: To review outcomes of 2 single-fraction lung stereotactic body radiation therapy (SBRT) schedules used for medically inoperable early stage lung cancer. Methods and Materials: Patients in our institution have been treated on and off pro- tocols using single-fraction SBRT (30 Gy and 34 Gy, respectively). All patients had node-negative lung cancer measuring 5 cm and lying 2 cm beyond the trachea- bronchial tree and were treated on a Novalis/BrainLAB system with the ExactTrac positioning system for daily image guidance. Results: For the interval from 2009 to 2012, 80 patients with 82 lesions were treated with single-fraction lung SBRT. Fifty-five patients (69%) and 25 patients (31%) received 30 Gy and 34 Gy, respectively. In a comparison of 30 Gy and 34 Gy cohorts, patient and tumor characteristics were balanced and median follow-up in months was 18.7 and 17.8, respectively. The average heterogeneity-corrected mean doses to the target were 33.75 Gy and 37.94 Gy for the 30-Gy and 34-Gy prescriptions, respec- tively. Comparing 30-Gy and 34-Gy cohorts, 92.7% and 84.0% of patients, respec- tively, experienced no toxicity (P was not significant), and had neither grade 3 nor higher toxicities. For the 30-Gy and 34-Gy patients, rates of 1-year local failure, over- all survival, and lung cancer-specific mortality were 2.0% versus 13.8%, 75.0% versus 64.0%, and 2. 1% versus 16.0%, respectively (P values for differences were not sig- nificant). Conclusions: This is the largest single-fraction lung SBRT series yet reported. and it confirms the safety, efficacy, and minimal toxicity of this schedule for inoperable early stage lung cancer. Ó 2014 Elsevier Inc. Reprint requests to: Gregory M.M. Videtic, MD, CM, FRCPC, Department of Radiation Oncology, Cleveland Clinic, 9500 Euclid Ave, Mailroom T28, Cleveland, OH 44195. Tel: (216) 444-9797; E-mail: [email protected]This work was presented in part at the 53rd Annual Meeting of American Society of Radiation Oncology, Miami, FL, October 2-6, 2011. Conflicts of interest: none. Int J Radiation Oncol Biol Phys, Vol. 90, No. 1, pp. 203e208, 2014 0360-3016/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ijrobp.2014.05.017 Radiation Oncology International Journal of biology physics www.redjournal.org
Transcript
International Journal of
Radiation Oncology
biology physics
www.redjournal.org
Clinical Investigation
30 Gy or 34 Gy? Comparing 2 Single-FractionSBRT Dose Schedules for Stage I MedicallyInoperable Non-Small Cell Lung CancerGregory M.M. Videtic, MD, CM, FRCPC, Kevin L. Stephans, MD,Neil M. Woody, MD, Chandana A. Reddy, MS, Tingliang Zhuang, PhD,Anthony Magnelli, MS, and Toufik Djemil, PhD
Department of Radiation Oncology, Taussig Cancer Institute, Cleveland Clinic, Cleveland, Ohio
Received Feb 4, 2014, and in revised form May 12, 2014. Accepted for publication May 14, 2014.
Summary
This is the largest institu-tional series to date to reportthe safety and efficacy ofsingle-fraction stereotacticbody radiation therapy forthe treatment of patients withmedically inoperable earlystage lung cancer. Incomparing outcomes of our 2single-fraction dose sched-ules (30 Gy and 34 Gy,respectively), we found thatboth of the schedules pro-vided equivalent local con-trol and overall survival rateswith minimal toxicity. Thisstudy further develops ourunderstanding of the feasi-bility and appropriateness oflung radiosurgery.
Purpose: To review outcomes of 2 single-fraction lung stereotactic body radiationtherapy (SBRT) schedules used for medically inoperable early stage lung cancer.Methods and Materials: Patients in our institution have been treated on and off pro-tocols using single-fraction SBRT (30 Gy and 34 Gy, respectively). All patients hadnode-negative lung cancer measuring �5 cm and lying �2 cm beyond the trachea-bronchial tree and were treated on a Novalis/BrainLAB system with the ExactTracpositioning system for daily image guidance.Results: For the interval from 2009 to 2012, 80 patients with 82 lesions were treatedwith single-fraction lung SBRT. Fifty-five patients (69%) and 25 patients (31%)received 30 Gy and 34 Gy, respectively. In a comparison of 30 Gy and 34 Gy cohorts,patient and tumor characteristics were balanced and median follow-up in months was18.7 and 17.8, respectively. The average heterogeneity-corrected mean doses to thetarget were 33.75 Gy and 37.94 Gy for the 30-Gy and 34-Gy prescriptions, respec-tively. Comparing 30-Gy and 34-Gy cohorts, 92.7% and 84.0% of patients, respec-tively, experienced no toxicity (P was not significant), and had neither grade 3 norhigher toxicities. For the 30-Gy and 34-Gy patients, rates of 1-year local failure, over-all survival, and lung cancer-specific mortality were 2.0% versus 13.8%, 75.0% versus64.0%, and 2. 1% versus 16.0%, respectively (P values for differences were not sig-nificant).Conclusions: This is the largest single-fraction lung SBRT series yet reported. and itconfirms the safety, efficacy, and minimal toxicity of this schedule for inoperable earlystage lung cancer. � 2014 Elsevier Inc.
etic, MD, CM, FRCPC,
Clinic, 9500 Euclid Ave,
(216) 444-9797; E-mail:
This work was presented in part at the 53rd Annual Meeting of
American Society of Radiation Oncology, Miami, FL, October 2-6, 2011.
Videtic et al. International Journal of Radiation Oncology � Biology � Physics204
Introduction
The optimal stereotactic body radiation therapy (SBRT)dose schedule for medically inoperable stage I non-smallcell lung cancer (NSCLC), defined as “peripheral” becauseit is located �2 cm from the proximal trachea-bronchialtree (1), is an active area of investigation. The RadiationTherapy Oncology Group (RTOG) phase 2 trial 0236established 60 Gy in 3 fractions as the reference schedulefor this clinical presentation in the United States (1). Asmall number of published reports (2-5) have suggested thatlung SBRT delivered as a single-fraction regimen may offerfeasibility, local control, and minimal toxicity similar tothat of fractionated SBRT. The recently completed RTOGrandomized phase 2 trial 0915 tested 34 Gy in 1 fractionversus 48 Gy in 4 fractions for medically inoperableNSCLC patients with peripheral lesions, with its primaryendpoint being a comparison of toxicity rates between thearms at 1 year (6). An ongoing randomized phase 2 lungSBRT trial led by the Roswell Park Institute (RPCI; NCIstudy I 124407) (3) is comparing 30 Gy in a single-fractionwith 60 Gy in 3 fractions with the primary endpoints beingtoxicity and survival for patients and is using the sameeligibility criteria as RTOG 0236 (7).
Our institution actively enrolled patients in the above-mentioned studies and, after developing expertise in treatingpatients randomized to the single-fraction arm of these trials,we elected to offer this approach to appropriately selectedpatients off protocol who were not able to be enrolled in thestudies, while still treating all such patients per the protocolparameters. Recalling that RTOG 0915 had a primaryendpoint measured at 1 year (6), we elected to report ourearly experience in treating patients with single-fraction lungSBRT to further help inform our understanding of the safetyand efficacy of this fractionation schedule.
Methods and Materials
Patients
For this retrospective review, we surveyed our institutionalreview board-approved SBRT prospective data registry for allmedically inoperable lung cancer patients treated with asingle-fraction up until July 2012. In all cases, medical inop-erability was established by an experienced thoracic surgeonand/or pulmonologist. Pretreatment evaluations included acomplete history and physical examination with a detailedrespiratory examination. Pretreatment investigations includedobjective pulmonary function tests that included spirometryand diffusion capacity. All patients were staged usingcomputed tomography (CT) of the chest, abdomen, and pelvis,imaging of the brain (using magnetic resonance imaging[MRI] or CT) and positron emission tomography (PET).Routine mediastinoscopy or bronchoscope-guided ultraso-nography (EBUS) nodal sampling was not required and was
performed at the discretion of the treating physicians. How-ever, if a mediastinal node was hypermetabolic on PET im-aging, it was recommended that the patient undergo EBUSsampling of the node. For patients to be considered for single-fraction SBRT but not enrolled in the relevant protocols (seebelow), atminimum they had tomeet the trials’ tumor size andperipheral location requirements. According to previouslypublished practice (5, 8), patients with lung lesions wherebiopsy was medically contraindicated or nondiagnostic butwhich had demonstrated growth on serial CT scan imagingandwere hypermetabolic onPETimagingwithout evidence ofregional nodal or distant disease were labeled as “clinical” or“radiographic” early stage malignancies and were thereforeeligible to be treated with lung SBRT.
Protocol and treatment overviews
Fully referenced and detailed protocols are available for theRTOG 0915 and RPCI trials (2, 3). Briefly, RTOG 0915randomly assigned patients to receive 34 Gy in 1 fraction or48 Gy in 4 consecutive once-daily fractions and compared therate of 1-year grade 3 or higher protocol-specified adverseevents that were attributable to the treatment. Eligible patientshad medically inoperable, biopsy-proven early stage T1/T2(�5 cm) NSCLC, were clinically node negative by PET, andhad peripherally located tumors (�2 cm in all directionsaround the proximal bronchial tree). According to this pro-tocol’s parameters, our patients were simulated using abdom-inal compression for tumormotion control; the planning targetvolume (PTV) consisted of the gross tumor volume (GTV)expanded to account for motion under maximal inhalation andexhalationwhile under compression; heterogeneity correctionswere used; and treatment involved image-guided intensitymodulated radiation therapy (IMRT)-based delivery. For RPCII 124407, patients were randomized to receive 30 Gy in 1fractionor 60Gy in 3 fractions delivered over 8 to 14 days,withthe trial’s primary endpoints being toxicity and survival. Pa-tient eligibility and SBRT planning and delivery were similarto those used in RTOG 0236 (1), including homogeneoustreatment planning. After restricting tumor excursion on fluo-roscopy to <1 cm, the PTV consisted of the GTV with fixedexpansions of an additional 0.5 cm in the axial plane and1.0 cm in the longitudinal plane.
Patients potentially eligible for these trials but missingeligibility criteria for enrollment (eg biopsy result showingproof of malignancy) were made aware of the possibility ofreceiving single-fraction lung SBRT off protocol. Havingdiscussed risks and benefits of this approach compared toroutine SBRT, treatment was only delivered followinginformed consent. Whether 30 Gy or 34 Gy was selected inthe off-protocol setting was a function of the time periodwhen the patient was treated and/or at the discretion of thetreating physician.
All patients in a given dose cohort received planning andprescriptions always consistent with the given protocol’sinstructions. However, because the protocols differed in the
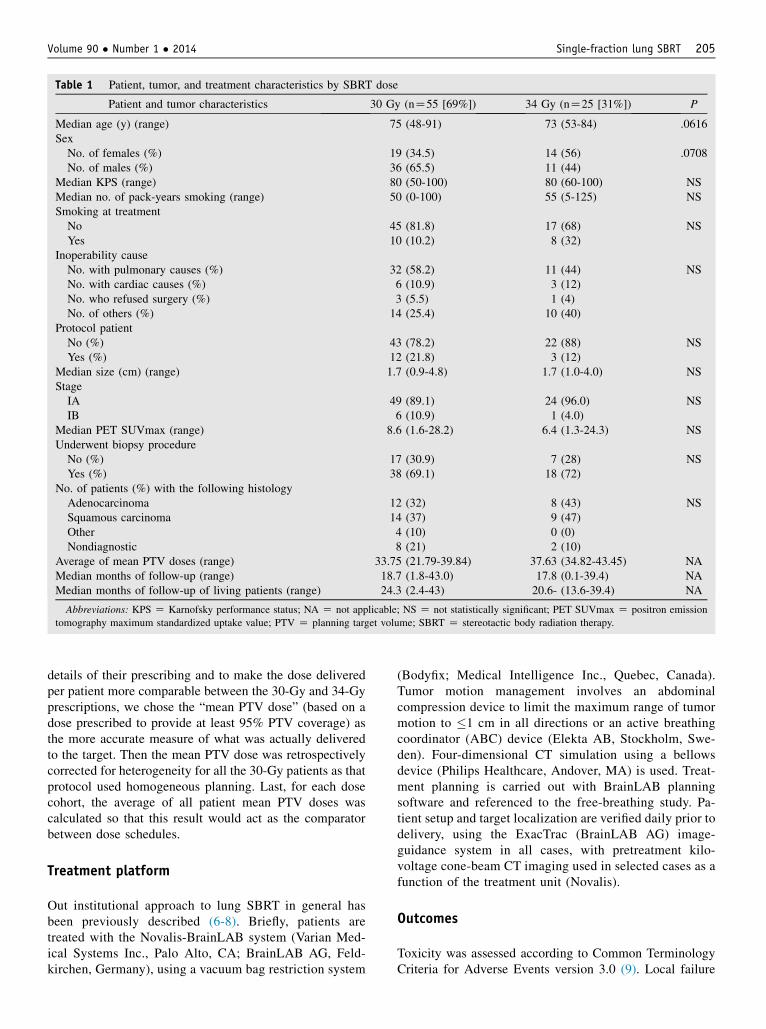
Table 1 Patient, tumor, and treatment characteristics by SBRT dose
Patient and tumor characteristics 30 Gy (nZ55 [69%]) 34 Gy (nZ25 [31%]) P
Median age (y) (range) 75 (48-91) 73 (53-84) .0616Sex
No. of females (%) 19 (34.5) 14 (56) .0708No. of males (%) 36 (65.5) 11 (44)
Median KPS (range) 80 (50-100) 80 (60-100) NSMedian no. of pack-years smoking (range) 50 (0-100) 55 (5-125) NSSmoking at treatment
No 45 (81.8) 17 (68) NSYes 10 (10.2) 8 (32)
Inoperability causeNo. with pulmonary causes (%) 32 (58.2) 11 (44) NSNo. with cardiac causes (%) 6 (10.9) 3 (12)No. who refused surgery (%) 3 (5.5) 1 (4)No. of others (%) 14 (25.4) 10 (40)
No. of patients (%) with the following histologyAdenocarcinoma 12 (32) 8 (43) NSSquamous carcinoma 14 (37) 9 (47)Other 4 (10) 0 (0)Nondiagnostic 8 (21) 2 (10)
Average of mean PTV doses (range) 33.75 (21.79-39.84) 37.63 (34.82-43.45) NAMedian months of follow-up (range) 18.7 (1.8-43.0) 17.8 (0.1-39.4) NAMedian months of follow-up of living patients (range) 24.3 (2.4-43) 20.6- (13.6-39.4) NA
Abbreviations: KPS Z Karnofsky performance status; NA Z not applicable; NS Z not statistically significant; PET SUVmax Z positron emission
tomography maximum standardized uptake value; PTV Z planning target volume; SBRT Z stereotactic body radiation therapy.
details of their prescribing and to make the dose deliveredper patient more comparable between the 30-Gy and 34-Gyprescriptions, we chose the “mean PTV dose” (based on adose prescribed to provide at least 95% PTV coverage) asthe more accurate measure of what was actually deliveredto the target. Then the mean PTV dose was retrospectivelycorrected for heterogeneity for all the 30-Gy patients as thatprotocol used homogeneous planning. Last, for each dosecohort, the average of all patient mean PTV doses wascalculated so that this result would act as the comparatorbetween dose schedules.
Treatment platform
Out institutional approach to lung SBRT in general hasbeen previously described (6-8). Briefly, patients aretreated with the Novalis-BrainLAB system (Varian Med-ical Systems Inc., Palo Alto, CA; BrainLAB AG, Feld-kirchen, Germany), using a vacuum bag restriction system
(Bodyfix; Medical Intelligence Inc., Quebec, Canada).Tumor motion management involves an abdominalcompression device to limit the maximum range of tumormotion to �1 cm in all directions or an active breathingcoordinator (ABC) device (Elekta AB, Stockholm, Swe-den). Four-dimensional CT simulation using a bellowsdevice (Philips Healthcare, Andover, MA) is used. Treat-ment planning is carried out with BrainLAB planningsoftware and referenced to the free-breathing study. Pa-tient setup and target localization are verified daily prior todelivery, using the ExacTrac (BrainLAB AG) image-guidance system in all cases, with pretreatment kilo-voltage cone-beam CT imaging used in selected cases as afunction of the treatment unit (Novalis).
Outcomes
Toxicity was assessed according to Common TerminologyCriteria for Adverse Events version 3.0 (9). Local failure
Videtic et al. International Journal of Radiation Oncology � Biology � Physics206
was defined as progressive and increasing CT scan abnor-malities, confirmed by progressive and incremental in-creases in a lesion’s standard uptake values (SUVs) onserial PET imaging, with or without biopsy. Nodal failurewas defined as radiographic (PET or CT) progression in thehilum or mediastinum. Distant failure was defined as thepresence of distant metastases on clinical examination orimaging. Outcomes were measured from the initiation ofSBRT until death or last patient contact. Local failure,nodal failure, distant metastases, and cause-specific mor-tality were calculated using cumulative incidence analysiswith death due to non-lung cancer causes treated as acompeting event. Overall survival estimates were calcu-lated using Kaplan-Meier analysis. Statistical analyses wereperformed using StatView version 5.0 and SAS version 9.2software (SAS Institute, Cary, NC), and a P value less than.05 was considered statistically significant.
Results
For this analysis, the interval from December 3, 2009, toJuly 1, 2012, was surveyed and yielded 80 patients with 82lesions treated with single-fraction lung SBRT. The firstpatient treated in our institution with single-fraction SBRTwas treated in the 30-Gy arm of the RPCI protocol onDecember 3, 2009. Our first patient randomized to the 34-Gy arm of RTOG 0915 was treated on September 9 and 21,2010. Regardless of indication and approach, 13% and 25%of 30-Gy and 34-Gy patients, respectively, had some formof mediastinal nodal sampling. Table 1 provides a summaryof patient, dose, and tumor characteristics, which overallwere balanced between the groups. Differences in medianfollow-up for all and living-only patients reflect initiationof the protocols at different points in time. Of interest, theaverage of the mean PTV doses for the 34-Gy patients wasgreater than that of the 30-Gy cohort.
All treatments were completed as planned. Comparing30-Gy and 34-Gy cohorts, 92.7% and 84.0% of patients,respectively, experienced no toxicity (PZnonsignificant),and no grade 3 or higher toxicity was reported in eithercohort. Table 2 provides details for the patients whoexperienced toxicities. Of those patients, the one with the
Table 2 Selected patient, tumor and treatment characteristics for pa
Date of SBRT(mo/day/y) Sex
Age atSBRT (y) Tumor size (cm) Dose (Gy)
12/3/2009 M 68 3.3 305/12/2010 F 77 3.8 307/26/2010 M 73 1.6 309/1/2010 F 76 1.4 3011/22/2010 F 75 3.5 345/23/2011 M 73 1.8 345/23/2011 F 83 1.9 3411/14/2011 F 54 1.5 34
Abbreviations: CWP Z chest wall pain/neuropathy; SBRT Z stereotactic b
longest time to resolution of toxicity (12.7 months) had hadprevious postradical mastectomy radiation therapy on thesame side as her lung cancer 59 years prior to her SBRT.Figure 1 through 3 present Kaplan-Meier curves for localfailure, overall survival, and lung cancer-specific mortality.Table 3 provides a summary of results at 1 year. For theseoutcomes, there were no significant differences betweeneither of the 2 treatment schedules.
Discussion
This single-institution retrospective study comparing out-comes for 2 single-fraction SBRT regimens modeled inrecent clinical trials is the largest single-fraction report todate. Mindful of the limitations of any such analysis, thefindings in the present report confirm the general findingsof lung SBRT that have been reported in the literature forother schedules, which include efficacy, seen as excellentlocal control, and safety, with minimal incidence andgrades of toxicity. Furthermore, overall survival remainsbetter than that in historic series in which similar patientswere treated with conventional radiation therapy (1). Themain cause of failure among lung SBRT patients remainsdistant recurrence, and noncancer-related deaths are themain cause of mortality. With respect to comparing the 2treatment schedules and mindful of the retrospective natureof this study, both of them also appeared to be similar withrespect to overall efficacy, failure, causes of death, andoverall survival. The absolute differences in local andregional control between the 2 doses that favored the 30-Gyschedule are provocative but must be considered withcaution, given the study limitations. In that context, it isinstructive to compare the present results with the those ofother published single-fraction lung SBRT studies usingeither of these dose schedules.
In 2006, Le et al (10) described a dose escalation expe-rience with single-fraction SBRT. In that study, 21 patientshad primary NSCLC, and 11 patients had lung metastases.Patients were treated as a dose cohort starting at 15 Gy/fraction, followed by dose escalation of 5 to 10 Gy to amaximal dose of 30 Gy/fraction. Only 2 patients were treatedwith 30 Gy, and the authors noted that this small number
prevented them from making any definitive statements otherthan it appeared to be safe in previously unirradiated patients.
Fritz et al (11) reported a prospective study of 58 pa-tients treated with single-fraction 30-Gy lung SBRT. Ofthose patients, 33 were patients with stage I NSCLC.Overall, our results are in keeping with results of thatreport, but it is remarkable that their median target diameterwas 5.5 cm (range, 1.5-10 cm), which is larger than oursand also larger than that reported in most North Americanlung SBRT series. With a median follow-up of 18 months,local tumor control was 83% and overall survival was 83%at 1 year and 39% at 4 years. There were no grade 3 orhigher toxicities reported.
A 2006 report by Hara et al (12) provided the basis forthe 34-Gy arm in the RTOG 0915 protocol, as it is thehighest reported single-fraction lung SBRT to date. Theauthors described outcomes for 59 patients with tumors
Fig. 2. Overall survival by stereotactic body radiationtherapy dose.
<4 cm in maximal dimension, treated with doses rangingfrom 26 to 34 Gy in a single fraction. Of note, only 11patients had primary lung tumors whereas the rest weremetastases. Median follow-up for the whole cohort was12 months (range, 2-42 months). Fifty tumors received�30 Gy (range, 30-34 Gy). Overall survival rates were76.5% at 1 year and 41% at 2 years, respectively. The2-year local progression-free rates for tumors that wereirradiated at doses �30 Gy were 83% and 52% for tumorstreated with <30 Gy. Overall, grade 3 respiratory toxicitywas seen in 1 patient, with no higher grade toxicities re-ported. Although the authors did suggest that a dose-response effect exists for single-fraction therapy (with thecutoff being 30 Gy), they did not otherwise stratify theiroutcomes by tumor type (primary vs metastatic), toxicity,or doses delivered, so comparisons with our results are notfeasible.
In 2007, Hof et al (13) reported outcomes for 42 patientswith stage I or II NSCLC treated with single-dose SBRT,with doses ranging from 19 Gy to 30 Gy. Thirty-two pa-tients were treated with doses between 26 Gy and 30 Gy,but results were not reported by dose schedule. For thewhole cohort and with a median follow-up of 15 months,overall survival and disease-free survival at 36 months were
Table 3 Outcomes at 1 year according to SBRT dose
Outcome
Rate at 1 y (95% CI) under thedose schedules shown
Videtic et al. International Journal of Radiation Oncology � Biology � Physics208
37.4% and 49.1%, respectively. Local tumor control at3 years was 67.9%. Local tumor control at 1 year wassignificantly improved in those patients receiving 26 to30 Gy (100%) versus those who received lower doses(62.5%; PZ.032). Interestingly they noted that 31% ofpatients failed distantly but that the results were not strat-ified by dose schedule. With respect to toxicity, no grade 3or 4 toxicity was noted. Our results are consistent withthose of that report.
In most institutions, single-fraction lung SBRT remainsinvestigational. The current North American referenceschedule established for treating the population of patientsin our report is based on RTOG 0236, which consisted of60 Gy in 3 fractions over 8 to 14 days (or 54 Gy in 3fractions, when planned with lung heterogeneity correc-tions) (1). This phase 2 study accrued 59 patients, 55 ofwhich were evaluable. For a median follow-up of34.4 months, the 3-year overall survival rate was 55.8%,with a median survival of 48.1 months. The 3-year localcontrol rate was 97.6%. The rate of toxicity � grade 3 was16.3%, with no grade 5 toxicity reported. Because ourcontrol and survival results are inferior to those prospectiveresults, this emphasizes clearly that the optimal under-standing of single-fraction lung SBRT will come from thecompletion of the trials cited above. In that regard, resultsfor RTOG 0915 were recently presented in abstract form.For the 34-Gy arm at 1 year; and rates of local control,progression-free survival, and overall survival were 97.1%,78.0%, and 85.4%, respectively. Grade 3 or higher toxicitywas reported in 9.8% of patients (14).
Conclusions
The present retrospective study is the largest single-fractionlung SBRT series reported to date. It describes 2 differentsingle-dose schedules, both of which appear feasible, safe,and effective and provide acceptable outcomes comparableto each other and to results from more conventional frac-tionated lung SBRT. Findings of this study are also inkeeping with those of published single-fraction lung SBRTliterature. Results from ongoing and completed prospectivetrials using a single-fraction approach will provide moreinsights into these high-dose schedules.
References
1. Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation
therapy for inoperable early stage lung cancer. JAMA 2010;303:1070-